Prognostic Factors of 30-Day In-Hospital Mortality in Critically Ill Patients Receiving Continuous Renal Replacement Therapy
Hyeon-Ju LEE, Taehee KIM, Heeyoung LEE, Youngeon LEE, Jinseon HEO, Youn-Jung SON

TL;DR
This study identifies factors that predict 30-day in-hospital mortality in critically ill patients undergoing kidney dialysis treatment called CRRT.
Contribution
The study identifies specific prognostic factors for mortality in CRRT patients, including hepatic failure and changes in consciousness and sodium levels.
Findings
Hepatic failure as a comorbidity significantly increases 30-day mortality risk in CRRT patients.
Higher Sequential Organ Failure Assessment Scores and lower Glasgow Coma Scores are associated with increased mortality.
Elevated sodium levels during CRRT are linked to higher in-hospital mortality.
Abstract
Continuous renal replacement therapy (CRRT) is a form of dialysis that effectively replicates the excretory function of the kidneys in critically ill patients suffering from acute kidney injury. The number of patients receiving CRRT in critical care settings is increasing globally. Although these patients are at greater risk of mortality after commencing CRRT, the comprehensive risk factors for in-hospital mortality in this population remain uncertain. The prognostic factors for 30-day in-hospital mortality in patients receiving CRRT are investigated in this study. This retrospective observational study was performed at a tertiary care university hospital between January 2018 and December 2020. Data from a total of 613 patients requiring CRRT were included. Pre-, intra-, and post-CRRT data were extracted from electronic medical records, and patients were grouped based on 30-day…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
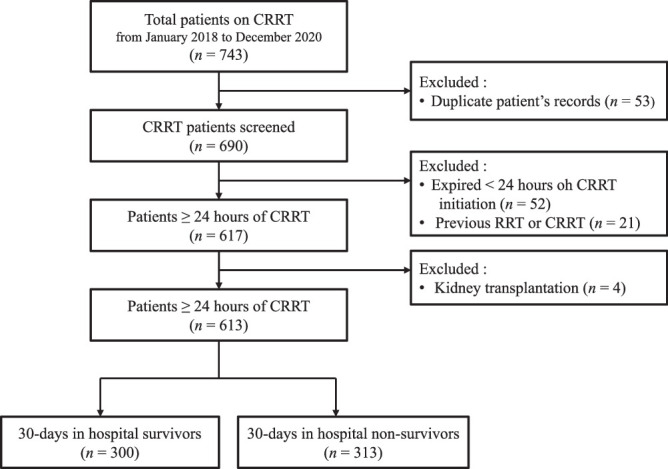 Figure 1
Figure 1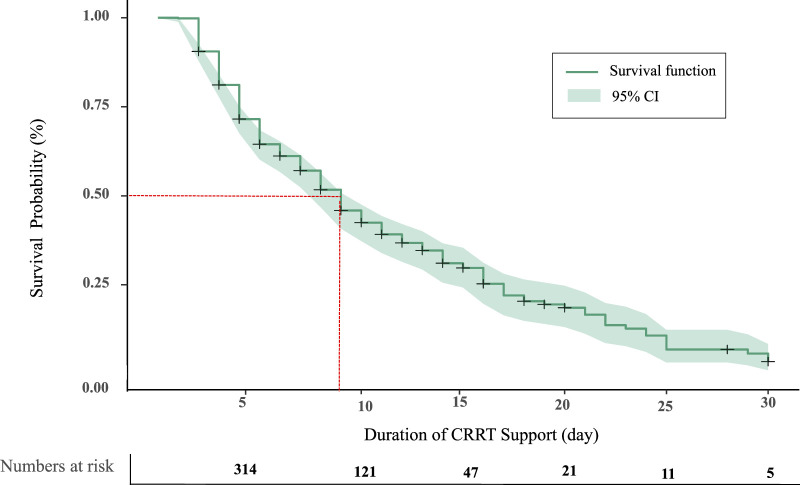 Figure 2
Figure 2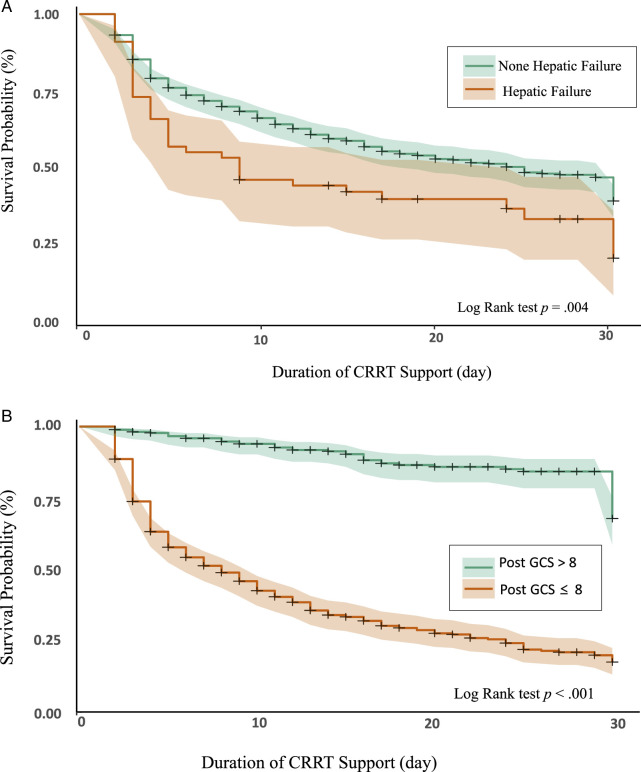 Figure 3
Figure 3| Characteristic | Total ( | Survivors ( | Nonsurvivors ( |
|
|
|---|---|---|---|---|---|
|
|
|
| |||
| Age (years; | 69.35±13.19 | 69.26±13.15 | 69.43±13.25 | −0.16 | .870 |
| Gender, male | 335 (54.6) | 157 (52.3) | 178 (56.9) | 1.27 | .259 |
| Smoking, yes | 115 (18.8) | 58 (19.3) | 57 (18.2) | 0.13 | .722 |
| Alcohol consumption, yes | 135 (22.0) | 70 (23.3) | 65 (20.8) | 0.59 | .443 |
| Body mass index (kg/m2; | 23.31±4.50 | 23.88±4.53 | 22.72±4.40 | 3.00 | .003 |
| Comorbidities a | |||||
| Diabetes mellitus, yes | 269 (43.9) | 162 (54.0) | 107 (34.2) | 24.42 | <.001 |
| Hypertension, yes | 317 (51.7) | 174 (58.0) | 143 (45.7) | 9.30 | .002 |
| Cerebrovascular disease, yes | 147 (24.0) | 72 (24.0) | 75 (24.0) | 0.01 | .991 |
| Heart failure, yes | 94 (15.3) | 46 (15.3) | 48 (15.3) | 0.01 | .999 |
| Respiratory failure, yes | 73 (11.9) | 34 (11.3) | 39 (12.5) | 0.19 | .667 |
| Hepatic failure, yes | 56 (9.1) | 18(6.0) | 32(12.1) | 6.96 | .008 |
| Cancer | 130 (21.2) | 43 (14.3) | 87 (27.8) | 16.61 | <.001 |
| Characteristic | Total ( | Survivors ( | Nonsurvivors ( |
|
|
