MEWDS-like Presentation Unmasking Sequential Bilateral Multifocal Choroiditis: Insights from Longitudinal Multimodal Imaging
Blerta Lang, Annekatrin Rickmann, Karl Thomas Boden, Stefanie Behnke, Peter Szurman

TL;DR
A patient initially diagnosed with MEWDS-like symptoms was later found to have sequential bilateral multifocal choroiditis through long-term imaging and treatment tracking.
Contribution
This case highlights longitudinal multimodal imaging's role in reclassifying MEWDS-like presentations to sequential bilateral multifocal choroiditis.
Findings
Initial MEWDS-like presentation evolved into sequential bilateral multifocal choroiditis over 4 years.
Longitudinal multimodal imaging revealed key diagnostic changes, including peripapillary inflammation and macular edema.
No choroidal neovascularization developed, avoiding anti-VEGF therapy.
Abstract
Background: Multiple evanescent white dot syndrome (MEWDS) is usually acute and self-limited, whereas multifocal choroiditis (MFC)/punctate inner choroidopathy (PIC) is relapsing; overlap can obscure early diagnosis and requires longitudinal multimodal imaging. Methods: We report a 4-year follow-up of a 31-year-old woman with fundus autofluorescence (FAF), fluorescein angiography (FA), indocyanine green angiography (ICGA), and spectral-domain optical coherence tomography (SD-OCT), plus a systemic/neurologic/rheumatologic work-up. Treatment included intravenous methylprednisolone for presumed optic neuritis, followed by topical, periocular, intravitreal, and systemic corticosteroids, later escalated to adalimumab and an intravitreal dexamethasone implant. Because foveal granularity could not be documented, baseline was termed “MEWDS-like”. Diagnostic labelling was benchmarked against…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
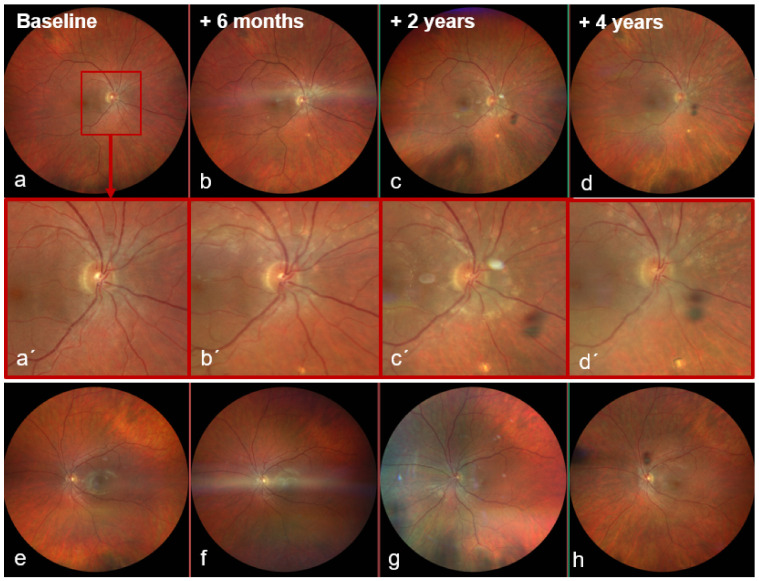 Figure 1
Figure 1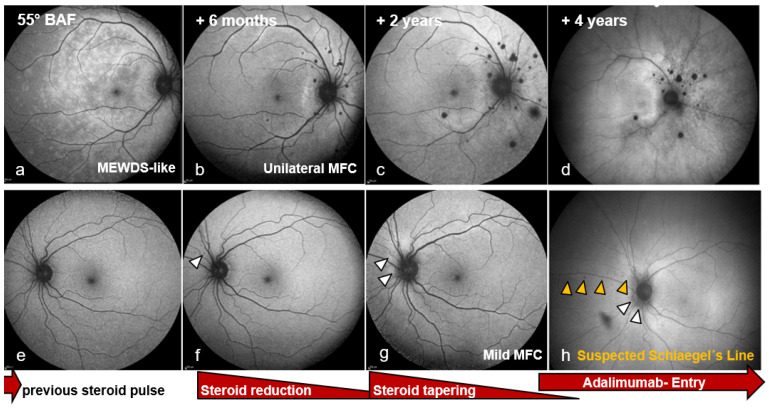 Figure 2
Figure 2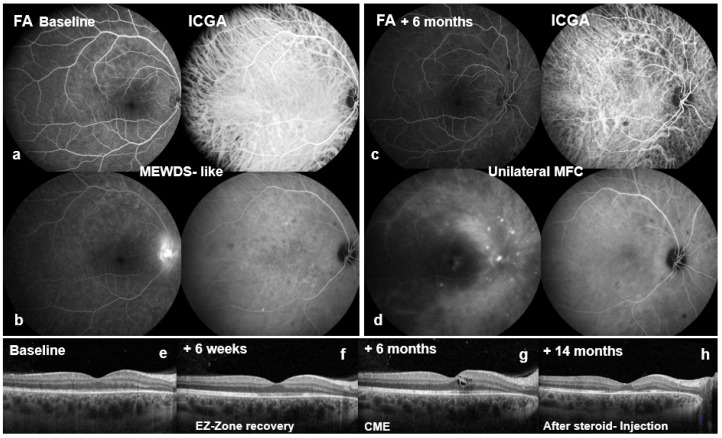 Figure 3
Figure 3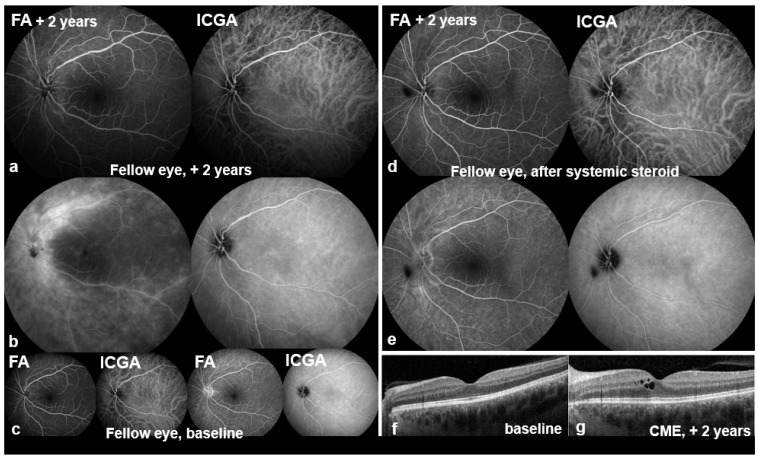 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Diseases and Behçet’s Syndrome · Ocular Oncology and Treatments · Retinal Diseases and Treatments
1. Introduction
