A Comprehensive Analysis of Therapeutic Potential of Medicinal Plant Extracts to Treat Ethanol-Induced Gastric Ulcer
Raja Singh Paulraj, Anbazhagan Sathiyaseelan, Parthasarathi Perumal, Arunkumar Ramachandran, Shanthi Grace Paulraj

TL;DR
This paper reviews how medicinal plant extracts can help treat gastric ulcers caused by alcohol, offering safer and effective natural alternatives.
Contribution
The paper provides a comprehensive review of medicinal plants with anti-ulcer properties, focusing on their mechanisms and therapeutic potential.
Findings
Medicinal plant extracts show gastroprotective effects through antioxidant activity and anti-inflammatory mechanisms.
Herbal remedies enhance mucosal defense and inhibit gastric acid secretion in experimental ulcer models.
Plant-based therapies offer promising alternative treatment strategies for peptic ulcer management.
Abstract
Background/Objectives: Gastric ulcer is a prevalent global gastrointestinal disorder influenced by multiple factors, including excessive alcohol consumption, poor dietary habits, psychological stress, smoking, and the chronic use of non-steroidal anti-inflammatory drugs. Among these, alcohol plays a critical role in gastric mucosal injury by enhancing gastric acid secretion, triggering inflammatory responses, inducing oxidative stress, and promoting epithelial cell apoptosis while simultaneously depleting key protective mediators such as nitric oxide and prostaglandin E2. Growing interest has focused on medicinal plants as promising sources of novel therapeutic agents for the management of peptic ulcer disease. Methods: This review summarizes commonly used medicinal plants documented in both Ayurvedic and modern medical systems that exhibit ulcer-healing potential. Experimental and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
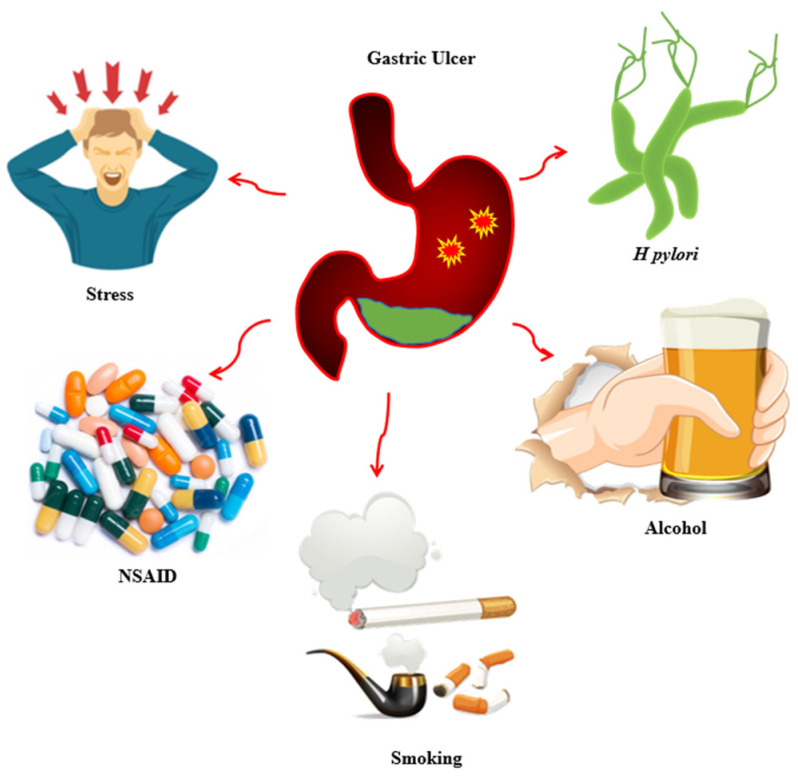 Figure 1
Figure 1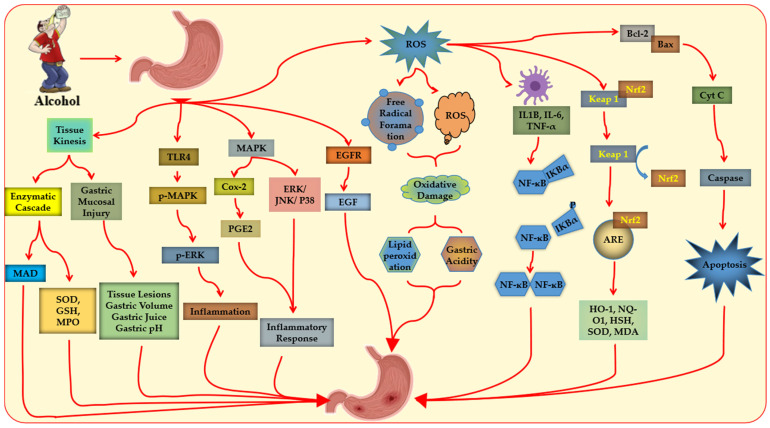 Figure 2
Figure 2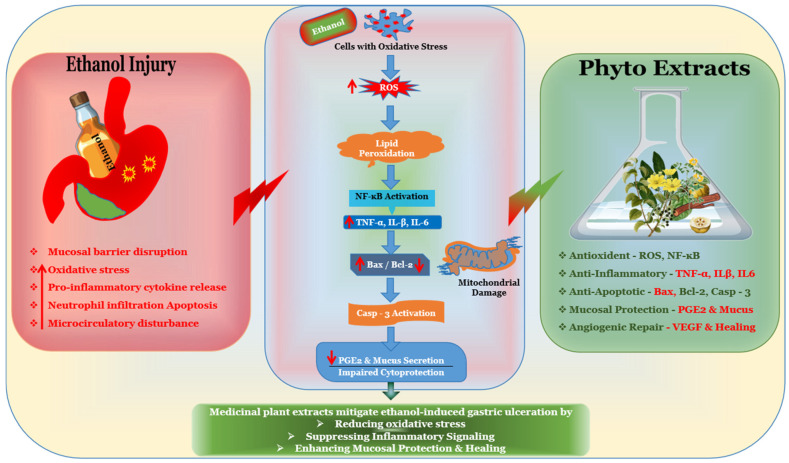 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHelicobacter pylori-related gastroenterology studies · Natural Products and Biological Research · Phytochemistry and biological activities of Ficus species
1. Introduction
