Intraosseous Non‐Hodgkin Lymphoma Mimicking a Periapical Lesion
Laryssa Thainá Mello Queiroz Cunha, Joab Cabral Ramos, Isabel Schausltz Pereira Faustino, Silvia Maria Paparotto Lopes, Alan Roger Santos‐Silva, Pablo Agustin Vargas, Márcio Ajudarte Lopes

TL;DR
A rare case of lymphoma in the jaw was mistaken for a dental lesion, highlighting the need for thorough diagnosis in persistent cases.
Contribution
This case report adds to the limited literature on primary intraosseous non-Hodgkin lymphoma in the jaws.
Findings
DLBCL was confirmed in a patient with a persistent periapical lesion unresponsive to dental treatments.
Chemotherapy led to complete remission and bone regeneration as shown by imaging.
The case emphasizes the importance of considering malignancies in differential diagnoses of persistent oral lesions.
Abstract
Periapical radiolucent lesions are commonly of endodontic origin; however, some persistent cases may indicate non‐endodontic pathologies, including malignancies. Diffuse large B‐cell lymphoma (DLBCL) is the most prevalent subtype of lymphoma affecting the oral and maxillofacial region, yet its primary occurrence in the jaws is rare. This case report highlights the diagnostic challenges in differentiating endodontic lesions from periapical lymphomas and includes a literature review of documented cases. A 44‐year‐old male presented with a persistent periapical lesion in the anterior maxilla, unresponsive to endodontic and periodontal treatments. Clinical examination revealed facial asymmetry, gingival edema, palatal swelling, and dental mobility. Imaging showed an ill‐defined hypodense lesion extending beyond the periapical region. Fine needle aspiration and incisional biopsy confirmed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
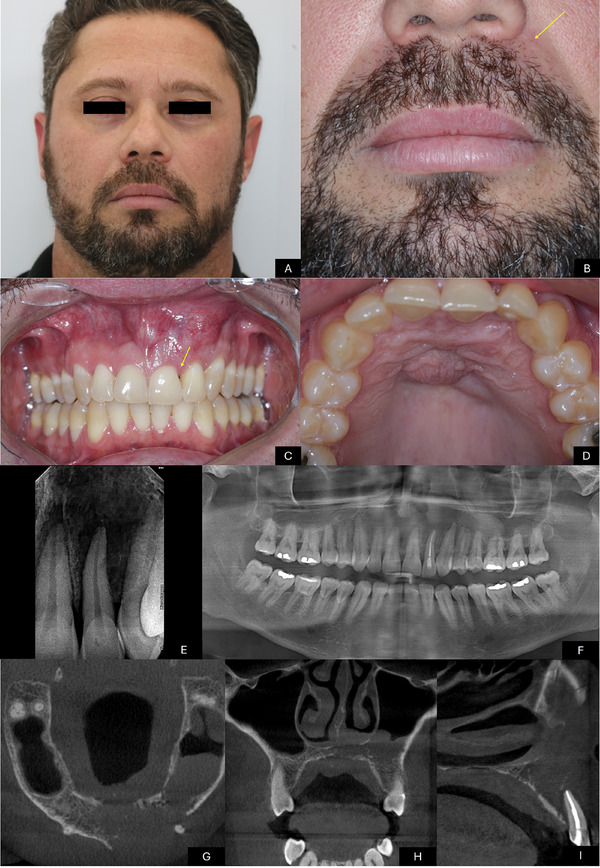 FIGURE 1
FIGURE 1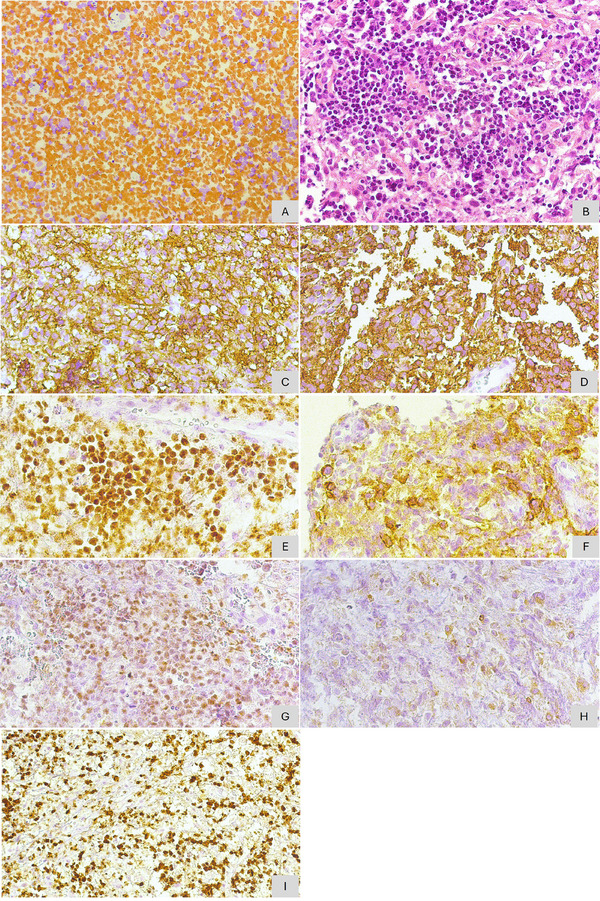 FIGURE 2
FIGURE 2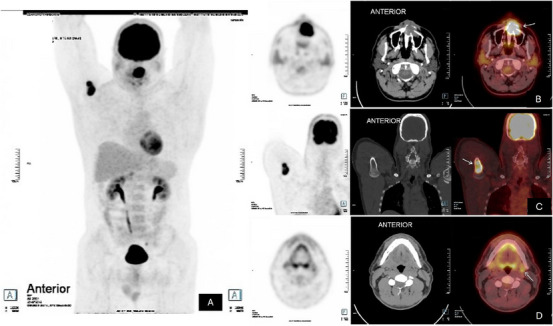 FIGURE 3
FIGURE 3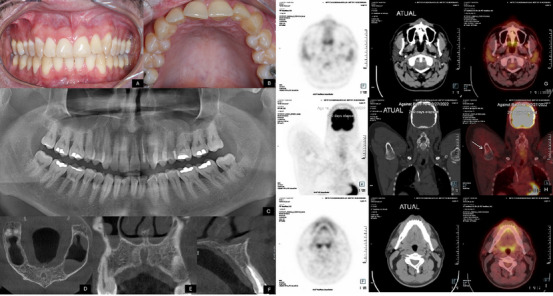 FIGURE 4
FIGURE 4| Antibody | Result |
|---|---|
| LCA | Positive |
| CD20 | Positive |
| CD3 | Negative |
| CD10 | Positive |
| BCl‐6 | Positive (>30%) |
| BCl‐2 | Positive (<30%) |
| MUM‐1 | Negative |
| PAX‐5 | Positive |
| Antígeno Ki67 | Alto (80%) |
| Author | Age | Gender | Location | Diagnosis | Endodontic treatment | Time to diagnosis |
|---|---|---|---|---|---|---|
| Eisenbud et al., [ | 49 | Female | Mandible | DLBCL | Yes | Several months |
