Multicenter Analytical Performance Evaluation of the BD Phoenix NMIC-461 Panel for Carbapenemase Classification and Antimicrobial Susceptibility Testing of Enterobacterales, Pseudomonas aeruginosa, and Acinetobacter spp
Jingjia Zhang, Liying Sun, Ge Zhang, Wei Kang, Tong Wang, Jin Li, Haotian Gao, Qiwen Yang, Kuixia Sun, Qian Wang, Hongli Sun

TL;DR
This study evaluates a new panel for detecting carbapenemase enzymes and antibiotic susceptibility in common bacteria, finding it effective but with some limitations in classification accuracy.
Contribution
The study introduces and validates the BD Phoenix NMIC-461 panel for rapid carbapenemase classification and antimicrobial susceptibility testing in clinical isolates.
Findings
The panel showed high sensitivity (98.8%) but moderate specificity (92.4%) for carbapenemase detection.
AST performance was excellent with essential agreement over 95% for ten antimicrobial agents.
Classification accuracy was reduced for Enterobacterales and Pseudomonas aeruginosa due to unclassified isolates.
Abstract
Objectives: To evaluate the capability of the BD Phoenix NMIC-461 panel in the detection and classification of carbapenemase production and antimicrobial susceptibility testing of 10 antimicrobial agents among Enterobacterales, Pseudomonas aeruginosa, and Acinetobacter spp. Methods: A total of 714 non-repetitive clinical isolates from three tertiary hospitals in China were enrolled. Carbapenemase production was confirmed by the modified carbapenem inactivation method (mCIM), while carbapenemase typing was validated by polymerase chain reaction (PCR) and Sanger sequencing. Antimicrobial susceptibility testing (AST) for ten antimicrobial agents was performed using broth microdilution (BMD) as the reference method. Results: The sensitivity and specificity of carbapenemase detection were 98.8% (95% CI, 96.6–99.6) and 92.4% (95% CI, 89.5–94.6) separately compared to sequencing.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
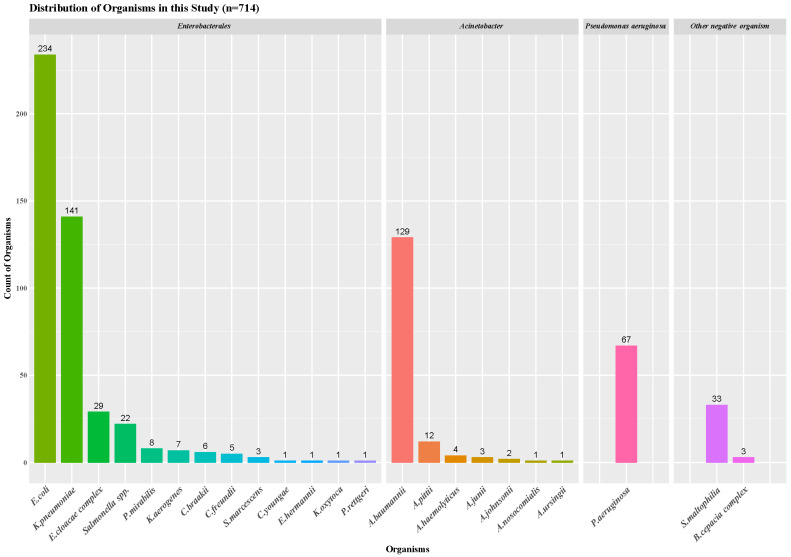 Figure 1
Figure 1- —National Science and Technology Major Project
- —National High-Level Hospital Clinical Research Funding
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Resistance in Bacteria · Bacterial Identification and Susceptibility Testing · Antibiotic Use and Resistance
1. Introduction
Carbapenemase-producing organisms (CPO) pose a global public health threat. In recent years, carbapenem-resistant Enterobacterales (CRE) and non-fermenting drug-resistant bacteria (Pseudomonas aeruginosa and Acinetobacter spp.) have remained prevalent. CHINET surveillance data indicate that carbapenem-resistant Klebsiella pneumoniae (CRKP) increased from 2.9% in 2005 to 25.0% in 2018, while carbapenem-resistant P. aeruginosa (CRPA) has shown a downward trend over the past decade, but in 2022, it still accounted for 23.8%, https://www.chinets.com/Data/GermYear (accessed on 28 February 2026). The proportion of carbapenem-resistant Acinetobacter spp. increased from 31% in 2005 to 74.5% in 2018, with a slight decrease to 65.8% in 2022 [1]. There are many reasons for the emergence of carbapenem resistance, such as changes or downregulation of porin proteins leading to reduced permeability, or carbapenemase-mediated hydrolysis of carbapenem antibiotics [2,3]. Among these mechanisms, the production of carbapenemase is the most common cause of carbapenem resistance [4]. Furthermore, clinical treatment options vary greatly depending on the carbapenemase types of bacterial strains. Therefore, rapid and accurate detection of the carbapenem-resistant bacterial strains is crucial in controlling the spread of carbapenem-resistant strains, a significant public health concern.
