Prevalence and Risk Factors of Acute Pancreatitis in Childhood Acute Leukemia
Kamonluk Thepuatrakul, Atchariya Chanpong, Natsaruth Songthawee, Pornpun Sripornsawan, Sirinthip Kittivisuit, Hansa Sriphongphankul, Thirachit Chotsampancharoen

TL;DR
This study finds that acute pancreatitis occurs in 2.8% of children with acute leukemia and is linked to higher mortality and specific treatment factors.
Contribution
The study identifies T-cell leukemia subtype and high-dose L-asparaginase chemotherapy as risk factors for acute pancreatitis in pediatric leukemia patients.
Findings
Acute pancreatitis occurred in 2.8% of 618 leukemia patients.
Higher mortality and treatment complications were observed in patients with AP.
High L-asparaginase doses and T-cell leukemia were significant risk factors.
Abstract
Acute pancreatitis (AP) is a rare but serious complication in children receiving treatment for acute leukemia. We retrospectively reviewed cases from 2004 to 2024 at Songklanagarind Hospital to determine prevalence, risk factors, and outcomes. Among 618 patients, 17 (2.8%) were diagnosed with AP, which was more common in patients with T-cell leukemia and in those receiving high- to very-high-risk chemotherapy. Compared with patients without AP, those with AP required more imaging studies, prolonged fasting, and greater intravenous fluid support. Overall mortality was significantly higher in the AP group. An increased AP risk was associated with the use of high- to very-high-risk treatment protocols and a cumulative L-asparaginase dose ≥55,200 IU/m2. Three patients received L-asparaginase after AP resolved; all were high- to very-high-risk cases, and one developed persistent AP with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
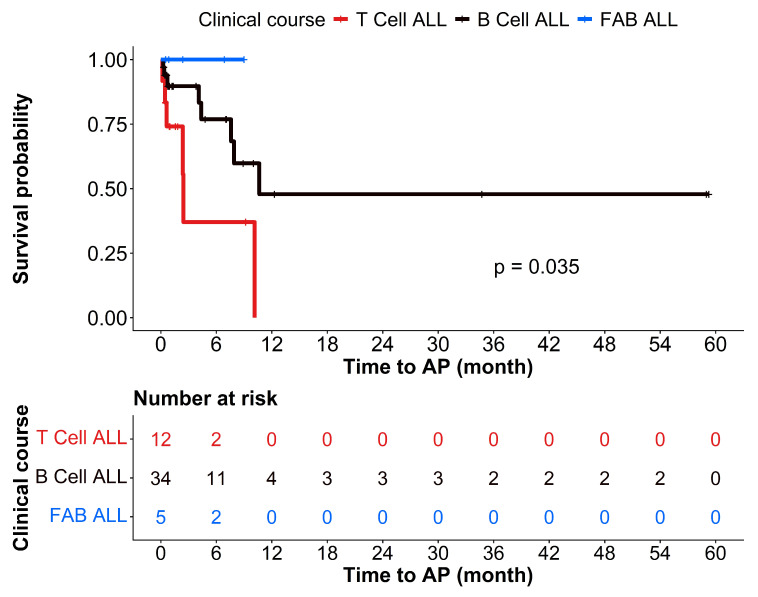 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatitis Pathology and Treatment · Acute Lymphoblastic Leukemia research · Gallbladder and Bile Duct Disorders
1. Introduction
Acute leukemia is the most common childhood malignancy, with survival rates of 80–90% in many settings [1]. Treatment-related complications are among the major contributors to morbidity and mortality worldwide. Acute pancreatitis (AP) remains an important complication in pediatric oncology [2,3]. AP diagnosis is established based on the presence of characteristic abdominal pain, increased serum pancreatic enzyme levels, and supportive findings on imaging studies [4].