Peptic ulcer (PU) has long been a major cause of gastrointestinal surgery, with high morbidity and mortality, and has been referred to as the “new plague of the 21st century”. Since 1990, peptic ulcer has accounted for 4404 deaths globally. However, age-standardized rates of prevalence, incidence, and mortality have declined significantly. Autoregressive integrated moving average (ARIMA) models predict that, despite an initial rise in cases, the overall burden will continue to decrease by 2050, reflecting improvements in management and preventive strategies [1,2,3].
PUs are mucosal lesions that extend beyond the muscularis mucosae, forming a cavity encircled by inflammation. They are primarily categorized into gastric ulcers and duodenal ulcers based on their location [2]. PU is a prevalent gastrointestinal illness, affecting a substantial proportion of individuals worldwide, with higher prevalence reported in developing countries. Major contributing factors include the misuse of non-steroidal anti-inflammatory drugs (NSAIDs) and infections with Helicobacter pylori (H. pylori) [4,5,6,7]. Additional risk factors comprise physical and psychological stress, environmental pollutants, pesticides, heavy metals, and tobacco and alcohol use [8,9,10,11].
The development of a gastric ulcer is multifactorial, resulting from an imbalance between aggressive factors—such as gastric acid, pepsin, ethanol exposure, NSAIDs, and H. pylori—and mucosal defensive mechanisms [3,4,12,13,14]. Protective mechanisms include mucus and bicarbonate secretion, prostaglandin synthesis, adequate mucosal blood flow, and antioxidant systems. These factors ultimately converge through shared pathophysiological pathways involving oxidative stress, inflammatory signaling, and disruption of the epithelial barrier [3,12,15].
Current pharmacological management of PU primarily includes proton pump inhibitors, H2 receptor antagonists, antacids, and antibiotic regimens for H. pylori eradication. Although these therapies are effective, long-term use is associated with adverse effects, recurrence, drug resistance, and incomplete mucosal healing in some patients. These limitations have stimulated increasing interest in alternative and complementary therapeutic approaches, particularly plant-derived bioactive compounds with antioxidant, anti-inflammatory, and cytoprotective properties [3,12,13,16,17].
