Beetroot Juice Enhances Nitrate Metabolism and Endothelial Function but Not Cardiovascular or Strength Performance in Bodybuilders with a History of Anabolic–Androgenic Steroid Abuse: A Crossover Trial
Leonardo Santos L. da Silva, Leonardo Da Silva Gonçalves, Marcio F. Tasinafo Junior, Yaritza B. Alves Sousa, Macario Arosti Rebelo, Carolina S. Guimaraes, Jose E. Tanus-Santos, Carlos R. Bueno Junior, Jonas Benjamim

TL;DR
This study found that beetroot juice improves endothelial function in bodybuilders with a history of steroid use but does not affect cardiovascular or strength performance.
Contribution
The study is the first to investigate the effects of dietary nitrate on vascular and cardiovascular responses in men with a history of anabolic–androgenic steroid abuse.
Findings
Beetroot juice significantly increased salivary nitrate and nitrite concentrations.
Flow-mediated dilation improved with nitrate-rich juice both before and after exercise.
No changes in blood pressure or strength performance were observed with nitrate supplementation.
Abstract
Inorganic nitrate (NO3−) has demonstrated therapeutic efficacy in several populations characterised by cardiovascular risk. However, it is unknown whether increasing nitric oxide (NO) bioavailability affects vascular and cardiovascular responses in men with androgenic–anabolic steroid (AAS) abuse. Objective: To investigate the effects of dietary NO3− on cardiovascular, autonomic, and strength performance in men with AAS abuse. Methods: In this double-blind, randomised, placebo-controlled crossover trial, participants consumed beetroot juice (12.8 mmol [800 mg] NO3−) or a placebo (0.3 mmol NO3−). After two hours, assessments included saliva collection, endothelial function, heart rate, and systolic (SBP) and diastolic (DBP) blood pressure at rest, during, and after an isometric handgrip test. Results: Thirteen resistance-trained males [mean (standard deviation) age: 31 (9) y; body mass…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
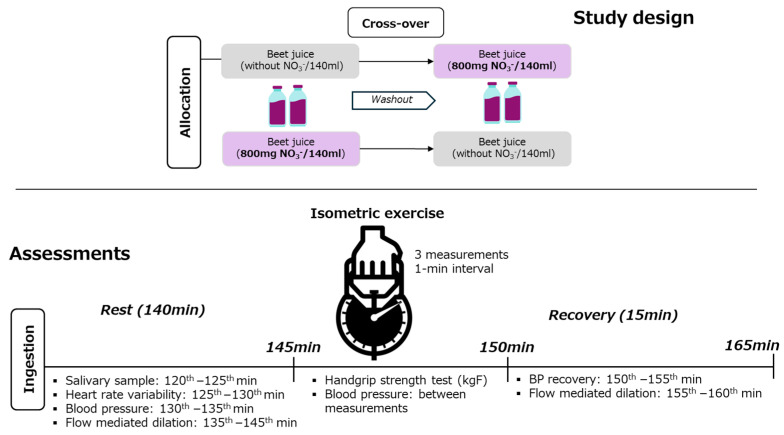 Figure 1
Figure 1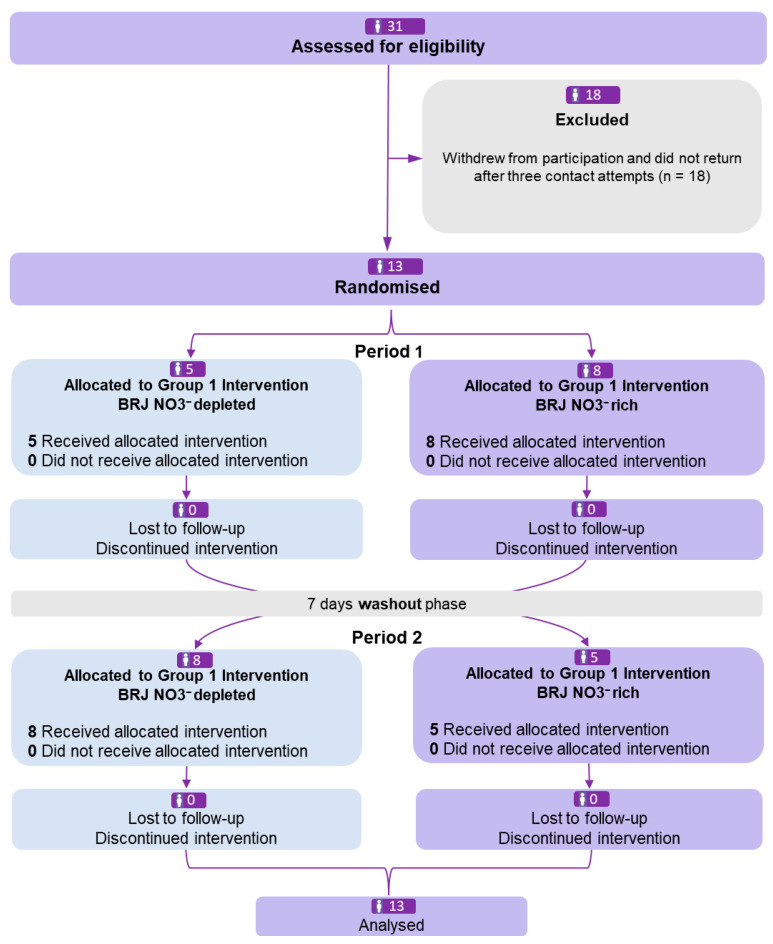 Figure 2
Figure 2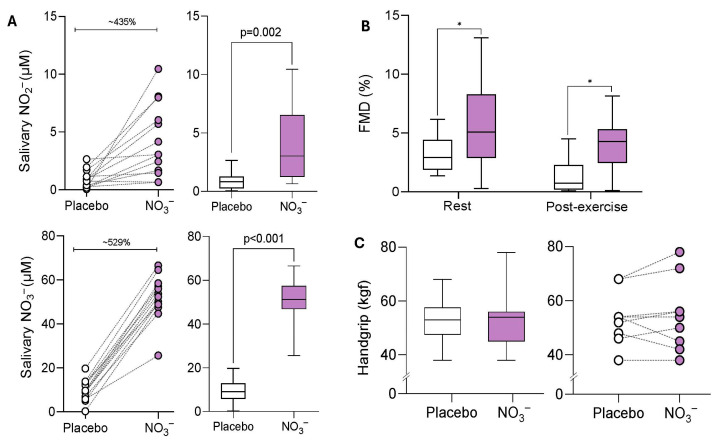 Figure 3
Figure 3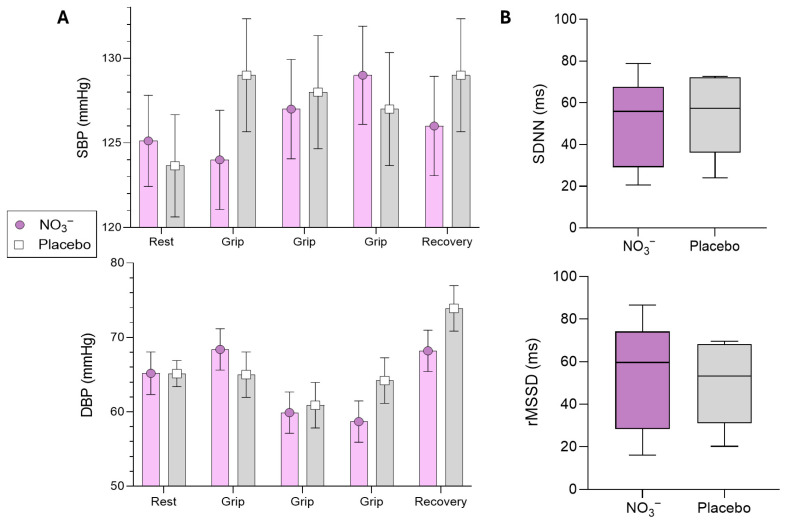 Figure 4
Figure 4- —School of Exercise and Nutrition Science, Deakin University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHormonal and reproductive studies · Menopause: Health Impacts and Treatments · Hormonal Regulation and Hypertension
1. Introduction
