Parental Knowledge, Attitudes and Practices on Antibiotic Use in Children: A Cross-Sectional Study from Tbilisi, Georgia
Tata Imnadze, Nana Mebonia, Lile Malania, Ekaterine Ruadze

TL;DR
This study in Tbilisi, Georgia, finds that many parents misuse antibiotics for their children due to knowledge gaps, contributing to antimicrobial resistance.
Contribution
The study provides new insights into parental antibiotic use behaviors and knowledge gaps in Georgia, a low- to middle-income country.
Findings
27.9% of parents engaged in at least one inappropriate antibiotic practice.
High parental knowledge was associated with lower inappropriate antibiotic use.
Forty percent of parents incorrectly believed antibiotics kill viruses.
Abstract
Background/Objectives: Inappropriate antibiotic use in children is a major driver of antimicrobial resistance (AMR), especially in low- and middle-income countries. In Georgia, little is known about parental behaviors related to pediatric antibiotic use. This cross-sectional study assessed knowledge, attitudes, and practices (KAP) related to antibiotic use and AMR among parents of preschoolers in Tbilisi kindergartens, identifying factors associated with inappropriate practices to inform stewardship interventions. Methods: During March–May 2025, we conducted a two-stage cluster-sampled cross-sectional survey of parents of children aged 2–6 years attending public kindergartens in Tbilisi, Georgia. We assessed knowledge, attitudes, and practices concerning antibiotics and AMR. Multivariable Poisson regression was utilized to identify factors associated with inappropriate antibiotic use,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
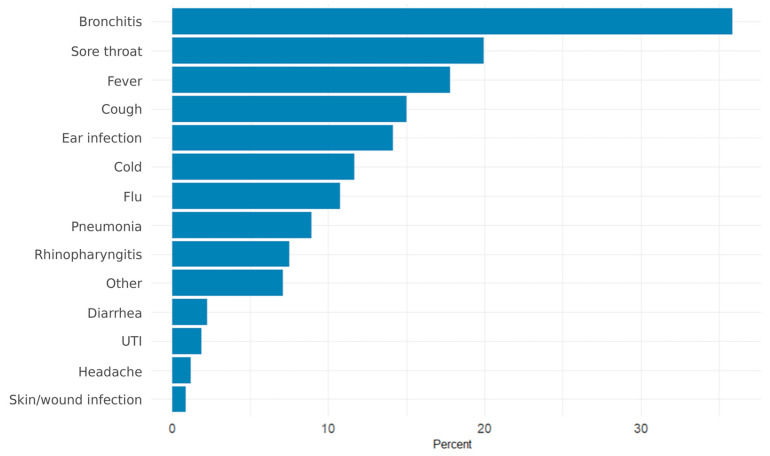 Figure 1
Figure 1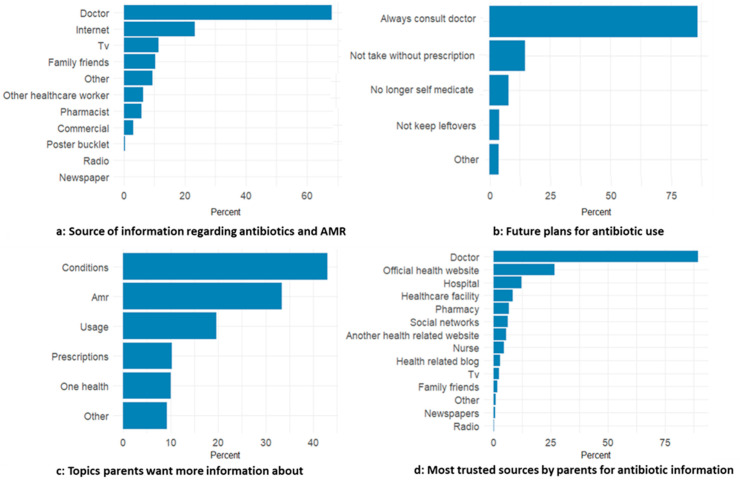 Figure 2
Figure 2- —European Union
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Use and Resistance · Pharmaceutical studies and practices · Pneumonia and Respiratory Infections
1. Introduction
Antimicrobial resistance (AMR) is a major global health threat. It was estimated to be associated with 4.95 million deaths in 2019, including 1.27 million deaths directly attributable to resistant infections [1]. Inappropriate antibiotic use is a key driver, especially in outpatient and community settings where regulatory oversight is weak and diagnostic support is limited [2,3]. In children, antibiotics are frequently prescribed for conditions such as viral upper respiratory tract infections, despite clear clinical guidelines advising against their use in these self-limiting, non-bacterial illnesses [4,5,6]. In several settings, more than one in five outpatient visits result in an antibiotic prescription, and early and repeated exposure in childhood contributes to the emergence and spread of AMR [7,8].