|---|---|---|---|---|---|
|
|
|
| |||
|
| |||||
| CPR, yes | 64 (10.4) | 24 (8.0) | 40 (12.8) | 3.74 | .053 |
| Mechanical ventilation, yes | 378 (61.7) | 145 (48.3) | 233 (74.4) | 44.17 | <.001 |
| Glasgow Coma Scale | 7.29±5.14 | 8.84±5.34 | 5.80±4.47 | 7.65 | <.001 |
| SOFA score | 9.81±3.26 | 8.76±2.96 | 10.91±3.16 | -9.05 | <.001 |
| Average MAP (mm Hg) | 81.94±15.76 | 84.81±16.97 | 79.20±13.99 | 4.45 | <.001 |
| Oliguria before CRRT, yes | 376 (61.3) | 174 (46.3) | 202 (53.7) | 2.76 | .097 |
| Laboratory data | |||||
| Creatinine (mg/dL) | 3.68±2.74 | 4.39±2.85 | 3.00±2.44 | 6.43 | <.001 |
| Sodium (mg/dL) | 138.78±7.57 | 137.97±6.97 | 139.56±8.03 | −2.61 | .009 |
| Potassium (mg/dL) | 4.63±1.67 | 4.75±1.26 | 4.52±1.06 | 2.48 | .013 |
| Total bilirubin (mg/dL) | 2.10±3.70 | 1.40±2.93 | 2.77±4.20 | −4.72 | <.001 |
| Hemoglobin (g/dL) | 9.85±2.23 | 9.87±2.06 | 9.83±2.38 | 0.22 | .823 |
| Platelets (103/μL) | 158.84±110.52 | 178.80±111.73 | 139.72±106.04 | 4.44 | <.001 |
| Lactic acid (mg/dL) | 5.87±5.27 | 4.28±4.17 | 7.34±5.75 | −5.22 | <.001 |
|
| |||||
| Vascular access | 3.68 | .273 | |||
| Internal jugular vein | 189 (30.8) | 96 (32.0) | 93 (29.7) | ||
| Femoral vein | 404 (65.9) | 198 (66.0) | 206 (65.8) | ||
| Subclavian vein | 2 (0.3) | 1 (0.2) | 1 (0.2) | ||
| Others | 18 (2.9) | 5 (0.8) | 13 (2.1) | ||
| Anticoagulant, yes | 344 (55.8) | 172(57.0) | 172(54.6) | 0.35 | .557 |
| Average prescription dose (mL/kg/h) | 44.46±11.01 | 42.93±9.05 | 45.92±12.45 | −3.42 | .001 |
| Characteristic | Total ( | Survivors ( | Nonsurvivors ( |
|
|
|---|---|---|---|---|---|
| Mean ± | Mean ± | Mean ± | |||
| Mechanical ventilation, yes ( | 384 (62.6) | 121 (4.3) | 263 (84.0) | 124.96 | <.001 |
| Glasgow Coma Scale | 7.75±5.10 | 1.83 ±4.53 | 4.80±3.68 | 18.07 | <.001 |
| SOFA score | 1.88±4.88 | 7.41±3.45 | 14.19±3.56 | −23.93 | <.001 |
| Average MAP (mm Hg) | 76.73±18.57 | 85.88±13.99 | 67.95±18.19 | 13.71 | <.001 |
| Laboratory data | |||||
| Creatinine (mg/dL) | 1.25±0.92 | 1.40±0.94 | 1.10±0.87 | 4.06 | <.001 |
| Sodium (mg/dL) | 138.44±5.61 | 137.08±3.33 | 139.75±6.96 | −6.08 | <.001 |
| Potassium (mg/dL) | 3.95±0.79 | 3.40±0.43 | 4.19±0.96 | −8.18 | <.001 |
| Total bilirubin (mg/dL) | 3.77±5.69 | 2.15±4.33 | 5.32±6.28 | −7.26 | <.001 |
| Hemoglobin (g/dL) | 9.13±1.52 | 9.11±1.25 | 9.15±1.75 | −0.32 | .751 |
| Platelets (103/μL) | 101.33±76.53 | 132.29±81.15 | 71.67±58.08 | 1.60 | <.001 |
| Lactic acid (mg/dL) | 7.87±8.06 | 3.02±5.24 | 12.18±7.68 | −13.91 | <.001 |
| Duration of CRRT support (days) | 6.47±5.18 | 6.28±4.62 | 6.65±5.67 | −0.90 | .369 |
| Predictor | Unadjusted HR (95% CI) |
| Adjusted HR (95% CI) |
|
|---|---|---|---|---|
| General characteristics | ||||
| Body mass index (kg/m2) | 0.96 [0.93, 0.99] | .006 | 0.98 [0.92, 10.4] | .500 |
| Diabetes mellitus, yes | 0.58 [0.46, 0.73] | <.001 | 0.78 [0.47, 1.29] | .331 |
| Hypertension, yes | 0.78 [0.62, 0.97] | .026 | 0.97 [0.58, 1.63] | .927 |
| Hepatic failure, yes | 1.60 [1.14, 2.25] | .006 | 2.75 [1.15, 6.58] | .023 |