Multiple evanescent white dot syndrome (MEWDS) is a rare, acute, self-limited outer retinal disorder (estimated incidence ~0.22 per 100,000 population/year) that typically presents unilaterally with characteristic multimodal imaging findings [1,2], whereas idiopathic multifocal choroiditis (MFC) is a chronic, relapsing choriocapillaritis/retinal pigment epithelium (RPE)-centred inflammatory chorioretinopathy that may become bilateral and cause structural complications. We report a MEWDS-like presentation that evolved into sequential bilateral MFC, underscoring diagnostic pitfalls and management implications. This report delineates a MEWDS-like baseline phenotype that was reclassified using SUN criteria during a 4-year multimodal imaging follow-up, culminating in sequential bilateral MFC and illustrating practical diagnostic “red flags” that should prompt closer monitoring and earlier steroid-sparing planning.
2. Case Report
A 31-year-old vegetarian woman was referred to ophthalmology from neurology with a provisional diagnosis of presumed retrobulbar optic neuritis after two days of stabbing right-sided headache and sudden profound visual loss in the OD. An external ophthalmologic assessment had documented marked visual acuity reduction with suspected visual field abnormalities. Pattern-reversal visual evoked potentials (VEP) showed reduced amplitudes in the OD with mildly prolonged P100 latency. During the index admission, cranial computed tomography (CT) was unremarkable and lumbar puncture showed clear cerebrospinal fluid (CSF) with 2 cells/µL. Magnetic resonance imaging (MRI) of the brain and cervical/thoracic spine showed no evidence of cerebral demyelination or other acute intracranial pathology; a faint T2-SPAIR hyperintensity at Th1/Th2 was noted, such that myelopathy could not be definitively excluded. High-dose intravenous (IV) methylprednisolone (1 g/day) had been initiated; she was on day two of a planned five-day course. The medical history included treated hypothyroidism and vitamin D/iron deficiency; two months earlier she had received a second Pfizer/BioNTech SARS-CoV-2 vaccination. No causal inference was made, and she reported no intercurrent SARS-CoV-2 infection or systemic symptoms. She otherwise took only a combined oral contraceptive.