Carbapenemases are classified by the Ambler scheme into three main classes: A, B, and D. Class A carbapenemases, also known as serine carbapenemases (e.g., KPC), are primarily plasmid-mediated and inhibited by avibactam. Class B carbapenemases, also known as metallo-β-lactamases (e.g., NDM, IMP, VIM), are resistant to common β-lactamase inhibitors. Class D mainly comprises OXA-48 and its variants [5,6,7].
The global distribution of CPO has driven innovations in diagnostic technologies and tools to obtain quicker and more accurate results. In clinical microbiology laboratories, the results of antimicrobial susceptibility testing (AST) can provide information on the resistance of bacterial strains to carbapenem antibiotics, suggesting that the strain may produce carbapenemases. Currently, both phenotypic and molecular methods are used to detect the presence of carbapenemases. The most commonly used phenotypic tests include the Carba NP test, modified carbapenem inactivation method (mCIM), and lateral flow immunoassay [8].
In 2024, BD (Becton, Dickinson and Company) introduced the BD Phoenix NMIC-461 panel to China. This panel includes a range of antibiotics, such as imipenem, meropenem, ceftazidime–avibactam, and colistin, in various combinations, and it also has the capability to detect carbapenemases, classifying them according to the Ambler system. Prior to this, countries and regions worldwide had evaluated the performance of the BD Phoenix CPO-related panels using strains isolated within their own territories [7,8,9,10,11,12,13,14].
This multicenter study aimed to evaluate whether the BD Phoenix NMIC-461 panel provides accurate antimicrobial susceptibility testing and reliable carbapenemase classification for clinical isolates in China, thereby potentially serving as an efficient alternative to current methods.
2. Results
2.1. Isolates Information
In this study, 67 strains of Pseudomonas aeruginosa, 152 strains of Acinetobacter spp., 459 strains of Enterobacterales, and 36 other negative organisms were detected and analyzed. The number of bacteria enrolled in each species is shown in Figure 1.
2.2. Performance Evaluation of BD NMIC-461 Detection and Classification of Carbapenemase-Producing Organisms
2.2.1. Performance Evaluation of CPO Detection
A total of 498 bacterial isolates were included in the performance evaluation for the CPO detection, including 433 Enterobacterales and 65 P. aeruginosa. For the overall 498 isolates, both sensitivity and specificity were above 92%, with a NPV of 99.4% (95% CI, 97.9–99.8); however, the PPV was 83.1% (95% CI, 77.5–87.7). When analyzing Enterobacterales and P. aeruginosa separately, the Enterobacterales demonstrated excellent detection performance, with sensitivity, specificity, PPV, and NPV all exceeding 94%. In contrast, for P. aeruginosa, only the NPV was 97.4% (95% CI, 91.2–99.5), while the other three metrics were below 90%, with specificity and PPV as low as 65.5% (95% CI, 52.7–76.4) and 23.1% (95% CI, 13.7–31.6), respectively (Table 1).