The pathophysiology of AP involves the premature activation of pancreatic digestive enzymes (particularly trypsin) within acinar cells, leading to autodigestion, local inflammation, vascular injury, and, in severe cases, systemic inflammatory responses [3]. Chemotherapy used in pediatric oncology may cause direct acinar toxicity, hypersensitivity reactions, mitochondrial injury, or metabolic disturbances, such as dyslipidemia, which could increase the risk of pancreatitis [5]. Patients may present with a range of clinical manifestations, from minor abdominal pain to multi-organ involvement [6].
The reported incidence of AP during leukemia therapy varies from 2.3% to 18% in international cohorts [2,7,8,9,10,11]. Direct mortality is relatively low; however, AP has the potential to seriously impede leukemia treatment by necessitating the postponement or permanent discontinuation of vital chemotherapeutic agents, which can increase the chance of relapse [2,9,12]. Children affected by AP can develop acute or chronic complications such as insulin dependence and pancreatic pseudocysts [2]. Older age and intensity of treatment have been reported as predictors of worsening outcomes [2,9,10,12].
However, most current evidence is derived from Western studies. In Thailand, available and up-to-date data are relatively limited, with few reports originating from the central region [10]. Notably, there is a paucity of data on AP in pediatric leukemia cases in Thailand, particularly in Southern Thailand, where toxicity profiles may be influenced by access to healthcare, demographics, and updated chemotherapy protocols. Substantial regional gaps in knowledge remain; accordingly, in this study, we sought to examine the epidemiology and clinical course of AP in children undergoing treatment for acute leukemia.
The aim of this study was to determine the incidence of AP in children treated for acute leukemia, identify associated risk factors, and evaluate their impact on treatment outcomes and overall survival.
2. Materials and Methods
Medical records of children ≤15 years old, diagnosed with acute leukemia at Songklanagarind Hospital between 2004 and 2024, were retrospectively reviewed. Pediatric patients diagnosed with acute leukemia who presented with acute abdominal pain thought to be caused by AP were included. To ensure the diagnosis of AP, the patient’s clinical history, laboratory tests, and imaging examinations were reviewed. This study was approved by the Ethics Committee of the Faculty of Medicine, Prince of Songkla University (REC. 59-107-01-1). The requirement for informed consent was waived owing to the retrospective nature of the study and use of de-identified data.
2.1. Data Collection and Definitions
Demographic data, clinical manifestations, diagnosis, clinical course of acute leukemia, previous investigations, medications administered, particularly chemotherapy, and outcomes were collected. The cumulative dose of L-asparaginase was defined as the total administered dose per body surface area (BSA), calculated from treatment initiation until the onset of abdominal pain. The cumulative dose was manually calculated based on the most recent BSA, using the measurement closest to the onset of abdominal pain, and the same method was applied to all patients. Fluids in the first 48 h referred to the total intravenous fluid requirement within 48 h after presentation with abdominal pain. Diagnostic amylase and lipase levels refer to the serum levels measured at the time of presentation with abdominal pain, whereas peak levels represent the maximum amylase and lipase concentrations observed during pain episodes.
AP was diagnosed according to the Atlanta criteria, as modified by the INSPPIRE group for pediatric patients [13,14]. The diagnosis required the presence of at least two of the following three criteria:
- -Abdominal symptoms consistent with acute pancreatitis;
- -Serum amylase or lipase levels elevated to at least three times the upper limit of normal;
- -Imaging evidence of acute pancreatitis on ultrasonography (USG), computed tomography (CT), or magnetic resonance imaging (MRI).
Wondmeneh TG et al. reported that the severity of acute pancreatitis was graded according to version 6.0 of the Common Terminology Criteria for Adverse Events (CTCAE v.6.0) as follows [15,16]:
- -Grade 1: No specific definition provided.
- -Grade 2: Elevated levels of pancreatic enzymes or abnormalities detected only on imaging.
- -Grade 3: Severe abdominal pain and vomiting; medical intervention indicated (e.g., analgesia, nutritional support).