Misuse is influenced by limited public awareness, sociocultural expectations, and gaps in pharmaceutical regulation. Practices such as obtaining antibiotics without prescription, stopping treatment early, and using antibiotics without diagnostic confirmation contribute to resistance and pose individual risks for children [9,10,11]. Studies from low- and middle-income countries show that caregivers often have limited knowledge about antibiotics and AMR, hold misconceptions about when antibiotics are appropriate, and may self-medicate or pressure clinicians to prescribe [10,12,13,14,15]. Structural and social determinants, including maternal education, household income, and access to healthcare, further influence these practices [16,17,18].
Children are particularly vulnerable: early-life antibiotic exposure can disrupt the developing microbiome and has been linked to long-term health consequences such as asthma, obesity, and immune dysregulation in both human and animal studies [19,20]. These risks make caregiver practices a critical target for stewardship, especially in settings where enforcement of prescription-only policies is inconsistent.
In Georgia, policy efforts to contain AMR have included the development of a national action plan and formal regulations prohibiting over-the-counter antibiotic sales [21,22]. However, enforcement remains inconsistent, and informal dispensing still occurs. Public knowledge about AMR is low [23], and no published studies have focused on caregivers of young children, a group that strongly influences household antibiotic use. Existing studies have primarily focused on adults, healthcare workers, or institutional settings [2]. Notably, a point prevalence study (PPS) conducted between 2015 and 2019 in Georgian pediatric hospitals revealed widespread empirical antibiotic prescribing and limited microbiological testing, highlighting broader systemic challenges in antimicrobial stewardship—even within the formal healthcare system [24].
Parents of children aged 2–6 years represent a particularly relevant population for antimicrobial stewardship research. Preschool children frequently present with respiratory infections in outpatient settings [25], where antibiotics are commonly prescribed, placing caregivers at the center of antibiotic-related decision-making within the household. Public kindergartens provide a structured and geographically distributed sampling frame, enabling cluster-based recruitment of caregivers and enhancing population-level representation across Tbilisi.
To address this gap, we conducted a cross-sectional study to assess the knowledge, attitudes, and practices (KAP) related to antibiotic use and AMR among parents of young children attending public kindergartens in Tbilisi, Georgia. We also aimed to identify sociodemographic and KAP-related factors associated with inappropriate antibiotic practice, with the goal of informing targeted interventions and contributing to Georgia’s broader AMR containment strategy.
2. Results
2.1. Participant Characteristics
A total of 639 parents participated (response rate 85.2%). Most respondents were women (93.4%), and the majority were aged 25–39 years (71.8%). Nearly half held a bachelor’s degree (47.2%). Weighted characteristics closely matched the unweighted sample distribution (Table 1).
2.2. Antibiotic Use in Children
Overall, 64.3% of parents (n = 412, 95% CI 60.3–68.1) reported giving their child antibiotics in the past 12 months. Among parents of 2–3-year-olds, the reported prevalence was (68.9%, 95% CI 63.2–74.6).
Among those who administered antibiotics, most reported 1–2 treatment courses in the past year (78.6%, 95% CI 73.7–83.4). Smaller proportions reported 3–5 courses (11.5%, 95% CI 7.7–15.3) or more than 5 courses (3.1%, 95% CI 1.5–4.6).