| Eisenbud et al., 1984 [ | 44 | Male | Mandible | DLBCL | Yes | NA |
| Eisenbud et al., 1984 [ | 29 | Male | Mandible | Lymphocytic/small cell cleaved lymphoma | No | 2 months |
| Eisenbud et al., 1984 [ | 44 | Female | Maxilla | DLBCL | No | NA |
| Eisenbud et al., 1984 [ | 42 | Male | Maxilla | Histiocytic/Immunoblastic lymphoma | Yes | NA |
| Keyes et al., 1988 [ | 24 | Male | Maxilla | Histiocytic lymphoma | Yes | 3 months |
| Keyes et al., 1988 [ | NA | Male | Mandible | Lymphoma | Yes | 2 years |
| Wen et al., 1988 [ | 37 | Male | Mandible | DLBCL | No | 2 months |
| Spatafore et al., 1989 [ | 46 | Male | Mandible | Lymphoma | No | 1 year |
| Wannfors and Hammarström, 1990 [ | 45 | Female | Mandible | Histiocytic lymphoma | Yes | NA |
| Gusenbauer et al., 1990 [ | 53 | Male | Mandible | DLBCL | No | Several months |
| Wright and Radman1, 1995 [ | 27 | Male | Mandible | DLBCL | Yes | 3 months |
| Mopsik and Milosbky, 1995 [ | 54 | Male | Maxilla | Diffuse lymphoblastic lymphoma | Yes | 1 year |
| Mopsik and Milosbky, 1995 [ | 59 | Male | Mandible | DLBCL | Yes | 4 months |
| Ardekian et al., 1999 [ | 16 | Male | Mandible | Burkitt lymphoma | Yes | 2 weeks |
| Kawasaki et al., 1997 [ | 60 | Female | Mandible | NHL T | Yes | 3 weeks |
| Liu et al., 2000 [ | 14 | Male | Maxilla | Burkitt Lymphoma | No | 3 weeks |
| Cheng and Wright, 2003 [ | 65 | Female | Mandible | DLBCL | No | NA |
| Kozakiewicz et al., 2003 [ | 54 | NA | Maxilla | B‐cell lymphoma | No | NA |
| Brooks et al., 2005 [ | 29 | Female | Maxilla | High grade B‐cell lymphoma | No | 1 week |
| Kini et al., 2009 [ | 55 | Male | Mandible | B‐cell lymphoma | No | 6 months |
| Balasubramaniam et al., 2009 [ | 36 | Female | Mandible | Burkitt Lymphoma | No | 4 weeks |
| Yamada et al., 2010 [ | 44 | Male | Maxilla | Adult T‐cell leukemia/lymphoma | No | 1 month |
| Saund et al., 2010 [ | 38 | Female | Maxilla | Lymphoma | Yes | 9 months |
| Agrawal et al., 2011 [ | 30 | Female | Mandible | DLBCL | No | 2 weeks |
| Hopp et al., 2012 [ | 39 | Male | Mandible | DLBCL | Yes | 2 years |
| Fischer et al., 2012 [ | 34 | Male | Maxilla | DLBCL | Yes | 3 weeks |
| Jessri et al., 2013 [ | 32 | Male | Mandible | DLBCL | Yes | 3 months |
| Wong et al., 2013 [ | 50 | Male | Maxilla | DLBCL | Yes | 6 months |
| Wong et al., 2013 [ | 31 | Female | Maxilla | DLBCL | Yes | 2 months |
