Tattoo-Associated Sarcoid-like Uveitis: A Multicenter Registry Study
Ryoji Yanai, Yuko Misaki, Mariko Egawa, Shido Nagaki, Kumi Shirai, Toshikatsu Kaburaki, Suguru Nakagawa, Yukako Hiramatsu, Kinya Tsubota, Yoshihiko Usui, Sho-Hei Uchi, Takanori Aoki, Kenji Nagata, Chie Sotozono, Shiori Kuramoto, Nobuyo Yawata, Koh-Hei Sonoda

TL;DR
This study examines the characteristics and outcomes of uveitis linked to tattoos, finding it often recurs and causes eye pressure issues.
Contribution
The study provides a detailed multicenter analysis of tattoo-associated sarcoid-like uveitis, highlighting its clinical course and treatment patterns.
Findings
70% of patients experienced uveitis recurrence during follow-up.
80% of patients required glaucoma or intraocular pressure-lowering therapy.
Extraocular inflammation was observed in 70% of patients at the tattoo site.
Abstract
Background: This study aims to characterize the clinical features and outcomes of tattoo-associated sarcoid-like uveitis using a multicenter uveitis registry given the limited existing data. Design: This is a retrospective study. Participants: Ten patients (20 eyes) diagnosed with tattoo-associated sarcoid-like uveitis took part in the study. Methods: The data of patients newly evaluated at participating registry centers from January 2000 to June 2025 were reviewed. Demographic data, treatments, visual acuity, recurrence, glaucoma/intraocular pressure (IOP)-lowering therapy, extraocular involvement, and histologic confirmation were extracted when available. Main Outcome Measures: Recurrence, glaucoma/IOP-lowering therapy, extraocular involvement, and change in logarithm of the minimum angle of resolution (logMAR) from presentation to final follow-up were measured. Results: Seven (70%)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
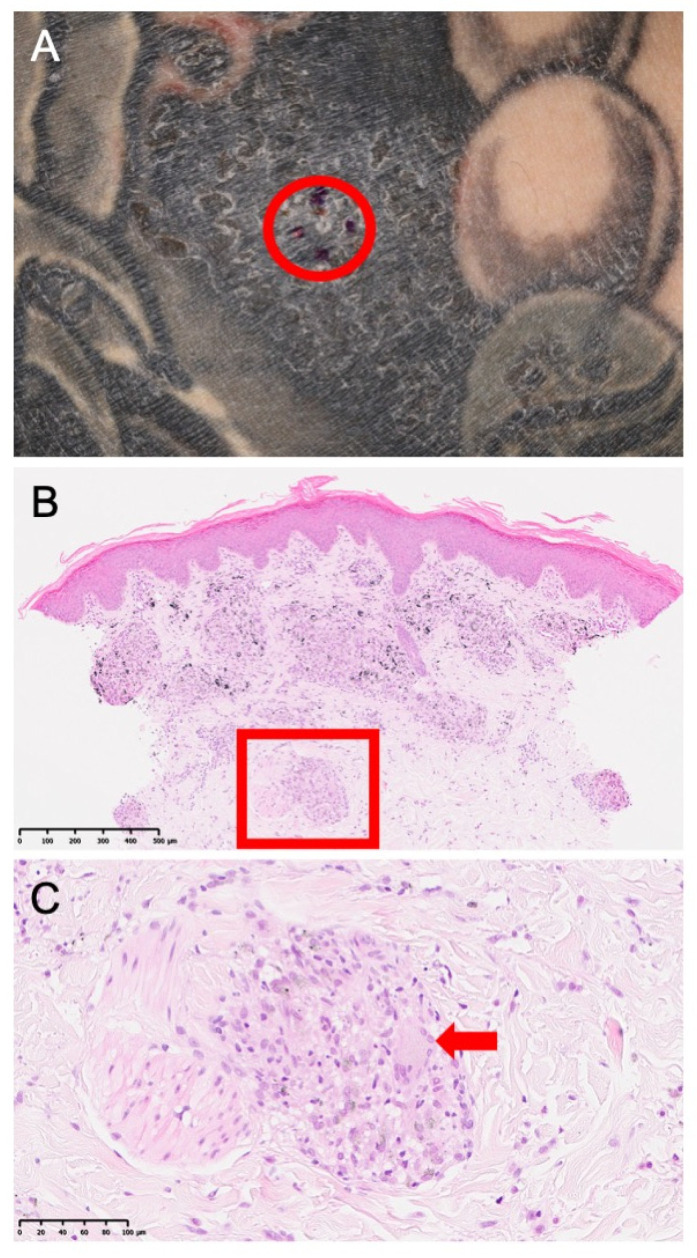 Figure 1
Figure 1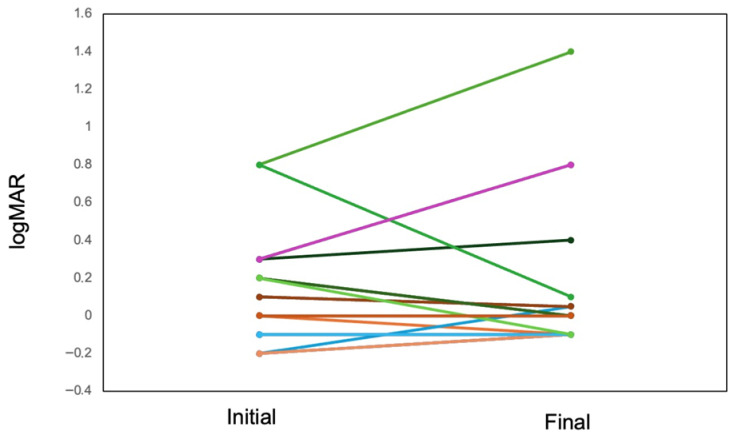 Figure 2
Figure 2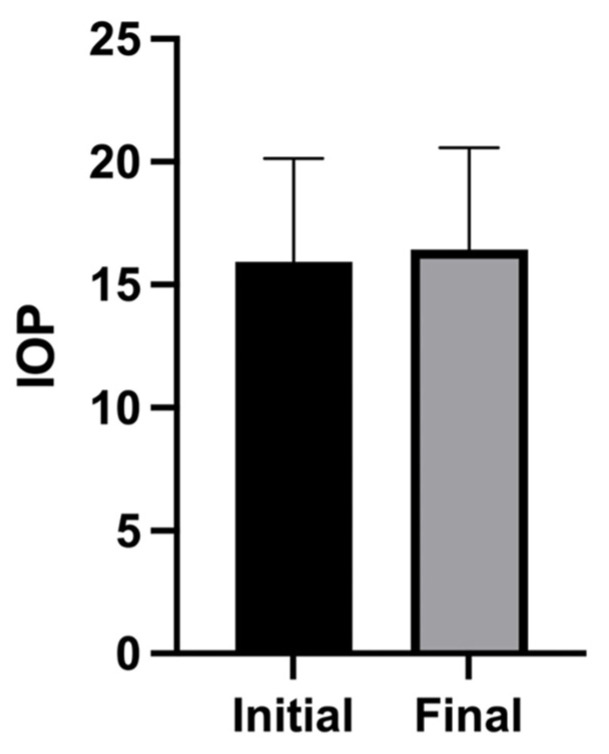 Figure 3
Figure 3- —JSPS KAKENHI
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTattoo and Body Piercing Complications · Sarcoidosis and Beryllium Toxicity Research · Ocular Diseases and Behçet’s Syndrome