Among antibiotic users in the past year, 27.9% (n = 114, 95% CI 23.3–32.9) engaged in at least one caregiver-controlled inappropriate practice (early discontinuation, use without a prescription, or saving leftovers).
2.3. Reasons for Antibiotic Use
Among parents or guardians who had sought antibiotic treatment for their children, the most frequent reasons were bronchitis (35.9%, 95% CI 31.7–40.1), sore throat (20.0%), fever (17.8%), cough (15.0%), ear infections (14.2%), and colds (11.7%) (Figure 1).
2.4. Sources and Administration of Antibiotics
Most antibiotics were given following a medical prescription (77.5%, 95% CI 72.8–82.2). Administration by a practitioner was reported by 16.8% (95% CI 12.6–21.0). Use based on prior experience (3.8%, 95% CI 1.8–5.8) or the advice of a pharmacist (0.4%) was uncommon.
Non-prescription acquisition was reported by 18.6% (95% CI 14.1–22.6) of parents. Pharmacies remained the primary source of antibiotics overall, with 62.3% (95% CI 56.8–67.8) of parents obtaining the most recent course with a prescription.
Diagnostic testing before treatment was reported by 79.2% (95% CI 74.0–84.3), while 20.6% (95% CI 15.4–25.8) reported no testing.
2.5. Knowledge About Antibiotics and AMR
Knowledge levels varied across topics. About four in ten parents believed antibiotics kill viruses (39.7%, 95% CI 34.6–44.7), while a similar proportion correctly disagreed. Over half (57.7%, 95% CI 52.4–63.0) knew that antibiotics do not help against influenza-like illness.
Most parents recognized that unnecessary antibiotic use can reduce effectiveness (74.0%, 95% CI 69.8–78.2).
Awareness of side effects was moderate: 60.9% (95% CI 56.3–65.6) knew antibiotics may cause adverse effects such as diarrhea.
The mean knowledge score was 2.3 (SD 1.3) out of 4, with a median of 2 (IQR 1–3) (Appendix A, Table A1). Overall, 10.0% of parents (95% CI 7.5–12.5) answered none of the knowledge items correctly, 18.2% (95% CI 14.6–21.9) scored one, 25.6% (95% CI 21.9–29.4) scored two, 22.3% (95% CI 18.5–26.1) scored three, and 23.8% (95% CI 19.1–28.5) achieved full scores. These findings indicate moderate overall knowledge with considerable heterogeneity and no clear clustering at the extremes.
2.6. Attitudes Toward Antibiotic Use
The majority of parents reported that they would consult a doctor before giving antibiotics to their child (87.2%, 95% CI 83.1–91.3).
Desire for antibiotic prescriptions was mixed: 57.4% (95% CI 52.7–62.1) did not desire the doctor to prescribe antibiotics when their child was ill, while 25.6% (95% CI 21.0–30.1) somewhat desired one, and 10.1% (95% CI 7.0–13.3) strongly desired one.
The mean attitude score was 1.47 (SD 0.62), with a median of 2 (IQR 1–2). A total of 6.2% of parents (95% CI 3.6–8.8) had the lowest attitude score, 39.4% (95% CI 34.9–43.9) had intermediate scores, and 52.4% (95% CI 47.3–57.6) had the highest attitude score.
2.7. Reported Practices
Completion of prescribed treatment was common: 70.4% (95% CI 66.4–74.4) reported always completing the course. Early discontinuation occurred in 14.7% (95% CI 11.4–17.9).
Among those who stopped treatment early, most did so because the child improved (67.6%, 95% CI 54.7–80.5). Side effects (21.7%) and child refusal (9.5%) were less frequent reasons.
Among parents who had given antibiotics to their children (n = 412), practice scores showed that most did not report any inappropriate practices. The mean practice score was 0.33 (SD 0.58), median 0 (IQR 0–1). Appropriate practice (score = 0) was observed in 72.1% (95% CI 67.3–76.9), while 22.4% (95% CI 17.8–27.1) reported one inappropriate practice, 5.3% (95% CI 3.1–7.5) reported two, and <1% reported three.
