Molecular and Structural Changes, and Skeletal Muscle Strength and Endurance in Chronic Obstructive Pulmonary Disease and Interstitial Lung Disease: Practical Applications of Assessment and Management
Nina Patel, Ahmet Baydur

TL;DR
This paper explores how lung diseases like COPD and interstitial lung disease affect muscle function and how pulmonary rehabilitation can help improve strength and quality of life.
Contribution
The paper provides practical insights into assessing and managing muscle dysfunction in lung diseases through rehabilitation and identifies future research directions.
Findings
Skeletal muscle dysfunction in lung diseases is driven by factors like inflammation, oxidative stress, and medication effects.
Pulmonary rehabilitation improves neuromuscular efficiency and functional outcomes but plateaus after three months.
Future research should focus on EMG thresholds and pathways like mitochondrial remodeling to combat muscle wasting.
Abstract
Chronic obstructive pulmonary disease, interstitial lung disease, and post-lung trans-plantation are often accompanied by skeletal muscle dysfunction that worsens the quality of life. Such physiological changes are driven by physical inactivity, systemic inflammation, oxidative stress, anabolic and hormonal resistance, and medication effects. Structural changes include impaired capillarization, fiber-type shifts (slow-to-fast in limb muscle and fast-to-slow in respiratory muscles), mitochondrial dysfunction, reduced oxidative capacity, and early lactate accumulation. Electromyography and dynamometry, both isokinetic and isometric, quantify neuromuscular drive through measuring strength, power, and endurance and are associated with functional outcomes (6-min walk, sit-to-stand, stair climbing tests). Pulmonary rehabilitation (PR) improves neuromuscular efficiency, dyspnea, exercise…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
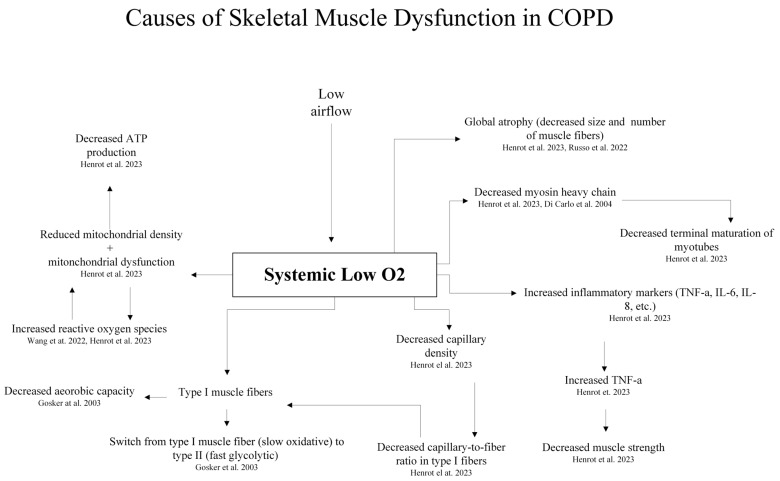 Figure 1
Figure 1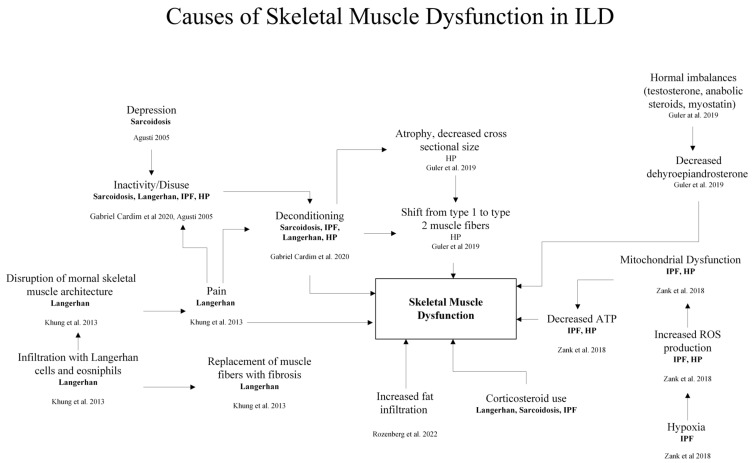 Figure 2
Figure 2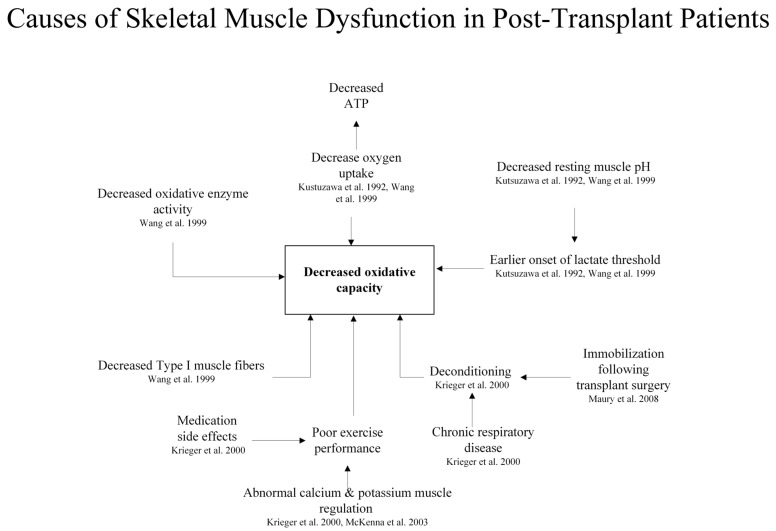 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Obstructive Pulmonary Disease (COPD) Research · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis · Cardiovascular and exercise physiology
1. Introduction: Physiological Changes in Skeletal Muscle in ILD, COPD, and Post-Transplant Patients
Chronic obstructive pulmonary disease (COPD) and interstitial lung disease (ILD) are debilitating respiratory conditions characterized by significant skeletal muscle dysfunction, profoundly impacting patient disability, morbidity, and general quality of life (Table 1) [1]. Systemic molecular and physiological changes affect the structure and function of skeletal muscles [2]. Reductions in muscle mass, strength, and endurance compromise exercise tolerance [3,4,5]. Other contributing factors include hormonal imbalances and oxidative stress [2,5]. Systemic inflammation inhibits protein synthesis, promotes protein muscle degradation, and contributes to muscle wasting [4]. Growth hormone, while maintaining its plasma concentration, exhibits decreased interaction with insulin-like growth factor, impairing proteostasis and decreasing muscle mass [6]. Pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6) are associated with the pathogenesis of muscle atrophy. Increased levels of catabolic hormones such as cortisol, and decreased levels of anabolic hormones such as testosterone, enhance muscle weakness and loss [6]. Structural alterations in skeletal muscle include a decrease in fatigue-resistant type 1 fiber size, which is important for endurance activities [5]. We review herein the background and recent developments in the field, including skeletal muscle structural and molecular changes occurring with chronic lung disease, methods of evaluating muscle function, and the benefits of pulmonary rehabilitation (PR) in the prevention and reversibility of such changes.
