The Resistance Paradox in COVID-19 Ventilator-Associated Pneumonia: A Retrospective Study on Rapid Molecular Stewardship
Andrei Mihai Bălan, Tudor-Mihai Magdaș, Andrada Elena Urda-Cîmpean, Constantin Bodolea, Andrada Nemeș, Lucreția Avram, Dana Crișan, Sebastian Trancă

TL;DR
This study found that ventilator-associated pneumonia in COVID-19 patients shows higher antibiotic resistance and benefits from faster molecular testing.
Contribution
The study identifies a distinct antimicrobial resistance profile in VAP-COVID and evaluates rapid molecular diagnostics for faster results.
Findings
VAP-COVID patients had higher resistance to carbapenems and fluoroquinolones compared to non-COVID-VAP patients.
POC-PCR significantly reduced diagnostic turnaround time compared to standard culture methods.
VAP-COVID patients had lower pleural effusion and higher neutrophil-to-lymphocyte ratios.
Abstract
Background/Objectives: The COVID-19 pandemic complicated the diagnosis of Ventilator-Associated Pneumonia (VAP), leading to empiric antibiotic overuse due to the difficulty in distinguishing viral progression from bacterial superinfection. However, it remains unclear whether COVID-19-associated VAP displays a distinct antimicrobial resistance profile compared to classical VAP. Methods: This monocentric, retrospective cohort study primarily investigated differences in clinical phenotypes and antibiotic resistance profiles between patients with VAP-COVID (n = 26) and non-COVID-VAP (n = 26). Logistic regression was used to identify factors associated with the COVID-19 phenotype and predictors of antimicrobial resistance. As a secondary objective, we evaluated the diagnostic efficacy of a multiplex Point-of-Care PCR (POC-PCR) system (n = 22) compared to standard culture (n = 26) regarding…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
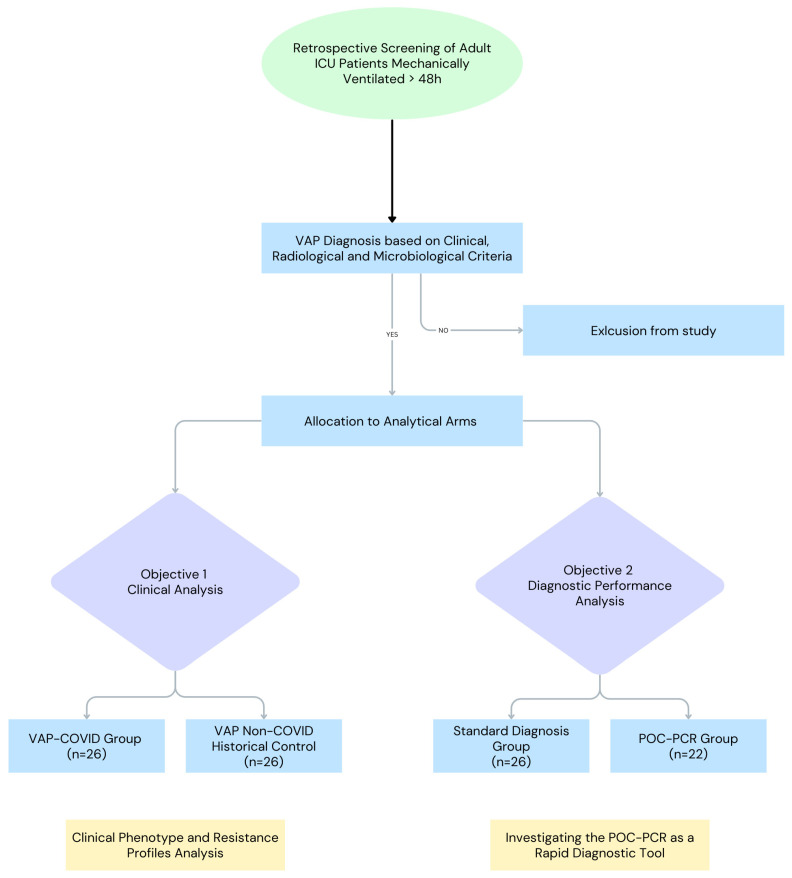 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNosocomial Infections in ICU · Antibiotic Use and Resistance · Infection Control and Ventilation
1. Introduction
The COVID-19 pandemic rapidly emerged as a healthcare emergency. Although the acute phase of the pandemic has subsided, we must acknowledge that the impact of the crisis extended beyond immediate mortality. While a total of 5.94 million deaths were reported between January 2020 and December 2021, excess mortality estimates suggest a toll as high as 18.2 million [1].