| Cancer, yes | 1.73 [0.35, 2.22] | <.001 | 1.06 [0.61, 1.82] | .847 |
| Pre-CRRT characteristics | ||||
| Mechanical ventilation, yes | 2.22 [1.72, 2.86] | <.001 | 1.69 [0.44, 6.46] | .443 |
| Glasgow Coma Scale | 0.92 [0.90, 0.94] | <.001 | 1.02 [0.90, 1.15] | .817 |
| SOFA score | 1.17 [1.13, 1.22] | <.001 | 0.91 [0.79, 1.04] | .174 |
| Average mean arterial pressure (mm Hg) | 0.96 [0.98, 0.99] | <.001 | 0.99 [0.97, 1.01] | .541 |
| Creatinine (mg/dL) | 0.85 [0.80, 0.90] | <.001 | 0.98 [0.84, 1.15] | .865 |
| Sodium (mg/dL) | 1.02 [1.01, 1.04] | .009 | 1.01 [0.98, 1.05] | .474 |
| Potassium (mg/dL) | 0.95 [0.86, 10.05] | .318 | 0.91 [0.71, 1.17] | .447 |
| Total bilirubin (mg/dL) | 1.04 [1.02, 1.06] | <.001 | 1.10 [1.00, 1.21] | .050 |
| Platelets (103/μL) | 0.99 [0.98, 0.99] | <.001 | 1.00 [1.00, 1.01] | .834 |
| Lactic acid (mg/dL) | 1.07 [1.04, 1.98] | <.001 | 0.10 [0.94, 1.06] | .919 |
| Intra-CRRT characteristics | ||||
| Average prescription dose (mL/kg/h) | 1.02 [1.01, 1.03] | <.001 | 0.10 [0.98, 1.01] | .609 |
| Post-CRRT characteristics | ||||
| Mechanical ventilation, yes | 4.69 [3.46, 6.36] | <.001 | 0.48 [0.16, 1.49] | .205 |
| Glasgow Coma Scale | 0.80 [0.78, 0.83] | <.001 | 0.82 [0.72, 0.94] | .004 |
| SOFA score | 1.27 [1.23, 1.30] | <.001 | 1.16 [1.02, 1.32] | .026 |
| Average mean arterial pressure (mm Hg) | 0.96 [0.96, 0.97] | <.001 | 0.99 [0.98, 1.01] | .317 |
| Creatinine (mg/dL) | 0.83 [0.71, 0.97] | .016 | 1.03 [0.85, 1.26] | .758 |
| Sodium (mg/dL) | 1.07 [1.05, 1.09] | <.001 | 1.05 [1.01, 1.10] | .026 |
| Potassium (mg/dL) | 1.78 [1.58, 2.01] | <.001 | 1.13 [0.88, 1.46] | .346 |
| Total bilirubin (mg/dL) | 1.04 [1.02, 1.05] | <.001 | 0.95 [0.90, 1.00] | .050 |
| Platelets (103/μL) | 0.99 [0.98, 0.99] | <.001 | 1.00 [0.99, 1.01] | .727 |
| Lactic acid (mg/dL) | 1.09 [1.08, 1.11] | <.001 | 1.02 [0.98, 1.06] | .430 |
- —the National Research Foundation of Korea (NRF) grant
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSepsis Diagnosis and Treatment · Acute Kidney Injury Research · Heart Failure Treatment and Management
Introduction
Continuous renal replacement therapy (CRRT) is a special type of dialysis given to unstable patients in the intensive care unit (ICU) whose bodies cannot tolerate regular hemodialysis (Bourbonnais et al., 2020). This modality is attractive because net fluid removal can be extended over 24 hours instead of the usual 4 hours for hemodialysis, thereby reducing the risk of hypotension (Tandukar & Palevsky, 2019). CRRT is the preferred option in critically ill patients who suffer from acute kidney injury (AKI), with or without baseline chronic renal impairment (Ahmed et al., 2019). CRRT is also utilized in cases of multiorgan failure and sepsis (Tandukar & Palevsky, 2019).