2.2.2. Performance Evaluation of CPO Classification
A total of 654 bacterial isolates were included in the performance evaluation for the classification of CPO, consisting of 459 Enterobacterales, 129 Acinetobacter baumannii, and 66 P. aeruginosa. PCR detected 64 strains producing class A enzymes, 68 strains producing class B enzymes, and 117 strains producing class D enzymes (Table 2). Among these, one P. aeruginosa strain produced both class A and B enzymes, one A. baumannii strain produced both class B and D enzymes, and one Enterobacter cloacae strain produced two types of B enzymes (NDM and IMP). The NMIC-461 panel correctly identified only 6 out of the 64 strains producing class A enzymes, with the remaining 58 K. pneumoniae detected as positive, unclassified. Of the 68 strains producing class B enzymes, NMIC-461 successfully identified 61, with two strains being misclassified as producing class A and D enzymes, and 5 strains (two K. pneumoniae, one E cloacae, and one Citrobacter braakii) detected as positive unclassified. Among the 117 strains producing class D enzymes, NMIC-461 correctly identified 88, misclassified 3 as producing class B enzymes, 21 positive unclassified A. baumannii, and 3 negative A. baumannii. Of the 407 PCR-negative strains, NMIC-461 still detected 15, 10, 4, and 2 strains (one P. aeruginosa and one K. pneumoniae) as producing class A, B, D enzymes and positive unclassified, respectively (Table 2).
To assess the sensitivity, specificity, PPV, and NPV of the NMIC-461 panel in CPO classification, we calculated two sets of data. These calculations were performed by both including and excluding the 86 strains that were detected as positive unclassified by NMIC-461. The resulting data are presented in Table 2.
In the detection of class A β-lactamase, all of the 58 positive unclassified strains were K. pneumoniae. As a result, the sensitivity for Enterobacterales was only 7.9% (95% CI, 1.3–14.6). If these 58 strains were not included in the analysis, the sensitivity of Enterobacterales and all A-class enzyme-producing strains was 100%. The specificity and PPV for P. aeruginosa were both relatively low (78.8% (95% CI, 67.0–87.3) and 6.7% (95% CI, 1.2–32.0), respectively), indicating a high number of false positives (13 strains).
In the detection of Class B enzymes, the overall sensitivity was 89.7% (95% CI, 79.9–95.3) (97.1% (95% CI, 89.7–99.2) after excluding 4 positives, unclassified) with a specificity of 97.6% (95% CI, 96.0–98.6), demonstrating robust detection performance. For P. aeruginosa, specificity and NPV are 95.1% (95% CI, 86.6–98.3) and 96.7% (95% CI, 88.7–99.1), but the sensitivity and PPV were also relatively low [66.7% (95% CI, 31.0–89.1) and 57.1% (95% CI, 25.1–84.2), respectively], with 2 false negatives (one is positive, unclassified, one is class A). For Enterobacterales, sensitivity, specificity, PPV and NPV are 91.8% (95% CI, 81.9–96.6), 98.2% (95% CI, 96.4–99.2), 88.9% (95% CI, 79.0–94.4) and 98.7% (95% CI, 97.1–99.5), 5 false negatives (4 are positive, unclassified, 1 is class D).
In the detection of Class D enzymes, all true positive strains were identified as A. baumannii. The specificity, PPV, and NPV were 99.1% (95% CI, 97.8–99.7), 94.7% (95% CI, 88.4–97.7), and 95.0% (95% CI, 92.8–96.6) respectively, while sensitivity was slightly lower at 76.1% (95% CI, 67.2–83.2) (94.0% (95% CI, 87.9–97.3) after excluding 21 unclassified positive strains). NMIC-461 detected 28 false negatives (including 21 positives, unclassified, 4 class B, and 3 negatives), leading to relatively low sensitivity and NPV [76.1% (95% CI, 67.2–83.2) and 53.5% (95% CI, 41.3–65.0)], respectively, of A. baumannii. Additionally, one false positive (sequencing as class B) was identified among the Enterobacterales, and three false positives were detected in P. aeruginosa.