1.1. Methods of Literature Review
For this review, we conducted a non-systematic literature search using the PubMed, Scopus, and Web of Science databases. We also searched the Cochrane Central Register of Controlled Trials via the Cochrane Register of Studies, MEDLINE (OvidSP), Embase (OvidSP), and the Physiotherapy Evidence Database (PEDro). Search terms prioritized key mechanistic and clinical studies. We included “skeletal muscle weakness”, “fatigue”, “skeletal muscle fiber types”, “electromyography”, “dynamometry”, “chronic obstructive pulmonary disease”, “interstitial lung disease”, “lung transplantation”, “inflammation”, “oxidative metabolism”, “pulmonary rehabilitation”, “quality of life”, and “respiratory function”. We screened and evaluated relevant studies and reviews in English published from 1977 through 2025. The selection of references was based on their relevance to the pathophysiology, assessment, and management of limb muscle weakness, with new information on laboratory studies, key observational studies, and systematic reviews. We excluded discussions of skeletal muscle changes occurring with neuromuscular disease, as they do not directly result from lung disease, and the topic is covered extensively in the neuromuscular literature. Given the narrative nature of this review, we did not perform a formal risk of bias assessment, independent duplicate screening, or meta-analysis.
1.2. Skeletal Muscle Dysfunction in COPD: Molecular Mechanisms
Skeletal muscle wasting in COPD is attributed to physical inactivity resulting from expiratory flow limitation (EFL) and dynamic air trapping leading to exertional dyspnea and loss of motivation to exercise [1]. Studies of skeletal muscle dysfunction in COPD have primarily focused on the quadriceps [56]. EFL decreases systemic oxygenation, impairing muscle aerobic capacity, force generation, and endurance. Muscle fibers switch from a slow oxidative to a fast glycolytic type and exhibit a decrease in cross-sectional area (CSA) resulting in global atrophy (Figure 1) [56,57,58]. Capillarization is impaired, with decreased capillary density and capillary-to-fiber ratio in type 1 muscle fibers, altering oxidative capacity [56].
Patients exhibit elevated serum inflammatory markers such as tumor necrosis factor (TNF-α), interleukin-6 (IL-6), and interleukin-8 (IL-8) (Figure 1), which negatively associate with lean muscle mass and reduced strength in cachectic patients. TNF-α may play a role in promoting inflammation and catabolism through the NF-κB pathways as well as anabolic effects such as promoting satellite cell differentiation [56]. Yet, therapies targeting TNF-α have not consistently improved dyspnea or COPD exacerbation rates, indicating that it is not the key driver of muscle dysfunction [56]. Similarly, while IL-6 and IL-8 are related to catabolic effects, the transcriptional levels of these interleukins are generally unchanged in COPD patients [56]. Patients with COPD exhibit reduced muscle phosphocreatine (PCr) and ATP, but increased lactate and inorganic phosphate [7,8,57]. Blood lactate levels increase rapidly with minimal exertion [9]. In many respects, such changes parallel events occurring in cancer and sepsis [7,9,56,57,58].
Hypercapnia and hypoxia induce reductions in mitochondrial density, muscle fiber size, and muscle mass (Figure 1) [59]. Members of the hypoxia inducible factor 1 (HIF-1) family regulate the expression of several genes involved in adaptive processes that facilitate cell survival under hypoxic conditions [62]. Several different HIF-1- and chromatin-associated co-regulators play important roles in the transcriptional activity of HIF-1, and in the selection of binding sites, promoters, and target genes [60,62]. Hypoxia decreases terminal maturation of myotubes through decreasing myosin heavy chain [56,62]. Mitochondrial dysfunction manifests as reduced membrane potential, deficiency in important mitochondrial proteins, impaired oxidative phosphorylation, and increased mitochondrial reactive oxygen species [56,60]. Smoking, hypoxia, and physical inactivity are exacerbating factors (Figure 1) [60]. Gender plays a role in muscle dysfunction with greater weakness and impairment in women than in men. Female COPD patients possess smaller type II fiber CSAs compared to men, and higher levels of pro-inflammatory cytokines such as TNF-α and IL-8 [10,11].
The maintenance of muscle mass is maintained by signaling pathways that regulate protein synthesis and degradation, including the transforming growth factor beta (TGFβ) receptor superfamily, the ubiquitin–proteasome axis, calcium-dependent proteolysis, and autophagy cascades [63,64]. While basic studies in muscle atrophy involve animal and cell models of cancer [63,64], the same molecular mechanisms are likely active in the cachexia of chronic inflammatory conditions, as in COPD and ILD.