CRRT is performed to provide kidney supportive care in ~10%–40% of critically ill patients (Ahmed et al., 2019; Tiglis et al., 2022). Despite the efforts to treat patients in need of CRRT, mortality rates among this population remain high (Tiglis et al., 2022). According to a recent review (H.-J. Lee & Son, 2020), in-hospital mortality rates vary between 38.6% and 62.4% for patients receiving CRRT, while the rate for patients with AKI requiring CRRT in the ICU ranges from 50% to 75% (Rewa et al., 2023). High mortality rates after CRRT may increase length of hospital stays, medical service durations, and health care costs (Järvisalo et al., 2022). The findings of a systematic review highlighted that investigating the 30-day in-hospital mortality may be beneficial in providing timely renal care after commencing CRRT (Xia et al., 2021). However, few studies have been published regarding the risk factors of 30-day in-hospital mortality in patients on CRRT in ICU settings (Priyamvada et al., 2018). Thus, determining the factors contributing to mortality risk in patients undergoing CRRT is vital to reducing avoidable deaths and developing transitional care plans from the ICU to home.
Based on the literature, older age, a high number of comorbidities, and low body mass index (BMI) have been linked to higher mortality risk in patients on CRRT (H.-J.Lee & Son, 2020; Rewa et al., 2023). In addition, unstable hemodynamic factors such as lower systolic and diastolic blood pressure values, extracorporeal membrane oxygenation use, and higher severity of illness scores have all been associated with a greater risk of in-hospital mortality in patients on CRRT (Jeon et al., 2021; Jiang et al., 2022; Peters et al., 2023). However, conflicting and inconsistent results have been reported. Moreover, existing evidence on the risk factors for mortality has focused primarily on a single time period, for example, pre- or post-CRRT (Jeon et al., 2021; Zhou et al., 2023). Thus, critical care teams should consider integrative risk assessment approaches to ensure patient safety during CRRT (Uusalo et al., 2021). ICU nurses are frontline health care professionals responsible for regularly monitoring and managing patients undergoing CRRT (Bourbonnais et al., 2020). In a prior study, nurses were shown to have played a key role in decreasing in-hospital mortality by 14% (Bourbonnais et al., 2020). In this respect, ICU nurses should keep in mind the significance of identifying risk factors related to in-hospital mortality among their patients on CRRT.
Recently, CRRT utilization has increased in many countries, including Korea, based on its benefits in the treatment of AKI and other critical illnesses (Zhou et al., 2023). However, clear evidence regarding the factors associated with the increased risk of mortality in patients on CRRT is not available (S. Park et al., 2018). Furthermore, a recent meta-analysis reported differences in CRRT outcomes due to heterogeneity among the regions in which the studies were conducted (Chander et al., 2024). Therefore, the objective of this study was to investigate the prevalence and prognostic factors of 30-day in-hospital mortality among Korean patients on CRRT. The findings are expected to contribute to the global response by providing evidence related to short-term mortality in CRRT patients.