At ophthalmic presentation, best-corrected visual acuity (BCVA) was 20/600 OD (right eye) and 20/20 OS (left eye). Intraocular pressure (IOP) measured 18 mmHg bilaterally. IOP was screened using non-contact tonometry (NIDEK) and verified with Goldmann applanation tonometry by the examining physician when clinically indicated. The anterior segment was quiet. Notably, several typical clinical features of optic neuritis were absent, including a relative afferent pupillary defect, red desaturation, pain on eye movements/retropulsion, and optic disc swelling; automated perimetry showed nonspecific defects but was unreliable in the OD due to >85% fixation losses. Dilated fundus examination was unremarkable in both eyes.
Four days into the steroid course, BCVA improved slightly to 20/400 OD, with the OS unchanged and IOP normal. It was planned that the patient would receive one further day of high-dose corticosteroids, to complete the full five-day regimen.
Colour fundus photography now showed a sharply demarcated disc and a dry macula without foveal reflex in the OD (Figure 1a), and a healthy disc and macula in the OS (Figure 1e). Multimodal imaging was performed: blue-light fundus autofluorescence (BAF, Spectralis^®^, Heidelberg Engineering GmbH, Heidelberg, Germany) of the OD showed numerous partly confluent hyperautofluorescent lesions (Figure 2a), whereas the OS displayed only two small nasal punctate hypoautofluorescent dots (Figure 2e). Early fluorescein angiography (FA) in the OD demonstrated multiple punctate, wreath-like hyperfluorescent spots—some coalescent—with late leakage and a pronounced hot disc (arm–retina transit time 19 s; Figure 3a,b). FA of the OS was normal apart from mild disc hyperfluorescence. Indocyanine green angiography (ICGA) in the OD disclosed multiple hypofluorescent choriocapillaris spots (Figure 3b,d); the OS showed only a few small nonspecific nasal hypofluorescent areas. Spectral-domain OCT (SD-OCT) revealed focal ellipsoid zone (EZ) disruption in the OD (Figure 3f), with a normal macula in the OS (Figure 4f).
Systemic and neurological investigations were initiated during the index admission. Neurological examination was normal. Infectious testing excluded HSV, VZV, HIV, tick-borne encephalitis, Borrelia spp., Mycobacterium tuberculosis, and Treponema pallidum. Aquaporin-4 and myelin oligodendrocyte glycoprotein antibodies were negative. Autoimmune and inflammatory screening showed a low-titer ANA, while ANCAs, lupus anticoagulant, and anticardiolipin antibodies were negative; ACE, soluble interleukin-2 receptor, and lysozyme were within local reference ranges, and serum protein electrophoresis was unremarkable. Owing to the low-titer ANA, the patient was referred to rheumatology at the 6-week follow-up, with no evidence of an underlying systemic rheumatologic disease. Differential diagnoses and the corresponding systemic/neurological investigations are summarized in Figure S3.
At six weeks, BCVA improved to 20/80 OD and remained 20/20 OS. The OD showed three small whitish peripapillary lesions and partial parafoveal EZ recovery on SD-OCT (Figure 3f). The acute unilateral presentation with wreath-like FA lesions and disc leakage, transient outer retinal/EZ disruption on SD-OCT, and absent anterior chamber/vitreous inflammation was consistent with key SUN classification elements for MEWDS [1]. Because foveal granularity and classic grey-white spots could not be objectively documented under the acute circumstances, the baseline phenotype was designated ‘MEWDS-like’ rather than fully classifiable MEWDS and elected close follow-up.