The sedentary lifestyle associated with advanced chronic lung disease suppresses autophagy activity [65]. Exercise is an autophagy inducer and is thought to contribute to the beneficial effects of exercise. Based on an acute exercise model in mice, Li et al. [65] identified lactate as a positive regulator of autophagy in skeletal muscle. Their mechanistic study showed that lactate enhances autophagy by inactivating the mammalian target of rapamycin complex 1 (mTORC1) through promoting mTOR lactylation. mTOR could be lactylated at myocyte lysine 921 (K921), which inactivated mTORcomplex1 (mTORC1), thereby linking lactate signaling to mTORC1-controlled autophagy during exercise. Their findings suggest a mechanism for explaining exercise-induced muscle adaptation, and a potential treatment strategy for muscle disuse and atrophy in individuals with chronic respiratory disease.
Mitochondrial dysfunction contributes to skeletal muscle atrophy, playing an important role in energy production, metabolic flexibility, controlling redox homeostasis, and regulation of apoptosis. Signaling pathways involved in skeletal muscle atrophy include the ubiquitin–proteasome system, autophagy, mitophagy, mitochondrial fission–fusion, and mitochondrial biogenesis [66].
Non-coding RNAs (ncRNAs) contribute to muscle dysfunction and muscle loss in patients with COPD [67,68,69,70]. The plasma levels of several myo-specific c-miRNAs are increased in patients with COPD and are possibly closely related to muscle turnover [59,67,68,69,70]. A reduction in skeletal muscle mass is associated with metabolic disorders such as insulin resistance and is a risk factor for cardiovascular diseases [59,68,69,70], which is also likely in patients who take inhaled glucocorticoids for COPD [71].
The myriad pathways contributing to muscle disuse and atrophy are frequently the consequence of environmental exposures as well as the mechanical stresses under which such patients labor, but at the same time they offer the potential for ameliorating and even reversing the associated physical impairment (discussed below).
1.3. Skeletal Muscle Dysfunction in ILD
As in COPD, deconditioning in ILD develops with inactivity and disuse as patients try to avoid dyspnea. In addition, changes in growth and sex hormones alter muscle function and mass. Patients with idiopathic pulmonary fibrosis (IPF) exhibit decreased levels of dehydroepiandrosterone (DHEA); anabolic steroids, myostatin, and testosterone have been related to disease-related wasting as in COPD patients (Figure 2) [12,35].
Fat infiltration of lower extremity muscles impairs mobility and muscle performance, particularly in older individuals (Figure 2) [13]. Similar to COPD, skeletal muscle atrophy occurs more in lower than in upper limbs [14]. There is greater muscle fat in patients experiencing functional impairment. Yet upper limb muscle dysfunction and decreased physical performance are not related to body fat percentage or muscle mass. The existence of alternative pathways in which limb muscle function and performance are affected by ILD [35], highlights a need for future study to clarify which alternate pathways that affect this process.
Oxygenation levels in the quadriceps of patients with ILD are decreased compared to intercostal muscles at rest, which is related to reduced blood flow to the lower extremities [15]. Yet, in a near-infrared spectroscopy (NIRS) study (a non-invasive technique used to determine the relative oxygen saturation of myoglobin and hemoglobin) comparing oxygen use in 30 healthy individuals and 30 patients with mild ILD. Pehlivan et al. [15] found that oxygenation of the exercising limb was similar in both groups. Instead, they proposed that the increase in the work of breathing diverted blood away from lower extremities, resulting in exercise intolerance [15].
1.4. Skeletal Muscle Dysfunction in Post-Lung Transplant Patients
Following lung transplantation, patient outcomes are associated with skeletal muscle dysfunction. In both single and double lung transplant patients, work capacity and peak oxygen uptake (VO_2_max) remain decreased despite exercise training [76]. NIRS shows altered venous and oxygen content and increased cardiac output (CO) before and after transplantation (Figure 3) [76]. Peak VO_2_ decreased in post-transplant patients 5 to 38 months after transplantation, although impaired ventilation, anemia, and arterial oxygen saturation do not account for these changes [16]. Nuclear magnetic resonance spectroscopy (NMR) analysis during quadriceps exercise exhibits a decrease in resting muscle pH (7.07 in post-transplant patients vs. 7.12 in healthy volunteers), an earlier onset of lactate threshold, and decreases in oxygen uptake and oxidative capacity (Figure 3) [16,17,18], ascribed to immunosuppressant toxicity [76] (Figure 3).
Skeletal muscle dysfunction immediately following transplantation is attributed to prolonged immobility in intensive care (Figure 3) [44]. Poor exercise performance relates to disorders of muscle calcium and potassium regulation: While muscle sarcoplasmic reticulum calcium is downregulated with decreased calcium release and calcium uptake, Sodium–Potassium Adenosine Triphosphatase (Na^+^-K^+^-ATPase) activity is increased by 31% [19], suggesting a dissociation in the expression of sarcoplasmic reticulum function and myosin ATPase (Figure 3) [19,76]. Exercise intolerance in post-transplant patients is associated with slow-to-fast muscle fiber conversion, reduced ATP content, and de-creased oxidative enzyme activity [17]. Immunosuppressants, such as cyclosporin A, inhibit calcineurin-activated pathways, also leading to slow-to-fast muscle fiber conversion [19].
