Treatment Failure and Overall Survival in Patients with Sinonasal Squamous Cell Carcinoma (SNSCC): A Systematic Review and Meta-Analysis
Urszula Kacorzyk, Aleksandra Krzywon, Magdalena Szymala-Cortez, Alexander Jorge Cortez, Krzysztof Składowski, Tomasz Rutkowski

TL;DR
This study finds that local recurrence is the main reason for treatment failure in sinonasal squamous cell carcinoma, with poor 5-year survival rates.
Contribution
The study provides a meta-analysis of treatment failure patterns and survival in sinonasal squamous cell carcinoma.
Findings
Local recurrence was the most common treatment failure (27%) in sinonasal squamous cell carcinoma.
The 5-year overall survival rate was approximately 50%.
No significant correlation was found between recurrence rates and overall survival.
Abstract
Sinonasal squamous cell carcinoma (SNSCC) is the most common malignant tumor of the sinonasal region and remains associated with poor survival. In this meta-analysis, we evaluated patterns of treatment failure—local recurrence (LR), nodal recurrence (NR), and distant metastasis (DM)—and their relationship with overall survival (OS). Across 13 studies including 749 patients, LR was the predominant mode of failure (27%), whereas NR and DM were less frequent. No significant correlations between recurrence rates and OS were observed, likely reflecting