At six months, recurrent visual decline occurred in the OD (BCVA 20/50 OD, 20/25 OS; IOP 13 mmHg both eyes). The OD fundus examination now showed multiple ill-defined peripapillary inflammatory foci, most dense superiorly/nasally, and new cystoid macular edema (CME) (Figure 1b). BAF revealed numerous round hypoautofluorescent peripapillary lesions interspersed with hyperautofluorescent spots, a discrete patch in the papillomacular bundle, and confluent signal along the superior arcade (Figure 2b). FA showed multiple early punctate peripapillary/arcade lesions with late staining and macular leakage; ICGA again disclosed multiple hypofluorescent dots (Figure 3c,d). FA of the OS remained normal, with only mild disc hyperfluorescence; ICGA was likewise unremarkable (Figure 4c). SD-OCT confirmed CME (Figure 3g). Inflammatory CNV was specifically considered and excluded on multimodal imaging (SD-OCT and FA/ICGA); anti-VEGF therapy was not required. Based on the non-monophasic relapse, evolving multifocal peripapillary inflammatory lesions with progressive hypoautofluorescent change, OCT-confirmed CME, and persistent multifocal ICGA hypofluorescent spots, the diagnosis was revised to unilateral MFC within an MFC/PIC spectrum (Table 1; Figure S1).
Therapy was escalated with topical steroidal and non-steroidal drops, parabulbar and intravitreal triamcinolone as needed, and systemic prednisolone (60 mg/day for five days, tapered over twelve weeks to 12.5 mg). Macular edema resolved with a dry macula at 14 months (Figure 3h) but recurred intermittently. Long-acting steroid implants were initially avoided due to phakia. Steroid-induced ocular hypertension developed and was controlled with a triple-agent topical regimen (fixed dorzolamide/timolol combination (Cosopt^®^) plus brimonidine (Alphagan^®^). Immunomodulation was deferred due to pregnancy planning.
Two years after presentation, the OS became symptomatic after two months of intermittent circular photopsias. An examination showed mild vitritis, blurred disc margins, central CME, and two small dot-like superior mid-peripheral hemorrhages (Figure 1g) without macular subretinal exudation; CNV was not evident on SD-OCT or angiography. BCVA remained 20/20 and IOP was normal; OD showed no new acute activity clinically (Figure 1c,c′). OS BAF showed peripapillary hyperautofluorescence with expansion of hypoautofluorescent areas (Figure 2g). FA demonstrated marked peripapillary leakage extending along the arcades (Figure 4a,b). ICGA showed delayed peripapillary filling with nasal/superior/temporal hypofluorescent spots persisting into the late phase; choroidal vessel calibre was unchanged. SD-OCT confirmed CME (Figure 4g). Given that baseline OS FA/ICGA had been essentially normal (Figure 4c), the diagnosis was revised to bilateral MFC, consistent with a chronic relapsing inflammatory trajectory.
Systemic prednisolone induced a rapid anatomical and functional response (Figure 4d,e). Because of the relapsing course, adalimumab 40 mg subcutaneously every two weeks was commenced after twelve weeks, with prednisolone maintained at 12.5 mg daily and then tapered; additional intravitreal triamcinolone was used for recurrences.
By year four, the OD required uncomplicated cataract surgery. Under continued immunomodulation, BAF showed a stable lesion burden in the OD (Figure 2d). In the OS, BAF demonstrated multiple small peripapillary hypoautofluorescent spots forming a subtle curved line along the superior nasal arcade suggestive of an early Schlaegel line (Figure 1h and Figure 2c,f,h). Across follow-up, BCVA in the OD fluctuated between 20/50 and 20/32 in parallel with intraretinal fluid on SD-OCT; the OS remained 20/20. Due to recurrent macular edema in the OD, therapy was ultimately switched to an intravitreal dexamethasone implant. Escalation to dual systemic immunosuppression (adalimumab and methotrexate) was recommended but postponed because of pregnancy planning. No inflammatory CNV developed in either eye during the four-year follow-up. Although OCTA could have provided additional information, repeated dye angiography and structural SD-OCT were considered sufficient to exclude CNV in this case. A summarized treatment timeline is provided in Figure S2.
In summary, an initially MEWDS-like presentation in the OD evolved into unilateral MFC with recurrent CME and was subsequently declared a sequential bilateral disease with fellow-eye involvement at two years.
3. Discussion
Phenotypic overlap across white dot syndromes is well recognized, and MEWDS-like presentations may occur within a broader spectrum of inflammatory chorioretinopathies such as MFC/PIC. Sequential or overlapping MEWDS and MFC has been reported for decades, including cases in which MEWDS-like episodes precede MFC-defining lesions or occur in eyes with established MFC, sometimes followed by scarring or CNV [5,6,7,8].