The abuse of androgenic–anabolic steroids (AAS) is associated with detrimental cardiovascular outcomes, primarily stemming from impairments in vascular function and dysregulation of cardiac autonomic control [1]. Among the notable cardiovascular alterations, epidemiological studies have elucidated transient arterial hypertension, autonomic dysfunction [2], and attenuated endothelial function [3,4]. These cardiovascular sequelae [5] are implicated in a threefold elevation in all-cause mortality risk, having cardiovascular adverse events as the primary leading cause [6]. While certain cardiac remodelling phenomena in habitual AAS users [7], such as hypertrophic cardiomyopathy, exhibit irreversible characteristics, recent findings have indicated that increased nitric oxide (NO) bioavailability can positively influence key independent cardiovascular risk factors [8,9,10] by decreasing blood pressure [11,12,13,14], restoring cardiac autonomic balance, and enhancing endothelial integrity in hypertension [15,16,17]. There is a growing body of literature that has substantiated the therapeutic efficacy of dietary inorganic nitrate (NO_3_^−^) within high-cardiovascular-risk (with hypertension and/or chronic heart failure) cohorts [18,19,20,21,22,23,24,25]. However, it is unclear whether increases in NO bioavailability can lead to improvements in cardiovascular variables in men with a history of androgenic–anabolic steroid abuse [26]. Accordingly, this study aimed to investigate the acute effects of inorganic NO_3_^−^ on cardiovascular responses at rest and during a standardised physical exertion in men with androgenic–anabolic steroid use. Based on the established role of NO_3_-derived NO in modulating vascular tone and metabolic efficiency, we hypothesised that NO_3_^−^ ingestion would improve endothelial function and cardiovascular responses during physiological stress. Conversely, we did not expect changes in maximal isometric strength performance, as dietary NO_3_^−^ primarily influences metabolic and vascular pathways rather than neural drive or motor unit recruitment, which are key determinants of maximal force production.
2. Materials and Methods
This randomised crossover study employed a double-masked and placebo-controlled design. The study protocol was approved by the Research Ethics Committee of the University of São Paulo, Brazil (CAAE: 66450622.4.0000.5659, 22 March 2023), and prospectively registered on ClinicalTrials.gov [NCT05835401] on 18 April 2023. All participants read and signed a consent form agreeing to the experimental protocol.
2.1. Participants
This study recruited adult men (18–45 years old) with current or previous ASS abuse for at least 12 months before inclusion. Participants were classified as current AAS users or previous AAS users based on self-reported history of anabolic-androgenic steroid use obtained through a structured interview. Previous AAS users had discontinued all AAS use, whereas current users maintained their habitual AAS use throughout the study period. Participants were excluded if they had a previous history of acute myocardial infarction/stroke, known allergy/intolerance to NO_3_^−^, or were currently