2. Methods of Evaluating Muscle Dysfunction
2.1. Electromyography (EMG) Analysis for Quantifying Skeletal Muscle Dysfunction: Technical Challenges
Electromyography (EMG) offers valuable insights into neuromuscular function with its ability to assess changes in muscle activation, muscle fiber recruitment, and neuromuscular transmission by recording the frequency and amplitude of electrical signals during muscle activation [77,78,79]. The decreased EMG amplitude recorded during maximal contractile effort indicates muscle weakness or impaired neuromuscular drive [80].
The surface myoelectric signal (MES) has been used as an input to controllers for powered prostheses for many years. Amongst the concerns of recording EMG signals have been differences between surface and intramuscular needle electrodes in signal detection. A potential disadvantage of MES is the loss of more global information contained in the surface MES. Hargrove and colleagues [81] studied 12 normally limbed subjects by placing four equally spaced surface electrodes to the circumference of the forearm. They compared the classification accuracy of six pattern recognition-based myoelectric controllers using multi-channel surface MES as inputs to the same controllers which used multi-channel intramuscular MES as inputs, with both sets of signals collected simultaneously for 10 different classes of isometric contraction. The investigators found that information obtained from either surface or intramuscular sensors provided excellent classification accuracy; both measurement techniques yielded classification accuracies between 95% and 99%.
The normalization of signals has been another challenge, with different approaches utilized to address it. Shin et al. [78] used surface EMG electrodes set by Surface Electromyography for the Non-invasive Assessment of Muscles (SENIAMs) [82]. Subjects performed two 5-s-long maximum voluntary isometric contractions (MVICs). The root mean square (RMS) value of the rectus femoris muscle divided by the MVIC was used to analyze the normalized RMS in the ramp exercise test. Gephine et al. [83] compared quadriceps oxygenation and surface EMG (sEMG) responses during 1-min sit-to-stand (1STS) tests in 14 individuals with severe COPD and 12 controls. sEMG signals were normalized for each sit-to-stand (STS) (one cycle) test using electrogoniometer signals during the 1STS.
Shifts to a lower frequency indicate reduce motor unit firing velocity and fatigue-related slowing of muscle fiber conduction velocity [84,85]. Fourier analysis of force-frequency changes occurring during muscle fatigue converts the EMG signal from the time domain into the frequency domain demonstrating slowing muscle fiber conduction during fatigue [86]. In experimental studies, the median frequency consistently decreases more than muscle fiber conduction velocity (MFCV). Lowery et al. [84] compared a new estimate of EMG frequency compression, the spectral compression estimate (SCE), with the median frequency of the EMG power spectrum, the median frequency of the EMG amplitude spectrum and MFCV measured during sustained isometric, fatiguing contractions of the brachioradialis muscle at 30, 50, and 80% maximum voluntary contraction. They found that the SCE provided a better estimate of the observed changes in MFCV than the median frequency of either the EMG power spectrum or EMG amplitude spectrum.
The net force exerted by muscle depends on the magnitude and timing of motor unit activity, the contractile properties of the activated muscle fibers, and the mechanical characteristics of the connective tissues transmitting the forces to the limb [87]. Limitations in interpreting motor unit activity from EMG recordings include the consequence of dissociation between motor unit characteristics and muscle fiber types. For example, the number of motor unit action potentials may not directly relate to the number of muscle fiber action potentials that contribute to an EMG signal [87]. As such, the EMG signal amplitude is not a direct index of the neural drive to muscle, especially during fatiguing contractions. Still, the signal amplitude provides a useful approximation of the amplitude of the neural drive to muscle during some controlled conditions.
COPD patients have decreased respiratory neuromuscular efficiency (reduced tidal volume with respect to diaphragm EMG output) with moderate exercise intensity and decreased peripheral neuromuscular efficiency (relationship between power output and vastus lateralis EMG) with just light exercise intensity [20]. Calatayud et al. [21] investigated the acute symptomatic and neuromuscular responses to increased elastic resistance exercise in 14 patients (9 male) with COPD. Neuromuscular activity was recorded during knee extensions against graded elastic resistances using sEMG for separate quadriceps muscles, together with the rate of perceived exertion, perceived quadriceps fatigue, dyspnea, oxygen saturation, and heart rate (HR). In most cases, at least a two-level resistance increase was needed to obtain a significant normalized root-mean-square increase during knee extensions. In some cases, EMG may not reflect minute changes in muscle function, such as the degree of activation or decreased oxidative capacity [36].
In summary, sEMG recording records the electrical activation of limb muscles while supporting clinical assessment and management of patients with chronic respiratory disease [78]. Standardizing the acquisition and presentation of limb muscle sEMG outcomes can be a challenge when reporting details of the applied hardware and software methods. Because sEMG is dynamic, guidelines should be established on how best to assess the reliability of recordings, thereby establishing the optimum variables and cutoff values that indicate relevant clinical changes. In doing so, sEMG can facilitate formulating a personalized training program.
2.2. Isokinetic vs. Isometric Dynamometry for Quantifying Skeletal Muscle Dysfunction: Strengths, Limitations
Isokinetic dynamometry:
Isokinetic dynamometry is often regarded as the “gold standard” for measuring muscle strength and power in both orthopedic and neurological patient populations [38]. It assesses muscle strength by measuring maximal torque or force generated during a dynamic contraction at a constant angular velocity. Compared to isometric dynamometry, it provides a more comprehensive evaluation of endurance and dynamic strength across a scope of motions and velocities [36,37,38]. The review by Bohannon et al. [37] found that, in general, reliability coefficients reported for isokinetic measurements in COPD were high yet were limited to test–retest reliability and derived from studies with fewer than 15 participants. These limitations impaired the ability to establish meaningful goals and interpret changes in patient performance over time.