To make our diagnostic labelling transparent, we benchmarked the evolving phenotype against published SUN Working Group classification criteria [1,3,4], acknowledging that these are classification rather than diagnostic criteria. In brief, MEWDS classification requires multifocal grey-white chorioretinal spots with foveal granularity plus characteristic wreath-like FA and/or typical outer retinal OCT lesions, with absent-to-mild anterior chamber/vitreous inflammation, whereas the MFC spectrum reflects true choroidal/chorioretinal inflammatory lesions that may scar, relapse, and develop structural complications (criteria mapping is summarized in Table 1 and visualized in Figure S1). At baseline, foveal granularity and classic grey-white spots were not objectively documented; therefore, we use the term “MEWDS-like”. Published MEWDS-like presentations later reclassified as MFC/PIC are summarized in Table 2; compared with prior reports, which often have shorter follow-up and limited detail on steroid-sparing escalation, our case provides a four-year multimodal imaging and treatment timeline demonstrating a phase shift to chronic-relapsing sequential bilateral MFC, including escalation to adalimumab and an intravitreal dexamethasone implant for recurrent CME.
Consistent with the masquerader framework, Russell et al. emphasized that hyperautofluorescent outer retinal lesions and EZ disruption are not pathognomonic and should prompt caution when the course deviates from the classic self-limited, monophasic pattern [10]. Our case illustrates this: early features were compatible with a MEWDS-like phenotype, yet relapse at six months with evolving peripapillary inflammatory foci and recurrent CME, followed by fellow-eye involvement with vitritis and peripapillary leakage, favoured an MFC/PIC-spectrum trajectory. Similar MEWDS-mimicking patterns in MFC/PIC have been reported, supporting the concept of secondary MEWDS-like reactions within an inflammatory chorioretinopathy rather than a strictly self-limited entity [13].
Sequential bilaterality is also compatible with MFC natural history. In our patient, the OS became involved after two years. Fung et al. reported that approximately 50% present bilaterally at baseline and approximately 25% of initially unilateral cases develop contralateral involvement within five years [12]. This context supports interpreting delayed fellow-eye involvement as recognized behaviour within the MFC spectrum.
Importantly, ICGA hypofluorescence is not specific to MFC/PIC and should not be used as a standalone discriminator from MEWDS. In MEWDS, both ICGA hypofluorescent spots and OCTA findings at the choriocapillaris level have been reported with heterogeneous results [17,18], and swept-source OCTA studies have also described transient, reversible choriocapillaris flow deficits during acute MEWDS that resolve with clinical recovery [19]. Cohort data comparing MEWDS with versus without overlapping MFC (including OCTA) further support this heterogeneity and report suspected choriocapillaris flow deficits in overlap cases, with later development of MFC lesions in the affected or fellow eye [8]. OCTA was not performed in this case, and quantitative OCTA/ICGA metrics were therefore not available. We recommend incorporating OCTA in future MEWDS-like/MFC-overlap presentations to assess choriocapillaris flow non-invasively and complement dye angiography. Accordingly, our conclusions do not require that MEWDS universally involves the choriocapillaris; in our patient, the diagnostic weight derived from the longitudinal multimodal pattern—relapse, progressive peripapillary inflammatory activity, recurrent CME, later vitritis/peripapillary leakage in the fellow eye, and persistent ICGA abnormalities—supported an evolving inflammatory chorioretinopathy. Practically, ICGA can be framed as a risk-stratifying modality in MEWDS-like presentations: extensive or persistent hypofluorescent spots, particularly when paired with recurrence, evolving hypoautofluorescence on FAF, vitreous activity, peripapillary inflammatory progression, or CME, should prompt heightened suspicion for an MFC/PIC-spectrum diagnosis and closer follow-up; early hypoautofluorescence may also indicate a more chronic inflammatory chorioretinopathy in the masquerader literature [10].
MEWDS-like presentations may be referred as neuro-ophthalmic disease when profound acute vision loss and optic disc leakage dominate, particularly when accompanied by reported visual field abnormalities and supportive (but non-specific) VEP changes. In our case, a high-dose IV corticosteroid pulse was administered for presumed retrobulbar neuritis, reflecting a recognized diagnostic pitfall; similar misclassifications have been reported [15,16]. While pulse steroids could theoretically modulate lesion visibility, causality remains speculative.
