Psychological Distress, Stress, and Personality Traits in Patients Undergoing Chronic Hemodialysis: A Comparative Psychometric Study
Simona Nicoleta Neagu, Aniella Mihaela Vieriu

TL;DR
This study compares the psychological health of patients on long-term hemodialysis with healthy individuals, finding higher stress, anxiety, and depression in dialysis patients.
Contribution
The study provides new insights into the psychological burden of chronic hemodialysis and its association with treatment duration.
Findings
Hemodialysis patients showed significantly higher psychological distress compared to healthy controls.
Large effect sizes were found for depression and perceived stress in dialysis patients.
Shorter dialysis duration was linked to higher stress levels, but not to anxiety or depression.
Abstract
Psychological comorbidity is increasingly recognized as a critical factor influencing outcomes in chronic illness management, particularly in patients with end-stage renal disease (ESRD). The present study examines the psychological burden associated with long-term hemodialysis in patients with ESRD, focusing on emotional distress and maladaptive personality traits. Specifically, it explores group differences between hemodialysis patients and matched healthy controls in levels of stress, anxiety, depression, and psychopathological tendencies, including neuroticism, paranoia, and psychopathy-related traits, as well as exploratory associations with treatment duration. A purposive sample of 60 participants (30 patients undergoing chronic hemodialysis and 30 age- and sex-matched healthy controls) was assessed using validated psychometric instruments: The Hospital Anxiety and Depression…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
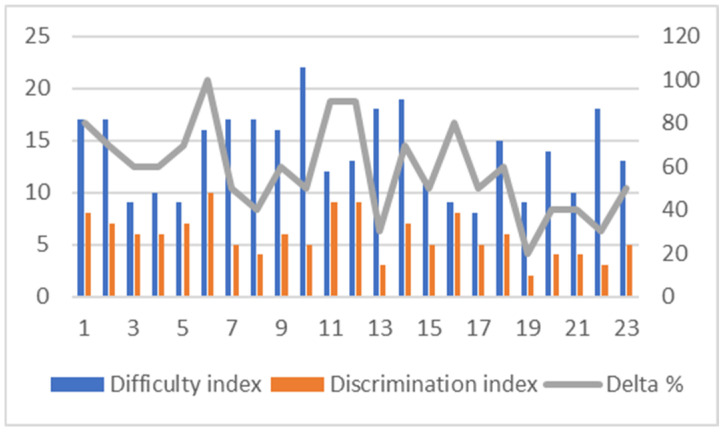 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDialysis and Renal Disease Management · Nursing care and research · Biological Research and Disease Studies
1. Introduction
End-stage renal disease (ESRD) represents a growing global health concern, with prevalence rates continuing to rise and imposing substantial physical, psychological, and socioeconomic burdens on affected individuals (Abbas et al., 2024; Doan et al., 2025). Hemodialysis remains an essential long-term treatment; however, its demanding schedule, strict lifestyle constraints, and ongoing dependence on medical technology profoundly shape patients’ daily routines, sense of autonomy, and emotional well-being (Lu et al., 2024; Zhang et al., 2024). Physical burdens such as fatigue and chronic pain exacerbate psychological strain (Bossola et al., 2011; Lopes et al., 2007; Weisbord et al., 2005). The cumulative effects of these constraints often manifest as persistent stress, anxiety, depressive symptoms, and reduced health-related quality of life (HRQoL) (Feroze et al., 2012; Song & Zhang, 2024; Yu et al., 2021).
A growing body of research indicates that psychological well-being plays a critical role in treatment adaptation, self-management behaviors, and overall outcomes in ESRD. Nevertheless, emotional distress and broader psychological vulnerabilities remain insufficiently addressed in routine nephrology care (Huang et al., 2020). Depressive symptoms are reported in approximately 30–50% of patients undergoing hemodialysis, while clinically relevant anxiety affects an estimated 20–30% (Bagasha et al., 2021; Chang & Kim, 2025). Beyond their impact on subjective well-being, these emotional difficulties are associated with poorer treatment adherence, increased healthcare utilization, and diminished quality of life (Yu et al., 2021; Zhang et al., 2024).