heterogeneity and limited reporting across studies. These findings confirm the dominant role of local failure in SNSCC and highlight the need for improved local control strategies. Objective: Prognosis in SNSCC remains poor mainly for local failure. Due to the rarity of this disease, and heterogeneity as to site and stage, most of the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
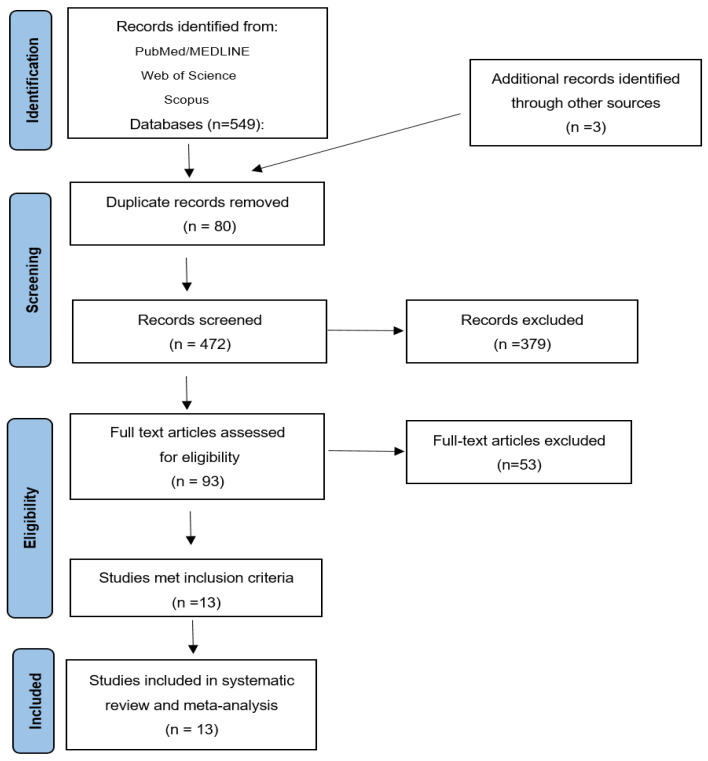 Figure 1
Figure 1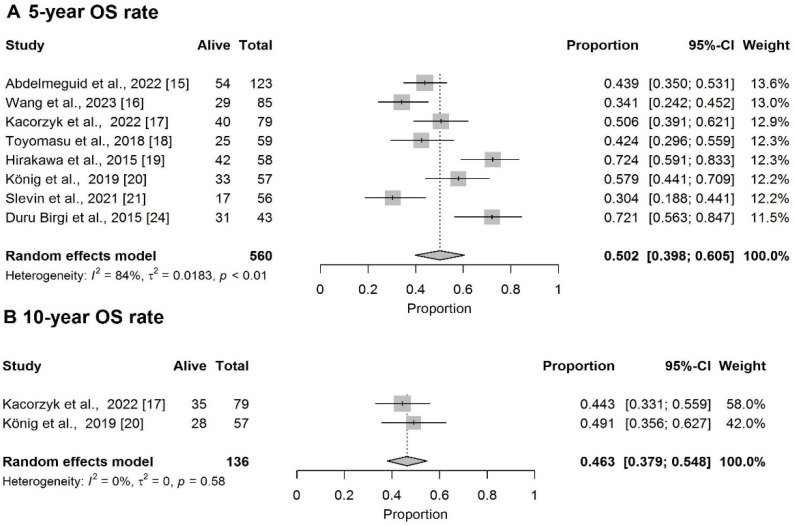 Figure 2
Figure 2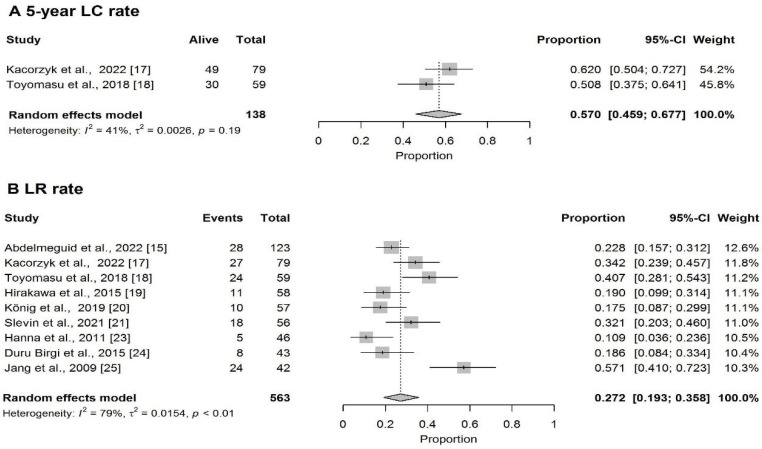 Figure 3
Figure 3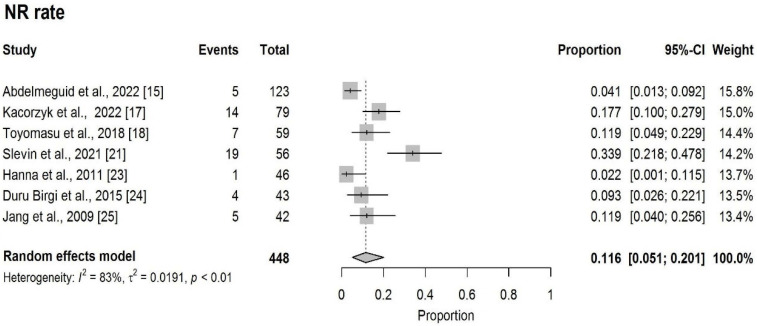 Figure 4
Figure 4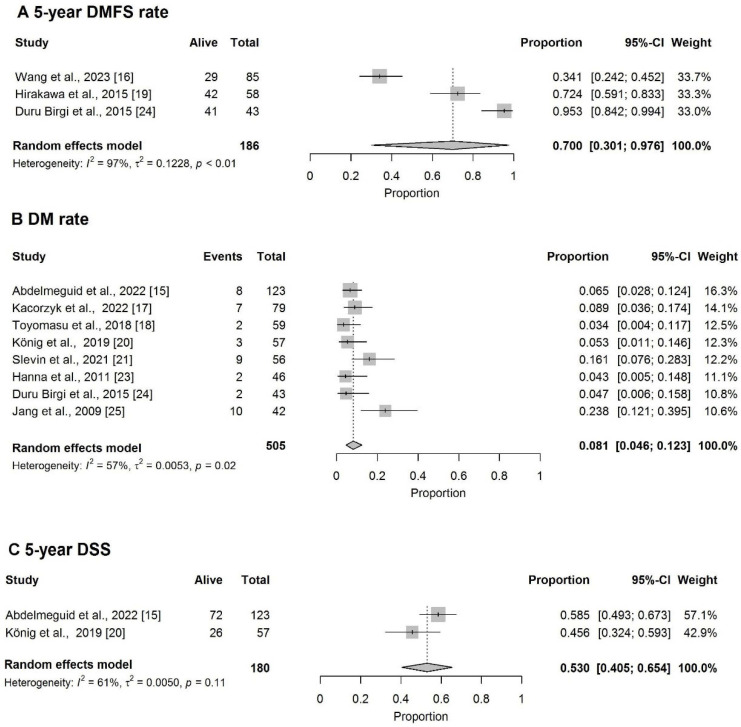 Figure 5
Figure 5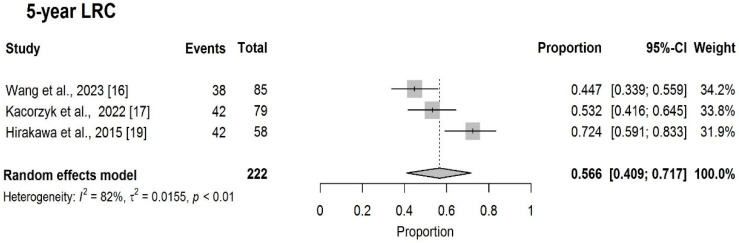 Figure 6
Figure 6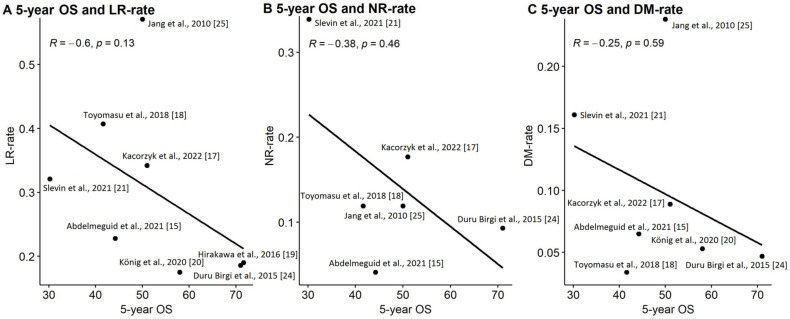 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHead and Neck Surgical Oncology · Sinusitis and nasal conditions · Salivary Gland Tumors Diagnosis and Treatment
1. Introduction
Sinonasal squamous cell carcinoma (SNSCC) is the most common histopathological subtype of malignant tumors of the sinonasal region.
Despite advances in treatment techniques and improvements in surgical and radiotherapy procedures, the prognosis for this patient group remains poor mainly for local failure [1,2,3,4]. The rarity of SNSCC and its heterogeneity as to primary locations and varying clinical stages mean that most of the existing studies are based on the experience of individual centers with a small group size. Because of this, the results of SNSCC treatment have also been summarized in few systemic reviews and meta-analyses [2,5,6], population-based comparisons [3,7,8], or comprehensive comparative analyses [9]. All of them, however, refer to data from before 2020, concentrate on a selected site of the sinonasal region [5,6] or assess mixed histopathological subtypes [3,7,8,9].
In this meta-analysis, we evaluated patterns of treatment failure—local recurrence (LR), nodal recurrence (NR), and distant metastasis (DM)—and their relationship with overall survival (OS), collating all patients with SNSCC of all sites in the sinonasal region.
2. Material and Methods
This study was conducted in accordance with the PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies that Evaluate Health Care Interventions, issued in 2009 [10]. The systematic review was not registered. This systematic review and meta-analysis investigated overall survival (OS) at 2, 3, 5, and 10 years, as well as 5-year local control (LC), local recurrence (LR) rate, nodal recurrence (NR) rate, and 5-year distant metastasis-free survival (DMFS), distant metastasis (DM) rate, and 5-year disease-specific survival (DSS) in radically treated SNSCC patients.