Reported actions linked to inappropriate practice are summarized in Table 2. Component behaviors included non-prescription acquisition (18.6%), early discontinuation (14.7%), and storing leftover antibiotics for later use (8.1%).
2.8. Information Sources and Perceived Impact
One-third of parents (34.2%, 95% CI 30.0–38.4) reported receiving information about antibiotics or AMR in the past year. Among them, 74.5% (95% CI 68.6–80.4) stated that this information changed their views.
As shown in Figure 2a, doctors were the most commonly reported information source, followed by the internet, while traditional media and interpersonal sources were less frequently reported. Figure 2b indicates that most parents intended to always consult a doctor, and a smaller proportion reported plans to avoid using antibiotics without a prescription. In Figure 2c, parents most often wanted more information on which conditions require antibiotics and on AMR, followed by safe use and prescription-related topics. Figure 2d shows that doctors were the most trusted source (89.4%, 95% CI 86.9–91.8), followed by official websites (26.7%). Trust in all other sources was below 12%.
2.9. Crude Associations with Inappropriate Antibiotic Practice
In crude regression analysis, several factors were associated with inappropriate antibiotic practice (Table 3).
Higher education, higher income, having two children, high knowledge, and positive attitudes were each associated with lower prevalence of inappropriate use.
Misconceptions showed the strongest associations: parents who believed antibiotics help for colds had more than twice the prevalence of inappropriate practice (PR 2.17, 95% CI 1.52–3.09), and those uncertain whether unnecessary antibiotic use leads to reduced effectiveness also reported higher misuse (PR 1.75, 95% CI 1.23–2.48). Misconceptions about cold treatment and uncertainty about AMR showed the largest relative differences in prevalence.
2.10. Multivariable Model
After restricting analyses to participants with complete data, multivariable models were fitted among parents who reported antibiotic use in the past year, accounting for clustering by kindergarten. Variance inflation factors indicated no concerning collinearity among predictors (all GVIF^(1/2df)^ < 1.2).
In the adjusted model (Appendix A, Table A2), only knowledge level remained significantly associated with inappropriate antibiotic practice. Parents with high knowledge scores had a lower adjusted prevalence of inappropriate use compared with those with low knowledge scores (aPR 0.66, 95% CI 0.45–0.97).
Number of children showed a borderline association: parents with two children had somewhat lower prevalence of inappropriate practice compared with those with one child, although this did not reach statistical significance (aPR 0.68, 95% CI 0.45–1.04).
Household income, parental education, and attitude were not significantly associated with inappropriate practice after adjustment (p > 0.05 for all).
3. Discussion
3.1. Summary of Main Findings
This study provides new evidence on antibiotic-related knowledge, attitudes, and practices among parents of young children in Tbilisi, Georgia. Antibiotic exposure in early childhood was common. Nearly two-thirds of parents reported administering antibiotics to their child in the past 12 months, with even higher use among parents of two- and three-year-olds. These levels exceed estimates reported for the general population in Georgia [23] and raise concern given the vulnerability of the developing childhood microbiome.
Despite generally moderate knowledge and positive attitudes, inappropriate caregiver-controlled practices persisted. About one in four parents who had used antibiotics reported at least one inappropriate behavior, most commonly non-prescription acquisition, followed by early discontinuation, or storage of leftovers. While appropriate behaviors were reported by many parents, the persistence of these practices highlights ongoing risks for antimicrobial resistance.
High antibiotic use among preschool-aged children is consistent with patterns reported in many settings where respiratory symptoms are frequent and diagnostic uncertainty is common. However, the magnitude observed in this study suggests that antibiotic exposure in Georgia remains high despite prescription-only regulations and clinical guidelines that discourage antibiotic use for viral infections.