Importantly, psychological functioning in ESRD is not limited to transient emotional states. Stable individual differences—such as personality traits related to emotional reactivity, interpersonal sensitivity, or behavioral regulation—may shape how patients perceive, interpret, and cope with the chronic demands of dialysis (Chilcot et al., 2010; Harenski et al., 2009). These tendencies reflect subclinical elevations along normative personality dimensions rather than clinical psychopathology. From a behavioral science perspective, subclinical variations may modulate stress responses, influence coping strategies, and contribute to differential patterns of adjustment over time.
Recent international studies emphasize that the interaction between personality structure and chronic illness-related stressors plays a meaningful role in psychological adaptation among patients with ESRD (Bazrafshan et al., 2023; Touil et al., 2023; Uzdil et al., 2023). Higher levels of neuroticism, lower conscientiousness, and reliance on maladaptive coping strategies have been linked to increased emotional distress and poorer HRQoL, whereas resilience, optimism, and problem-focused coping are associated with more favorable psychological adjustment (Cukor et al., 2007; Kovacs et al., 2011). The results suggest the relevance of incorporating trait-level psychological assessment alongside traditional symptom-focused screening in dialysis care, allowing for early identification of patients who may be more vulnerable to stress exposure.
Validated psychometric instruments provide valuable tools for capturing both current emotional distress and enduring personality-related vulnerabilities. The Hospital Anxiety and Depression Scale (HADS) is widely used to assess anxiety and depressive symptoms in medical populations, while the Pichot Neuroticism and Psychopathy Questionnaire offers insight into normative personality tendencies related to emotional instability, suspiciousness, and behavioral regulation (Anastasi & Urbina, 1997; Pichot, 1987; Zigmond & Snaith, 1983). Elevated scores indicate relative predispositions along a continuum, not clinical diagnoses. Their combined use allows for a comprehensive behavioral and psychological profile of individuals undergoing long-term hemodialysis, supporting more personalized psychosocial interventions.
1.1. Theoretical Background and Rationale
International literature consistently documents elevated psychological distress among patients with ESRD, with recent findings indicating heightened vulnerability during periods of external stress, such as the COVID-19 pandemic (Cordoș et al., 2024; Yu et al., 2021). However, much of the existing research focuses narrowly on anxiety and depression, with limited attention to broader subclinical personality-related tendencies—such as heightened suspiciousness or emotional dysregulation—that may further influence coping and adjustment to chronic treatment demands. In addition, cross-cultural variations in healthcare systems, social support, and coping norms may affect psychological responses to dialysis, limiting the generalizability of findings across populations (Soponaru et al., 2016).
In Romania, empirical research addressing the psychological dimensions of chronic hemodialysis remains relatively scarce. Available studies suggest elevated stress levels, reduced HRQoL, and a predominance of emotion-focused coping strategies among dialysis patients; however, few investigations have systematically examined subclinical personality correlates or integrated multiple validated psychometric measures within a single framework (Cordoș et al., 2024; Soponaru et al., 2016). This gap constrains the development of culturally informed psychosocial interventions tailored to the needs of Romanian ESRD populations.
The present study seeks to address these limitations by adopting a multidimensional behavioral science approach that integrates measures of perceived stress, emotional symptoms, and subclinical personality-related tendencies. By comparing patients undergoing chronic hemodialysis with healthy controls, the study aims to clarify the associations between subclinical personality tendencies and emotional distress, including how these traits interact with dialysis-specific stressors. Dialysis duration is examined in an exploratory manner to assess whether prolonged exposure to treatment demands may be associated with differences in perceived stress, while acknowledging the limitations imposed by subgroup size.
1.2. Study Aim and Hypotheses
The primary aim of this study is to explore psychological and psychopathological correlates of chronic hemodialysis in patients with ESRD, with a focus on perceived stress, anxiety, depression, and maladaptive personality-related tendencies—specifically neuroticism, paranoid ideation, and psychopathy-related traits—compared to a healthy control group.