Experimental models play a critical role in understanding gastric ulcer pathogenesis and screening potential therapeutic agents. Among these, the ethanol-induced gastric ulcer model is widely employed due to its reproducibility and ability to rapidly induce mucosal damage through oxidative stress, inflammation, lipid peroxidation, and epithelial necrosis. This model closely mimics acute gastric mucosal injury and allows systematic evaluation of gastroprotective mechanisms of medicinal plant extracts [15,18,19,20,21].
Although numerous studies have reported the gastroprotective effects of individual medicinal plants in ethanol-induced ulcer models, the available evidence remains fragmented and mechanistically dispersed across experimental studies. A comprehensive synthesis focusing specifically on the molecular pathways, phytochemical classes, and translational relevance of plant extracts evaluated in ethanol-induced gastric ulcer models is currently lacking. Understanding these mechanisms not only clarifies the actions of bioactive compounds but also guides future translational research in anti-ulcer therapy [15,18,21].
Therefore, this review aims to critically summarize and integrate recent experimental findings on medicinal plant extracts tested in ethanol-induced gastric ulcer models, with particular emphasis on their antioxidant, anti-inflammatory, and cytoprotective mechanisms.
2. Selection of Medicinal Plant Extracts
Although this review is narrative in nature, a structured and transparent approach was adopted to identify relevant medicinal plant extracts for inclusion. A comprehensive literature search was conducted using the PubMed, Scopus, and Google Scholar databases to identify experimental studies published between 2001 and 2025 that evaluated plant-derived extracts in ethanol-induced gastric ulcer models. The search strategy included combinations of the following keywords: (“ethanol-induced gastric ulcer” OR “alcohol-induced gastric injury”) and (“medicinal plant” OR “plant extract” OR “phytotherapy” OR “natural compound”). Only articles published in English were considered.
Studies were included if they (i) employed in vivo ethanol-induced gastric ulcer models, (ii) investigated plant-derived extracts or isolated phytochemicals, and (iii) reported quantitative outcomes such as ulcer index, histopathological findings, or mechanistic biomarkers (e.g., antioxidant or inflammatory parameters). Exclusion criteria encompassed review articles, clinical-only studies, studies without clearly described experimental design, or those not directly relevant to ethanol-induced gastric injury.
To enhance transparency and minimize bias, data extraction and standardization were conducted systematically, with doses expressed in mg/kg body weight, ethanol concentrations in % (v/v), and exposure times in a uniform format. This approach ensured consistency across studies while maintaining the narrative scope of the review.
3. Methodological Limitations
While a structured and transparent approach was applied, several limitations should be considered. Restricting inclusion to English-language publications may introduce language bias, and searching only PubMed, Scopus, and Google Scholar could have missed relevant studies in other databases. The included studies exhibited heterogeneity in animal species, extract preparation, doses, and exposure times, which may affect direct comparability. As a narrative review, this study does not provide pooled effect estimates, and publication bias cannot be fully excluded. Finally, while efforts were made to standardize data presentation, inherent variability across experimental protocols may influence the interpretation of results.
4. Pathways of Gastric Ulcer Pathogenesis
Gastric ulcer disease is a multifactorial disorder resulting from an imbalance between aggressive factors and mucosal defense mechanisms. As illustrated in Figure 1, gastric mucosal injury may be triggered by microbial infection, prolonged exposure to ulcerogenic drugs, psychological and physical stress, and lifestyle-related factors, each operating through distinct pathogenic pathways. Well-established etiological factors include smoking [22], NSAID use [4], H. pylori infection [23], alcohol consumption [24], and stress [25]. These factors contribute to mucosal injury through mechanisms such as suppression of prostaglandin synthesis, increased gastric acid secretion, oxidative stress, inflammatory cytokine release, and neuroendocrine dysregulation [14,26,27].
Although these pathways are important for general gastric ulcer pathogenesis, ethanol-induced gastric injury involves a distinct mechanism characterized by direct mucosal damage, microvascular impairment, oxidative stress, and activation of inflammatory mediators. Therefore, this review specifically focuses on ethanol-induced gastric ulcer models to evaluate the gastroprotective potential of medicinal plant extracts within this well-established experimental framework.