2.1. Literature Search Strategy
A systematic search was conducted in MEDLINE (PubMed), Scopus and Web of Science databases for studies published up to 30 November, 2025. The search included the following core terms: ‘Cancer of maxilla and sinonasal region’, ‘Sinonasal malignancy’, ‘Neoplasms of the maxillo-ethmoid massif’, ‘Maxillary sinus squamous cell carcinoma’, ‘Cancer of nasal cavity and paranasal sinuses’, ‘Sinonasal cancer’, ‘Paranasal sinuses malignancies’, ‘Nasal and paranasal sinus carcinoma’, ‘Malignant tumors of the nasal cavity, ethmoid and sphenoid sinuses’, ‘Malignant neoplasms of the sinonasal tract’, ‘paranasal sinus neoplasms, ‘maxillary sinus neoplasms’, ‘ethmoid sinus neoplasms’, ‘sphenoid sinus neoplasms’, ‘frontal sinus neoplasms’, ‘surgery’, ‘radiotherapy’, ‘radical treatment’, and ‘definitive treatment’. Detailed search strategies are presented in Supplementary Materials S1 (Tables S1–S4).
2.2. Eligibility Criteria
Studies were included if they met the following criteria: (1) patients aged ≥18 years (single cases of children were allowed), (2) patients diagnosed with SNSCC, (3) patients who underwent radical treatment (surgery or radiotherapy), (4) studies with a sample size of ≥15 patients, (5) studies reporting at least one of the following endpoints (OS, LC, nodal control (NC), DM, DSS, LR rate, NR rate, DM rate). Studies were excluded if they (1) included only pediatric patients (<18 years), (2) were not published in English, (3) were reviews, meta-analyses, case reports, or conference abstracts, (4) were published before 1 January 2000, (5) used data from the Surveillance, Epidemiology, and End Results (SEER) database or other national databases, or (6) were multi-center studies containing data from different countries.
2.3. Data Selection and Extraction
Two independent investigators (A.J.C. and A.K.) conducted the literature search based on both restrictive (quotation-based) and liberal approaches (without quotation marks) (Supplementary File S1 (Tables S1–S4)). Articles were collected in the data management software EndNote X7 (Clarivate Analytics (US) LLC, Philadelphia, PA, USA) (A.J.C.) and Mendeley Reference Manager v. 2.77.0 (Elsevier, Amsterdam, The Netherlands) (A.K.). Publication databases were combined and duplicates were removed using R environment (R Foundation for Statistical Computing, Vienna, Austria, http://www.r-project.org). The titles and abstracts of the remaining studies were independently screened by U.K. and M.S.-C. based on the inclusion and exclusion criteria using the retools package (v. 0.4.1) [11]. Full texts of eligible studies were further screened by U.K. and M.S.-C. Disagreements were adjudicated by T.R. Outcome data included OS, LC, NC, DM, and DSS at 2, 3, 5, and 10 years, as well as LR rate, NR rate and DM rate.
2.4. Risk of Bias
The risk of bias was independently assessed by two authors (U.K. and M.Sz.-C) using Cochrane’s Risk of Bias in Non-Randomized Studies of Interventions (ROBINS-I) tool [12]. Each bias domain in non-randomized studies was classified as “low”, “moderate”, “serious,” or “critical” risk. The following seven domains were evaluated: “confounding”, “selection of participants”, “classification of interventions”, “deviations from intended interventions”, “missing data”, “measurement of outcomes”, and “selection of reported result”. The risk of bias was visualized with the Risk-of-bias VISualization (robvis) tool [13].
2.5. Statistical Analysis
Proportional meta-analysis was used to obtain pooled effect estimates, expressed as OS, LC, DMFS, DSS, LR rate, NR rate and DM rate. The number of events (failures) and the number of surviving patients at 2, 3, 5, and 10 years were calculated as percentages multiplied by sample size. Forest plots with a 95% confidence interval (CI) were generated and visualized. The random-effects model with double arcsine transformation (Freeman–Tukey transformation) was used. The level of heterogeneity across studies was evaluated with the Cochrane Q test and I2 statistics. Heterogeneity was considered low if I2 < 30%, moderate if I2 30–75%, and high if I2 > 75% [14]. Significant heterogeneity was indicated by p < 0.05 in the Cochrane Q test. Spearman correlation coefficients were classified as follows: 0.0 ≤ |r| < 0.1 (negligible correlation), 0.1 ≤ |r| ≤ 0.39 (weak correlation), 0.4 ≤ |r| ≤ 0.69 (moderate correlation), 0.7 ≤ |r| ≤ 0.89 (strong correlation), and 0.9 ≤ r ≤ 1 (very strong correlation). All computational analyses were performed in the R environment for statistical computing (version 4.1.1 released on 10 August 2021; R Foundation for Statistical Computing, Vienna, Austria, http://www.r-project.org) (Accessed on 9 March 2026).