General hypothesis: Prolonged exposure to the psychosocial demands associated with ESRD and chronic hemodialysis is associated with higher levels of emotional distress and a greater expression of maladaptive personality-related tendencies relative to healthy individuals.
Specific hypotheses:
H1. Patients undergoing hemodialysis report significantly higher perceived stress levels than healthy controls.
H2. Anxiety and depressive symptoms are more prevalent among hemodialysis patients.
H3. Personality-related tendencies associated with neuroticism, paranoid ideation, and psychopathy-related traits are more pronounced in the patient group.
H4 (Exploratory). Differences in perceived stress may emerge between patients with shorter (<10 years) and longer (≥10 years) durations of hemodialysis, though conclusions are considered hypothesis-generating due to sample size limitations.
By integrating emotional, cognitive, and personality-related dimensions, this study contributes to a more nuanced behavioral understanding of psychological adaptation in ESRD and supports the implementation of systematic psychological screening and psychosocial support within nephrology care.
2. Materials and Methods
2.1. Study Design
The present study employed a cross-sectional, case–control design to examine psychological distress and personality-related tendencies in patients undergoing chronic hemodialysis compared to a non-clinical control group.
The independent variable was group membership (hemodialysis patients vs. healthy controls).
The dependent variables included perceived stress, anxiety, depressive symptoms, and personality-related tendencies (neuroticism, paranoid ideation, and psychopathy-related traits).
Dialysis duration (<10 years vs. ≥10 years) was examined as an exploratory grouping variable within the clinical sample.
2.2. Participants and Sampling
A non-probabilistic purposive sampling strategy was used to recruit participants who met the study’s inclusion criteria. The final sample consisted of 60 adults, divided into two groups:
Hemodialysis group (n = 30): Patients diagnosed with end-stage renal disease and undergoing chronic hemodialysis, recruited from the Hemodialysis Department of Dr. Carol Davila Clinical Hospital, Bucharest, Romania.
Control group (n = 30): Community-dwelling adults recruited from the general population, including employees of The National University of Science and Technology POLITEHNICA Bucharest and Metrorex S.A.
The control group was selected to approximate the clinical group in terms of age and educational level, while excluding individuals with known chronic medical or psychiatric conditions.
Inclusion criteria: Age between 18 and 65 years; Ability to understand and complete self-report questionnaires; For the clinical group: ongoing hemodialysis treatment; For controls: absence of diagnosed chronic medical or psychiatric illness.
Exclusion criteria: Documented severe psychiatric disorders (e.g., psychotic disorders); Cognitive impairment preventing questionnaire completion.
Within the hemodialysis group, participants were further categorized based on treatment duration (<10 years vs. ≥10 years) for exploratory analyses.
2.3. Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki (World Medical Association, 1975/2013) and was approved by the Scientific Research Ethics Committee of the National University of Science and Technology POLITEHNICA Bucharest (Approval No. 92; Approval Date: 31 January 2025).
Participants undergoing hemodialysis were recruited with the support of the clinical psychologist working within the dialysis center, who informed eligible patients about the study and provided the questionnaire link only to those who voluntarily expressed interest in participating. The research team had no direct contact with potential participants prior to their consent.
The questionnaire was administered online via Google Forms. Before accessing the questionnaire, participants were presented with detailed study information, including the purpose of the research, voluntary nature of participation, right to withdraw at any time, and assurances of anonymity and confidentiality.
Due to the anonymous and minimal-risk design of the study, written informed consent was not required. Informed consent was obtained electronically through the participants’ voluntary completion and submission of the questionnaire, in accordance with the approval of the Ethics Committee.
2.4. Research Instruments
The Hospital Anxiety and Depression Scale (HADS; Zigmond & Snaith, 1983) is a 14-item self-report questionnaire designed to assess anxiety and depressive symptoms in medical populations while minimizing confounding from somatic symptoms. It consists of two subscales (Anxiety and Depression), each containing seven items rated on a 4-point Likert scale. The scale was originally developed by Zigmond and Snaith and published by the NFER-Nelson Publishing Company (Windsor, UK). The instrument demonstrates good reliability and validity across clinical populations.