Typically, isokinetic measurements are performed at fixed angular velocities of 60° to 90° [88]. Evaluation of dynamic muscle strength has relatively high reliability, while evaluation of static muscle strength is of moderate to high reliability [39,88]. Saey et al. [39] found that a 30-maximum repetition isokinetic muscle endurance test could be performed in a reliable fashion in sedentary patients with moderate to severe COPD and similar body composition, particularly at 90° per second. While isokinetic peak torque (Tq) and total muscle work were reliable at angular velocities of 90° and 180° per second, test–retest measurements of work slope and fatigue index (FI) were only reproducible at 90° per second. Meanwhile, changes in dyspnea and leg fatigue perception scores failed to achieve acceptable test–retest reproducibility, regardless of the velocity applied. Saey et al. [39] recommended the development of endurance muscle testing in patients with COPD, an area for which no standardized guidelines are available.
Isokinetic dynamometry has been used to determine muscle fiber distribution as slower velocities indicate type I fibers and faster velocities emphasize type II fibers. In a murine study, Kupa et al. [89] compared surface-detected EMG median frequency and conduction velocity (CV) variables with histochemical characterization of muscle fiber-type composition and CSA. EMG signals were recorded during tetanic contractions from different muscles. Muscles with faster glycolytic fibers exhibited higher initial values and more reduction in MF and CV during contraction. Fiber-type composition could be predicted based on MF parameters. Nevertheless, multiple factors other than fiber composition influence fiber type. Moreno-Justicia et al. [90] applied transcriptomic and proteomic workflows to single myofibers from human vastus lateralis in patients with nemaline myopathy. They identified metabolic, ribosomal, and cell junction proteins, as well as myosin heavy chain isoforms, as sources of variation between myofibers. They did not, however, study individuals with chronic lung disease.
Amaral et al. [91] described the contribution of mechanical and physiological factors to torque generation as being additionally represented by the maximum work repetition number, work fatigue percentage, and angle of peak torque. They suggested that maximum work should be employed to characterize torque generation capacity assessments. Alt et al. [92] evaluated the effects of angular velocity and training status on dynamic control equilibrium, a modification of the quotient of maximal eccentric hamstring and maximal concentric quadriceps moments in 58 trained and 58 untrained male participants. Higher DRCe moments and angles were associated with an increased capacity to resist high eccentric knee flexor moments, particularly during rapid knee extensions. Employing such an approach has clinical potential in patients with chronic lung disease to compare changes in limb muscle imbalance before and after pulmonary rehabilitation. As can be seen, the variability of which functional indices are assessed calls for standardization in clinical application.
In summary, patients with COPD and ILD exhibit reductions in maximum torque and power and increased fatiguability [3,22,23,24,45]. From a clinical standpoint, isokinetic quadriceps strength associates with functional outcomes such as stair climbing power, STS, timed-up-and-go, gait performance, and six-minute walk distance [24,25,40]. Addition-ally, isokinetic testing exhibits gender-related differences in thigh muscle strength for COPD patients, with females showing an increased tendency for decreased thigh muscle strength [93]. Increases in strength following neuromuscular electrical stimulation, whole body exercises, and resistance training consistently follow interventions [23,46]. Additional research is required to create guidelines for standardized metrics which should enable isokinetic testing to be increasingly clinically applicable [39].
bIsometric dynamometry:
Isometric dynamometry measures the maximum force generated against resistance at a fixed muscle length and joint angle. It is typically conducted with hydraulic resistance devices or force transducer platforms adapted to weight machines [39]. While more accessible for clinical settings, it provides limited insight into dynamic muscle function or endurance [41]. Testing at a 90° knee angle is recommended for quadriceps strength assessment [26,47,48]. Handheld dynamometry (isometric) is another reliable method of measuring elbow flexor and knee extensor strength for patients with ILD [48].
3. Reversing Physiological Changes Through Pulmonary Rehabilitation (PR)
Pulmonary rehabilitation (PR) is a multi-faceted intervention that utilizes exercise training as a central therapeutic modality. Individually tailored exercise programs encompass both resistance and endurance training. They improve quality of life and functional capacity in both COPD and ILD [1,49,50,51,94]. Dowman et al. [49] found that participants with idiopathic pulmonary fibrosis (IPF) exhibited improvements in six-minute walk test results, maximum exercise capacity, dyspnea, and health-related quality of life. The increase in the 6MWT was similar among participants with IPF (37 m) and other forms of ILD (40 m in all individuals) and exceeded the minimal clinically significant difference for the 6MWT in people with IPF (29 m to 34 m) [95].
Exercise increases energy demand with the production of myokines and metabolic intermediates such as lactate. This leads to benefits including improved insulin sensitivity, which is potentially important in COPD patients who receive glucocorticoids for disease control. Mechanical loading during exercise attenuates a loss of muscle mass and function [96]. Mechanotransducers and other stress-signaling compounds promote skeletal muscle adaptation in response to exercise [97,98].
While measuring quadriceps muscular strength is recommended in COPD during a pulmonary rehabilitation program, the instruments for assessing quadriceps maximal voluntary contraction (QMVC), and the clinical relevance of the results for a given patient need further refining. Vaidya et al. [99] evaluated the minimal important difference (MID) of QMVC using fixed handheld dynamometry in 157 COPD patients (mean FEV1 [forced expiratory volume] 47% predicted). They found that simple QMVC evaluation using a fixed dynamometer is reliable for depicting improvement of quadriceps muscle strength by the end of a PR program. Similarly, Bui et al. [41] aimed to validate the test–retest reliability of an isometric maximal voluntary contraction (iMVC) testing protocol in 31 individuals with COPD (mean FEV1 52% predicted) using a commercially available handheld dynamometer on two separate days. They found an intra-class correlation coefficient of 0.96, a mean variation of 0.7% between the two visits, and a mean of the difference of 1.6% between visits, concluding that standardized handheld quadriceps dynamometry is a reliable tool to assess iMVC in people with COPD.