under pharmacological therapy involving proton pump inhibitors, beta-blockers, calcium-antagonist channel, or antibiotic use over the last 4 weeks due to their potential influences on oral NO_3_^−^ reducing metabolism and function. During an initial screening, participants were asked about their health status and provided with a familiarisation session with research protocols. None of the enrolled participants had a clinical diagnosis of hypertension or were using antihypertensive drugs at the time of the study.
At the beginning of the session, blood samples were collected to analyse blood lipids and total free testosterone levels. In sequence, a dual X-ray absorptiometry was performed with the participants to analyse their body compartments (see Table 1).
2.2. Intervention
After the initial interview, participants were instructed to avoid foods high in NO_3_^−^ exceeding 15 mg per serving [27,28]. This guideline was applied throughout the study, including the washout period. Additionally, participants were advised not to use mouthwash, which is critical for maintaining oral microbiota NO_3_^−^ reducing capacity [29]. They completed a food questionnaire before each intervention and were asked to refrain from vigorous physical activity one day before and on testing days. One day before lab testing, participants were reminded not to consume caffeine (coffee, energy drinks, teas) for 12 h before each phase of the study and to avoid alcohol 24 h beforehand [30]. This study employed a two-arm intervention testing the effects of an acute dose of 140 mL of beetroot juice (BJ) rich in NO_3_^−^ 800 mg NO_3_^−^ [12.8 mmol]) compared to 140 mL of BJ depleted in NO_3_^−^ (0.3 mmol). The NO_3_^−^ content was based on manufacturer certification, with all products stored under recommended conditions, used within their expiration date, and functionally verified by increases in salivary NO_3_^−^ and NO_2_^−^ concentrations. Both interventions were matched in flavour, colour, and taste, which were purchased from the same manufacturer (James White Ltd., Ashbocking, UK). The randomisation (1:1) has been performed to allocate the participants to the first intervention using randomizer.org by an independent researcher who has not been involved with the research. After the first intervention, they completed a one-week washout and returned to perform the opposite intervention. The washout time was chosen based on previous studies that demonstrated that 7 days is enough to avoid carryover effects [21,31]. The process of concealing the treatment allocation order was performed by an independent researcher. Participants were not informed of the intervention order. The researcher measuring variables was blinded, while an external researcher handled the juice delivery. A masked collaborator conducted the statistical analysis.