Importantly, most antibiotics reported in this study were prescribed by healthcare professionals. This suggests that caregiver-controlled inappropriate practice is not driven solely by parental misunderstanding or non-prescription acquisition. Instead, it occurs within a wider care pathway in which most antibiotic courses are clinician-prescribed. We did not assess the appropriateness of clinician prescribing; however, contextual factors such as diagnostic uncertainty, limited diagnostic support, and parental expectations during acute illness episodes may influence antibiotic use. Similar patterns have been reported in other low- and middle-income countries in the WHO European Region, where legal restrictions coexist with high pediatric antibiotic use.
Non-prescription acquisition was reported despite formal regulations. This suggests an implementation gap between policy and practice rather than absence of regulation. Without consistent enforcement and accountability mechanisms, prescription-only laws alone are unlikely to substantially reduce inappropriate antibiotic use.
The most frequently reported indication for antibiotic use was bronchitis. This finding should be interpreted cautiously. In routine outpatient practice, diagnostic labels such as “bronchitis” may be applied broadly and may encompass a mix of viral and bacterial respiratory syndromes. Because diagnoses were parent-reported and not clinically validated, we cannot determine whether antibiotic prescribing was clinically appropriate for specific episodes. Diagnostic labeling may also shape parental expectations regarding antibiotic treatment, complicating efforts to distinguish caregiver behavior from provider prescribing norms.
Although a high proportion of parents reported that diagnostic testing preceded antibiotic use, this finding should be interpreted cautiously. The survey did not specify the type of test performed, and caregiver interpretations of “testing” may include physical examination, blood tests, or imaging rather than microbiological diagnostics. In outpatient pediatric care in Georgia, bacteriological testing and antimicrobial susceptibility testing are rarely performed prior to treatment, and prescribing is largely empirical. Therefore, reported testing should not be interpreted as evidence of guideline-concordant diagnostic stewardship.
Poor understanding or misconceptions about antibiotics and their use emerged as the strongest correlate of inappropriate practice. Parents with higher knowledge scores had a lower prevalence of inappropriate behaviors, while education, income, and attitudes were not independently associated after adjustment. This finding should not be interpreted causally. Antibiotic use is also influenced by prescribing and dispensing contexts, so knowledge alone may not fully determine behavior. The cross-sectional design cannot establish whether knowledge leads to better practice or whether parents who behave appropriately acquire more accurate information. Still, the association supports existing evidence that correcting specific misconceptions may be a practical intervention target. Our findings on caregiver knowledge should be interpreted within this broader context. Because our primary outcome combined several caregiver-controlled practices, determinants may differ by practice, and future analyses could model these components separately.
3.2. Strength and Limitations
Strengths include the cluster sampling approach, large, representative sample, high response rate, and a clearly defined outcome focused on caregiver-controlled behaviors. The use of GEE models appropriately accounts for clustering at the kindergarten level.
Several limitations must be considered in interpreting our findings.
Selection bias is possible, as we could not confirm strict adherence to the distribution protocol in kindergartens. More engaged or health-conscious parents may have been more likely to participate, potentially inflating knowledge scores or underestimating misuse. Despite follow-up with kindergarten managers, non-random participation remains a concern.
Social desirability bias may have also led to underreporting of sensitive practices, such as self-medication or early treatment discontinuation. If present, such biases likely result in conservative estimates meaning actual rates of misuse may be even higher.
Recall bias is inherent in self-reported data, especially over a 12-month reference period. Some parents may have misclassified symptom episodes or antibiotic courses. We attempted to mitigate this by focusing on the past year, but inaccuracies remain. Non-response bias is another consideration: some kindergartens had incomplete returns, and non-responders may systematically differ from participants. While we used post-stratification weights to adjust for this, residual bias may persist.
Measurement limitations also apply. The binary KAP scoring system may oversimplify complex decision-making and reduce variability by collapsing potentially meaningful gradients in knowledge and attitudes. In addition, dichotomization the knowledge score may have reduced detail and limited detection of more nuanced associations. Treating “don’t know” responses as incorrect may conflate uncertainty with misinformation. In the practice score, all inappropriate behaviors were weighted equally despite differing clinical implications.