Changes in contractile activity induce remodeling of biochemical, metabolic, and force-generating properties [100]. The transcriptional response to acute exercise reverts to baseline within hours to days, with significant variations amongst individual genes, highlighting the importance of patients with chronic lung disease maintaining a consistent program during pulmonary rehabilitation. Various factors modify the response of skeletal muscle to exercise, including training strategies, age, or sex. Resistance exercise (RE) is characterized by high intensity and short duration, and promotes the synthesis of contractile and structural proteins, leading to muscle hypertrophy [101,102]. In summary, numerous signals, sensors, regulators, and effectors are involved in these adaptive processes. Mechanisms underlying signal integration, output coordination, and other complex traits of muscle adaptation need further elucidation.
In a small pilot study, Grandio et al. [52] found that an 8-week PR program resulted in less quadriceps stimulation to generate the same torque as pre-PR (Table 1). These changes aligned with an improvement in quality-of-life scores and survival. Patients with pulmonary fibrosis who exhibited increased physical performance during PR exhibit improved survival [53]. Both resistance and endurance training improve quadriceps muscle function in patients with COPD [54]. Endurance, but not resistance training, resulted in a decrease in the proportion of glycolytic type IIa muscle fibers and phosphofructokinase content in muscle protein, and an increase in citrate synthase. Functional performance declined after 3 months of PR and was associated with reversal of such changes in muscle properties. Some pulmonary rehabilitation programs incorporate eccentric resistance training to counteract this decline [55]. Vaes et al. [27] found a positive relationship between quadriceps endurance and strength and exercise performance in COPD patients by measuring peak oxygen use (VO_2_) and walking distance in patients (Table 1). While both factors contributed to exercise intolerance, endurance was a stronger predictor of exercise capacity than quadriceps strength. Additionally, quadriceps function was more strongly related to peak VO_2_ than 6MWT [27].
While respiratory and limb muscle dysfunction exhibit similar alterations, the diaphragm exhibits greater fatigue resistance with a predominance of slow-twitch muscle fibers in contrast to limb muscles which possess relatively more glycolytic type 2 fibers. Both muscle groups are subject to oxidative and mitochondrial stress, the activation of proteolytic enzymes, and increased inflammatory mediators [1,16,28,42,56,103,104,105]. Respiratory muscles adapt with fast-to-slow fiber shifts with greater oxidative capacity, while lower limb muscles adapt with atrophy, fat infiltration, and slow-to-fast muscle fiber shifts [29,30,31,32,33,34,105]. As such, factors that improve ventilation and limb muscle function must be layered together. Muscle injury can be prevented through the appropriate use of bronchodilation, oxygen supplementation, and assisted ventilation; muscle regeneration can be facilitated through endurance training [106,107].
Many PR programs incorporate nutritional counseling to address muscle wasting and malnutrition. Nutritional supplementation focuses on optimizing protein intake and addresses nutrient deficiencies to facilitate muscle repair and growth [108]. While supplements such as creatine improve exercise capacity in healthy people, they have not shown clear improvements in COPD patients [109]. Supplements like L-carnitine, involved in fatty acid oxidation in mitochondria, benefit athletes but show only modest improvements in COPD patients. Anabolic drugs, including testosterone, oxandrolone, selective androgenic receptor modulators, or growth hormone, have positive effects on muscle mass, but no clear functional benefits [108]. Other supplements have shown promise [109,110], but clinical trials are needed for confirmation.
4. Quality and Strength of Review and Meta-Analysis Papers Discussed
The analytical rigor utilized in the meta-analyses and systematic reviews discussed herein varies. In general, limitations amongst systematic reviews include differences amongst training protocols, outcome definitions, small sample sizes, and an incomplete blinding of outcome assessments (Table 1). For example, the systematic review of van der Woude discussing isokinetic dynamometry in the evaluation of muscle strength and power was comprehensive and utilized the PubMed, Cumulative Index of Nursing and Al-lied Health (CINAHL), and Embase electronic databases. First, they assessed the methodological quality of the studies according to the Consensus-Based Standards for the Selection of Health Measurement Instruments guidelines (COSMIN) (Van Der Woude et al., 2022) [38]. Next, the authors determined the methodological quality and combined the quality of measurement properties of the studies to obtain a best-evidence synthesis. Their study was limited, however, to patients with neuromuscular disorders (NMDs) and did not include patients with chronic lung disease.
Bohannon [37] conducted a search of isokinetic testing procedures in older adults with COPD, identifying 27 suitable articles. Only one bibliographic database (PubMed) of note was searched. A wider search may have provided more evidence for the conclusions presented and allowed for a meta-analysis of some variables and for a quality grading of the included articles. In addition, only a single examiner (the author) conducted the literature search. The review of pulmonary rehabilitation in individuals with ILD by Dowman et al. [49] incorporated a pooled quantitative analysis of clinically homogeneous trials and a fixed-effect or random effects model depending on an assessment of heterogeneity using the Chi2 test and the I2 statistic. They utilized multiple search engines, identifying 21 eligible studies comparing pulmonary rehabilitation (yes or no) or sham control among people with a variety of ILDs.
The meta-analysis of Li et al. [51] pooled data using mean and standardized mean differences (SMDs) with subgroup analyses based on the type of training modality (Table 1 in ref. [51]). A random-effects model was used for analysis. The authors used the percentage of variation (I2 statistic) to assess heterogeneity across studies. Sensitivity analyses were conducted to assess the source of heterogeneity based on the intervention program characteristics of the participants when subgroup analysis could not determine the source of heterogeneity. The quality of methodology of randomized control trials was assessed using the physiotherapy evidence database (PEDro) scale, which includes 11 items with 10 scores with higher scores indicating better quality.