5. Ethanol-Induced Ulcer
The ethanol-induced gastric ulcer model involves direct mucosal damage caused by excessive ethanol, resulting in hemorrhages, cellular exfoliation, inflammation, and mucosal edema [20,26,27,28]. Ethanol easily penetrates the gastric mucosa, exposing it to acidic conditions and pepsin, which damage the epithelial membrane. It also reduces gastric blood flow, disrupts vascular endothelium, and increases xanthine oxidase activity, thereby promoting oxidative stress and microvascular injury [12,29,30,31].
During ethanol metabolism, alcohol dehydrogenase converts ethanol to acetaldehyde, which xanthine oxidase can further convert to reactive oxygen species (ROS). Free radicals generated in this process decrease mucus and bicarbonate secretion, increase lipid peroxidation (LPO), and damage capillary and endothelial cells, leading to necrosis, bleeding, and epithelial erosion [3,18,32]. Vasoactive mediators such as leukotriene C4, endothelin-1, and histamine increase vascular permeability, worsening mucosal injury. Neutrophil infiltration further amplifies ROS production, damaging lipids, proteins, and other cellular components [33,34,35].
The molecular mechanisms of ethanol-induced gastric ulcer, involving oxidative stress, inflammation, and apoptosis, are illustrated in Figure 2. Activated neutrophils increase myeloperoxidase (MPO) activity and nuclear factor kappa B (NF-κB)-mediated production of pro-inflammatory cytokines such as TNF-α, exacerbating mucosal injury [36,37,38,39,40]. Ethanol exposure reduces levels of anti-inflammatory cytokines (e.g., IL-10) and depletes endogenous antioxidants, including total antioxidant capacity (TAC), glutathione (GSH), and glutathione peroxidase (GPx), while increasing lipid peroxidation. Additionally, ethanol lowers cytoprotective molecules such as nitric oxide (NO) and Prostaglandin E_2_ (PGE_2_), further compromising mucosal integrity [36,38,41,42,43].
6. Current Pharmacological Management
Currently, gastric ulcers are managed using pharmacological agents that provide mucosal protection and reduce gastric acidity. Triple therapy, consisting of two antibiotics and a proton pump inhibitor, is standard for H. pylori-associated peptic ulcers, whereas acid-suppressive and cytoprotective treatments are applied for ethanol-induced ulcers [44,45]. Omeprazole, a widely used proton pump inhibitor, reduces acid secretion but is associated with side effects, highlighting the need for safer therapeutic options [46,47,48].
7. Phytotherapy Treatment for Ethanol-Induced Gastric Ulcer
Phytotherapy—the use of medicinal plants to treat illnesses—has been employed since ancient times [47]. Plant-derived bioactive compounds, or phytochemicals, are concentrated in roots, bark, leaves, seeds, and fruits. These compounds exhibit anti-inflammatory, antioxidant, cytoprotective, and anti-secretory activities, making them valuable candidates for gastroprotective therapy [48,49,50,51,52].
In ethanol-induced gastric ulcer models, phytochemicals mitigate mucosal injury by restoring antioxidant balance, reducing ROS, modulating inflammatory pathways, and promoting tissue regeneration. Key classes include alkaloids, which regulate gastric acid secretion and provide cytoprotection [48]; Flavonoids, which accelerate ulcer healing through anti-inflammatory and antioxidant effects [49]; and essential oils and polyphenols, which protect the mucosa and exhibit anti-secretory and anti-inflammatory activities [50].
The imbalance between defensive mechanisms (mucus, PG synthesis, endothelial blood flow) and aggressive factors (acid, pepsin, ethanol, H. pylori) underlies ethanol-induced gastric ulcer [53]. Ethanol exacerbates mucosal damage via its hydrolytic and proteolytic effects while decreasing blood flow, increasing ROS, and elevating pro-inflammatory cytokines [8,26,53,54,55,56,57,58].
Herbal extracts demonstrate significant gastroprotective effects due to their high phytochemical content, antioxidant activity, and anti-inflammatory properties [59]. These extracts provide a complementary approach to conventional therapy, particularly in ethanol-induced gastric ulcers, where H. pylori-targeted quadruple therapy is not indicated. Screening for high-efficacy, low-toxicity phytochemicals is therefore essential to enhance patient outcomes and reduce reliance on drugs with adverse effects [47,60,61,62,63].