Ventilator-associated pneumonia (VAP) is defined as pneumonia that occurs in patients who require mechanical ventilation for more than 48 h. It is one of the most common infectious complications in critical care and is associated with increased morbidity and mortality [2,3,4,5,6,7]. The incidence of VAP increased significantly during the pandemic, with reported rates reaching up to 50% [8,9,10,11,12,13,14,15,16,17,18,19]. This increase was caused by various factors: intrinsic pathophysiological issues, such as extensive lung damage and immune dysregulation, and operational challenges, like staffing shortages and inadequate personal protective equipment (PPE), which led to cross-contamination [14,20,21,22,23,24,25,26,27,28]. The clinical presentation of COVID-19 often included severe hypoxemia, leukocytosis, and extensive bilateral infiltrates, which greatly overlap with bacterial superinfection. Traditional diagnostic criteria have proven unreliable in COVID-19 cases, severely impairing accurate diagnosis and stewardship efforts [29,30].
This diagnostic ambiguity led to the overuse of broad-spectrum empiric antibiotics despite the absence of a confirmed bacterial cause [31,32]. This approach conflicts with the core principles of effective stewardship and has altered the resistance patterns of multiple pathogens [33,34,35]. Although the acute viral surge has subsided, the diagnostic challenges identified remain highly relevant to current practice, where distinguishing viral inflammation from bacterial sepsis continues to be a daily ICU challenge.
This study examined the distinct clinical and microbiological phenotypes of COVID-19 VAP compared to VAP non-COVID-19. We examined the microbiological resistance patterns, according to international guidelines for the responsible use of antimicrobials, to specifically characterize the surge in antimicrobial resistance under the pandemic operational pressures [32,36,37].
Additionally, we conducted a secondary sub-analysis to compare the turnaround time and effectiveness of Point-of-Care PCR (POC-PCR) with standard microbiological culture to assess its role as a key stewardship tool.
2. Results
The findings presented should be interpreted as exploratory and hypothesis-generating. Given the limited sample size and the presence of small cell counts in several comparisons, the results are susceptible to random variation and statistical instability. Accordingly, the primary objective of this analysis is not to establish definitive causal inferences but rather to describe and characterize the clinical and microbiological profiles of patients in the COVID-19 and historical control cohorts, and to identify potential signals that warrant further investigation in larger, adequately powered studies.
2.1. Patient Characteristics
A total of 52 patients were included in the study and divided into two analysis groups: VAP-COVID (n = 26) and VAP non-COVID (n = 26). Baseline demographics (age, sex) were similar, but the admission diagnoses differed significantly between groups. The primary admission diagnosis in the VAP-COVID group was acute respiratory failure (96.15%), whereas the VAP non-COVID group mainly presented with septic shock (61.53%) and altered neurological status (53.84%).
Baseline comorbidities differed significantly (Table 1). In the VAP-COVID group, there was a higher prevalence of Diabetes Mellitus (50% vs. 23.1%, p = 0.044). Conversely, the VAP non-COVID group showed higher rates of ischemic heart disease (p = 0.020), vascular disease (p = 0.016), and gastroesophageal reflux disease (GERD) (p = 0.010).
2.2. Risk Factors and Clinical Presentation
The VAP non-COVID group showed a higher prevalence of traditional risk factors for multidrug-resistant (MDR) infections, including septic shock at admission (p < 0.0001), recent hospitalization (p = 0.008), and recent antibiotic exposure (p = 0.008) (Table 2). The specific location of previous hospitalizations could not be verified due to the unavailability of comprehensive medical records, which may have influenced the selection of initial empirical antimicrobial therapy for these patients.
The VAP-COVID group had higher rates of iatrogenic risk factors for VAP, such as increased exposure to systemic corticosteroids (96.2% vs. 26.9% in the non-COVID group, p < 0.001) and proton pump inhibitors (84.6% vs. 19.2%, p < 0.001) (Table 2).