3. Results
3.1. Study Selection and Characteristics
A search strategy yielded 549 articles from PubMed/MEDLINE, Web of Science and Scopus, with an additional 3 articles identified through other sources. After excluding 80 duplicate records, 472 articles were screened based on titles and abstracts. Ninety-three articles were fully reviewed. A total of 13 studies fulfilled the eligibility criteria and were included in the final meta-analysis (Figure 1). These selected studies comprised a total of 749 patients, with sample sizes ranging from 18 to 123 patients per article [15,16,17,18,19,20,21,22,23,24,25,26,27]. The studies were conducted in Europe [17,20,21,24], North America [15,23], or Asia [16,18,19,25,26,27]. All studies were published between 2009 and 2023. Patients were diagnosed between 1988 and 2017, with a median follow-up of 36 months [IQR: 32.5–43] [15,16,17,18,19,20,21,22,23,24,25,26,27]. The median age of patients was 60 years [IQR: 59–60]. Key information, including authors, year of publication, country, sample size, patient characteristics, details of histopathological subtype, median follow-up, and outcomes, is presented in Table 1.
Among a subgroup of 646 patients with sufficient data, the distribution across T stages was as follows: T1—2%, T2—5.4%, T3—14%, and T4—78.6%. Nodal involvement (N+) was reported in 22.8% of patients. All patients in the cohort received radical treatment.
Multimodal treatment (at least two methods of surgery, RT, CHRT, iCH) was administered in 588 cases (78%), while single-modality treatment was used in 161 cases (22%). Across the entire cohort, 356 patients (47.5%) were treated with surgery followed by adjuvant RT or CHRT. CHRT or RT instead of surgery was used in 393 patients (52.5%). Particle beam radiation therapy (PT) or carbon ion therapy (CIT) were used in 65 (9%) and 21(3%) patients, respectively. Induction chemotherapy was administered in 300 cases (40%). Of these, 156 patients (52%) received iCH prior to surgery, and 144 patients (48%) received it prior to RT or CHRT (Table 1).
3.2. Overall Survival
The pooled 2-year and 3-year OS rates were 74% (95%CI: 63.5–83.0%) and 51.7% (95%CI: 40.8–62.4%), respectively (Supplementary Materials S1, Figures S1 and S2). The pooled 5-year and 10-year OS rates were 50.2% (95%CI: 39.8–60.5%) and 46.3% (95%CI: 37.9–54.8%) (Figure 2A,B).
3.3. Local Control
The pooled 5-year LC rate was 57% (95%CI: 45.9–67.7%) (Figure 3A) and the pooled LR rate was 27.2% (95%CI: 19.3–35.8%) (Figure 3B).
3.4. Nodal Control
The pooled NR rate was 11.6% (95%CI: 5.1–20.1%) (Figure 4).
3.5. Distant Metastases
The pooled 5-year DMFS rate was 70.0% (95%CI: 30.1–97.6%) (Figure 5A) and the pooled DM rate was 8.1% (95%CI: 4.6–12.3%) (Figure 5B). The pooled 5-year DSS rate was 53% (95%CI: 40.5–65.4%) (Figure 5C).
The pooled 5-year LRC was 56.6% (95%CI: 40.9–71.7%) (Figure 6).
There is no statistically significant correlation between 5-year OS and LR-rate (R = −0.6, p = 0.13), NR-rate (R = −0.38, p = 0.46) and DM- rate (R = −0.25, p = 0.59) (Figure 7).
3.6. Assessment of Bias Risk
The summary of the risk of bias is presented in Supplementary Materials S1. Authors’ assessments of each domain for all included studies are shown in Supplementary Materials S1, Figures S3 and S4. Overall, the included studies exhibited a low or moderate risk of bias.