By contrast, the review of diagnostic and therapeutic approaches for limb and respiratory dysfunction in COPD by Barrio and Gea et al. [4,6] does not describe selection methods nor provide a quality assessment of the studies reviewed. A targeted literature review of the molecular and structural changes in the skeletal muscle of COPD patients by the same group [111] exhibits the same limitations. Jaitovich et al. [42] reviewed the mechanistic aspects of muscle dysfunction in patients with COPD, utilizing more than 200 references to describe mitochondrial metabolic dysfunction. The authors integrated biomolecular and metabolic aspects of muscle wasting with various limb training and PR programs employed to reverse muscle weakness and improve quality of life. There was no discussion of between-study heterogeneity or a comparison of molecular techniques amongst different in vitro studies.
Gosker et al. [31] screened electronic databases to find studies in which quadriceps fiber-type proportions were determined in patients with COPD. PubMed, EMBASE, and the Cochrane Library were searched using various terms relevant to muscle fiber types, myosin heavy chains, and COPD. Online abstracts of relevant conferences were also screened from the American Thoracic and European Respiratory Societies. From the selected reports, fiber-type composition, and respiratory function data were extracted and age-matched with healthy control groups of the selected COPD-related papers.
An excellent review of the state of the field by Maltais et al. [1] provides an update of the current scientific and clinical knowledge on the topic and provides guidance for future research directions. A librarian was consulted to perform a search of the literature using PubMed, Embase, and CINAHL, incorporating several terms relevant to chronic lung disease and muscle strength, wasting, and oxidative stress. The authors also ensured that the methodological process was consistent with the approved methodology of the American Thoracic Society documents development and implementation committee.
A number of small interventional pilot studies should be interpreted cautiously be-cause of limited power and potential type II error [18,52,54,55].
5. Future Considerations for Investigation
Further investigation on mitochondrial remodeling and mechanisms linked to hypoxia, oxidative stress, and mitochondrial biogenesis failure would be useful to identify antioxidant or mitochondrial-targeted therapies. There is a need to clarify anabolic resistance and cortisol/testosterone imbalances as they relate to sex to inform hormone-based trials. Electrical stimulation and pharmacologic modulators to promote type I fiber regeneration should be further explored.
Studies involving EMG and isokinetic/isometric monitoring would be key in defining signal thresholds as they relate to PR. An area of interest would be to compare the ratio of quadriceps peak EMG signal to the torque produced during knee extensions during isokinetic dynamometry in patients with COPD and those with restrictive disorders [52]. One would expect a higher ratio in COPD because of the greater diaphragm force generation required to overcome air trapping and the shorter resting length of diaphragm fibers. As respiratory pressures are related to lung volume, one would also expect a high ratio in ILD patients.
Magnetic resonance imaging (MRI) or NIRS can be paired with EMG and dynamometry to visualize intramuscular oxygen concentration and microvascular changes. Assessment of PR components may identify methods to sustain PR benefits beyond three months. Studies of dietary supplementation to enhance strength, endurance, and survival outcomes would facilitate the individual personalization and tailoring of programs.
Shear wave ultrasound elastography (UE) has the potential to assess muscle dysfunction in ILD and COPD by measuring muscle stiffness and elasticity. Strain elastography (SE), acoustic radiation force impulse (ARFI) technology, and shear wave elastography (SWE) are the three main UE methods [111,112,113,114]. UE should be considered to assess structural changes in limb muscle before and after PR.
The study of environmental factors such as smoking, vaping, and exposure to particulate matter may reveal their effects on ncRNAs synthesis. Future research can be directed to (1) determine whether ncRNAs can become new therapeutic targets or diagnostic markers; (2) assess whether ncRNAs provide a means for optimizing rehabilitative management of muscular atrophy in individuals with chronic lung disease; and (3) generate the development of novel and effective nutritional supplements, drugs, and targeted therapy in such patients [67].
Clarifying molecular pathways leads to new drug targets to prevent muscle wasting. ncRNAs have the potential to become new biomarkers as diagnostic tools and therapeutic targets for muscle atrophy in patients with COPD and ILD, including those with CTD-ILD. Identifying novel ncRNA species, investigating their targets and specific mechanisms of action can provide information regarding the regulatory roles of ncRNAs in muscle atrophy, which may allow drug development targeting the expression and activity of disease-related ncRNAs [67,68,69,70].
An intriguing avenue for investigation is the potential use of the mTOR inhibitor FK506 in the prevention and reversal of muscle atrophy associated with chronic wasting diseases [115], including COPD and ILD. In cachectic tumor-bearing mice, FK506 pre-vents muscle and body weight loss and protects from neuromuscular junction alteration by inhibiting the intracellular FK506 binding protein 12 (FKBP12), an immunophilin that limits and prevents uncontrolled activation of bone morphogenetic protein (BMP) signaling by binding the cytoplasmic domain of the type I BMP receptor [115]. To further elucidate the impact of FK506 treatment on COPD or ILD-induced cachexia (as it is applied in cancer models), employing the agent in animal models of emphysema or pulmonary fibrosis should be considered as a next step, followed by human trials (if animal studies are promising).
Given that structural changes occurring with chronic lung disease mimic events in aging (4 Barreiro, Gea), such as telomere attrition, inflammation, and mitochondrial dysfunction [116], stem cells may serve as a replacement for atrophic myocytes. Muscle stem cells are needed for regenerating skeletal muscle under resting conditions, during which they remain quiescent. During regeneration after injury (mitochondrial and oxidative damage), they become activated, begin to proliferate, and can differentiate into muscle fibers or replenish the stem cell pool [117]. In a murine model, Kang et al. [118] recently reported an increase in the expression of the tumor suppressor gene N-myc downregulated gene (Ndrg1), which encodes a protein that represses downstream the P13K-AKT-mTOR pathway. The authors propose that molecular changes associated with cellular aging may compensate for drivers of age-related decline. Such an approach can be considered potentially useful in individuals who have healthy lungs, i.e., those who have received lung transplantation.