Respiratory support before intubation in the ICU also differed (Table 2). At admission, 69.2% of VAP-COVID patients required noninvasive ventilation (NIV/CPAP), whereas 53.8% of VAP non-COVID patients were already invasively ventilated (p < 0.001). Immediately prior to intubation, 88.5% of the VAP-COVID group were on NIV, compared to only 42.3% of the non-COVID group (p < 0.001).
We observed notable differences in the initial antimicrobial management. The VAP-COVID group was primarily treated with Ceftriaxone (73%) or Doxycycline (34.6%), whereas the VAP non-COVID group received broad-spectrum antibiotic combinations (e.g., Vancomycin or Linezolid combined with Gram-negative agents) (23% vs. 3.84%, p = 0.04).
2.3. VAP Diagnostic Findings
Radiological patterns varied between groups (Table 3). In the non-COVID group, 100% of VAP cases were identified by new lung consolidations, while VAP-COVID patients exhibited more ambiguous, progressive infiltrates (42.3%) or mixed patterns. Additionally, parapneumonic pleural effusion was observed in 84.6% of non-COVID patients but was absent in the VAP-COVID group (19.2%; p < 0.001).
Septic shock was significantly more common in the VAP non-COVID group (92.3% vs. 61.5%, p = 0.008) at the time of VAP diagnosis. Clinical criteria, such as leukocytosis, purulent secretions, or worsening oxygenation, were present in similar proportions in both groups (Table 3).
The average laboratory turnaround time for bacteriological validation was notably longer for the VAP-COVID group compared to the VAP non-COVID group, but the VAP-COVID group spent statistically detectable fewer days in different stages and developed VAP quicker than the VAP non-COVID group (Table 3).
2.4. Microbiology and Antimicrobial Resistance
The most common causes of VAP were Acinetobacter baumannii, Klebsiella pneumoniae, and Pseudomonas aeruginosa in both study groups. Escherichia coli and Staphylococcus aureus (MRSA and MSSA) were detected more often in the VAP non-COVID group. Fungal co-infections (Candida spp.) occurred more frequently in the VAP-COVID group (26.9% vs. 11.5%). Higher resistance rates were observed in the VAP-COVID group, with increased resistance to carbapenems (76.9% vs. 50%, p = 0.04) and fluoroquinolones (88.5% vs. 61.53%, p = 0.02). Unadjusted odds ratio (OR) for Carbapenem Resistance rate in VAP-COVID vs. non-COVID was 3.33 (95% CI [1.01; 11]). Unadjusted OR for Fluoroquinolone Resistance rate in VAP-COVID vs non-COVID was 4.79 (95% CI [1.14; 20.2]). Both results suggest higher odds in the COVID cohort, but confounding is possible due to baseline severity differences. In early-onset VAP (≤5 days), carbapenem resistance was even higher in the VAP-COVID group (80% vs. 36.36%, p = 0.043).
Empiric antibiotic therapy initiated before microbiological results was inadequate in a high proportion of patients from both groups (88.46% VAP-COVID vs. 73% VAP non-COVID, p = 0.15) (Table 4).
We analyzed multiple logistic regression models to evaluate the potential drivers of carbapenem resistance. The first model, which incorporated the study group, SAPS II scores, and the Charlson Comorbidity Index, was statistically significant (χ^2^(3) = 10.793, p < 0.05) and explained 20.2% (Nagelkerke R2) of the variance. Despite the overall model significance, no individual factor reached statistical threshold in this analysis. A subsequent model, which substituted the comorbidity index with septic shock at admission, also achieved significance (χ^2^(3) = 10.793, p < 0.05). This version explained 25.6% of the variance and correctly classified 81.8% of cases, revealing that lower SAPS II values at admission were associated with a marginally higher likelihood of carbapenem resistance (OR: 0.95, 95% CI [0.91; 0.99]).
In contrast, the regression models for fluoroquinolone resistance did not achieve statistical significance. A model including the study group, SAPS II, and the Charlson Comorbidity Index reached a significant chi-square (χ^2^(3) = 10.793), explaining only 16.5% of the variance with no significant predictors. Similarly, a model adjusting for study group, SAPS II, and septic shock was found to be non-significant (χ^2^(3) = 7.621, p > 0.05), accounting for 20.2% of the variance in fluoroquinolone resistance without reaching statistical thresholds for individual factors.