8. Phytotherapy-Focused Discussion
Herbal extracts are effective in treating stomach ulcers due to their high phyto-chemical content and their anti-inflammatory and antioxidant properties, as summarized in Table 1. The main treatment strategies include healing the gastric mucous membrane, managing pathogens, and reducing acid secretion [49]. Quadruple therapy (a proton pump inhibitor, bismuth, and two antibiotics) is used for H. pylori-related gastric ulcers, whereas ethanol-induced ulcers are managed with acid-suppressive and cytoprotective treatments [50]. The limitations of quadruple therapy, including high relapse rates, side effects, and pathogen resistance, have led to a greater need for new treatment options [51]. Modern medical research indicates that phytomedicine offers low toxicity and multiple targeting effects, making it suitable for integration with quadruple therapy in the treatment of gastric ulcers [16,52,53]. As a result, screening phytomedicine for high-efficiency and low-toxicity monomers is crucial for improving the quality of life of gastric ulcer patients and increasing the efficacy of treatment.
9. Integrative Mechanistic Perspective on Ethanol-Induced Anti-Ulcer Phytotherapeutics
Despite extensive phytochemical diversity, the evaluated plant-derived interventions converge into five principal gastroprotective pathways: (i) enhancement of mucus production and reinforcement of mucosal barrier integrity; (ii) antioxidant-mediated cytoprotection through attenuation of lipid peroxidation and restoration of endogenous enzymatic defenses (SOD, CAT, GSH); (iii) anti-secretory activity involving suppression of gastric acidity and inhibition of H^+^/K^+^-ATPase; (iv) anti-inflammatory modulation characterized by downregulation of TNF-α, NF-κB, COX-2, and related mediators; and (v) NO and PGE_2_-dependent cytoprotective signaling.
Across experimental models of ethanol-induced gastric injury, mucosal reinforcement and attenuation of oxidative stress emerge as the most consistently reported protective mechanisms. Restoration of endogenous antioxidant systems frequently parallels reductions in MDA, a marker of lipid peroxidation, indicating coordinated suppression of oxidative damage rather than isolated biochemical modulation. Importantly, antioxidant recovery often coincides with diminished inflammatory signaling, suggesting functional interplay between redox homeostasis and NF-κB-mediated cytokine regulation.
Anti-secretory mechanisms, although less universally documented, demonstrate mechanistic integration with prostaglandin-mediated mucosal defense and NO-dependent microcirculatory regulation. The recurrent overlap among these pathways supports a multi-target pharmacodynamic model in which phytotherapeutic agents mitigate ethanol-induced gastric damage through simultaneous reinforcement of epithelial integrity, restoration of redox balance, and attenuation of inflammatory cascades.
Collectively, this mechanistic convergence underscores a systems-level pattern of gastroprotection, emphasizing functional integration over botanical taxonomy and strengthening the translational relevance of phytotherapeutic interventions in experimental ulcer models.
10. Mechanistic Synthesis of Gastroprotective Effects
Although ethanol concentrations (50–100% v/v), administered volumes, and exposure times varied substantially among studies, a clear mechanistic convergence is evident. The majority of plant extracts significantly attenuated ulcer severity (↓ ulcer index and lesion area) while enhancing endogenous antioxidant systems (↑ GSH, SOD, CAT; ↓ MDA and lipid peroxidation) and suppressing key inflammatory mediators (↓ TNF-α, IL-1β, MPO). Several studies further demonstrated modulation of apoptosis-related proteins (↓ Bax, ↓ Caspase-3; ↑ Bcl-2), preservation of gastric mucus content, and stimulation of nitric oxide and prostaglandin pathways, suggesting integrated cytoprotective, antioxidant, and mucosal defensive mechanisms. Flavonoid- and tannin-rich extracts frequently exhibited dose-dependent effects, reinforcing the role of polyphenolic compounds as principal bioactive contributors [15,66].
The reproducibility of protective outcomes relative to reference drugs such as Omeprazole, Ranitidine, and Lansoprazole further validates the translational relevance of the ethanol-induced ulcer model [59,66,67,69,70,72,78,79,118,119,120,124].
Taken together, these findings indicate that phytochemicals exert multi-target gastroprotection primarily through coordinated antioxidant and anti-inflammatory pathways. The integrated molecular mechanisms underlying ethanol-induced gastric injury and phytochemical-mediated gastroprotection are schematically illustrated in Figure 3. Nevertheless, harmonization of dosing strategies and experimental protocols is required to strengthen quantitative comparability and translational extrapolation.