Overall, from the comprehensive evaluation of NMIC-461 for detecting CPO, sensitivity, specificity, and NPV all exceeded 90%, with PPV being slightly lower at 88.8% (95% CI, 84.5–92.1). However, certain limitations requiring further optimization were identified; the main issue with NMIC-461 in the detection of CPO was the high number of positive unclassified results, which accounted for 34.8% of all CPO positive strains (86/247). A total of 31 false positives were detected, including 20 cases of P aeruginosa, 10 cases in Enterobacterales, and 1 case of A. baumannii.
2.3. Performance of BD NMIC-461 AST Results
The provisions in CLSI M52 [15] were used as the criteria for the evaluation of CA, EA, MIE, ME, and VME of strains (Table 3). Overall, the NMIC-461 system demonstrates excellent performance in antimicrobial susceptibility testing for ten antibiotics across four bacterial categories. With EA exceeding 95% and CA exceeding 90% except for levofloxacin, ME and VME remain below 3% and 1.5%, respectively. These metrics indicate high accuracy and reliability in detecting antimicrobial susceptibility profiles.
Among the ten antibiotics evaluated, ceftazidime-avibactam and colistin—two key agents in clinical CPO management—showed particularly strong performance with NMIC-461. The system demonstrated 100% CA for ceftazidime-avibactam susceptibility testing against both Enterobacterales and P. aeruginosa, with EA rates of 97% and 100%, respectively. No ME or VME was detected for this antibiotic. Similarly, colistin testing-maintained CA and EA values exceeding 95% across Enterobacterales, P. aeruginosa, and Acinetobacter spp., with no VME observed during validation.
The ME rate for the detection of Acinetobacter spp. by ceftazidime was 4.8% (1/21). This observation may be attributed to the limited number of Acinetobacter spp. strains included in the study cohort. Nevertheless, the system-maintained CA and EA values exceeding 96%, with zero VME detected throughout the testing process. The CA rate for the detection of Enterobacterales by ciprofloxacin was somewhat reduced at 88.5% (376/425). The MIE rate of 11.5% was primarily attributed to excessive intermediate categorization, which compromised CA. Notably, EA remained robust at 97.9%, demonstrating preserved methodological accuracy despite interpretive challenges. For the detection of P. aeruginosa by imipenem, the ME rate was relatively high at 11.8% (2/17), and the CA rate was low at 83.3% (20/24). The comparative distributions of MICs for various bacterial strains, as determined by the NMIC-461 panel and the broth microdilution (BMD) method, are presented in Figures S2–S5.
3. Discussion
In this study, a total of 714 non-repetitive clinical isolates were initially enrolled. However, during the analysis of antimicrobial susceptibility or enzyme production capability, isolates that exhibited poor growth, no growth on the panel, or contamination were excluded from the corresponding statistical evaluations. As a result, the number of isolates included in the analysis varied across different antimicrobial agents. Detailed exclusion criteria and the corresponding numbers of excluded isolates are provided in Text S1.
In China, the rising isolation rate of CPOs has led to constrained therapeutic options. Current clinical management of CPO infections primarily relies on ceftazidime/avibactam, polymyxin B, tigecycline, and carbapenem-β-lactamase inhibitor combinations. As the CPO detection and classification results of this panel are reported at the same time with the above antibiotic drugs, compared to routine testing, the implementation of the CPO test allowed a mean reduction of 21.3 h (95% CI, 17.6–25) in turnaround time, 16.8 min (95% CI, 13.4–20.2) in hands-on time, and 20.6 CHF (95% CI, 16.5–24.8) in costs [16].
Notably, carbapenems such as imipenem remain empirically prescribed for Gram-negative bacterial infections prior to CPO confirmation through microbiological identification. Overall, the NMIC-461 demonstrated robust performance in AST for imipenem, with CA and EA both exceeding 95%, while ME and VME rates were maintained below 0.6%. The assay exhibited strong concordance for Enterobacterales and Acinetobacter spp. However, its performance was less robust for P. aeruginosa isolates. The ME rate was 11.8% (2/17), with both CA and EA falling below 90%. Previous studies have also reported low CA values for imipenem detection using BD panels [17]. Imipenem is typically degraded by dehydropeptidase-1 (DHP-1), necessitating co-administration with a DHP-1 inhibitor, such as cilastatin [16]. This characteristic of imipenem may contribute to the observed challenges in its susceptibility testing performance.