2.5. Clinical Outcomes and Prognostic Scoring
Overall ICU mortality was high and similar between the two groups (80.8% VAP-COVID versus 88.5% VAP Non-COVID; p = 0.442, Chi-square test). Kaplan–Meier analysis revealed different mortality patterns. The VAP-COVID group had a shorter median survival of only 18 days (95% CI: 15–27 days), compared to 45 days (95% CI: 27–66 days) in the VAP Non-COVID group. Survival rates were similar only during the first week (~96%). After this initial period, the VAP-COVID curve declined sharply, and by Day 21, survival dropped to 30.8%, versus 68.0% in the Non-COVID group. Overall mortality was similar (>80% in both groups) due to late deaths in the Non-COVID group. Therefore, overall survival did not differ significantly between groups (Log-rank p = 0.34) (Figure 1).
The progression of this disease in the VAP-COVID cohort was linked to the resistance profile analysis. In the VAP-COVID group, patients with Extensively Drug-Resistant (XDR) organisms experienced the highest early mortality rates, with 40% of deaths happening between days 14 and 28. In opposition, in the VAP Non-COVID group, XDR-related deaths mainly occurred later, with most (70.6%) happening after Day 28. The overall mortality rate in the sample was a bit smaller in the VAP-COVID group than the VAP-COVID group, but with no detectable significance (OR = 0.55 95% CI [0.11; 2.58]).
VAP non-COVID patients had longer survival times with no detectable significance, but with significantly more total hospital days (average 43.3 vs. 17.4 days, p = 0.004) and longer mechanical ventilation durations (average 24.2 vs. 13.3 days, p = 0.001).
The evolving pattern of organ failure scores was associated with mortality (Figure 2; Table 5). Patients in the VAP non-COVID group had higher Charlson Comorbidity Index (CCI; 8.16 vs. 4.77; p < 0.001) and higher baseline SOFA scores two days before VAP diagnosis (10.85 vs. 8.47; p = 0.008). In contrast, VAP-COVID patients had lower assessment scores until superinfection occurred. From the point of VAP diagnosis, non-survivors in the VAP-COVID group exhibited a sharp, significant linear increase in SOFA scores leading up to death (p < 0.05).
A logistic regression was performed to o ascertain the effects of group, SAPS II and Charlson Comorbidity Index at admission on the likelihood that participants would die. The logistic regression model was not statistically significant, χ^2^(2) = 2.492, p > 0.05.
2.6. Hematological Profile of Deceased Patients
In a sub-analysis restricted just to deceased patients (VAP-COVID n = 21; VAP non-COVID n = 23), notable differences in hematological profiles were observed, while age and platelet counts remained similar (Table 6). At ICU admission, the VAP-COVID group already showed significant lymphopenia (median 0.44 vs. 0.68 K/µL, p = 0.019). This difference became more pronounced at the time of VAP diagnosis, with the VAP-COVID group exhibiting a different inflammatory response, characterized by significantly higher neutrophils (median 15.63 vs. 10.04 K/µL, p < 0.001) and persistently lower lymphocytes (median 0.46 vs. 0.77 K/µL, p = 0.004). Consequently, the Neutrophil-to-Lymphocyte Ratio (NLR) was significantly higher in the VAP-COVID group compared to the non-COVID group (median 41.36 vs. 9.63, p < 0.001). NLR was also significantly elevated at Day 28 (p < 0.001). Conversely, the VAP non-COVID group consistently had higher counts of monocytes, eosinophils, and basophils, along with a significantly higher RDW-SD at all three measured time points (p < 0.001).
2.7. Rapid Molecular Diagnostic Sub-Analysis (POC-PCR)
To assess potential solutions to diagnostic delays, we compared a subgroup of VAP patients diagnosed with Point-of-Care PCR (POC-PCR; n = 22) with those diagnosed with standard culture (n = 26). Baseline demographic characteristics and severity scores (SOFA, APACHE II) were similar between these subgroups.
The analysis demonstrated that POC-PCR significantly reduced the mean time to result validation to 61.31 ± 9.87 min, compared with 3752.72 ± 1675.45 min (~62.5 h) for standard culture (p < 0.001). POC-PCR detected resistance markers not identified by phenotypic testing, yielding a significantly higher detection rate of Colistin resistance than standard methods (36.4% vs. 3.8%; p = 0.003).