2.3. Outcomes
The participants arrived in the laboratory in a fasted state (8 h) and then ingested the BJ. After a standard two-hour period, unstimulated saliva samples were collected using the spitting method [32] and quickly centrifuged at 3000 rpm at 4 °C for 15 min and stored at −80 °C. This was the only saliva collection in each condition. The laboratory environment has been controlled with a temperature between 22 and 24 °C and a humidity of 50–60% [15]. The evaluations started in the morning at the same time point (e.g., 07:00 a.m.) for each participant to standardise the influence of the circadian rhythm on the variables collected. During the evaluations, the participants kept quiet and silent [33].
2.3.1. Blood Pressure
The sBP and dBP values were indirectly measured on the participant’s dominant arm using a clinically validated BP monitor (OMRON-M2^®^, HEM-7121-E, Sao Paulo, Brazil) previously calibrated. The measurements were performed in the supine position.
2.3.2. Secondary Outcomes
Heart rate (HR) was recorded beat-by-beat using a Polar^®^ H10 monitor (1000 Hz, RS800CX, Kempele, Finland). After each session, HR data were exported, and segments containing at least 256 stable R–R intervals (RRis) with more than 95% sinus beats were included. The initial 256 RRis from each 5 min window were imported into Kubios software (v2.1) to calculate HRV indices. Time-domain measures included the root mean square of successive differences (RMSSD) and the standard deviation of normalised R–R intervals (SDNN) [34,35,36,37]. Endothelial function was evaluated by flow-mediated dilatation (FMD) using a high-resolution Doppler ultrasound system 2D bidirectional ultrasound system (SAEVO^®^, Sao Paulo, Brazil) equipped with a 14 MHz linear transducer. Participants were positioned supine with the right arm abducted. The transducer was aligned longitudinally over the brachial artery, 5–10 cm above the antecubital crease, to measure pre-exercise diameter. The forearm cuff was subsequently inflated to 50 mmHg above the participant’s resting systolic blood pressure using an automated rapid-inflation system. The cuff remained inflated for five minutes to completely occlude blood flow to the forearm. After the 5 min occlusion period, the cuff was rapidly deflated to induce reactive hyperaemia. After cuff deflation, the brachial artery post-occlusion diameter was recorded for 2 min at the same site. Post-occlusion diameter was identified using manual frame-by-frame analysis by the same trained and experienced operator. Saliva was analysed for NO_2_^−^ and NO_3_^−^ concentration. An ozone-based reductive chemiluminescence assay has been performed, as previously described [38]. To quantify NO_2_^−^, 100 μL of saliva in duplicate was injected into an acidified tri-iodide solution purged with nitrogen and connected in-line with a chemiluminescence NO analyser (Sievers Model 280, Boulder, CO, USA). For NO_3_^−^ quantification, saliva samples were reduced with vanadium (III) in 1 mol/L HCl at 90 °C, and the released NO was carried by nitrogen gas to the analyser. In both assays, the reactive NO gas generated a chemiluminescent signal upon interaction with ozone (O_3_), and signal intensity was quantified using eDAQ-Chart software version 5.5.27 [38]. Isometric exercise test: To assess maximum voluntary contraction, a CAMRY^®^ brand adjustable and calibrated handgrip device with a scale of 0 to 100 kg was employed. Participants were seated with their shoulders slightly forward, elbows extended, arms beside the trunk and forearms and wrists in a neutral position. Their hand position was adjusted to the proximal interphalangeal joint positioned under the bar, and the grip was performed between the fingers and the thenar eminence with maximum comfort. During the test, participants performed a maximum of 5 s contractions for each arm with a 1 min interval [39,40]. Time points where each variable has been collected can be visualised in Figure 1.