- -Grade 4: Life-threatening consequences; urgent intervention required.
- -Grade 5: Death.
2.2. Chemotherapy Protocols
For patients with acute lymphoblastic leukemia (ALL) treated between 2004 and 2005, chemotherapy protocols were based on the Children’s Cancer Study Group (CCG) criteria, including CCG-104, CCG-105, and CCG-106 for patients with good, intermediate, and poor prognosis, respectively [17,18,19,20]. Between 2006 and 2013, the Thai national protocol, including ALL-01-05, ALL-02-05, and ALL VHR-08 were implemented for patients with standard-, high-, and very high-risk ALL, respectively [19,21,22]. Notably, the latest version of the Thai national protocol, modified from the Children’s Oncology Group (COG)-AALL00P2 and COG-AALL0232 regimens, was used between 2014 and 2024. These included ALL 1301, ALL 1302, and ALL 1303 for patients with standard-, high-, and very high-risk ALL, respectively [19,23]. Notably, the risk stratification at presentation was determined according to the National Cancer Institute risk group classification [19,24,25].
For patients with acute myeloid leukemia (AML), those treated before 2007 received the AML–Berlin–Frankfurt–Munster (BFM)-83 protocol, whereas patients treated between 2008 and 2013 received the AML-BFM-98 protocol [26,27,28]. Between 2014 and 2024, patients with AML were treated using the Thai national protocol adapted from the COG, using AML-1301 and AML-1302 for standard-risk and high-risk AML, respectively [27,29,30].
All patients received native L-asparaginase because it was the only formulation available at our institution.
2.3. Statistical Analysis
All analyses were conducted using R (version 4.4.3; R Foundation for Statistical Computing, Vienna, Austria). Baseline characteristics are reported as median (interquartile range [IQR]), mean ± standard deviation (SD), or number (percentage), as appropriate. Continuous and categorical variables were compared using Fisher’s exact test, the Mann–Whitney U test, or the Kruskal–Wallis test, as applicable.
Univariable and multivariable logistic regression analyses were performed to examine associations between potential risk factors and AP diagnosis. Variables with a p value < 0.2 in the univariable analysis were included in the multivariable model. Logistic regression results are presented as odds ratios (ORs) with 95% confidence intervals (CIs). Variance inflation factors were calculated to assess multicollinearity among the variables in the multivariable models.
Receiver operating characteristic (ROC) curve analysis was used to evaluate the diagnostic accuracy of continuous variables. Kaplan–Meier survival analysis was applied to estimate the time to AP occurrence across different leukemia subtypes. p < 0.05 was considered statistically significant.
3. Results
3.1. Patient Characteristics
Of the 853 children referred to Songklanagarind Hospital and diagnosed with acute leukemia, 618 were treated with chemotherapy and followed up at our center; 50.6% had B-cell ALL, 10.0% had T-cell ALL, 12.9% had French–American–British-classified acute lymphoblastic leukemia (FAB-ALL), and 26.4% had AML. Among the 618 children, 70 were evaluated for suspected AP (presenting with abdominal pain), of whom 17 were diagnosed with AP, representing 24.3% of patients who presented with abdominal pain. Of the 17 patients with AP, 6 had T-cell ALL, 8 had B-cell ALL, 3 had AML, and none had FAB-ALL. The overall AP prevalence was 2.8%. Among the 17 AP cases, the majority (65%) were classified as moderate to severe (CTCAE grades 3–5) pancreatitis, and three patients died because of the AP episode.
There were no significant differences in the baseline characteristics (age and sex) between patients with acute leukemia with and without pancreatitis (Table 1). Children with T-cell ALL who presented with abdominal pain were more likely to develop AP than those with other types of acute leukemia (Table 1). Kaplan–Meier survival analysis showed that children with T-cell ALL were likely to develop AP earlier than other types, most commonly within the first 6–10 months of treatment (Figure 1). Children receiving high- to very-high-risk chemotherapy protocols had a significantly increased risk of developing AP when they presented with abdominal pain (p = 0.026; Table 2). In particular, children with AP tended to receive a higher dose of L-asparaginase than children without AP (64,692.5 vs. 34,483, p = 0.094; Table 2).