3. Discussion
3.1. The Diagnostic Ambiguity
Effective antimicrobial management relies on a physician’s ability to distinguish bacterial superinfection from viral progression. In the context of COVID-19, however, traditional clinical and radiological signs are unclear, leading to antibiotic overuse despite low confirmed bacterial causes [10,30,38,39].
The progressive consolidations observed radiologically in SARS-CoV-2 infection, present in 42.3% of the cohort, reflect specific pathophysiological mechanisms such as immunothrombosis and pulmonary infarction, rather than bacterial consolidation [31]. Notably, another classic sign of bacterial pneumonia, the parapneumonic pleural effusion, was less common in the VAP-COVID group than in the non-COVID controls (19.2% vs. 84.6%), consistent with the literature and indicating that its presence predicts the absence of COVID-19 pneumonia [40,41]. Although the type of sampling can affect the power of the microbiological part of the diagnostic process, in this study, only classic sampling from the endo-tracheal tube was used due to the lack of staff competencies and lack of specific equipment (bronchoscopes). This could have led to contamination and could be a reason for over-diagnosis.
To further complicate diagnosis, biological markers such as C-Reactive Protein and Procalcitonin were not reliable in distinguishing overlapping bacterial infections in COVID-19 [42,43,44]. This altered inflammatory response results from both the viral infection itself and from the immunomodulatory treatments used, like dexamethasone and tocilizumab [4,5,16,42,43,44,45,46]. Therefore, to overcome the limitations of subjective clinical judgment and improve prescription accuracy, diagnostic-guided algorithms are essential, as emphasized by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) [36].
3.2. The Impact of Empiric Antibiotic Overuse
Local microbiological patterns remain a key factor in VAP etiology and cause significant variation across different centers [4,5,46]. In our study group, consistent with the broader literature, the main pathogens of COVID-19 VAP were Gram-negative bacteria—Enterobacteriaceae, Acinetobacter baumannii, and Pseudomonas aeruginosa [16,19,47,48,49]. In our study, the VAP-COVID group had notably fewer traditional admission risk factors but experienced significantly higher rates of Carbapenem resistance (76.9% vs. 50%, p = 0.04) and fluoroquinolone resistance (88.5% vs. 61.5%, p = 0.02) compared to historical controls. These resistance rates likely reflect a multi-factorial mechanism, driven by iatrogenic pressures such as almost universal use of systemic corticosteroids (96.2%) and PPIs (86.4%), with consequent immunosuppression and prolonged non-invasive ventilation time (88.5%), and the pandemic associated operational strain. Early intervention, meticulous monitoring and personalized care are paramount for enhancing survival in SARS-CoV-2 pneumonia, but due to staffing shortages, high ICU workloads and the lack of protective equipment (PPE), the prevention of secondary hospital-acquired infections was likely hindered [50].
Prudent antibiotic use is essential to prevent MDR development [51]. Guidelines advise against antibiotic use in patients with negative cultures, but due to the diagnostic challenges associated with COVID-19 infection and the fear of missing a bacterial superinfection, widespread empirical antibiotic use was observed from the start of treatment [14,52,53]. A notable example is the heavy reliance on azithromycin during early pandemic waves, a common practice later disproven but still contributing to the selective pressure for MDR [52,54].
In cohorts where patients with an unconfirmed diagnosis of pneumonia received broad-spectrum antibiotics, a resistant phenotype emerged, with carbapenem resistance rates reaching as high as 100% for Acinetobacter isolates, and a significant rise in high-risk clones carrying blaOXA-23 and blaNDM genes [55,56,57,58].
Iatrogenic factors specific to pandemic protocols further increased this risk. The widespread use of systemic corticosteroids (96.2%) and proton pump inhibitors (PPIs) (84.6%) in our VAP-COVID group may have contributed to secondary infections. Corticosteroids are known to promote VAP development by affecting the immune response [59,60], and high PPI use causes hypochlorhydria and colonization of the aerodigestive tract [61,62]. Prolonged Non-Invasive Ventilation (NIV), used frequently in our cohort (88.5% of VAP-COVID patients), is a risk factor for pulmonary microaspiration [31]. Additionally, longer laboratory turnaround times contributed to the emergence of resistant phenotypes by extending the period of inadequate empiric therapy, which occurred in 88.5% of our VAP-COVID cases [29,63].