Methods
Study Design and Settings
Data for this retrospective observational study were obtained from the electronic medical records of all patients admitted to the medical and surgical ICU of a single tertiary care university hospital with 842 beds in South Korea from January 2018 to December 2020.
Samples
Hospital electronic medical records from January 2018 to December 2020 were analyzed, and 743 ICU patients aged ≥18 years on continuous venovenous hemodiafiltration were screened. Continuous venovenous hemodiafiltration provides both diffusive and convective solute clearance (Peters et al., 2023). After excluding 53 duplicate records, 690 medical records were included in the initial sample. Records of patients with any of the following criteria were excluded: (1) died within the first 24 hours of CRRT (n = 52), (2) previous recipient of RRT or CRRT (n = 21), and (3) recipient of kidney transplantation (n = 4). The final sample included the medical records of 613 patients (Figure 1).
Flow Diagram of the Study Note. CRRT = continuous renal replacement therapy.
A sample size calculation using G*power 3.1 was conducted (Faul et al., 2009). Based on previous studies (H.-J. Lee & Son, 2020; Yang et al., 2016), a minimum sample size of 620 is required to identify a predictor variable with an OR of 1.3 in a population with 80% power and a two-sided α level of .05. Thus, the 613-patient sample in this study was somewhat insufficient.
Measures
Patient general characteristics at baseline
Data on patient age, gender, smoking status, alcohol consumption, and BMI (kg/m^2^) were collected. Comorbidities were categorized into the following categories: diabetes mellitus, hypertension, cerebrovascular disease, heart failure, respiratory failure, hepatic failure, and cancer.
Pre-CRRT patient characteristics
Pre-CRRT characteristics data were collected before CRRT initiation based on a literature review (Peters et al., 2023; Tiglis et al., 2022). Cardiopulmonary resuscitation (CPR), mechanical ventilation use, and the Glasgow Coma Scale (GCS) were used to evaluate the patient’s level of consciousness (Bodien et al., 2021). Sequential Organ Failure Assessment (SOFA) score, mean arterial pressure (MAP), and presence of oliguria information, as well as laboratory data such as creatinine, sodium, potassium, total bilirubin, hemoglobin, platelets, and lactic acid levels, were collected. The SOFA score is widely used for the prognostication and assessment of multiple organ dysfunctions in critically ill patients (Bahtouee et al., 2019). This score is the sum of 6 organ dysfunctions (respiratory, cardiovascular, hepatic, coagulation, renal, and neurological systems). The SOFA score was calculated at hospital admission and every 24 hours until ICU discharge or death for every included patient. SOFA total scores range from 0 (normal organ function) to 4 (worst organ function), with higher scores reflecting higher organ failure progression. The mean SOFA was calculated as the average of daily SOFA scores for each patient over their ICU stay.
In this study, the average MAP value was calculated using the MAP values taken 24 hours before CRRT initiation.
Intra-CRRT patient characteristics
The intra-CRRT characteristics included data related to the application of CRRT. Data included the site of vascular access, use of anticoagulants, and average prescribed dose (mL/kg/h). The average prescribed dose for each patient was derived from the prescribed dose based on the duration of CRRT (H.-J. Lee & Son, 2020; K.Y. Lee et al., 2022).
Post-CRRT patient characteristics
Post-CRRT characteristics included data from the day of CRRT device implantation to in-hospital survival within 30 days. Based on a literature review (Ahmed et al., 2019; Chander et al., 2024; Järvisalo, et al., 2022), data considered included use of mechanical ventilation, GCS and SOFA scores, average MAP, duration of CRRT (in days), and laboratory data such as creatinine (mg/dL), sodium (mg/dL), potassium (mg/dL), total bilirubin (mg/dL), hemoglobin (g/dL), platelets (10^3^/μL), and lactic acid (mg/dL) levels. In patients who were sedated, the GCS score was evaluated by the ICU nurse during the sedation break. Average MAP values for the survivor and nonsurvivor groups were calculated as the average value from CRRT initiation until, respectively, just before stopping CRRT and just before death.
30-day in-hospital mortality
The 30-day in-hospital mortality was used as the primary outcome. Death was defined as all-cause in-hospital death during hospitalization within 30 days of CRRT initiation.
Ethical Considerations and Data Collection
Institutional review board approval was obtained from Chung-Ang University (IRB No. 2020-12-046-002) before commencing this study. The patient records were collected retrospectively and closely reviewed by the researchers. Medical record reviews included hospital and ICU admissions, CRRT notes, nursing records from ICUs and general wards, medication administration records, laboratory data, and discharge records. Patient identification numbers were deleted for anonymization purposes during data collection.
Data Analysis
All data analysis was conducted on SPSS version 27.0 (IBM Corp., Armonk, NY, USA). Continuous variables were summarized as mean with SD; categorical variables were reported as frequencies with percentages; and independent t tests, χ^2^ tests, or Fisher’s exact tests were used to confirm differences in baseline patient characteristics and pre-, intra-, and post-CRRT data between nonsurvivors and survivors.