In the detection and classification of CPOs, NMIC-461 yielded a certain number of positive unclassified results, primarily involving 58 K. pneumoniae strains producing KPC and 21 A. baumannii strains producing OXA. However, in clinical isolates commonly encountered in China, Class A and Class D carbapenemase-producing strains are predominantly K. pneumoniae and A. baumannii, respectively [18,19]. Chinese antimicrobial-resistant bacterial strains share clonal dissemination with those from other countries/regions, yet exhibit distinct strain predominance patterns [20]. For instance, carbapenem-resistant K. pneumoniae (CRKP) predominantly exhibits sequence type ST11 in China, contrasting with the ST258 dominance observed in Europe and the United States [21].
Previous international studies on BD CPO panels from multiple countries have consistently detected positive unclassified strains harboring diverse resistance mechanisms [9,10,11,12,13,14], including various carbapenemase types, ESBLs, AmpC enzymes, and potentially novel uncharacterized carbapenemase resistance determinants. Phenotypic detection and classification of such strains remain challenging due to co-occurring resistance mechanisms that interfere with antimicrobial agent/β-lactamase inhibitor combination-based phenotypic assays [14]. Despite the number of unclassified positive results, NMIC-461 can still provide clinicians with a preliminary and actionable reference result in a timely manner.
NMIC-461 exhibited a higher rate of false positives in both the detection and classification of carbapenemase production in P. aeruginosa. This phenomenon may be attributed to the intrinsic or acquired resistance of P. aeruginosa to nearly all available antimicrobial agents. Multiple mechanisms can contribute to its antimicrobial resistance, including the production of carbapenemases, target site mutations, loss of outer membrane proteins, and multidrug efflux systems [9]. Resistance to carbapenems in P. aeruginosa is primarily mediated by non-carbapenemase mechanisms, such as the loss of OprD porin expression and/or upregulation of the MexAB-OprM efflux pump. The specificity of NMIC-461 may be compromised by the non-specific effects of inhibitors used in the assay, which can disrupt bacterial outer membrane permeability through chelation. Additionally, low carbapenem hydrolysis activity, lack of or minimal expression of carbapenemase genes, and slow bacterial growth could also contribute to the failure of NMIC-461 detection [12]. The reference method used to define which carbapenemases are present is limited to a specific set of genes, so some apparent false positives or positive unclassified results might actually be caused by other enzymes or resistance mechanisms that were not tested. Given these limitations, it is recommended that positive results be confirmed using an alternative method for P. aeruginosa.
In this study, we enrolled a sufficient number of isolates through a multicenter approach, particularly for Enterobacterales. In comparison with previous international studies of a similar nature, we revealed a higher incidence of positive unclassified results. Notably, our study demonstrated a low false-negative rate. After excluding positive unclassified strains, only two and seven false negatives were identified in class B and class D carbapenemase detection assays, respectively. However, false positives were observed in the detection of Class A, B, and D carbapenemases. Chiou et al. [7] evaluated the classification performance of Carba NP, mCIM, and BD Phoenix CPO in detecting carbapenemase production among 190 Enterobacterales isolates. The sensitivity and specificity of BD Phoenix CPO were 89.4% and 66.7%, respectively, while the other two methods achieved values above 90%. Similarly, Cho et al. [22] tested 47 carbapenemase-producing Enterobacterales (CPE), 52 carbapenem-resistant Enterobacterales without carbapenemase production (non-CP-CRE), and 136 carbapenem-susceptible Enterobacterales (CSE). The sensitivity and specificity for detecting CPOs were 97.9% and 100%, respectively, whereas the specificity for non-CP-CREs was only 32.7%. These findings also highlight the issue of significant false positives in carbapenemase detection assays.