1. Introduction
Tattooing has become increasingly prevalent worldwide, particularly among younger individuals [1,2,3,4], and cutaneous reactions to tattoo pigments range from acute inflammation to chronic granulomatous disease [1]. During tattooing, ink is injected into multiple skin layers, where it becomes fixed within the dermis. The process is intended to temporarily suppress local immune responses, but trace ink particles are transported systemically by circulating white blood cells. A proportion of pigment remains at the injection site through uptake by tissue-resident macrophages and persists via a “capture–release–recapture” mechanism, ensuring long-term visibility [5,6].
Tattoo granuloma with uveitis is recognized as a distinct clinical entity, often overlapping clinically and histopathologically with sarcoidosis [7,8,9,10]. According to prior reports and reviews, tattoo-associated uveitis is commonly bilateral and recurrent, and may be accompanied by systemic sarcoidosis or sarcoid-like inflammation [7,8,9,10,11,12,13,14]. However, the existing evidence is limited to single-center series and case reports, and comprehensive data on the treatment patterns and outcomes remain scarce [8,10]. To address this gap, the present study aimed to explore the clinical spectrum, treatments, recurrence, and glaucoma-related outcomes of tattoo-associated sarcoid-like uveitis in Japan using a national coverage-multicenter uveitis registry.
2. Materials and Methods
Study design and setting: We conducted a retrospective analysis of the data obtained from patients enrolled in a national coverage-multicenter uveitis registry. Patients newly presenting to the participating registry centers from January 2000 to June 2025 were included.
Definition: In the present study, tattoo-associated sarcoid-like uveitis was defined as follows: (1) uveitis with granulomatous features clinically consistent with ocular sarcoidosis; (2) a temporal association with tattoo inflammation or pigment-related cutaneous findings; and (3) physician attribution of uveitis to tattoo-associated sarcoid-like disease.