As mitochondrial dysfunction is a major contributing mechanism to skeletal muscle atrophy, exercise, mitochondria-targeted antioxidants, and the use of Peroxisome Proliferator-Activated Receptor Gamma Coactivator 1 via in vivo transfection are potential areas of investigation for therapeutic strategies in skeletal muscle atrophy. Mitochondrial transplantation is another potential consideration for skeletal muscle atrophy in chronic lung disorders [66].
Identifying mechanisms that mediate the adaptive response to exercise has the potential to uncover molecular targets to facilitate the design of new compounds to manage muscle dysfunction and atrophy in chronic respiratory disease. Several signaling, epigenetic, and transcriptional compounds involved in the adaptive response to exercise have been pharmacologically employed in proof-of-concept studies [96,97,98].
6. Summary and Conclusions
Skeletal muscle dysfunction, common in patients with COPD, ILD, and post-transplant patients, is systemic and reversible. Patients experience global atrophy and a shift from type I to type II fibers, with decreased capillarization and increased mitochondrial dysfunction. ILD patients experience increased fat infiltration and exercise tolerance while post-lung transplant patients experience increased muscle weakness from prolonged immobility, immunosuppressant toxicity, and metabolic changes. Additional adverse factors include medications (e.g., glucocorticoids), systemic inflammation, hormonal imbalance, and physical inactivity. Atrophy is a consequence of altered balance between protein synthesis and degradation. Technologies grounded in principles of cell biomechanics such as EMG, muscle strength testing, ultrasound elastography, magnetic resonance elastography, along with cellular and molecular biology techniques are utilized to detect and assess muscle atrophy. Integrating clinical diagnostic methods with these tools enhances diagnostic accuracy and treatment efficacy. While isometric tools are typically used for the assessment of limb muscle dysfunction, isokinetic testing better reflects endurance and daily activities.
PR should include a combination of resistance, endurance, and eccentric training to increase strength and quality of life and decrease dyspnea. Programs should be tailored to fit unique patient needs. Nutrition is critical to ensure the patient is adequately fueled. Clinical trials should confirm the benefits of selected supplements.
Avoidance of disease-accelerating environmental factors (such as pollution, stress, sedentary lifestyles, and unhealthy diets), the application of health-promoting lifestyle factors (such as diet, exercise, regular sleeping patterns, and social activities), the administration of relatively non-specific agents with multiple effects (such as MTORC1 inhibitors), or specific medical interventions should contribute to maintenance of muscle, as well as lung health.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Maltais F. Decramer M. Casaburi R. Barreiro E. Burelle Y. DebigaréR. Dekhuijzen P.N.R. Franssen F. Gayan-Ramirez G. Gea J. An Official American Thoracic Society/European Respiratory Society Statement: Update on Limb Muscle Dysfunction in Chronic Obstructive Pulmonary Disease Am. J. Respir. Crit. Care Med.2014189 e 15e 6210.1164/rccm.201402-0373 ST 24787074 PMC 4098112 · doi ↗ · pubmed ↗
- 2Hussain S. Cheol K. Mofarrahi M. Skeletal Muscle Dysfunction in Patients with Chronic Obstructive Pulmonary Disease Int. J. COPD 2008363765810.2147/COPD.S 448019281080 PMC 2650609 · doi ↗ · pubmed ↗
- 3Stoffels A.A.F. Allard N.A.E. Spruit M.A. Klijn P. Hopman M.T.E. Meys R. Franssen F.M.E. Timmers S. Van Den Borst B. Van Hees H.W.H. Relationship between Volitional and Non-Volitional Quadriceps Muscle Endurance in Patients with Chronic Obstructive Pulmonary Disease Diagnostics 20241419010.3390/diagnostics 1402019038248067 PMC 10814454 · doi ↗ · pubmed ↗
- 4Barreiro E. Gea J. Respiratory and Limb Muscle Dysfunction in COPDCOPD J. Chronic Obstr. Pulm. Dis.20151241342610.3109/15412555.2014.97473725438125 · doi ↗ · pubmed ↗
- 5Mathur S. Brooks D. Carvalho C.R.F. Structural Alterations of Skeletal Muscle in Copd Front. Physiol.2014510410.3389/fphys.2014.0010424678302 PMC 3958732 · doi ↗ · pubmed ↗
- 6Gea J. Pascual S. Casadevall C. Orozco-Levi M. Barreiro E. Muscle Dysfunction in Chronic Obstructive Pulmonary Disease: Update on Causes and Biological Findings J. Thorac. Dis.20157 E 418E 43810.3978/j.issn.2072-1439.2015.08.0426623119 PMC 4635259 · doi ↗ · pubmed ↗
- 7Fiaccadori E. Del Canale S. Vitali P. Coffrini E. Ronda N. Guariglia A. Skeletal Muscle Energetics, Acid-Base Equilibrium and Lactate Metabolism in Patients with Severe Hypercapnia and Hypoxemia Chest 19879288388710.1378/chest.92.5.8833665604 · doi ↗ · pubmed ↗
- 8Jakobsson P. Jorfeldt L. Brundin A. Skeletal Muscle Metabolites and Fibre Types in Patients with Advanced Chronic Obstructive Pulmonary Disease (COPD), with and without Chronic Respiratory Failure Eur. Respir. J.1990319219610.1183/09031936.93.030201922311744 · doi ↗ · pubmed ↗