The 30-day in-hospital survival probability was analyzed using Kaplan–Meier methods. Log-rank tests were utilized to compare 30-day in-hospital survival probability between groups, and univariate and multivariable Cox proportional hazards models were used to confirm predictors of 30-day in-hospital mortality in adult patients on CRRT. To determine predictors of 30-day in-hospital mortality, statistically significant variables in the univariable analysis (p < .05) were maintained in the multivariable Cox proportional hazard regression model.
Results
In-Hospital Mortality and Between-Group Comparison of Baseline Patient Characteristics
The 30-day in-hospital mortality rate in the entire sample was 52.1% (n = 313). As shown in Table 1, the mean age of the sample was 69.35±13.19 years and the proportion of male patients was 54.6% (n = 335). Significant differences between the survivor and nonsurvivor groups were found in terms of BMI (t = 3.00, p = .003), comorbid diabetes mellitus (χ^2^ = 24.42, p < .001), hypertension (χ^2^ = 9.30, p = .002), hepatic failure (χ^2^ = 6.96, p = .008), and cancer (χ^2^ = 16.61, p < .001). No significant between-group differences were found for other baseline characteristics.
Between-Group Differences in Pre-CRRT Variables
As shown in Table 2, significant between-group differences were found in use of mechanical ventilation (χ^2^ = 44.17, p < .001), GCS score (t = 7.65, p < .001), SOFA score (t = −9.05, p < .001), average MAP (t = 4.45, p < .001), creatinine level (t = 6.43, p < .001), sodium level (t = −2.61, p = .009), potassium level (t = 2.48, p =0.013), total bilirubin level (t = −4.72, p < .001), platelet level (t = 4.44, p < .001), and lactic acid level (t = −5.22, p < .001) before CRRT initiation. No significant between-group differences were found for other pre-CRRT characteristics.
Between-Group Differences in Intra-CRRT Variables
As shown in Table 2, the average prescription CRRT dose (t = −3.42, p = .001) was the only factor to reveal a statistically significant difference between survivors and nonsurvivors during the intra-CRRT period.
Between-Group Differences in Post-CRRT Variables
As shown in Table 3, significant between-group differences were found in use of mechanical ventilation (χ^2^ = 124.96, p < .001), GCS (t = 18.07, p < .001), SOFA score (t = −23.93, p < .001), average MAP (t = 13.71, p < .001), creatinine level (t = 4.06, p < .001), sodium level (t = −6.08, p < .001), potassium level (t = −8.18, p < .001), total bilirubin level (t = −7.26, p < .001), platelet level (t = 10.60, p < .001), and lactic acid level (t = −13.91, p < .001) after CRRT implementation. No significant between-group differences were found for other post-CRRT characteristics.
Predictors of 30-Day In-Hospital Mortality
As shown in Figure 2, the results of the Kaplan–Meier analysis showed the 50th percentile of patients survived for 9 days after initiating CRRT, and that 30-day in-hospital mortality was significantly related to comorbid hepatic failure (p = .004) and post-CRRT GCS score (p < .001; Figure 3).
Overall Survival Probability ( %) of Patients on Continuous Renal Replacement Therapy Note. CI = confidence interval; CRRT = continuous renal replacement therapy.
(A) Probability of Survival With and Without Comorbid Hepatic Failure. (B) Probability of Survival Based on Post-CRRT GCS Score Range Note. CRRT = continuous renal replacement therapy; GCS = Glasgow coma scale.
Notably, after controlling for confounding variables with p values < .05 in the univariate analysis, the multivariate Cox proportional hazards model revealed comorbid hepatic failure (adjusted HR = 2.75, 95% CI [1.15, 6.58], p = .023), post-CRRT GCS score (adjusted HR = 0.82, 95% CI [0.72, 0.94], p = .004), post-CRRT SOFA score (adjusted HR = 1.16, 95% CI [1.02,1.32], p = .026), and post-CRRT sodium level (adjusted HR = 1.05, 95% CI [1.01, 1.10], p = .026) to relate significantly to a high risk of 30-day in-hospital mortality (Table 4).
Discussion
Despite advancements in CRRT technology and its increased application among critically ill patients, in-hospital mortality rates among these patients remain high (Järvisalo et al., 2022). In this study, 30-day in-hospital mortality was shown to be high among ICU patients on CRRT (51.1%), which is consistent with studies reporting 30-day mortality rates of 66.2% (K. Y. Lee et al., 2022) and 51.0% (Peters et al., 2023), respectively. However, other prior research has shown significantly lower mortality rates (16.0%–33.3%; Kee et al., 2018; Prasad et al., 2016). The disparity between our findings and those of prior studies may relate to differences in the timing of the primary outcome measurement. In this study, the focus was on 30-day in-hospital mortality, as this time period is considered to offer an effective indicator of acute health care service quality (Xia et al., 2021). In particular, the findings of this study indicate mortality rates increase 9 days after CRRT unit initiation. Accordingly, ICU nurses should recognize the importance of early preventable risk factor screenings to reducing in-hospital mortality among patients on CRRT.