Finally, survey terminology may have been interpreted inconsistently. “Diagnostic testing” may have referred to anything from a physical examination to laboratory tests. Reported indications should therefore be interpreted as caregiver perceptions rather than verified clinical diagnoses. Diagnostic labels such as “bronchitis” may be used broadly in routine practice and may represent heterogeneous syndromes, including viral and bacterial conditions. This limits inference about appropriateness by indication. Similarly, “administered by a healthcare provider” might have been read as “prescribed by” rather than literal administration especially given the focus on oral medications. Additionally, high reported frequencies of antibiotic use (e.g., >5 times/year) among healthy children suggest misunderstanding of what constitutes a treatment course. This may have led to overestimation of true antibiotic exposure.
4. Materials and Methods
4.1. Study Design and Setting
We conducted a cross-sectional survey among parents of children aged 2–6 years enrolled in public kindergartens in Tbilisi, Georgia. Data collection took place between March and May 2025. The study aimed to measure parental KAP regarding antibiotic use and antimicrobial resistance (AMR).
In Georgia, public kindergartens are municipal early childhood education settings that enroll preschool-aged children, including children aged 2–6 years.
4.2. Study Population
Eligible participants were parents aged 18 years or older who had a child attending one of the selected public kindergartens; one parent per child was invited to participate. Parents unable to read Georgian were excluded. Participation was voluntary, and returning a completed questionnaire implied informed consent.
4.3. Sample Size Estimation and Sampling Strategy
The minimum required sample size was calculated using a single proportion formula, assuming a 50% prevalence of inappropriate antibiotic practice, 5% margin of error, and 95% confidence level. This yielded 385 participants. Because the study used a cluster sampling design, we applied a design effect of 1.6, informed by WHO guidance for complex survey designs and selected as a conservative value [26], resulting in 616 participants. To account for an anticipated 20% non-response rate, the target sample size was increased and rounded up to 750 parents.
We used a two-stage cluster sampling design. In stage one, 50 kindergartens were selected from all 190 public kindergartens in Tbilisi, using probability proportional to size (PPS) based on total child enrollment. In the second stage, a fixed number of 15 questionnaires per selected kindergarten were distributed to parents. To capture potential variation in antibiotic use across child age groups, each kindergarten was assigned a specific age group (2–5 years) for targeted distribution.
The PPS design combined with a fixed number of questionnaires per kindergarten produced a mathematically self-weighting sample. Non-response weights were calculated as the inverse of the kindergarten-specific response rate. These weights were normalized to a mean of 1.0 for variance estimation.
4.4. Instruments and Data Collection
A structured, paper-based questionnaire was adapted from the WHO European Region knowledge, attitudes and behaviors survey on antibiotic use and AMR (2022) [23], with modifications for relevance to caregivers of young children in Georgia. Additional items were based on publicly available KAP surveys. The adapted Georgian version was reviewed for clarity and cultural appropriateness by the study team, with consultation from a practicing pediatrician and AMR/public health specialist. The instrument was pilot-tested before field implementation.
Questionnaires were distributed via kindergarten staff to eligible parents and returned anonymously. Staff were instructed that participation was voluntary and that they should not track which parents responded.
4.5. Measures and Variable Definitions
Sociodemographic information included parent age, sex, education, employment status, household income, and number of children (Details on category collapsing and variable recoding are provided in Appendix B, Section Category Collapsing and Variable Recoding Strategy).
The primary outcome was inappropriate antibiotic practice. This captured caregiver-controlled behaviors inconsistent with recommended stewardship, specifically: obtaining antibiotics without a prescription, stopping a prescribed course prematurely, or storing antibiotics for future use. Each inappropriate practice (including “don’t know”) was given a score of 1, while appropriate practice was scored as 0. A binary outcome classified respondents as having appropriate practice (score = 0) or inappropriate practice (score ≥ 1) if they reported at least one of the three inappropriate behaviors. Provider-driven factors, such as antibiotics prescribed for viral illnesses or absence of diagnostic testing, were not included in the definition because these decisions fall outside parental control.