2.4. Statistics
Our sample estimation was based on expected within-subject changes in systolic blood pressure (sBP) variation data from a prior meta-analysis investigating the NO_3_^−^ effectiveness after exercise [8]. Using the G*Power software (v. 3.1.9.2), a two-way ANOVA with repeated measures (three time points) was applied to assess the group-by-time interaction. The mean difference (SD) values of sBP following NO_3_^−^ supplementation were −4.5 (7) mmHg compared to placebo, yielding an estimated effect size of 0.46 [18]. To detect significant differences with 80% power (β = 0.2) at a significant level of 0.05, 12 participants were required. To account for potential dropouts, we aimed to recruit 14 participants. Data normality distribution was assessed using the Shapiro–Wilk test. Statistical analyses were conducted with RStudio (v. 5.0.0) using an intention-to-treat approach. A linear mixed model (LMM) evaluated the effectiveness of the NO_3_^−^ intervention versus placebo, accounting for participants as a random effect, along with time and treatment group interactions. Interventions were treated as a group factor, time points from the submaximal exercise test and recovery were treated as repeated measures (the resting values of each variable have been used as covariates in the final model). The effects of treatments on cardiovascular measurements before and after exercise were tested, applying Bonferroni’s correction for multiple comparisons. Intergroup differences (placebo vs. NO_3_^−^) were assessed using LMM in direct comparisons, or t-test or Mann–Whitney U test, with significance set at p < 0.05.
3. Results
Thirteen apparently healthy resistance-trained men under current (~77%) and previous AAS use (~23%) for at least 12 months completed the randomised, crossover trial without dropouts (Figure 2). All details of the drugs used by the sample are presented in the Supplementary Material Table S1.
Supplementation with NO_3_^−^-rich BJ effectively increased salivary NO_3_^−^ (40.59 μM [95%CI: 34.99 to 46.19], p < 0.001) and NO_2_^−^ (3.08 μM [95%CI: 1.26 to 4.90], p = 0.002) concentrations compared with the placebo, confirming protocol compliance (Figure 3A). Endothelial function (flow-mediated dilation) was significantly greater in the NO_3_^−^ group compared with placebo under both pre-exercise (2.37% [95%CI: 0.31 to 4.40], p = 0.02) and post-exercise conditions (2.57% [95%CI: 0.54 to 4.60], p= 0.01). These findings demonstrated that NO_3_^−^ supplementation enhanced endothelial function independently of exercise (Figure 3B). Comparisons between protocols (NO_3_^−^ vs. placebo) to the isometric strength test (handgrip) did not reveal changes (0.02 kgf [95%CI: −9.74 to 9.71, p = 0.99) (Figure 3C).
Regarding blood pressure responses, the sBP showed no significant differences between conditions during the exertion (Grip 1: NO_3_^−^ vs. PLA: −4.0 mmHg [95%CI: −11.2 to 3.20, p = 0.270]; Grip 2: NO_3_^−^ vs. PLA: −0.7 mmHg [95%CI: −7.8 to 6.5, p = 0.858]; and Grip 3: NO_3_^−^ vs. PLA: −1.3 mmHg [95%CI: −5.9 to 8.4, p = 0.731]) and during recovery from exercise (NO_3_^−^ vs. PLA: −2.4 mmHg [95%CI: −9.6 to 4.8, p = 0.506]). Similarly, dBP also did not show significant differences between conditions during the exertion (Grip 1: NO_3_^−^ vs. PLA: 3.4 mmHg [95%CI: −3.5 to 10.3, p = 0.326]; Grip 2: NO_3_^−^ vs. PLA: −1.0 mmHg [95%CI: −7.9 to 5.9, p = 0.768]; and Grip 3: NO_3_^−^ vs. PLA: −5.6 mmHg [95%CI: −12.4 to 1.3, p = 0.112]) and during recovery from exercise (NO_3_^−^ vs. PLA: −5.7 mmHg [95%CI: −12.5 to 1.2, p = 0.104]) (Figure 4A). In addition, no changes were found to HRV indices, SDNN (p = 0.99) or RMSSD (p = 0.68), suggesting that NO_3_^−^ was unable to enhance cardiac autonomic modulation at rest (Figure 4B).