This resistance paradox represents a lasting “ecological scar,” not just a temporary anomaly from the past crisis [55]. It is reported that resistance phenotypes have not reverted to pre-pandemic levels but have stabilized at dangerous new highs [64,65,66]. Antunes et al. reported that resistance rates in Klebsiella pneumoniae doubled during the surge (from 26% to 51%) and remained high at 42% post-pandemic. Additionally, carbapenem resistance in Acinetobacter baumannii surged to 92% and settled at 85% after the surge, far above pre-pandemic levels [64]. In China, resistance in Carbapenem-Resistant K. pneumoniae (CRKP) to monobactams peaked at 96.9% in 2024 [65]. Turkish data further reinforce this trend, showing significant post-pandemic increases in resistance of Acinetobacter and Klebsiella to gentamicin and colistin [66].
This landscape has become the new norm for MDR microorganisms, as empirical coverage shifts with the expansion of hypervirulent lineages [67]. Given the high resistance levels and diagnostic uncertainties, implementing vigilance tools is essential. Validated risk stratification methods, such as the Clinical Pulmonary Infection Score (CPIS), along with high-sensitivity rapid molecular tests, are necessary to enable targeted therapy [64].
3.3. Rapid Molecular Diagnostic Sub-Analysis
Our data may indicate that POC-PCR offers quick microbiological insights that can support early treatment decisions in the ICU, as it considerably shortened the diagnostic turnaround time from 62 h to just 1 h [68,69,70]. This practice helps meet the World Health Organization’s standards for prompt diagnosis to guide antimicrobial therapy and aligns with the European Commission’s goal to implement rapid diagnostics that aid clinical decision-making and reduce unnecessary antimicrobial use [37,71].
Molecular tools have higher diagnostic sensitivity, allowing for detection of pathogens and resistance markers that standard cultures may miss. This enables the clinical team to initiate targeted antibiotics within the first hour of suspicion [29]. Therefore, these tools provide a promising way to safely shorten antibiotic courses, reduce overuse, and facilitate early de-escalation [72]. Recent data confirms that implementing such diagnostic bundles significantly decreases broad-spectrum antibiotic use while maintaining similar clinical outcomes, establishing POC-PCR as a vital tool in ICU care [73]. These findings could impact antimicrobial stewardship by enabling earlier microbiological guidance.
3.4. Limitations
Our study recognizes several limitations. First, it is a retrospective, single-center study with a relatively small sample size, which inherently limits its statistical power, generalizability of the findings and causal inference. The absence of data regarding antibiotic administration regimes makes the relationship between empiric overuse and the microbial resistance largely inferential. We acknowledge that microbial ecology is institution-specific and that resistance rates reported here represent site-specific data rather than a universal overview applicable to other ICUs. Consequently, our results are intended to be exploratory and highlight trends, but we recognize that broader multicenter prospective studies are required to ensure generalizability. Comparing a pandemic cohort to a historical control may also introduce temporal bias in clinical practices over time, but matching criteria and statistical significance support our findings. Furthermore, the use of a historical control group introduces inherent temporal bias, and changes in ICU practices and antimicrobial stewardship strategies may account for some differences observed. Additionally, due to the small sample size, there were not enough patients with concomitant chronic key conditions to support a statistically significant analysis. We also acknowledge the risk of selection bias, as the patients were included only if complete microbiological data were available, potentially overestimating resistance rates, mortality or the proportion of inadequate empiric therapy.
The main limitation of rapid molecular tests is the inability to distinguish between bacterial colonization and active infection organisms [74,75,76]. In our study, we lacked a specific assessment of fungal infection and viral reactivations to delimitate a clear distinction between colonization and invasive disease.
The study may also be affected by selection bias, as patients were included only if complete microbiological data were available. This approach may preferentially include patients with more severe disease or longer ICU stays, potentially inflating resistance rates, mortality, and the proportion of inadequate empiric therapy. Additionally, our study did not measure if employing the rapid molecular tests translated into direct clinical benefits, such as earlier antibiotic de-escalation or improved survival.
Furthermore, our study lacks diagnostic depth regarding fungal and viral co-pathogens. While Candida species were detected, the retrospective design prevented us from definitively distinguishing between airway colonization and invasive fungal disease, as specialized biomarkers or histopathological data were unavailable. Additionally, we did not explore viral reactivations, such as Herpes Simplex Virus (HSV) or Cytomegalovirus (CMV), which are increasingly recognized as contributors to ICU morbidity and may have confounded our inflammatory markers and outcome measures. The high rates of systemic inflammation observed may therefore reflect a more complex interplay of multiple infectious drivers than currently captured in our microbiological analysis.