Knowledge about antibiotics and antimicrobial resistance was measured using four factual items assessing whether respondents understood that antibiotics do not kill viruses, are not effective for colds, that unnecessary antibiotic use reduces its effectiveness, and that antibiotics may cause side effects, such as diarrhea. Each correct answer was given a score of 1, while incorrect and “don’t know” responses were scored as 0. “Don’t know” responses were grouped with incorrect answers because both indicate absence of correct knowledge relevant to antibiotic use. A total Knowledge Score (range 0–4) was calculated and dichotomized into high knowledge (≥3 correct responses) and low knowledge (≤2 correct responses). Dichotomization was used to improve interpretability and to limit model complexity given events-per-variable considerations in the multivariable analysis.
Parental attitudes toward antibiotic use were measured using two items that assessed the desire for antibiotic prescription from a doctor when a child is ill and the likelihood of consulting a doctor before giving antibiotics. Responses indicating appropriate attitudes (not desiring an antibiotic prescription and intending to consult a doctor before giving antibiotics to their child) were scored as 1. The resulting Attitude Score ranged from 0–2 and was categorized as positive (score of 2) or negative (score of 0–1).
4.6. Data Entry and Management
Completed questionnaires were entered into KoboToolbox (server version 2.025.x) and exported to R (version 4.3.1). Data entry and cleaning occurred concurrently. Logical checks, skip pattern verification, and cross-validation with original questionnaires were performed to minimize errors. No personal identifiers were collected.
4.7. Statistical Analysis
All analyses were conducted in R (version 4.3.1). Data were first described using weighted proportions and 95% confidence intervals, applying normalized non-response weights. Weighted estimates were obtained with the survey R-package (version 4.4-2), specifying kindergarten as the primary sampling unit and using Taylor linearization for variance estimation.
For analytical models, we used generalized estimating equations (GEE) with a Poisson distribution [27] and log link to estimate adjusted prevalence ratios (PR) and 95% confidence intervals for the common outcome. Kindergarten was specified as the clustering variable, with an independence working correlation structure. Robust (sandwich) standard errors were used to account for within-cluster correlation.
Covariates for the multivariable model were selected based on conceptual relevance, evidence of association in crude analyses (95% confidence intervals excluding the null value), and assessment of multicollinearity using generalized VIF. Multicollinearity was assessed across all candidate predictors considered for the multivariable model; no concerning collinearity was observed. The number of predictors was constrained according to events-per-variable considerations to minimize overfitting. The final model included parental education, socio-professional category, household income, number of children, knowledge level, and attitude. Number of antibiotic courses was not included due to evidence of recall error and implausible values. Sex and age of parents were excluded because they showed no association in crude analyses. As sensitivity analyses, we fitted survey-weighted and unweighted Poisson models with a log link and unweighted logistic regression models. These produced similar patterns of association and did not change the substantive conclusions, so we report unweighted GEE Poisson results as the primary analysis.
4.8. Ethical Considerations
Ethical approval was obtained from the Institutional Review Board of the National Center for Disease Control and Public Health (NCDC), Georgia (IRB #2022-085). The questionnaire was anonymous and no identifiable information was collected.
4.9. Generative AI Disclosure
Generative artificial intelligence tools (ChatGPT by OpenAI) were used to assist with wording refinement, and structural editing. No AI tools were used for data collection, analysis, or interpretation. All statistical analyses were performed by the authors.
5. Conclusions
This study provides the first targeted assessment of antibiotic-related knowledge, attitudes, and practices among parents of young children in Georgia. The findings highlighted a disconnect between recommended antibiotic stewardship practices and real-world antibiotic use, shaped by both caregiver behavior and provider prescribing practices. A substantial proportion of parents reported inappropriate antibiotic use, indicating that misuse remains normalized across social and educational groups rather than confined to specific subpopulations. Knowledge deficits emerged as the most consistent correlate of inappropriate practices, while demographic characteristics showed limited explanatory value.