3.2. Clinical and Laboratory Profiles
Regarding the clinical and laboratory profiles, patients with pancreatitis presented with fewer days of abdominal pain before diagnosis (median, 1 day vs. 2 days, p = 0.031; Table 3) than those without pancreatitis. Compared with the non-AP group, the AP group showed significantly higher diagnostic and peak serum amylase and lipase levels (p < 0.001), but lower albumin levels (3.2 ± 0.9 vs. 3.7 ± 0.7 g/dL, p = 0.023). These findings are consistent with the established diagnostic criteria for AP and highlight the severity of the inflammatory process in children with AP. The approaches to requesting radiological investigations differed significantly between patients with acute leukemia with and without pancreatitis (Table 3). Imaging was performed in all patients diagnosed with AP; however, only half of the non-AP patients underwent radiologic investigation (p = 0.003; Table 3). CT revealed pancreatic swelling in 78.6% of the patients with AP who underwent the examination. USG showed peripancreatic swelling and collection in 42.9% and 28.6% of the patients with AP who underwent the scan, respectively.
3.3. The Management of Acute Pancreatitis
Regarding AP management, almost all patients with AP required nil per os (NPO) at diagnosis (82.4% vs. 24.5%, p < 0.001), and the fasting duration was longer than in those without pancreatitis (median 3 days vs. 0 days, p < 0.001; Table 3). Children with AP also required significantly higher fluid volumes in the first 48 h (5675.4 mL vs. 3271.6 mL, p = 0.003). Opioid and fentanyl requirements were higher in the AP group (Table 3). Among the 17 patients with AP, L-asparaginase was introduced in three of them after AP resolved, all of whom had grade 2 AP. Among these three patients, one subsequently developed persistent AP (walled-off necrosis) following L-asparaginase administration, requiring additional intervention. Importantly, the overall mortality rate (all-cause during follow-up) was significantly higher in the patients with AP than in those without pancreatitis (76.5% vs. 34.0%, p = 0.005).
3.4. Risk Factors of Acute Pancreatitis
Logistic regression analysis adjusted for potential confounders, including age, sex, and chemotherapy protocol, showed that using a high- to very-high-risk chemotherapy protocol was the only factor contributing to AP development in children with acute leukemia (Table 4). From the ROC analysis, the L-asparaginase accumulative dose of ≥55,200 IU/m^2^ could predict the risk of pancreatitis [Odds ratio = 5.25 (1.29, 24.67), p = 0.025] with an area under the ROC curve of 0.695 and a sensitivity of 66.67%, a specificity of 72.4%, a positive predictive value of 50.0%, and a negative predictive value of 84.0%.
Since patients with T-cell ALL may require more intensive treatment, a subgroup analysis was performed in 23 children with T-cell ALL and B-cell ALL who received comparable intensity therapy (high-risk protocol). Among patients presenting with abdominal pain suggesting AP, 16 had B-cell ALL and 7 had T-ALL. AP developed in 6 of 16 patients with B-cell ALL and in 4 of 7 patients with T-cell ALL (p = 0.796). In AP cases, the mean cumulative L-asparaginase dose tended to be higher in patients with T-cell ALL than in those with B-cell ALL, although the difference was not statistically significant (83,039 ± 75,709.6 vs. 77,799.8 ± 38,356.4 U/m^2^, p = 0.896). Furthermore, the mean interval from leukemia diagnosis to AP onset (3.9 ± 4.3 vs. 4.6 ± 4.1 months, p = 0.786) and the timing of L-asparaginase administration were also not significantly different between the two subtypes (21.0 ± 26.2 vs. 28.0 ± 35.1 days, p = 0.751).