4. Discussion
To our knowledge, this is the first study to investigate the effects of dietary NO_3_^−^ in men undergoing AAS abuse. Our preliminary findings indicated that enterosalivary pathway metabolism has been changed upon NO_3_^−^ ingestion, observed by an increase in saliva NO_3_^−^ and NO_2_^−^. In this regard, we also observed that some participants blunted the oral capacity to reduce NO_3_^−^ orally, being noted by no individual changes in saliva NO_2_^−^ concentrations across the dietary NO_3_^−^ and placebo conditions. Our findings also demonstrated that NO_3_^−^ can elicit changes in endothelial functions assessed by FMD aligned with increases in oral NO_3_^−^/NO_2_^−^ concentrations following NO_3_^−^ ingestion, but these improvements did not translate to changes in blood pressure, even at rest and during post-exercise. Based on these findings, the detrimental effects of AAS on blood pressure and on cardiac autonomic modulation may not be counteracted with increased NO bioavailability.
The clinical relevance of the observed improvement in FMD should be interpreted within the acute nature of the intervention. Acute NO_3_^−^ studies consistently report modest but significant increases in FMD, reflecting enhanced endothelial NO-dependent responsiveness rather than long-term vascular adaptation. The magnitude of the FMD change observed in the present study is comparable to that reported in prior acute interventions and falls within a range generally considered physiologically meaningful in endothelial function research [17,41]. However, while such acute improvements are indicative of favourable vascular responsiveness, they should not be interpreted as direct evidence of sustained cardiovascular risk reduction. Notably, some participants appeared to exhibit a blunted oral NO_3_^−^-reducing capacity, evidenced by the absence of a rise in salivary NO_2_^−^ after NO_3_^−^ ingestion. This inter-individual variability is likely driven primarily by differences in the oral microbiome, particularly the abundance and activity of NO_3_^−^-reducing bacteria located on the tongue [42,43,44]. Recent oral hygiene practices, such as toothbrushing, tongue scraping, or the use of antibacterial mouthwash, may acutely suppress these bacteria and impair NO_3_^−^ to NO_2_^−^ conversion. Habitual diet may also play a role, as regular intake of NO_3_^−^-rich vegetables may promote microbial adaptation, whereas low plant consumption may reduce this capacity [45]. Additional contributors include salivary flow rate, circadian variation, smoking, medication use (e.g., antibiotics or proton pump inhibitors), ageing, and cardiometabolic health [46,47]. Together, these factors highlight the strong oral and lifestyle dependence of the enterosalivary NO_3_^−^-NO_2_^−^-NO pathway and help explain the variability in salivary NO_2_^−^ responses.
The participants in our sample presented high blood pressure levels but lacked a hypertension clinical diagnosis, and the lack of effects on this variable indicates that AAS abuse can target other mechanisms (e.g., oxidative stress) related to blood pressure not assessed in this study [48,49]. The handgrip test has been used to induce cardiovascular stress in this population and mimic isometric strength training routinely performed by this population in a gymnasium. As expected, no changes have been identified between NO_3_^−^ and placebo conditions. The lack of effects during the handgrip strength test is strongly supported by previous research [28]. Furthermore, these outcomes are widely explained by the bioenergetics contributions to NO_3_^−^ to exercise capacity, where it is more related to exercise actions that last between 2 and 10 minutes of duration [50,51]. During the initial six months of recruitment, several participants gave up participating. It delayed the conclusion of the research, but most importantly, it shed light on the challenges to developing research projects focused on health in this population. Importantly, the small sample size and the absence of a non-AAS control group limit the generalizability of the present findings, and therefore, the results should be interpreted with caution. Due to the exploratory nature of this study, we would be pleased to see further randomised trials on this topic to confirm these results, but also to dive into variables not assessed in our research.
For instance, our findings demonstrate that while dietary inorganic NO_3_^−^ can enhance oral NO_3_^−^ metabolism through NO_3_^−^ and NO_2_^−^ salivary concentrations and elicit modest improvements in endothelial function, acutely these adaptations do not mitigate the persistent elevations in blood pressure induced by AAS abuse or improvements in cardiac autonomic modulation. It suggests that alternative or complementary mechanisms beyond nitric oxide bioavailability may underlie the blood pressure dysregulation observed in this population (e.g., oxidative stress, baroreflex impairment, microvascular rarefaction). However, due to the nature of the study (acute) and limited sample size, future long-term clinical trials with this population are warranted.