The Pichot Neuroticism and Psychopathy Questionnaire (PNP; Pichot, 1987) assesses personality-related tendencies across three dimensions: neuroticism, paranoid ideation, and psychopathy-related traits. The instrument was originally developed by Pierre Pichot at Hôpital Sainte-Anne (Paris, France). In the present study, the PNP was used to capture personality-related tendencies within a psychometric framework rather than clinical diagnoses of personality disorders.
Dialysis-Specific Stress Questionnaire. The dialysis-specific stress questionnaire was developed for research purposes to assess perceived stress related to health status, daily functioning, and treatment-related burden. Item content was generated based on clinical experience, review of relevant literature on dialysis-related stress, and consultation with healthcare professionals working in nephrology settings. The questionnaire was administered to both hemodialysis patients and healthy controls to allow comparative analysis of perceived stress levels. Items are rated on a 5-point Likert scale. Preliminary psychometric validation was conducted in a pilot sample of 30 hemodialysis patients following classical test theory principles, including item difficulty, item discrimination, item-total correlations, and internal consistency analysis. Although the instrument demonstrated excellent internal consistency in the present sample (Cronbach’s α = 0.94), further research is needed to establish its construct validity and factor structure. The full instruments are provided in Appendix A. The Dialysis-Specific Stress Questionnaire is a study-specific instrument; details regarding its psychometric validation are provided in Appendix B.
2.5. Analysis
Data were analyzed using descriptive and inferential statistics to compare psychological outcomes between patients undergoing chronic hemodialysis and healthy controls. Statistical analyses were conducted using IBM SPSS Statistics for Windows, Version 22 (IBM Corp., Armonk, NY, USA). Descriptive statistics (means and standard deviations) summarized anxiety, depression, stress, and personality-related variables. Group differences were examined using independent samples t-tests, including exploratory comparisons based on dialysis duration (<10 years vs. ≥10 years). Assumptions of normality and homogeneity of variance were assessed prior to analysis. Statistical results are reported with corresponding effect sizes (Cohen’s d). In addition, 95% confidence intervals for effect sizes were calculated to provide an estimate of the magnitude and precision of group differences. Given the exploratory nature of the study and the modest sample size, no formal correction for multiple comparisons was applied; therefore, results should be interpreted with appropriate caution.
3. Results
3.1. Sample Characteristics
The final sample consisted of 60 participants, divided equally into a hemodialysis group (n = 30) and a healthy control group (n = 30). In the hemodialysis group, 19 participants were males and 11 females, while the control group included 17 males and 13 females. The gender distribution was relatively balanced across groups.
Regarding educational level, the groups were broadly comparable. Among patients undergoing hemodialysis, 14 participants (46.7%) had completed higher education, 15 (50%) had completed high school, and one participant (3.3%) had completed secondary education only. In the control group, 15 participants (50%) had completed higher education, and 15 (50%) had completed high school.
Within the hemodialysis group, most participants reported no prior history of psychological difficulties before the onset of chronic kidney disease (93.3%). A subset of patients (36.7%) reported previous medical conditions commonly associated with chronic illness, such as diabetes, hypertension, or cardiovascular disease. These data were collected to contextualize psychological vulnerability and to distinguish between pre-existing conditions and those potentially emerging during long-term treatment.
The duration of hemodialysis treatment varied widely, ranging from less than one year to more than 20 years, reflecting substantial heterogeneity in treatment experience. For exploratory analyses, patients were grouped according to dialysis duration into those receiving treatment for less than 10 years (n = 15) and those receiving treatment for 10 years or longer (n = 15).
3.2. Anxiety and Depression (HADS)
Anxiety and depression were assessed using the Hospital Anxiety and Depression Scale (HADS) in patients undergoing chronic hemodialysis (n = 30) and matched healthy controls (n = 30).
Hemodialysis patients reported significantly higher anxiety scores (M = 10.93, SD = 4.77) compared to healthy controls (M = 8.20, SD = 2.81), t(58) = 2.86, p = 0.006, Cohen’s d = 0.70, 95% CI [0.18, 1.22], indicating a moderate effect size (Table 1).