11. Clinical Evidence and Translational Relevance
A substantial body of experimental evidence supports the gastroprotective effects of medicinal plant extracts in ethanol-induced gastric ulcer models. However, clinical evidence in humans remains limited. Most protective effects of the plant extracts discussed in this review have been demonstrated primarily in preclinical settings, particularly rodent models of ethanol-induced gastric injury [15,34,55,66,80].
Available clinical studies and traditional usage reports suggest potential benefits of certain plants—especially those rich in flavonoids, polyphenols, and mucilaginous compounds—in reducing gastric irritation and alleviating dyspeptic symptoms. Where clinical evidence exists, we summarize the study design (e.g., clinical trial, observational study), population (healthy volunteers or patients with ulcers), intervention (extract dose and duration), and outcomes (ulcer healing, symptom improvement, or gastric protection markers). For extracts without clinical data, this is explicitly indicated [16,17,125,126].
In conclusion, while preclinical studies strongly support the gastroprotective effects of medicinal plant extracts, clinical evidence in humans is limited. Available trials and traditional reports suggest potential benefits, particularly for plants rich in flavonoids, polyphenols, and mucilaginous compounds. Further well-designed clinical studies are needed to confirm efficacy, determine optimal dosing, and assess safety before routine clinical use [17,66,80,125].
12. Discussion
The studies summarized in Table 1 confirm the significant gastroprotective potential of medicinal plant extracts in ethanol-induced gastric ulcer models [17,66,68,80,125]. Ethanol-induced mucosal injury results from a complex interplay of oxidative stress, inflammatory cytokine production, apoptosis, and acid-mediated epithelial damage [19,20,28,32]. Phytochemicals, particularly flavonoids, polyphenols, alkaloids, and tannins, exert coordinated protective effects by reducing ulcer severity, enhancing antioxidant defenses (↑ GSH, SOD, CAT; ↓ MDA) [37,125], suppressing inflammatory mediators (↓TNF-α, IL-1β, MPO) [33,38,44], and preserving mucosal integrity through stimulation of mucus, nitric oxide, and prostaglandin pathways [17,26,27].
Dose-dependent gastroprotection was consistently observed, with polyphenolic- and tannin-rich extracts such as Punica granatum [66], Rosmarinus officinalis [86], Glycyrrhiza glabra [80], and Rhodiola rosea [17] demonstrating robust modulation of oxidative stress, apoptosis-related proteins (Bax/Bcl-2, Caspase-3) [33,125], and inflammatory signaling [38,44]. These findings highlight the multi-mechanistic nature of phytochemical action, which extends beyond acid suppression and positions these compounds as promising candidates for complementary or preventive interventions.
Comparisons with standard anti-ulcer drugs, including Omeprazole, ranitidine, and lansoprazole, validate the ethanol-induced ulcer model and reinforce the translational relevance of the observed gastroprotective effects [45,127]. Several extracts exhibited both cytoprotective and anti-inflammatory activities, indicating that convergent mechanisms, rather than a single pathway, mediate mucosal protection [44,125].
Despite these promising preclinical outcomes, several methodological limitations warrant consideration. Heterogeneity in ethanol concentration, exposure duration, extract composition, dosage, and animal species introduces variability and limits direct quantitative comparison across studies [107,128]. Moreover, most findings are derived from rodent models, and clinical evidence in humans remains limited [17,125]. Therefore, direct extrapolation to clinical protocols should be made cautiously, and additional well-designed human studies are needed to confirm efficacy, optimal dosing, and safety.
Collectively, the evidence indicates that medicinal plant extracts act via integrated antioxidant, anti-inflammatory, cytoprotective, and anti-apoptotic mechanisms, offering multi-target gastroprotection with lower toxicity relative to conventional therapies. Standardization of extract preparation, administration, and treatment duration, along with rigorous clinical validation, is essential to translate these preclinical findings into potential therapeutic applications, particularly as adjuvant or preventive interventions for high-risk populations [17,125].