Finally, the therapeutic course provides pragmatic implications. Early BCVA improvement coincided with partial EZ restoration; later fluctuations mirrored OCT-confirmed CME. Recurrent CME drove morbidity and necessitated repeated corticosteroid exposure, culminating in predictable steroid-related sequelae (ocular hypertension and cataract surgery). Because inflammatory CNV is a major cause of exudation and vision loss in the MFC/PIC spectrum [14], CNV must be actively assessed whenever macular fluid recurs; in our patient, repeated episodes represented OCT-confirmed CME without multimodal evidence of CNV, and anti-VEGF therapy was therefore not required. These real-world trade-offs underscore the need to consider earlier steroid-sparing strategies in relapsing MFC/PIC rather than repeated cycles of local/systemic corticosteroids. The escalation to adalimumab is supported by the VISUAL I/II trials, which demonstrated reduced relapse risk and improved disease control in noninfectious intermediate uveitis, posterior uveitis, and panuveitis [20,21]. Recurrent CME was ultimately managed with an intravitreal dexamethasone implant, consistent with HURON trial evidence in non-infectious posterior uveitis, albeit with predictable adverse effects [22]. Intravitreal triamcinolone remains effective for uveitic CME but is limited by a shorter duration and frequent IOP elevation [23].
4. Conclusions
A MEWDS-like onset may be the first sign of an evolving MFC spectrum and can conceal a chronic-relapsing course with delayed fellow-eye involvement. Serial multimodal imaging is crucial to detect evolution early, support timely reclassification, and guide steroid-sparing management, with targeted local therapy for CME and vigilant monitoring for steroid-related ocular hypertension and cataract. When such cases are referred as presumed retrobulbar neuritis, structured interdisciplinary evaluation helps prevent misdiagnosis; MEWDS-like presentations that relapse, develop CME, or show progressive FAF changes should be managed as potential MFC masqueraders and followed accordingly. Further studies are needed to refine mechanisms and imaging-guided management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The Standardization of Uveitis Nomenclature (SUN) Working Group. Classification Criteria For Multiple Evanescent White Dot Syndrome Am. J. Ophthalmol.202122819820410.1016/j.ajo.2021.03.05033845025 PMC 8594763 · doi ↗ · pubmed ↗
- 2Abu-Yaghi N.E. Hartono S.P. Hodge D.O. Pulido J.S. Bakri S.J. White dot syndromes: A 20-year study of incidence, clinical features, and outcomes Ocul. Immunol. Inflamm.20111942643010.3109/09273948.2011.62428722106911 PMC 3346947 · doi ↗ · pubmed ↗
- 3The Standardization of Uveitis Nomenclature (SUN) Working Group. Classification Criteria for Punctate Inner Choroiditis Am. J. Ophthalmol.202122827528010.1016/j.ajo.2021.03.04633845011 PMC 8675391 · doi ↗ · pubmed ↗
- 4The Standardization of Uveitis Nomenclature (SUN) Working Group. Classification Criteria for Multifocal Choroiditis with Panuveitis Am. J. Ophthalmol.202122815215810.1016/j.ajo.2021.03.04333845016 PMC 8559518 · doi ↗ · pubmed ↗
- 5Callanan D. Gass J.D. Multifocal choroiditis and choroidal neovascularization associated with the multiple evanescent white dot and acute idiopathic blind spot enlargement syndrome Ophthalmology 1992991678168510.1016/S 0161-6420(92)31755-51280798 · doi ↗ · pubmed ↗
- 6Kuznetcova T. Jeannin B. Herbort C.P. A case of overlapping choriocapillaritis syndromes: Multimodal imaging appraisal J. Ophthalmic Vis. Res.20127677522737390 PMC 3381111 · pubmed ↗
- 7Bryan R.G. Freund K.B. Yannuzzi L.A. Spaide R.F. Huang S.J. Costa D.L. Multiple evanescent white dot syndrome in patients with multifocal choroiditis Retina 20022231732210.1097/00006982-200206000-0001012055465 · doi ↗ · pubmed ↗
- 8Kang H.G. Kim T.Y. Kim M. Byeon S.H. Kim S.S. Koh H.J. Lee S.C. Lee C.S. Expanding the Clinical Spectrum of Multiple Evanescent White Dot Syndrome with Overlapping Multifocal Choroiditis Ocul. Immunol. Inflamm.202230818910.1080/09273948.2020.179520632870040 · doi ↗ · pubmed ↗