Similarly, depression scores were significantly higher in the hemodialysis group (M = 10.90, SD = 5.01) than in controls (M = 5.67, SD = 3.04), t(58) = 4.57, p < 0.001, Cohen’s d = 1.26, 95% CI [0.71, 1.81], indicating a large effect size.
Exploratory analyses examining dialysis duration (<10 years vs. ≥10 years) revealed no statistically significant differences in anxiety (p = 0.230) or depression (p = 0.478).
3.3. Personality Traits (PNP)
Personality traits were assessed using the Pichot Neuroticism and Psychopathy Questionnaire.
Hemodialysis patients demonstrated significantly higher neuroticism scores (M = 65.77, SD = 11.45) compared to controls (M = 59.13, SD = 11.37), t(58) = 2.29, p = 0.025, Cohen’s d = 0.58, 95% CI [0.06, 1.10], indicating a moderate effect size (Table 2).
Psychopathy-related trait scores were also significantly higher in hemodialysis patients (M = 62.57, SD = 8.73) compared to controls (M = 53.97, SD = 12.04), t(58) = 2.76, p = 0.008, Cohen’s d = 0.82, 95% CI [0.29, 1.35], indicating a large effect size.
Paranoid trait scores were higher in the hemodialysis group (M = 56.40, SD = 18.12) compared to controls (M = 51.30, SD = 11.55), but this difference did not reach statistical significance, t(58) = 1.29, p = 0.202, with a small effect size (Cohen’s d = 0.34) and a 95% confidence interval [−0.17, 0.85], suggesting a modest and imprecisely estimated difference.
For descriptive purposes, elevated neuroticism scores (T > 70) were observed in 57% (n = 17) of hemodialysis patients compared to 23% (n = 7) of controls. Elevated psychopathy-related scores were present in 37% (n = 11) of hemodialysis patients and 13% (n = 4) of controls. Elevated paranoid trait scores were observed in 40% (n = 12) of hemodialysis patients compared to 17% (n = 5) of controls. These categorizations reflect elevated trait levels based on psychometric conventions and do not represent clinical diagnoses. Reporting both continuous scores and categorical distributions is intended to enhance transparency, particularly given the modest sample size.
Exploratory subgroup analyses based on dialysis duration revealed no statistically significant differences for neuroticism (p = 0.734), paranoid tendencies (p = 0.481), or psychopathic traits (p = 0.889).
3.4. Dialysis-Specific Stress
Dialysis-specific stress was assessed in both hemodialysis patients and healthy controls to allow comparative analysis. Hemodialysis patients reported significantly higher stress scores (M = 62.40, SD = 20.83) compared to healthy controls (M = 37.23, SD = 11.14), t(58) = 5.84, p < 0.001, Cohen’s d = 1.51, 95% CI [0.93, 2.09], indicating a large effect size (Table 3).
Within the hemodialysis group, patients receiving treatment for less than 10 years reported significantly higher stress levels (M = 71.27, SD = 20.58) than those undergoing dialysis for 10 years or more (M = 53.53, SD = 17.50), t(28) = −2.54, p = 0.017.
Given the study-specific nature of the instrument and its preliminary psychometric validation, these findings should be interpreted with appropriate caution.
4. Discussion
This study examined psychological outcomes—including dialysis-specific stress, affective symptoms (anxiety and depression), and personality traits—in patients undergoing chronic hemodialysis compared to healthy controls. Four hypotheses guided this research, focusing on stress prevalence, affective symptoms, personality traits, and the influence of dialysis duration on psychological outcomes.
4.1. Hypotheses Overview
H1—Stress prevalence in hemodialysis patients: Supported. Patients reported significantly higher dialysis-specific stress than healthy controls. Stress was greater in patients on dialysis for less than 10 years. This pattern may reflect psychological adaptation over time; however, given the cross-sectional design, alternative explanations—such as the possibility that long-term patients represent a resilient “survivor” subgroup—cannot be ruled out (Chang & Kim, 2025; Sprangers & Schwartz, 1999).