Data collection: Demographic data (age and sex), laterality, laboratory results, extraocular involvement, treatments (topical corticosteroids, periocular corticosteroid injections, systemic corticosteroids, and immunomodulatory therapy), and clinical outcomes were extracted from the patients’ medical records. Missing data were assessed for each variable. The analyses were primarily conducted using available-case (pairwise) data; the denominator, therefore, varies across analyses depending on data availability. No imputation was performed because missingness reflected incomplete documentation in routine clinical care.
Outcome measures: The primary outcomes included uveitis recurrence, glaucoma/intraocular pressure (IOP)-lowering therapy, extraocular involvement, and change in logarithm of the minimum angle of resolution (logMAR) visual acuity from presentation to final follow-up, with visual acuity analyzed at the eye level (20 eyes). Uveitis recurrence was defined as disease activity requiring the initiation or escalation of anti-inflammatory treatment, and glaucoma/IOP-lowering therapy was defined as the need for the initiation or escalation of IOP-lowering treatment.
Statistical analysis: Continuous variables are presented as means ± standard deviations or medians (interquartile ranges), whereas categorical variables are provided as counts (percentages).
3. Results
Ten patients (20 eyes) met the inclusion criteria, representing 100% of the patients enrolled in the registry (Table 1). Among these, seven (70%) were male, and the mean age was 35.1 ± 7.8 (27–44) years. The median follow-up duration was 19.1 (interquartile range: 8.3–26.0) months. Histologic confirmation at the tattoo site was obtained in four patients (40%, Figure 1). Bilateral hilar lymphadenopathy was not observed in any case (0/10). Elevated angiotensin-converting enzyme and elevated soluble IL-2 receptor levels were documented in 2/10 and 4/10 cases, respectively (Table 2). T-spot testing was negative in patients in whom it was performed, with several cases not assessed (Table 2). Data on latency from tattooing to uveitis onset, which ranged from 1 to 29 years, were available in four cases (Table 2).
At the eye level, the mean logMAR visual acuity across 20 eyes was 0.12 at presentation and 0.15 at the final follow-up (Figure 2). Consistent with this, the patient-level mean logMAR values showed a limited overall change between baseline and final follow-up across individual cases (Table 2). The IOP changed from 14.5 ± 4.1 mmHg (mean ± standard deviation) at the initial visit to 17.6 ± 4.0 mmHg at the final visit (Figure 3). Macular edema was frequently observed, occurring bilaterally in seven patients and unilaterally (left eye) in one patient, affecting a total of 15 out of 20 eyes (75%) (Table 2). Anterior segment inflammation (anterior chamber inflammatory cells) was frequently observed. Vitreous involvement—manifesting as clumped and/or diffuse vitreous opacities—was also common. Posterior segment vasculitic features, including retinal periphlebitis, perivascular nodules, and candle-wax-like retinochoroidal exudates, were variably present. Granulomatous lesions involving the optic disc and/or choroid were noted in a subset of eyes. Structural complications, including tent-shaped/trapezoidal peripheral anterior synechiae and photocoagulation-like retinochoroidal atrophic lesions, were also observed in some cases (Table 3). All cases in the present study had bilateral glaucoma associated with uveitis. Etiologically, 70% of the patients were classified as having glaucoma related to sarcoidosis/uveitis, 50% as having steroid-induced glaucoma, and 40% as having mixed (overlapping) mechanisms. Recurrence occurred in seven cases (70%), and glaucoma/IOP-lowering therapy was required in eight cases (80%) (Table 4). Extraocular inflammation affected the skin/tattoo in seven patients (70%) and the axillary lymph nodes in one (10%) patient.
All patients received topical corticosteroids. Periocular corticosteroid injections were administered in seven patients (70%), oral systemic corticosteroids in four (40%), cyclosporin in one (10%), and adalimumab in two (20%) (Table 4 and Table 5).
4. Discussion
A key strength of the present multicenter registry study is its presentation of a comprehensive case series, which included substantially more patients in the analysis compared with prior reports. Tattoo-associated sarcoid-like uveitis was consistently bilateral and frequently recurrent, with over half of the patients requiring IOP-lowering therapy. These findings align with previous case series and comparative reviews, which describe a chronic course and an overlap with systemic sarcoidosis or sarcoid-like granulomatous inflammation [8,9,10].
The high rates of recurrence and glaucoma/IOP-lowering therapy provision suggest that ongoing inflammation can cause secondary structural complications. The proposed mechanisms include persistent antigenic stimulation by tattoo pigments and delayed hypersensitivity or foreign-body granulomatous reactions, potentially extending from the skin to the ocular tissues [10,15]. Elevated IOP was attributed to chronic inflammation in three eyes, steroid-induced glaucoma in one eye, and both mechanisms in four eyes. These findings also indicate that persistent ocular inflammation is a key feature of tattoo-associated sarcoid-like disease and highlight the need for careful differentiation between inflammation-driven and steroid-induced IOP elevations in clinical management.