In summary, the BD NMIC-461 panel can provide relatively reliable antimicrobial susceptibility results for commonly encountered Gram-negative bacterial isolates. BD NMIC-461 is capable of detecting and classifying CPO and integrates this functionality into routine antimicrobial susceptibility testing, which potentially reduces the turnaround time for CPO detection. The strains with unclassified positive results could be confirmed by other alternative methods and could refer to the related antibiotic agents’ results reported at the same time by the same panel. Clinicians can integrate MIC values of carbapenems, ceftazidime-avibactam, and colistin from the panel to inform therapeutic decisions (Table S2). Overall, implementation of the Phoenix NMIC-461 panel may positively influence laboratory workflow optimization and enhance evidence-based therapeutic and infection control strategies.
4. Materials and Methods
4.1. Isolates
In this study, we enrolled 714 non-repetitive clinical isolates from three tertiary hospitals in China, including 459 Enterobacterales, 152 Acinetobacter spp., 67 P. aeruginosa, and 36 other Gram-negative bacteria. The isolates were inoculated into cryovials containing 20% (w/v) skimmed milk and stored at −80 °C. From July 2020 to October 2022, the performance of the BD Phoenix NMIC-461 panel was evaluated at the three centers. The study was approved by the Research Ethics Committee of Peking Union Medical College Hospital (Ethical Approval Number: KS2021282).
4.2. BD Phoenix
The BD Phoenix NMIC-461 panel includes 10 antimicrobial agents that were evaluated, which include Amoxicillin-Clavulanic Acid, Ceftaroline, Ceftazidime-Avibactam, Ceftazidime, Ceftriaxone, Ciprofloxacin, Colistin, Imipenem, Levofloxacin, and Meropenem. The BMD method served as the reference method. The detection and classification of carbapenemase-producing organisms in this panel was evaluated compared to mCIM and sequencing.
Antimicrobial susceptibility testing is conducted according to the manufacturer’s instructions. A 0.5–0.6 McFarland turbidity standard bacterial suspension is prepared using the Phoenix turbidity meter. A 25 µL bacterial suspension is transferred into Phoenix AST broth, and before adding it to the plates, one drop of Phoenix AST indicator is added to detect microbial growth. The panel is sealed, recorded, and loaded into the Phoenix M50 system. After incubation for 16 h, the results are interpreted using the Epicenter Data Management Software, Version 7.22A (BD Diagnostics, Franklin Lakes, NJ, USA) [17].
4.3. Broth Microdilution (BMD)
The standard BMD method is performed according to the guidance document ISO 20776-1 [23]. E. coli ATCC 25922, P. aeruginosa ATCC 27853, K. pneumoniae ATCC 700603, and K. pneumoniae ATCC BAA-1705 were used as quality control strains as recommended by Clinical and Laboratory Standards Institute (CLSI) M100, 2023 [24].
4.4. Modified Carbapenem Inactivation Method (mCIM)
In this study, mCIM was used as the control method for carbapenemase production in isolates. mCIM was performed according to the CLSI guidelines to detect the presence of carbapenemase [24]. For each isolate tested, a 1 μL loopful of bacteria for Enterobacterales or a 10 μL loopful of bacteria for Pseudomonas aeruginosa from an overnight blood agar plate was emulsified in 2 mL Trypticase Soy Broth (TSB). A 10 µg meropenem disk was placed in each tube, and the tubes were incubated at 35 °C for 4 h ± 15 min. Subsequently, the disks were removed and applied to MH agar plates (Oxoid, Basingstoke, UK) freshly plated with a 0.5 McFarland suspension of a carbapenem-susceptible E. coli ATCC 25922 strain. The plates were incubated at 35 °C for 16–20 h. The mCIM result was considered to be carbapenemase negative if the zone diameter was ≥19 mm, positive if the zone diameter was 6–15 mm, or the presence of pinpoint colonies within a 16–18 mm zone. The presence or absence of a carbapenemase could not be confirmed if the zone diameter was 16–18 mm or ≥19 mm, and the presence of pinpoint colonies within the zone.