4. Discussion
SNSCC includes about 60% of cancers arising in the sinonasal region and is the most common cancer subtype in this region [1]. Despite this, treatment recommendations are based mostly on meta-analyses and population-based studies and no randomized clinical trial has been published on this group of patients. In general, for patients with SNSCC, the 5-year OS is about 50% [1]. In our report, the 5-year OS for SNSCC patients was 50.2% and is similar to other authors, who report results between 53% and 57% [2,6,7,9,28]. Each of these meta-analyses present a wide range of results which depend on various clinical factors and treatment methods. In our study, the range of 5-year OS was between 30.4% and 72.4%. Slieker et al. showed 5-year OS rates between 25% and 82.2% for 19 studies and almost 1500 patients with SCC of the maxilla [6]. Dutta et al. also observed a wide range of treatment outcomes according to tumor localization in the sinonasal tract, with a 5-year OS of 30.2% for sphenoid sinus to 74.5% for the nasal cavity [7]. Nguyen reported a 5-year OS between 48.8% and 69.9% depending on treatment method and between 44.3% and 68.9% according to stage of disease [2].
Local recurrence (LR) is the main reason for treatment failure [4,9,29,30]. Considering the relatively low risk of nodal and distant spread of this cancer (10–15%), the achievement of local control is crucial for ultimate treatment success. Although LR and NR are often combined under the term locoregional recurrence, LR predominates, occurring in approximately 30–80% of cases depending on stage of disease and treatment modality, among other factors [29,31,32,33,34,35,36,37,38]. Our data indicated a 5-year LC rate of 57% with an LR incidence of 27.2% (range: 10.9–57.1%). Nguyen et al. reported a 5-year recurrence rate (RR) of 20.5% and a locoregional control rate of 67.1%, with an overall relapse rate (including local, regional, and distant recurrences) of 42.7% [2]. Slieker et al. reported a 5-year LR rate of 19.4% (range: 9–46.8%) for maxillary SCC [6].
According to Dooley et al., the risk of regional spread is highest for SCC followed by other histopathological subtypes like adenocarcinoma (AC), sinonasal undifferentiated carcinoma (SNUC), and adenoid cystic carcinoma (ACC), occurring in 28%, 25%, 12%, and 10% of cases, respectively [31]. Ranasinghe et al. found an overall nodal spread risk of 13.2% for SCC across all subsites, rising to 19.3% in sinus locations compared to 7.9% for the nasal cavity [39]. Our study confirmed a relatively low overall NR rate of 11.6%. Nevertheless, regional relapses are associated with significantly worse prognosis in SNSCC patients [8,40]. In fact, patients with NR often succumb to subsequent distant metastases or combined progression of local disease [8,41]. Distant metastasis is relatively uncommon for SNSCC patients, occurring in 3–20% of cases [3,9,29]. Based on our meta-analysis, the average DM risk for SNSCC patients was 8.1%. Liu et al. categorized patients with sinonasal carcinoma by their risk of distant failure, placing SNSCC alongside AC and esthesioneuroblastoma (ENB) in the low-risk group (risk of distant spread <25%), in contrast to sinonasal neuroendocrine carcinoma (SNEC), mucosal melanoma (MM), and soft tissue sarcoma (STS), which were classified as high-risk (>25%) [42]. Data from single centers indicates that patients with local or locoregional failure present significantly worse outcomes [17,43]; however, such a correlation reported from meta-analyses is less direct.
Consequently, we tried to assess how LR, NR and DM may influence OS. No correlation between these parameters was found. Similar results were obtained by Kaplan et al., who found in the studied group that DM and LR have no impact on OS; however, only 45% of patients in their study group were diagnosed with SNSCC [44]. Our observation may be due to the heterogeneity of our group, which takes into account all sites in the sinonasal region, which differ according to treatment effectiveness, most common stage of local advancement of disease or the risk of nodal spread. Primary tumor location and the probability of infiltration of nearby critical anatomical structures, like the skull base, are certainly related to the risk of treatment failure. It has also been found that the maxillary sinus is associated with a higher risk of LR than other subsites [2,45]. Also, the primary site of the tumor may influence NR with a higher risk for maxilla than ethmoid sinus infiltration. These factors influence the probability of obtaining clear resection margins (R0), detecting recurrence early or salvage effectiveness.