Notably, not all tattoos pose the same health risks. In traditional Japanese hand-poked tattooing (tebori), famously depicted in Jun-Ichirō Tanizaki’s debut novella Shisei (“The Tattooer”), carbon-based sumi ink, which is regarded as less allergenic owing to carbon’s relative biocompatibility, is often used. Contrarily, modern machine tattoos may incorporate chemically diverse pigments, including azo dyes, quinacridones, phthalocyanines for vivid blue and green hues, and inorganic pigments (e.g., iron oxides and titanium dioxides). These mixtures have been implicated in hypersensitivity reactions and may pose infectious and systemic safety risks [16,17,18,19].
Beyond pigment composition, experimental and ex vivo human studies have indicated that tattoo pigments and trace-element impurities are not confined to the dermis. Using synchrotron-based analyses, colored pigments and associated metals were detected in the regional lymph nodes of tattooed donors, providing evidence of translocation via the lymphatic pathways. Although the clinical significance of such deposition remains unclear, pigment accumulation in the lymph nodes could promote chronic immune activation, complicate lymphadenopathy interpretation, and contribute to sarcoid-like granulomatous responses in predisposed individuals [20].
Most patients were treated with topical and periocular corticosteroids, whereas systemic corticosteroids and biologic therapies were used selectively. Given the potential for systemic involvement, including lymphadenopathy and pulmonary disease, as reported previously [3,10,12], coordinated evaluation with dermatology and internal medicine may be warranted when tattoo-associated inflammation occurs alongside uveitis [21].
The present study has several limitations, including the small sample size, variable data completeness across centers, and lack of standardized, detailed phenotyping, such as uniform anterior chamber cell grading or imaging biomarkers. However, its multicenter registry design provides pragmatic real-world data on the treatment patterns and clinically meaningful outcomes of this rare condition. From a clinical perspective, our findings underscore the importance of considering the presence of tattoo-associated sarcoid-like disease in patients with recurrent uveitis, particularly when ocular flares coincide with inflammation or swelling of the tattooed skin and support the need for coordinated ophthalmologic and systemic evaluations to guide the diagnosis and management of this condition. Another limitation is that the patients’ visual acuity was analyzed at the eye level, whereas the other outcomes were evaluated at the patient level. Although clinically appropriate for bilateral disease, this difference in analytic units may introduce bias in interpretation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kluger N. Epidemiology of tattoos in industrialized countries Curr. Probl. Dermatol.20154862010.1159/00036917525833619 · doi ↗ · pubmed ↗
- 2Kluger N. SeitéS. Taieb C. The prevalence of tattooing and motivations in five major countries over the world J. Eur. Acad. Dermatol. Venereol.201933 e 484e 48610.1111/jdv.1580831310367 · doi ↗ · pubmed ↗
- 3Theune L.E. Ghoreishi N. Weikert C. Müller-Graf C. Engel C. Wirkner K. Baber R. Laux P. Luch A. Giulbudagian M. Characteristics of a tattooed population and a possible role of tattoos as a risk factor for chronic diseases: Results from the LIFE-adult-study P Lo S ONE 202520 e 031922910.1371/journal.pone.031922940924708 PMC 12419626 · doi ↗ · pubmed ↗
- 4Baranska A. Shawket A. Jouve M. Baratin M. Malosse C. Voluzan O. Vu Manh T.P. Fiore F. Bajénoff M. Benaroch P. Unveiling skin macrophage dynamics explains both tattoo persistence and strenuous removal J. Exp. Med.20182151115113310.1084/jem.2017160829511065 PMC 5881467 · doi ↗ · pubmed ↗
- 5Strandt H. Voluzan O. Niedermair T. Ritter U. Thalhamer J. Malissen B. Stoecklinger A. Henri S. Macrophages and fibroblasts differentially contribute to tattoo stability Dermatology 202123729630210.1159/00050654032344413 · doi ↗ · pubmed ↗
- 6Lin C. Marquardt Y. Rütten S. Liao L. Rahimi K. Haraszti T. Baron J.M. Bartneck M. Macrophage-like rapid uptake and toxicity of tattoo ink in human monocytes Immunology 202417138840110.1111/imm.1371437964593 · doi ↗ · pubmed ↗
- 7Ostheimer T.A. Burkholder B.M. Leung T.G. Butler N.J. Dunn J.P. Thorne J.E. Tattoo-associated uveitis Am. J. Ophthalmol.2014158637643.e 110.1016/j.ajo.2014.05.01924875002 · doi ↗ · pubmed ↗
- 8Kluger N. Tattoo-associated uveitis with or without systemic sarcoidosis: A comparative review of the literature J. Eur. Acad. Dermatol. Venereol.2018321852186110.1111/jdv.1507029763518 · doi ↗ · pubmed ↗