13. Limitations and Future Directions
Despite compelling preclinical evidence, several limitations constrain the translational applicability of phytotherapeutics for ethanol-induced gastric ulcers. Most studies are restricted to animal models with variability in species, ethanol dosing, extract composition, administration routes, and treatment durations, limiting direct clinical translation [17,18]. Sample sizes are often small, and statistical rigor is sometimes insufficient [86,129].
Key gaps remain in understanding the bioavailability, pharmacokinetics, and potential interactions of herbal compounds with conventional medications. Heterogeneity in extract composition and preparation methods further limits reproducibility. Future research should focus on standardized extracts, rigorously designed preclinical protocols, and well-controlled clinical trials to evaluate efficacy, optimal dosing, and safety. Investigating synergistic effects with conventional anti-ulcer drugs may reveal novel combination therapies and enhance translational potential [16,17,88,125].
14. Conclusions
Ethanol-induced gastric ulcer models consistently demonstrate the multi-target gastroprotective potential of medicinal plant extracts. Phytochemicals, particularly flavonoids, polyphenols, tannins, and alkaloids, mitigate mucosal damage through coordinated antioxidant, anti-inflammatory, cytoprotective, and anti-apoptotic mechanisms. Compared with conventional therapies, these natural compounds may exhibit lower toxicity in preclinical models and demonstrate multifaceted protective effects, making them promising candidates for further investigation as adjunctive or alternative ulcer therapies.
Although preclinical evidence is robust, however, clinical validation remains limited, and well-designed human studies are essential to confirm efficacy, determine optimal dosing, and evaluate safety. Overall, plant-derived bioactive compounds represent promising, safe, and cost-effective alternatives or adjuncts for gastric ulcer management, highlighting the translational potential of phytotherapy in future clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1He K. Ye S. Kou Y. Du S. Yuan W. Ge L. Tian Y. Luo B. Ha Y. Zhan L. Global trends and future predictions of gastrointestinal ulcers in youth Front. Public Health 202513151105010.3389/fpubh.2025.151105040756384 PMC 12315113 · doi ↗ · pubmed ↗
- 2Najm W.I. Peptic ulcer disease Prim. Care Clin. Off. Pract.20113838339410.1016/j.pop.2011.05.00121872087 · doi ↗ · pubmed ↗
- 3Amandeep K. Robin S. Ramica S. Sunil K. Peptic ulcer: A review on etiology and pathogenesis Int. Res. J. Pharm.201233438
- 4Ko K.A. Lee D.-K. Nonsteroidal Anti-Inflammatory Drug-Induced Peptic Ulcer Disease Korean J. Helicobacter Up. Gastrointest. Res.202525344110.7704/kjhugr.2025.000440550526 PMC 12173566 · doi ↗ · pubmed ↗
- 5Zapata-Colindres J.C. Zepeda-Gómez S. Montaño-Loza A. Vázquez-Ballesteros E. de Jesús Villalobos J. Valdovinos-Andraca F. The association of Helicobacter pylori infection and nonsteroidal anti-inflammatory drugs in peptic ulcer disease Can. J. Gastroenterol. Hepatol.20062027728010.1155/2006/175217 PMC 265990516609757 · doi ↗ · pubmed ↗
- 6Alexander S.M. Retnakumar R.J. Chouhan D. Devi T.N.B. Dharmaseelan S. Devadas K. Thapa N. Tamang J.P. Lamtha S.C. Chattopadhyay S. Helicobacter pylori in human stomach: The inconsistencies in clinical outcomes and the probable causes Front. Microbiol.20211271395510.3389/fmicb.2021.71395534484153 PMC 8416104 · doi ↗ · pubmed ↗
- 7Levenstein S. Rosenstock S. Jacobsen R.K. Jorgensen T. Psychological stress increases risk for peptic ulcer, regardless of Helicobacter pylori infection or use of nonsteroidal anti-inflammatory drugs Clin. Gastroenterol. Hepatol.201513498506.e 110.1016/j.cgh.2014.07.05225111233 · doi ↗ · pubmed ↗
- 8Deding U. Ejlskov L. Grabas M.P.K. Nielsen B.J. Torp-Pedersen C. Bøggild H. Perceived stress as a risk factor for peptic ulcers: A register-based cohort study BMC Gastroenterol.20161614010.1186/s 12876-016-0554-927894275 PMC 5126869 · doi ↗ · pubmed ↗