Recurrence diagnosed with nasal endoscopy has a higher probability of salvage surgery (SS) success than tumors diagnosed with imaging alone [46]. Salvage surgery for tumor localization in the nasal cavity or ethmoid sinuses showed better 5-OS than tumors arising in the maxillary, frontal sinuses or orbital and clivus infiltration [30,44,47].
While direct evidence linking early detection of recurrence to improved OS is lacking, for patients with SNSCC, salvage therapy is feasible in 50–70% of patients with LR and is successful in approximately 33% of cases undergoing such treatment [17,30]. The longer the time to primary treatment failure, the more effective the salvage [48]. Surgery is considered as the most effective means of salvaging but RT may also be used with good results. Kacorzyk et al. indicated 43% and 25% permanent cure after salvage surgery or RT, respectively [17]. Due to the data indicating promising results in terms of salvage for SNSCC, we also tried to analyze disease-specific survival (DSS) in this meta-analysis (Figure 5). Disease-specific survival refers to the proportion of patients who have not died from their cancer within a defined period after treatment, even despite their tumor not being cured. This parameter seems to be useful in patients with prolonged clinical disease course. The consequences of salvage may prolong clinical course of SNSCC and could be potentially seen in longer DSS. Pecorari et al.’s study indicated significantly higher DSS than OS, suggesting that patients suffering from SNSCC do not die as often because of cancer [48]. A comparison of 5-year OS and 5-year DSS for SNSCC indicates that the gap between OS and DSS is in the range of 10–40% [15,20,48,49,50]. It depends on several clinical factors including primary site of tumor, local and nodal stage of disease or treatment approach [51,52]. We found a 5-year DSS of 53% (Figure 5), which is slightly higher compared to the 50.2% 5-year OS in this group of patients Dutta et al. also reported a 5-year DSS of 52.3% in the group of 11,000 patients with SNSCC, but with no relation to OS but to relative survival (RS) [7]. Relative survival (RS) reflects the ratio between the observed survival rate and the expected survival rate in the comparable general population (matched by age, sex, or other factor). Because most survival data from patients with SNSCC comes from population-based studies where the actual cause of death is not known, RS is also commonly reported for SNSCC as an approach to DSS [48,53,54]. The RS-OS gap is in the range of 4–11% [52,53,54]. The difference between the DSS-OS gap and RS-OS gap is probably due to the fact that these two parameters rely on different assumptions: accurate determination of cause of death and adjustment of background mortality for DSS and RS, respectively. Nevertheless, higher DSS may reflect, among others, the influence of salvage on survival.
Salvage therapy for SNSCC may provide durable control in a subset of selected patients, particularly when complete resection (R0) is achievable and the optimal selection of patients for salvage seems to be pivotal for the success of the procedure, which must always maintain a balance between the chance (cure) and the risk (complications). There is not much data defining potential prognostic factors for recurrence. Kaplan et al. reported primary tumor site, histology, perineural invasion (PNI), and infiltration of carotic artery or clivus as factors significantly reducing salvage effectiveness [44]. Mattavelli et al. suggested scoring based on, among others, the type of primary treatment, histology, adjuvant treatment and postoperative histopathological results in terms of margin status and PNI [32].
5. Limitations
Several factors limit the strength of our conclusions. Some studies included small patient groups, while others covered long recruitment periods during which diagnostic and treatment standards evolved.
Due to the rarity of SNSCC, treatment decisions are often based on institutional experience rather than universally accepted guidelines, reducing the generalizability of findings. To mitigate these limitations, we applied strict selection criteria, although this reduced the number of included studies. Additionally, treatment outcomes depend on multiple variables, including tumor site, T and N stage, and treatment modality. A detailed analysis of these factors would enable a more individualized assessment of prognosis and treatment success.