3.5. Future Perspectives for the Post-Pandemic Era
The persistence of high-level resistance phenotypes, such as sustained carbapenem resistance in Acinetobacter spp. and Klebsiella spp., suggests that traditional “escalation” strategies may now carry increased risks of early treatment failure [37,65,66,67,68,69,70,71,72,73,74,75,76,77]. As the current microbiological landscape has changed significantly, future research focused on measuring the reduction in empiric antibiotic days could provide the necessary clinical and economic justification. There is a need to determine if the integration of POC-PCR translates clinically to a reduction in antibiotic days and lower rates of resistance emergence.
Also, as emerging post-pandemic data identified a ‘resistance paradox’, universal conclusions require a larger number of patients to ensure representativeness through future multicenter prospective studies and meta-analyses.
4. Materials and Methods
4.1. Study Design and Rationale
We conducted a retrospective observational study in the ICU of Cluj-Napoca Municipal Clinical Hospital. The study aimed to: (1) characterize the clinical and microbiological profile of VAP in COVID-19 patients compared to historical controls, and (2) compare the turnaround time and resistance detection performance of Point-of-Care PCR versus traditional microbiological culture. The study protocol adhered to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Hospital Ethics Committee (Approval No. 7/2020).
4.2. Study Population and Cohort Stratification
We included adult patients (>18 years) who were mechanically ventilated for at least 48 h and developed Ventilator-Associated Pneumonia (VAP). Patients with early mortality (<48 h after admission) were excluded. Patients were selected consecutively based on the availability of complete microbiological data. After retrospective chart screening, patients were assigned to two distinct analytical groups (Figure 3):
Objective 1: Clinical and Microbiological Phenotype Analysis
To assess the impact of the pandemic on VAP outcomes and resistance, we compared:
- VAP-COVID Group (n = 26): Patients admitted during the pandemic (2020–2021) with severe SARS-CoV-2 pneumonia and confirmed VAP.
- VAP non-COVID historical Control (n = 26): A historical cohort with comparable baseline characteristics admitted in the pre-pandemic period (January 2018–January 2020) with VAP.
Objective 2: Diagnostic Performance Analysis
To evaluate the usefulness of molecular diagnostics outside of pandemic-related operational limitations, we studied a separate group of patients from the pre-pandemic period. We used this study design to avoid the confounding effects of COVID-19 isolation protocols.
Standard Diagnostics Group (n = 26): Patients diagnosed exclusively via standard culture and antibiogram (disk diffusion/automated systems).POC-PCR Group (n = 22): Patients diagnosed using standard culture combined with a multiplex Point-of-Care PCR system.
Study design and patient allocation flowchart. Patients were stratified into two analytical arms: (Left) A clinical phenotype analysis comparing pandemic vs. historical cohorts, and (Right) A diagnostic performance sub-analysis comparing standard culture vs. Point-of-Care PCR.
4.3. Definitions and Criteria
VAP diagnosis was established according to international guidelines [4,5]. Only the first episode of VAP for each patient was included in the analysis. A confirmed case required the presence of a new or worsening radiological infiltrate combined with at least two clinical signs of infection: fever > 38.3 °C, purulent tracheal secretions, or leukocytosis (>12,000/µL) or leukopenia (<4000/µL). Microbiological diagnosis was confirmed with a positive quantitative culture (≥10^5^ CFU/mL) from endotracheal aspirates. Endotracheal aspiration was the sampling technique of choice, as fiberoptic bronchoscopy for bronchoalveolar lavage was not available during the study period. Resistance profiles were classified as Multidrug-Resistant (MDR), Extensively Drug-Resistant (XDR), or Pandrug-Resistant (PDR).
4.4. Data Collection
For the clinical analysis, we documented demographics, comorbidities (Charlson Index), severity scores (SOFA, APACHE II, SAPS II), and treatment data (corticosteroids, gastric suppression). The SOFA score was monitored dynamically at admission, intubation, 2 days before VAP, at VAP diagnosis, and at discharge to assess ongoing organ failure. For the diagnostic sub-analysis, we specifically recorded the time to result validation (measured in minutes from sampling to the identification of the pathogen) and the concordance of resistance detection between PCR and culture.