4. Discussion
In this study, the overall prevalence of AP among children diagnosed with acute leukemia was 2.8%, which is consistent with a previously reported prevalence ranging from approximately 2.3% to 18% in pediatric ALL populations, particularly in association with asparaginase-containing chemotherapy regimens [2,7,8,9,10,11].
Importantly, children with T-cell ALL who presented with abdominal pain were more likely to develop AP than those with other leukemia subtypes. This observation aligns with those in prior studies [9,10,31] suggesting that certain treatment-related factors, such as treatment under high- to very high-risk chemotherapy protocols [9,31], as well as leukemia subtype, were associated with AP occurrence [10]. The significantly increased risk of pancreatitis highlights the importance of vigilant monitoring and early diagnostic intervention, particularly in children with T-cell ALL during the first 6–10 months of chemotherapy. We found that using high- to very high-risk chemotherapy protocols was the most significant risk factor for AP in children with acute leukemia.
Knoderer HM et al. reported that the development of pancreatitis associated with L-asparaginase is unpredictable [32] and may be related to genetic susceptibility [33]; nevertheless, we additionally proposed a cumulative L-asparaginase dose cut-off value of ≥55,200 IU/m^2^ to help predict the risk of developing AP in pediatric patients with acute leukemia. This was different from the previously reported cut-off intensity of >45,000 U/m^2^/month as a predictor of AP development [9]. Additionally, Rank CU et al. suggested that L-asparaginase reintroduction should be considered only in patients at a high risk of leukemic relapse [34]. In our study, three patients were readministered L-asparaginase after AP resolution, all of whom were receiving high- to very-high-risk chemotherapy. Only one patient developed persistent AP (walled-off necrosis) following L-asparaginase administration, which may be attributable to specific genetic risk factors [33]. However, genetic testing for predisposition to asparaginase-induced pancreatitis was not performed in this study.
From a clinical perspective, children with AP exhibit shorter durations of abdominal pain before diagnosis than those without pancreatitis. This finding may reflect the more abrupt and severe inflammatory response characteristic of pancreatitis, prompting earlier diagnostic evaluation. Consistent with established diagnostic criteria, patients with pancreatitis demonstrated significantly higher diagnostic and peak serum amylase and lipase levels, as well as hypoalbuminemia, suggesting a more intense systemic inflammatory process. Radiological evaluation plays a crucial role in confirming the diagnosis of pancreatitis. All patients diagnosed with pancreatitis underwent imaging studies, whereas only half of the non-pancreatitis group underwent radiologic investigations [4]. CT revealed pancreatic swelling in most cases of pancreatitis, while USG frequently revealed peripancreatic swelling and fluid collections. Similarly, the importance of imaging in identifying pancreatic edema, necrosis, or complications such as pseudocyst formation, particularly in severe cases, has been previously emphasized [5,35]. The significantly different imaging utilization between groups likely reflects higher clinical suspicion and disease severity in patients with pancreatitis.
Management strategies also differ substantially between patients with and without pancreatitis. Almost all patients with pancreatitis required bowel rest at diagnosis and remained on an NPO for a significantly longer duration. They also received greater volumes of intravenous fluids within the first 48 h, consistent with the guideline-recommended supportive management of AP aimed at maintaining intravascular volume and mitigating systemic inflammation. Additionally, opioid requirements were higher in the pancreatitis group, reflecting more severe abdominal pain and supporting the clinical distinction between pancreatitis-related pain and other causes of abdominal discomfort during leukemia treatment [6].
Importantly, the mortality rate was significantly higher in patients with pancreatitis than in those without. Deaths were not necessarily directly attributable to pancreatitis alone; nonetheless, this finding highlights pancreatitis as a marker of severe treatment-related toxicity and overall vulnerability in children with acute leukemia. AP could also affect continued L-asparaginase use in adequate amounts, which may increase the risk of ALL recurrence and shorten the disease-free interval [36]. Previous studies have reported pancreatitis-related mortality rates ranging from 2% to 9%, particularly in severe or necrotizing cases and in patients requiring treatment modification or asparaginase discontinuation [2,12].