Not all included studies reported LR, NR, and DM together with OS, which substantially reduced the number of datasets available for correlation analysis. In addition, the pooled studies were heterogeneous with respect to primary tumor site, stage distribution, nodal status, and treatment strategies, and most series were small single-institution cohorts. The included series differed substantially in primary tumor site distribution, with some studies restricted to specific subsites (e.g., maxillary sinus) and others including mixed sinonasal locations. This heterogeneity likely reflects institutional case selection and may influence pooled survival and control estimates.
The correlation analysis between LR and OS should be interpreted with caution, as the number of studies reporting both endpoints was limited, and the impact of salvage treatment on ultimate survival could not be consistently evaluated.
These factors likely reduced statistical power, may have obscured true associations between recurrence patterns and survival, and reflect the intrinsic heterogeneity of sinonasal malignancies and the challenges of conducting homogeneous meta-analyses in this rare disease setting. This heterogeneity is inherent to sinonasal malignancies and limits the interpretability of pooled estimates and correlation analyses.
Despite these limitations, this study provides a current assessment of primary treatment outcomes and highlights the potential effectiveness of salvage treatment in a selected group of patients.
6. Conclusions
SNSCC remains an aggressive disease with an approximately 50% 5-year OS rate in contemporary series. LR was the main reason for treatment failure, with an LR rate 27%. The pooled DM and NR rates were 8.1% and 11.6%, respectively. These findings confirm the dominant role of local failure in SNSCC and highlight the need for improved local control strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Thawani R. Kim M.S. Arastu A. Feng Z. West M.T. Taflin N.F. Chandra R.A. The contemporary management of cancers of the sinonasal tract in adults CA Cancer J. Clin.2023737211210.3322/caac.2175235916666 PMC 9840681 · doi ↗ · pubmed ↗
- 2Nguyen E.S. Risbud A. Birkenbeuel J.L. Murphy L.S. Goshtasbi K. Pang J.C. Kuan E.C. Prognostic Factors and Outcomes of De Novo Sinonasal Squamous Cell Carcinoma: A Systematic Review and Meta-analysis Otolaryngol. Head Neck Surg.202216643444310.1177/0194599821102102334253092 · doi ↗ · pubmed ↗
- 3Turner J.H. Reh D.D. Incidence and survival in patients with sinonasal cancer: A historical analysis of population-based data Head Neck 20123487788510.1002/hed.2183022127982 · doi ↗ · pubmed ↗
- 4Ferrari M. Taboni S. Carobbio A.L.C. Emanuelli E. Maroldi R. Bossi P. Nicolai P. Sinonasal Squamous Cell Carcinoma, a Narrative Reappraisal of the Current Evidence Cancers 202113283510.3390/cancers 1311283534200193 PMC 8201377 · doi ↗ · pubmed ↗
- 5Scurry W.C. Goldenberg D. Chee M.Y. Lengerich E.J. Liu Y. Fedok F.G. Regional Recurrence of Squamous Cell Carcinoma of the Nasal Cavity: A Systematic Review and Meta-Analysis Arch. Otolaryngol. Head Neck Surg.200713379680010.1001/archotol.133.8.79617709619 · doi ↗ · pubmed ↗
- 6Slieker F.J.B. Rombout D.A.A. de Bree R. Van Cann E.M. Local recurrence and survival after treatment of oral squamous cell carcinoma of the maxilla: A systematic review and meta-analysis Oral Surg. Oral Med. Oral Pathol. Oral Radiol.202213362663810.1016/j.oooo.2021.10.00335165055 · doi ↗ · pubmed ↗
- 7Dutta R. Dubal P.M. Svider P.F. Liu J.K. Baredes S. Eloy J.A. Sinonasal malignancies: A population-based analysis of site-specific incidence and survival Laryngoscope 20151252491249710.1002/lary.2546526228792 · doi ↗ · pubmed ↗
- 8Unsal A.A. KılıçS. Dubal P.M. Baredes S. Eloy J.A. EUROCARE-5 Working Group. A population-based comparison of European and North American sinonasal cancer survival Auris Nasus Larynx 20184581582410.1016/j.anl.2017.09.00929056464 · doi ↗ · pubmed ↗