Previous studies investigating NO_3_^−^ supplementation have consistently demonstrated improvements in endothelial function, particularly FMD, whereas effects on autonomic modulation and neuromuscular performance appear more variable and context-dependent [17]. Acute NO_3_^−^ ingestion has been shown to enhance FMD in healthy and clinical populations, supporting the notion that endothelial responsiveness is especially sensitive to short-term increases in NO bioavailability. In contrast, changes in HRV are less consistently observed following acute supplementation and may require longer intervention periods, higher training stimuli, or populations with greater baseline impairment [35,52]. Key limitations include the short supplementation duration and limited power for secondary outcomes. Future studies should consider longer-term NO_3_^−^ supplementation, larger samples, and the inclusion of additional vascular (e.g., arterial stiffness, microvascular reactivity), autonomic (e.g., baroreflex sensitivity), and neuromuscular or performance-related outcomes to better delineate the temporal and mechanistic effects of inorganic NO_3_^−^.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Windfeld-Mathiasen J. Heerfordt I.M. Dalhoff K.P. Andersen J.T. Andersen M.A. Johansson K.S. Biering-Sørensen T. Olsen F.J. Horwitz H. Cardiovascular Disease in Anabolic Androgenic Steroid Users Circulation 202515182883410.1161/CIRCULATIONAHA.124.07111739945117 · doi ↗ · pubmed ↗
- 2Maior A.S. Carvalho A.R. Marques-Neto S.R. Menezes P. Soares P.P. Nascimento J.H.M. Cardiac Autonomic Dysfunction in Anabolic Steroid Users Scand. J. Med. Sci. Sports 20132354855510.1111/j.1600-0838.2011.01436.x 22257181 · doi ↗ · pubmed ↗
- 3Liu J.-D. Wu Y.-Q. Anabolic-Androgenic Steroids and Cardiovascular Risk Chin. Med. J.20191322229223610.1097/CM 9.000000000000040731478927 PMC 6797160 · doi ↗ · pubmed ↗
- 4Schwingel P.A. Zoppi C.C. Cotrim H.P. The Influence of Concomitant Use of Alcohol, Tobacco, Cocaine, and Anabolic Steroids on Lipid Profiles of Brazilian Recreational Bodybuilders Subst. Use Misuse 2014491115112510.3109/10826084.2014.90375324766402 · doi ↗ · pubmed ↗
- 5Alizade E. AvcıA. Fidan S. TabakçıM. Bulut M. Zehir R. Simsek Z. Evlice M. ArslantaşU. Çakır H. The Effect of Chronic Anabolic-Androgenic Steroid Use on Tp-E Interval, Tp-E/Qt Ratio, and Tp-E/Qtc Ratio in Male Bodybuilders Ann. Noninvasive Electrocardiol.20152059260010.1111/anec.1225625631523 PMC 6931420 · doi ↗ · pubmed ↗
- 6Vecchiato M. Ermolao A. Da Col M. Aghi A. Berton G. Palermi S. Battista F. Savino S. Drezner J. Zorzi A. Mortality in Male Bodybuilding Athletes Eur. Heart J.2025463006301610.1093/eurheartj/ehaf 28540393525 PMC 12342505 · doi ↗ · pubmed ↗
- 7Fyksen T.S. Vanberg P. Gjesdal K. von Lueder T.G. Bjørnerheim R. Steine K. Atar D. Halvorsen S. Cardiovascular Phenotype of Long-Term Anabolic-Androgenic Steroid Abusers Compared with Strength-Trained Athletes Scand. J. Med. Sci. Sports 2022321170118110.1111/sms.1417235460300 PMC 9540672 · doi ↗ · pubmed ↗
- 8Jones D.A. Beirne A.-M. Kelham M. Wynne L. Andiapen M. Rathod K.S. Parakaw T. Adams J. Learoyd A. Khan K. Inorganic Nitrate Benefits Contrast-Induced Nephropathy after Coronary Angiography for Acute Coronary Syndromes: The NITRATE-CIN Trial Eur. Heart J.2024451647165810.1093/eurheartj/ehae 10038513060 PMC 11089333 · doi ↗ · pubmed ↗