H2—Anxiety and depression in hemodialysis patients: Supported. Hemodialysis patients showed higher anxiety and depression than controls, consistent with prior studies estimating that 30–40% of dialysis patients experience clinically relevant affective symptoms (Cukor et al., 2007; Feroze et al., 2012; Pereira et al., 2017). While duration of dialysis did not significantly influence these symptoms, claims about early stabilization of emotional distress should be interpreted cautiously, as longitudinal data would be needed to confirm true temporal trends.
H3—Elevated personality traits (neuroticism, psychopathic tendencies) among hemodialysis patients: Partially supported. Patients exhibited higher neuroticism and psychopathic tendencies, while paranoid traits were elevated but non-significant. These traits indicate vulnerability to emotional instability and maladaptive coping (Feroze et al., 2012; Griva et al., 2013; Nunnally & Bernstein, 1994).
H4—Relationship between dialysis duration and stress: Supported. Patients on dialysis ≥10 years reported lower stress. This may indicate adaptive mechanisms over time, but alternative explanations (e.g., survivor effects) should be considered. No significant differences in affective symptoms or personality traits were observed between dialysis duration subgroups at the time of assessment (Saracho-Rotaeche, 2013; Sprangers & Schwartz, 1999).
These findings provide a framework for understanding the interplay between situational stressors, affective symptoms, and stable personality traits in chronic dialysis patients.
4.2. Dialysis-Specific Stress (H1 and H4)
Consistent with H1, dialysis-specific stress was significantly higher in patients compared to controls. Stress arises from procedural demands, lifestyle restrictions, and dependency on medical staff (Palmer et al., 2013; Weisbord et al., 2005). Although patients on dialysis for <10 years reported higher stress than those treated longer, this should be interpreted tentatively. The lower stress in long-term patients could reflect adaptation or alternatively, a selection effect whereby patients who cope poorly may discontinue dialysis or experience higher morbidity/mortality.
This highlights that stress is situational and sensitive to adaptation, whereas affective symptoms may persist regardless of dialysis duration. These findings underscore the importance of early intervention to mitigate psychological burden during the initial years of treatment.
4.3. Anxiety and Depression (H2)
Consistent with H2, hemodialysis patients exhibited higher anxiety and depression than controls (Cukor et al., 2007; Feroze et al., 2012; Pereira et al., 2017). Approximately one-third of patients reported moderate to severe symptoms, whereas the majority of controls scored within normal ranges.
Although duration of dialysis did not significantly affect affective symptoms, any suggestion of “stabilization” over time is tentative. Longitudinal research is needed to confirm whether emotional distress truly decreases with prolonged treatment. These results reinforce the need for routine mental health screening in nephrology care, particularly during the early stages of dialysis (Chang & Kim, 2025; Saracho-Rotaeche, 2013).
4.4. Personality Traits (H3)
H3 examined personality differences between patients and controls. Hemodialysis patients displayed elevated neuroticism and psychopathic tendencies, indicating higher vulnerability to emotional reactivity, frustration, and impulsivity (Feroze et al., 2012; Griva et al., 2013; Kimmel, 2001). Paranoid traits showed a non-significant trend toward elevation, suggesting possible subclinical vulnerabilities.
Importantly, personality traits were relatively stable across dialysis duration, suggesting that trait-level characteristics are less influenced by chronic stress than situational factors like stress or affective symptoms (Crocker & Algina, 2006; Ebel & Frisbie, 1991; Kelley, 1939; Nunnally & Bernstein, 1994). These findings highlight the relevance of assessing individual personality profiles to guide personalized psychological interventions for patients at higher risk of maladaptive coping.
4.5. Limitations
This study has several limitations that warrant cautious interpretation of the findings.
First, the cross-sectional design precludes causal inference; observed differences between ESRD patients and healthy controls may reflect bidirectional influences between dialysis-related stressors, affective symptoms, and enduring personality-related tendencies rather than direct causal effects.