4.5. Screening of Carbapenemase Genes
All enrolled Enterobacterales, P. aeruginosa, and Acinetobacter spp. were Sanger sequenced, and Ambler classified to determine whether the enzyme class detected by the NMIC-461 plate was accurate. The polymerase chain reaction (PCR) and Sanger sequencing were employed to screen out carbapenemase genes, including KPC, NDM, VIM, IMP, OXA-48, OXA-23, OXA-24, and OXA-58. The oligonucleotide sequences of the primers are listed in Supplementary Table S1. The PCR products were sequenced and analyzed using BLAST (Version 2.17.0), http://www.ncbi.nlm.nih.gov/BLAST, (accessed on 28 February 2026). The BLAST cut-off was a percentage identity of 100%.
4.6. Data Analysis
Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated to assess the ability of NMIC-461 to detect carbapenemase-producing compared to mCIM and carbapenemase genes. The same parameters were also used to assess the ability of NMIC-461 to detect enzyme-producing Ambler classification of strains. Agreement and validity values were calculated with a 95% confidence interval (CI) based on an exact binomial distribution. For the drugs with BMD as the control method, essential agreement (EA), category agreement (CA), minor error (MIE), major error (ME), and very major error (VME) were calculated separately [15]. All analyses were performed using R Statistical Software (v4.4.0; R Core Team 2024).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Qin X. Ding L. Hao M. Li P. Hu F. Wang M. Antimicrobial resistance of clinical bacterial isolates in China: Current status and trends JAC Antimicrob. Resist.20246 dlae 05210.1093/jacamr/dlae 05238549710 PMC 10977948 · doi ↗ · pubmed ↗
- 2Tenover F.C. Nicolau D.P. Gill C.M. Carbapenemase-producing Pseudomonas aeruginosa—An emerging challenge Emerg. Microbes Infect.20221181181410.1080/22221751.2022.204897235240944 PMC 8920394 · doi ↗ · pubmed ↗
- 3Sfeir M.M. Hayden J.A. Fauntleroy K.A. Mazur C. Johnson J.K. Simner P.J. Das S. Satlin M.J. Jenkins S.G. Westblade L.F. EDTA-Modified Carbapenem Inactivation Method: A Phenotypic Method for Detecting Metallo-beta-Lactamase-Producing Enterobacteriaceae J. Clin. Microbiol.201957 e 01757-1810.1128/JCM.01757-1830867235 PMC 6498035 · doi ↗ · pubmed ↗
- 4Logan L.K. Weinstein R.A. The Epidemiology of Carbapenem-Resistant Enterobacteriaceae: The Impact and Evolution of a Global Menace J. Infect. Dis.2017215 S 28S 3610.1093/infdis/jiw 28228375512 PMC 5853342 · doi ↗ · pubmed ↗
- 5Bush K. Past and Present Perspectives on beta-Lactamases Antimicrob. Agents Chemother.20186210112810.1128/AAC.01076-18PMC 615379230061284 · doi ↗ · pubmed ↗
- 6Queenan A.M. Bush K. Carbapenemases: The versatile beta-lactamases Clin. Microbiol. Rev.20072044045810.1128/CMR.00001-0717630334 PMC 1932750 · doi ↗ · pubmed ↗
- 7Ong C.H. Ratnayake L. Ang M.L.T. Lin R.T.P. Chan D.S.G. Diagnostic Accuracy of BD Phoenix CPO Detect for Carbapenemase Production in 190 Enterobacteriaceae Isolates J. Clin. Microbiol.201856 e 01043-1810.1128/JCM.01043-1830209186 PMC 6258855 · doi ↗ · pubmed ↗
- 8Jonas D. Reuter S. Klassen S. Weber S. Buck M. Giani T. Rossolini G.M. Grundmann H. Evaluation of the BD Phoenix CPO detect panel for prediction of Ambler class carbapenemases Sci. Rep.2021111315010.1038/s 41598-021-92336-334162904 PMC 8222379 · doi ↗ · pubmed ↗