4.5. Statistical Analysis
All statistical analyses presented in the results section are exploratory, no corrections were made despite low sample size. Continuous variables were reported as mean ± standard deviation (SD) or median with interquartile range (IQR) for non-normally distributed data, while categorical variables are shown as frequencies (n) and percentages (%). Statistical analysis was performed using Student’s t-test or the Mann–Whitney U test for continuous variables, and to estimate effect sizes we computed Standardized Mean Differences (Cohen’s d) and 95% confidence intervals. For the categorical variable, we used the Chi-square test or Fisher’s exact test, and to estimate effect sizes we computed Standardized Mean Differences (SMD) for binary variables. For survival analysis, we employed Kaplan–Meier curves with Log-rank testing. A p-value < 0.05 was considered statistically significant. Statistical analyses were conducted using SPSS v.28.0 (IBM Corp., Armonk, NY, USA), Jamovi v. 2.3 (The jamovi project (2022) https://www.jamovi.org, accessed on 10 February 2026) using R: A Language and environment for statistical computing v 4.1 (R Core Team (2021) https://cran.r-project.org, accessed on 10 February 2026) and Microsoft Excel (Microsoft Office Professional Plus 2021).
5. Conclusions
Aligning with emerging global post-pandemic data, we identified a distinct COVID-19 VAP phenotype characterized by iatrogenic risk factors, diagnostic ambiguity, and a “resistance paradox,” where patients exhibit high carbapenem resistance despite fewer traditional risk factors. To address the emergence of this high-resistance landscape, our analysis confirms that implementing Point-of-Care PCR reduces diagnostic turnaround time by over 60 h compared to standard culture. The integration of rapid molecular diagnostics may support earlier microbiological guidance in an era of diagnostic uncertainty. These exploratory findings support further prospective studies to clarify the clinical impact of early microbiological information in critically ill patients with VAP.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1COVID-19 Excess Mortality Collaborators. Estimating Excess Mortality Due to the COVID-19 Pandemic: A Systematic Analysis of COVID-19-Related Mortality, 2020–21Lancet 20223991513153610.1016/S 0140-6736(21)02796-335279232 PMC 8912932 · doi ↗ · pubmed ↗
- 2Lim W.S. Pneumonia—Overview Encyclopedia of Respiratory Medicine 2nd ed. Janes S.M. Academic Press Oxford, UK 202218519710.1016/B 978-0-12-801238-3.11636-8 · doi ↗
- 3Papazian L. Klompas M. Luyt C.-E. Ventilator-Associated Pneumonia in Adults: A Narrative Review Intensive Care Med.20204688890610.1007/s 00134-020-05980-032157357 PMC 7095206 · doi ↗ · pubmed ↗
- 4Torres A. Niederman M.S. Chastre J. Ewig S. Fernandez-Vandellos P. Hanberger H. Kollef M. Li Bassi G. Luna C.M. Martin-Loeches I. International ERS/ESICM/ESCMID/ALAT Guidelines for the Management of Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia Eur. Respir. J.201750170058210.1183/13993003.00582-201728890434 · doi ↗ · pubmed ↗
- 5Kalil A.C. Metersky M.L. Klompas M. Muscedere J. Sweeney D.A. Palmer L.B. Napolitano L.M. O’Grady N.P. Bartlett J.G. CarratalàJ. Management of Adults with Hospital-Acquired and Ventilator-Associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society Clin. Infect. Dis.201663 e 61e 11110.1093/cid/ciw 35327418577 PMC 4981759 · doi ↗ · pubmed ↗
- 6Ferrer M. Torres A. Epidemiology of ICU-Acquired Pneumonia Curr. Opin. Crit. Care 20182432533110.1097/MCC.000000000000053630080701 · doi ↗ · pubmed ↗
- 7Saied W. Martin-Loeches I. Timsit J.-F. What Is New in Non-Ventilated ICU-Acquired Pneumonia?Intensive Care Med.20204648849110.1007/s 00134-019-05859-931938826 PMC 7223396 · doi ↗ · pubmed ↗
- 8Pierce J. Stevens M.P. COVID-19 and Antimicrobial Stewardship: Lessons Learned, Best Practices, and Future Implications Int. J. Infect. Dis.202111310310810.1016/j.ijid.2021.10.00134624517 PMC 8491953 · doi ↗ · pubmed ↗