Second, the sample size was modest (n = 30 per group), which limits statistical power, reduces the stability of effect size estimates, and constrains generalizability to broader and more heterogeneous ESRD populations. Consistent with this limitation, some effect size estimates were associated with relatively wide confidence intervals, indicating limited precision and highlighting the need for replication in larger samples.
Third, multiple independent statistical comparisons were conducted across several psychological outcomes. No formal correction for multiple testing was applied, given the exploratory nature of the study and the risk of increasing Type II error in small samples. However, this approach may increase the risk of Type I error, and therefore the findings should be interpreted with appropriate caution.
Fourth, the reliance on self-report measures (HADS, PNP, Stress Questionnaire) introduces the potential for response biases, including social desirability and recall bias (Crocker & Algina, 2006; Nunnally & Bernstein, 1994).
Fifth, potentially important confounding variables—including prior psychiatric history, psychotropic medication use, comorbid medical conditions, socioeconomic status, and social support—were not controlled for and may have influenced psychological outcomes.
Sixth, the Dialysis-Specific Stress Questionnaire, although demonstrating excellent internal consistency and preliminary psychometric validation, was validated in a relatively small pilot sample (n = 30). While item analysis and reliability indicators supported its internal consistency and discrimination capacity, further validation in larger and more diverse samples is necessary to confirm its construct validity, factor structure, and generalizability. Therefore, findings related to dialysis-specific stress should be interpreted with appropriate caution.
Seventh, sampling bias may limit generalizability. Healthy controls were recruited from university and corporate settings, which may not be socioeconomically comparable to the clinical group. This could influence observed group differences.
Eighth, online data collection via Google Forms introduces additional considerations, particularly in a medical population. Factors such as supervision, digital literacy, environmental distractions, and variability in attention during questionnaire completion may have affected responses and should be acknowledged.
Finally, although validated instruments were used and the inclusion of a Romanian sample represents a strength, cultural, healthcare system, and contextual factors may limit the direct generalizability of these findings to other populations.
Despite these limitations, the study provides preliminary evidence supporting a multidimensional model of psychological functioning in ESRD, illustrating how dialysis-related stress, emotional distress, and personality-related vulnerability traits may co-occur and interact in patients undergoing chronic hemodialysis. These findings should be considered exploratory and hypothesis-generating, and they underscore the need for larger, longitudinal studies to clarify causal pathways and clinical implications.
4.6. Future Directions
Future research should aim to expand and deepen the understanding of psychological functioning in ESRD patients. Longitudinal designs are recommended to track the trajectories of dialysis-specific stress (H1, H4), anxiety and depression (H2), and personality adaptation (H3) over time, identifying periods of heightened vulnerability and potential adaptation (Chang & Kim, 2025; Saracho-Rotaeche, 2013). Larger, multicenter studies with diverse ESRD populations would enhance generalizability and allow for subgroup analyses by demographic and clinical characteristics.
Moreover, future studies should examine the efficacy of tailored psychological interventions, including cognitive–behavioral therapy, mindfulness-based stress reduction, and group support programs, particularly for patients demonstrating high neuroticism or maladaptive coping patterns. Integrating clinician-rated diagnostic tools with validated self-report measures would strengthen assessment validity and provide a more comprehensive profile of ESRD patients’ psychological health (Field, 2013; George & Mallery, 2003; Thurstone, 1931).
Ultimately, such research could inform personalized intervention strategies, optimizing mental health outcomes and treatment adherence in ESRD patients undergoing long-term hemodialysis.
5. Conclusions
This study provides evidence that chronic hemodialysis is associated not only with elevated emotional distress but also with a distinct psychological vulnerability profile characterized by the interaction between situational stressors and stable personality-related predispositions. This finding is consistent with previous research documenting high prevalence rates of anxiety, depression, and psychological symptom burden among patients with end-stage renal disease undergoing dialysis (Feroze et al., 2012; Palmer et al., 2013; Weisbord et al., 2005).