These findings suggest that efforts to improve antibiotic stewardship in Georgia must extend beyond general awareness raising. Targeted correction of common misconceptions, particularly regarding antibiotic use for viral illnesses, early discontinuation, and reuse of leftovers, remains necessary. Given that healthcare professionals were identified as the most trusted information source, stewardship messaging is likely to be most effective when integrated into routine maternal and child health services, vaccination visits, and pediatric consultations.
At the same time, improving parental knowledge alone will be insufficient. Most antibiotics reported in this study were prescribed by clinicians, indicating important opportunities to strengthen outpatient antimicrobial stewardship. Because prescribing appropriateness was not measured, our outcome reflects caregiver-controlled behaviors rather than clinician decision-making. Strengthening guideline-concordant prescribing, enhancing diagnostic support, and reinforcing stewardship practices in ambulatory pediatric care are critical priorities.
Regulatory enforcement also requires attention. Reported non-prescription access to antibiotics suggests fragmented implementation of prescription-only policies. Strengthening verification mechanisms, pharmacy oversight, and monitoring systems is essential to ensure that existing regulations translate into practice.
Overall, these findings provide a baseline for monitoring antibiotic-related behaviors among parents of young children in Tbilisi and for evaluating future interventions under Georgia’s national antimicrobial resistance strategy. Coordinated action across education, clinical practice, and regulation will be required to close the gap between policy, knowledge, and practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO Antimicrobial Resistance. Key Facts Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance(accessed on 18 May 2025)
- 2Kandelaki K. Lundborg C.S. Marrone G. Antibiotic Use and Resistance: A Cross-Sectional Study Exploring Knowledge and Attitudes among School and Institution Personnel in Tbilisi, Republic of Georgia BMC Res. Notes 2015849510.1186/s 13104-015-1477-126420302 PMC 4589112 · doi ↗ · pubmed ↗
- 3Dantuluri K.L. Bonnet K.R. Schlundt D.G. Schulte R.J. Griffith H.G. Luu A. Charnogursky C. Perkins J.M. Whitmore C.C. Banerjee R. Antibiotic Perceptions, Adherence, and Disposal Practices among Parents of Pediatric Patients P Lo S ONE 202318 e 028166010.1371/journal.pone.028166036758043 PMC 9910628 · doi ↗ · pubmed ↗
- 4Alumran A. Hurst C. Hou X.-Y. Antibiotics Overuse in Children with Upper Respiratory Tract Infections in Saudi Arabia: Risk Factors and Potential Interventions Clin. Med. Diagn.2011181610.5923/j.cmd.20110101.02 · doi ↗
- 5Amin M.T. Abd El Aty M.A. Ahmed S.M. Elsedfy G.O. Hassanin E.S. El-Gazzar A.F. Over Prescription of Antibiotics in Children with Acute Upper Respiratory Tract Infections: A Study on the Knowledge, Attitude and Practices of Non-Specialized Physicians in Egypt P Lo S ONE 202217 e 027730810.1371/journal.pone.027730836327297 PMC 9632891 · doi ↗ · pubmed ↗
- 6Alidema F.B. Hasani Alidema A. Mustafa L.S. Havolli M. Abazi F. Prevalence and Patterns of Antibiotic Prescribing Among Children Aged 1–7 Years in Primary Health Care Centers in Prishtina and Ferizaj, Kosovo (2022–2025): A Retrospective Observational Study Antibiotics 202514128210.3390/antibiotics 1412128241463782 PMC 12729371 · doi ↗ · pubmed ↗
- 7Pitaloka D.A.E. Insyirah A. Oktariani A.N. Mardhiyyah C.A. Alfarafisa N.M. Parental Knowledge, Attitude, and Practice on Self-Medication of Antibiotics for Children in Bandung, Indonesia: A Questionnaire-Based Survey and Module-Based Learning Intervention BMC Pediatr.20252568710.1186/s 12887-025-06084-840993564 PMC 12462208 · doi ↗ · pubmed ↗
- 8Hersh A.L. Shapiro D.J. Pavia A.T. Shah S.S. Antibiotic Prescribing in Ambulatory Pediatrics in the United States Pediatrics 20111281053106110.1542/peds.2011-133722065263 · doi ↗ · pubmed ↗