The main findings of this study show that comorbid hepatic failure and post-CRRT characteristics, such as poor GCS and SOFA scores and higher sodium levels, significantly increase 30-day in-hospital mortality risk in patients on CRRT. In this study, hepatic failure was identified as the strongest prognostic factor for 30-day in-hospital mortality. A previous study conducted in the United States found 70% of patients with acute hepatic failure had AKI and 30% required RRT (Tujios et al., 2015). In another study conducted in Europe, the reported incidence of AKI in patients with hepatic failure was 63.4% (Hadem et al., 2019). Liver cell death in hepatic failure can lead to renal tubular cell apoptosis in the kidneys (Sharma et al., 2024). In addition, Nishino et al. (2024) reported bilirubin levels, as an indicator of hepatic function, to be an independent prognostic factor for mortality among AKI patients with CRRT. Similarly, the univariate Cox regression model in this study found total bilirubin level to be higher in nonsurvivors than in survivors. Consequently, it is important to monitor changes in renal and liver functions continuously in patients with either hepatic failure or AKI, with more studies needed to identify causal relationships between the two conditions.
Second, better GCS scores during CRRT were linked to a decreased risk of 30-day in-hospital mortality. The GCS is often used to assess the level of consciousness in critically ill patients (Reith et al., 2016), and GCS scores of ≤8 are typically used to determine severe brain injury (Fitzgerald et al., 2022). In this study, the average GCS score was ~10 in the survivor group and 4 in the nonsurvivor group, which is in line with the between-group findings of previous studies (Ahmadi et al., 2023; Fitzgerald et al., 2022). Lower GCS scores may be considered an adverse outcome indicator of CRRT use, as rapid fluctuations in blood urea concentration caused by RRT may lead to changes in osmotic pressure, potentially leading to adverse outcomes such as cerebral edema and elevated intracranial pressure (Mistry, 2019).
According to a recent systematic review, patients with acute brain injury undergoing RRT due to AKI are more likely to experience neurological complications (Husain-Syed et al., 2023). That finding points to a need to promptly identify the causes of AKI and administer CRRT in a timely manner. However, that study relied on retrospective data only. Thus, large prospective studies are needed to determine the bidirectional relationship between GCS scores and the positive outcomes of CRRT in ICU patients. Moreover, studies designed to determine optimal GCS score cutoff points are needed to predict the likelihood of in-hospital mortality among ICU patients on CRRT.
Third, having a higher SOFA score during CRRT support was shown to be linked to a greater risk of 30-day in-hospital mortality in patients on CRRT. This finding supports previous findings that the SOFA score is significantly associated with mortality risk in critically ill patients with AKI on CRRT (Chang et al., 2014; Wang et al., 2020) but contradicts Schaffer et al. (2022), who reported that higher SOFA scores were not a risk factor for in-hospital mortality in patients on CRRT. Several studies have also reported that the Acute Physiology and Chronic Health Evaluation (APACHE) II and SOFA are reliable tools for predicting in-hospital mortality in ICU patients on CRRT (Gong et al., 2019; H. Park et al., 2023). Thus, further studies are required to identify which severity scoring systems are useful tools for assessing mortality risk in patients on CRRT and to develop kidney-specific severity scoring systems. Furthermore, multicenter, larger cohort studies are required to determine the optimal cutoff SOFA score for predicting high-risk patients on CRRT.
Finally, sodium levels during CRRT were identified in this study as a significant predictor of 30-day in-hospital mortality. The mean sodium levels in the nonsurvivor group were significantly higher than those in the survivor group during CRRT, even though the the level in both groups was maintained within the normal range of 135– 145 mEq/L. This finding is partly supported by a previous study, which related larger changes in serum sodium levels during CRRT to increased 90-day mortality risk among critically ill patients on CRRT (Petnak et al., 2022). However, in another previous study, sodium levels at the start of CRRT were identified as a significant predictor of mortality (Han et al., 2016). In this study, mean pre- and post-CRRT sodium levels in the nonsurvivor group were 139.56 and 139.75 mEq, respectively, which were slightly higher than those in the survivor group. Unfortunately, the retrospective nature of this study prohibited reporting on the serum trajectories during CRRT. In several prior studies, patients with dysnatremia, including hyponatremia and hypernatremia, and sodium trajectories have been identified as at a higher risk of mortality than those in stable condition (Huang et al., 2024; Yessayan et al., 2021). Based on the above, many studies will be needed to examine the impact of dysnatremia and changes in sodium levels on CRRT outcomes.