Importantly, the results suggest that dialysis-specific stress represents a dynamic and potentially modifiable psychological burden, particularly during the earlier stages of treatment, whereas emotional symptoms and personality-related tendencies may reflect more stable psychological patterns. This observation aligns with previous findings showing that psychosocial adaptation varies according to dialysis duration and is influenced by patients’ psychological adjustment processes (Chang & Kim, 2025; Kimmel, 2001).
From a clinical perspective, these findings support the importance of integrating routine psychological assessment into nephrology care. Beyond identifying anxiety and depression, assessing personality-related vulnerability factors may provide additional insight into individual differences in emotional adjustment and coping. Previous studies have shown that personality traits and coping mechanisms significantly influence psychological well-being, treatment adherence, and quality of life in dialysis patients (Saracho-Rotaeche, 2013; Soponaru et al., 2016; Touil et al., 2023).
Furthermore, the present findings contribute to the understanding of psychological adaptation in chronic illness by supporting a multidimensional framework in which emotional distress reflects both situational stress exposure and enduring psychological characteristics. This perspective is consistent with the broader psychosocial model of end-stage renal disease, which emphasizes the role of psychological and behavioral factors in patient adjustment and outcomes (Cukor et al., 2007; Kimmel, 2001; Lu et al., 2024).
In terms of generalization, although the findings should be interpreted with caution due to the sample size and single-center design, the observed relationships between dialysis-related stress, emotional distress, and personality vulnerability are consistent with previous research in hemodialysis populations (Ebel & Frisbie, 1991; Soponaru et al., 2016; Weisbord et al., 2005).
Finally, these results highlight the clinical value of early identification of psychological vulnerability and support the implementation of targeted psychosocial and psychoeducational interventions. Such interventions have been shown to reduce psychological distress and improve quality of life in patients undergoing maintenance hemodialysis (Zigmond & Snaith, 1983). Integrating psychological screening and intervention into routine nephrology care may therefore improve emotional adjustment and overall patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abbas E. M. Harshavardhan R. Mohammed H. Loona V. Faseeh K. M. An assessment of quality of life in ESRD patients undergoing hemodialysis Egyptian Journal of Internal Medicine 20243610410.1186/s 43162-024-00370-0 · doi ↗
- 2Anastasi A. Urbina S. Psychological testing 7th ed.Prentice Hall 1997
- 3Bagasha P. Namukwaya E. Leng M. Kalyesubula R. Mutebi E. Naitala R. Katabira E. Petrova M. Comparison of the health-related quality of life of end-stage kidney disease patients on hemodialysis and non-hemodialysis management in Uganda BMC Palliative Care 2021205210.1186/s 12904-021-00743-033794849 PMC 8017791 · doi ↗ · pubmed ↗
- 4Bazrafshan F. D. Darvizeh Z. Banijamali S. S. The relationship between hemodialysis patients’ treatment adherence, procrastination, and difficulty in emotion regulation: A cross-sectional study in southeast Iran Frontiers in Psychology 202313104191210.3389/fpsyg.2022.104191236726495 PMC 9885004 · doi ↗ · pubmed ↗
- 5Bossola M. Vulpio C. Tazza L. Fatigue in chronic dialysis patients Seminars in Dialysis 201124555055510.1111/j.1525-139X.2011.00956.x 21917000 · doi ↗ · pubmed ↗
- 6Chang A. K. Kim A. Y. Predictors of psychosocial adaptation in haemodialysis patients according to haemodialysis vintage: A quantitative study Contemporary Nurse 20256137738910.1080/10376178.2025.250121640350163 · doi ↗ · pubmed ↗
- 7Chilcot J. Wellsted D. Farrington K. Illness representations are associated with fluid nonadherence among hemodialysis patients Journal of Psychosomatic Research 201068220321210.1016/j.jpsychores.2009.08.01020105704 · doi ↗ · pubmed ↗
- 8CordoșM. Silisteanu S. Costea A. I. Toma V. DănăilăL. Foia L. G. Increased anxiety among hemodialysis patients during the COVID-19 pandemic: A single center experience Medico-Surgical Journal 2024128114115110.22551/MSJ.2024.01.15 · doi ↗