This study was limited by its retrospective nature and small sample size; however, it included the largest cohort of children diagnosed with acute leukemia in Southern Thailand. Overall, our findings suggest that AP, although relatively uncommon, represents a clinically significant complication in children with acute leukemia, particularly among those receiving intensive chemotherapy regimens. Early detection of abdominal pain, prompt laboratory evaluation, and appropriate imaging are essential to ensure timely diagnosis and management. Given the association between pancreatitis and adverse outcomes, heightened vigilance is warranted in high-risk patients, especially those with T-cell ALL or receiving high-intensity treatment protocols with an accumulative L-asparaginase dose ≥55,200 IU/m^2^.
5. Conclusions
The risk factors for AP development include using high- to very-high-risk chemotherapy regimens and certain types of acute leukemia. Therefore, early diagnosis and prompt supportive care are essential to reduce complications. Further multicenter studies with larger sample sizes are needed to confirm these risk factors and improve leukemia treatment outcomes in children.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hunger S.P. Mullighan C.G. Acute Lymphoblastic Leukemia in Children N. Engl. J. Med.20153731541155210.1056/NEJ Mra 140097226465987 · doi ↗ · pubmed ↗
- 2Wolthers B.O. Frandsen T.L. Baruchel A. Attarbaschi A. Barzilai S. Colombini A. Escherich G. Grell K. Inaba H. Kovacs G. Asparaginase-Associated Pancreatitis in Childhood Acute Lymphoblastic Leukaemia: An Observational Ponte Di Legno Toxicity Working Group Study Lancet Oncol.2017181238124810.1016/S 1470-2045(17)30424-228736188 · doi ↗ · pubmed ↗
- 3Jones M.R. Hall O.M. Kaye A.M. Kaye A.D. Drug-Induced Acute Pancreatitis: A Review Ochsner J.201515455125829880 PMC 4365846 · pubmed ↗
- 4Frossard J.-L. Steer M.L. Pastor C.M. Acute Pancreatitis Lancet 200837114315210.1016/S 0140-6736(08)60107-518191686 · doi ↗ · pubmed ↗
- 5M’harzi S. Elouali A. Lahrache K. Ghanam A. Babakhouya A. Rkain M. Benajiba N. Acute Pancreatitis Following L-Asparaginase in Acute Lymphoblastic Leukemia Leuk. Res. Rep.20221810035710.1016/j.lrr.2022.10035736405565 PMC 9668613 · doi ↗ · pubmed ↗
- 6Szatmary P. Grammatikopoulos T. Cai W. Huang W. Mukherjee R. Halloran C. Beyer G. Sutton R. Acute Pancreatitis: Diagnosis and Treatment Drugs 2022821251127610.1007/s 40265-022-01766-436074322 PMC 9454414 · doi ↗ · pubmed ↗
- 7Morawiak A. Salamonowicz-Bodzioch M. Królak A. Kałwak K. Owoc-Lempach J. Kowalczyk J. Zawitkowska J. Szczepański T. Irga-Jaworska N. Adamkiewicz-Drożyńska E. Acute Pancreatitis in Pediatric Acute Lymphoblastic Leukemia (Acu PA Study): A Nationwide Survey in Poland Cancers 202416264010.3390/cancers 1615264039123368 PMC 11312082 · doi ↗ · pubmed ↗
- 8MINS. Kim H. Shin J. Suh J.K. Kang S.H. Koh K.-N. Im H.J. Seo J.J. Risk Factors of Acute Pancreatitis in Pediatric Acute Lymphoblastic Leukemia Patients: A Single-Center Experience Blood 2019134507710.1182/blood-2019-128236 · doi ↗