In this multivariable Cox regression analysis, no association was found between BMI and elevated risk of 30-day in-hospital mortality in either group. This finding is inconsistent with previous research (H.-J. Lee & Son, 2020; Peters et al., 2023). This study included only a single BMI reading at baseline and did not account for changes in BMI over time. Thus, future studies on this issue should consider the body composition trajectory.
Based on the findings, comprehensive risk assessments should be conducted during CRRT. These findings may help health care providers develop strategies to reduce the risk of 30-day in-hospital mortality in critically ill patients on CRRT. Critical care nurses should be aware of the importance of identifying comorbid hepatic failure, early detection of deterioration in mental status and disease severity, and close monitoring of sodium levels during CRRT support to prevent avoidable adverse events in patients on CRRT.
Limitations
This study was affected by a number of limitations. The relatively small sample size advises careful consideration when generalizing the findings to other populations. Multicenter, prospective cohort studies will be required to confirm our findings. Second, only patients on CRRT for more than 24 hours were included, which may lead to selection bias. Third, patients’ medical records may be missing in the process of collecting medical records, which may result in information bias. Also, indications for CRRT initiation were not included in this study. Finally, nutritional status, such as tube feeding, was not reflected in the analysis, making it impossible to demonstrate a relationship between nutritional support and mortality.
Conclusions
Over half of the ICU patients undergoing CRRT experienced significantly higher 30-day in-hospital mortality. Based on the findings, ICU nurses should be more concerned about the impact of comorbid hepatic failure on adverse outcomes in patients requiring CRRT. In addition, the primary results emphasize the importance of closely observing patients’ consciousness level, illness severity score, and serum sodium levels after initiating CRRT. Significantly, early detection and management of these risk factors should be performed within 9 days of CRRT initiation. However, the pre- and intra-CRRT characteristics were not found to relate significantly to the risk of 30-day in-hospital mortality. Therefore, more studies are needed to investigate the comprehensive risk factors of in-hospital mortality among patients on CRRT using multicenter, larger cohort samples.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ahmadi S. Sarveazad A. Babahajian A. Ahmadzadeh K. Yousefifard M. 2023. Comparison of Glasgow Coma Scale and Full Outline of Un Responsiveness score for prediction of in-hospital mortality in traumatic brain injury patients: A systematic review and meta-analysis. European Journal of Trauma and Emergency Surgery, 49(4), 1693–1706. 10.1007/s 00068-022-02111-w 36152069 · doi ↗ · pubmed ↗
- 2Ahmed A. R. Obilana A. Lappin D. 2019. Renal replacement therapy in the critical care setting. Critical Care Research and Practice, 2019, Article ID 6948710. 10.1155/2019/6948710 PMC 666449431396416 · doi ↗ · pubmed ↗
- 3Bahtouee M. Eghbali S. S. Maleki N. Rastgou V. Motamed N. 2019. Acute physiology and chronic health evaluation II score for the assessment of mortality prediction in the intensive care unit: A single-centre study from Iran. Nursing in Critical Care, 24, 375–380. 10.1111/nicc.12401 30924584 · doi ↗ · pubmed ↗
- 4Bodien Y. G. Barra A. Temkin N. R. Barber J. Foreman B. Vassar M. Robertson C. Taylor S. R. Markowitz A. J. Manley G. T. Giacino J. T. Edlow B. L. TRACK-TBI Investigators . 2021. Diagnosing level of consciousness: The limits of the Glasgow Coma Scale total score. Journal of Neurotrauma, 38(23), 3295–3305. 10.1089/neu.2021.0199 34605668 PMC 8917895 · doi ↗ · pubmed ↗
- 5Bourbonnais F. F. Slivar S. Malone-Tucker S. 2020. Caring for patients on CRRT—Key safety concerns identified by nurses. The Canadian Journal of Critical Care Nursing, 31(2), 13–19.
- 6Chander S. Luhana S. Sadarat F. Parkash O. Rahaman Z. Wang H. Y. Kiran F. Lohana A. C. Sapna F. Kumari R. 2024. Mortality and mode of dialysis: Meta-analysis and systematic review. BMC Nephrology, 25, Article No. 1. 10.1186/s 12882-023-03435-4 PMC 1076309738172835 · doi ↗ · pubmed ↗
- 7Chang C.-H. Fan P.-C. Chang M.-Y. Tian Y.-C. Hung C.-C. Fang J.-T. Yang C.-W. Chen Y.-C. 2014. Acute kidney injury enhances outcome prediction ability of sequential organ failure assessment score in critically ill patients. PLOS ONE, 9(10), Article e 109649. 10.1371/journal.pone.0109649 25279844 PMC 4184902 · doi ↗ · pubmed ↗
- 8Faul F. Erdfelder E. Buchner A. Lang A. G. 2009. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods, 41(4), 1149–1160. 10.3758/BRM.41.4.1149 19897823 · doi ↗ · pubmed ↗