| Mendonca et al., 2013 [ | 38 | Female | Mandible | DLBCL | Yes | Several months |
| Carbone et al., 2014 [ | 71 | Female | Mandible | DLBCL | No | NA |
| Pereira et al., 2015 [ | 48 | Male | Mandible | DLBCL | Yes | 5 months |
| Alshahrani et al., 2015 [ | 18 | Male | Mandible | DLBCL | No | 6 months |
| Bugshan et al., 2015 [ | 54 | Male | Mandible | High grade B‐cell lymphoma | Yes | NA |
| Buchanan et al., 2015 [ | 35 | Male | Maxilla | DLBCL | No | 2 months |
| Tetik et al., 2016 [ | 43 | Male | Mandible | DLBCL | No | 1 month |
| Kumar et al., 2016 [ | 41 | Female | Maxilla | DLBCL | Yes | 4 months |
| Syed et al., 2016 [ | 81 | Male | Maxilla | DLBCL | No | 1 month |
| Vasudevan et al., 2016 [ | 19 | Female | Mandible | Plasmablastic lymphoma | No | 3 months |
| Srikant et al., 2016 [ | 64 | Male | Mandible | Spindle‐cell variant of NHL | No | 6 months |
| MacDonald et al., 2017 [ | 59 | Female | Maxilla | B‐cell lymphoma | Yes | NA |
| Dolan et al., 2017 [ | 68 | Male | Maxilla/ Mandible | Marginal zone lymphoma / Lymphoplasmacytic lymphoma | No/Yes | 4 months |
| Hassona et al., 2017 [ | 75 | Male | Mandible | DLBCL | Yes | 2 weeks |
| Varun et al., 2017 [ | 65 | Male | Mandible | B‐cell lymphoma | No | NA |
| Fuessinger et al., 2018 [ | 40 | Female | Mandible | High grade B‐cell lymphoma | No | 1 month |
| Zou et al., 2018 [ | 67 | Female | Maxilla | DLBCL | No | 6 months |
| Cabras et al., 2018 [ | 15 | Female | Maxilla | Burkitt Lymphoma | Yes | NA |
| Silva et al., 2018 [ | 29 | Female | Mandible | THRLBCL | No | 2 months |
| Lapthanasupkul et al., 2019 [ | 55 | Female | Maxilla | ALCL | No | 1 month |
| Janardhanan et al., 2019 [ | 32 | Female | Maxilla | DLBCL | No | NA |
| Siqueira et al., 2019 [ | 51 | Male | Mandible | DLBCL | No | 4 months |
| Badabaan and Fatahzadeh, 2020 [ | 54 | Male | Mandible | DLBCL | Yes | Few months |
| Karadwal et al., 2020 [ | 50 | Male | Mandible | Diffused B‐cell lymphoma, mixed small and large cell type | No | 1 month |
| Theofilou et al., 2020 [ | 70 | Female | Maxilla | DLBCL | No | 3 years |
| Goutzanis et al., 2020 [ | 20 | Male | Mandible | T‐LBL | No | 2 weeks |
| Shilkofski et al., 2020 [ | 72 | Male | Maxilla | DLBCL | Yes | Few weeks |
| Silveira et al., 2020 [ | 14 | Female | Maxilla | B‐cell Lymphoblastic lymphoma | No | 1 month |
| Coskunses et al., 2020 [ | 82 | Female | Mandible | DLBCL | No | 2 months |
| Nosrat et al., 2020 [ | 40 | Female | Maxilla | DLBCL | Yes | 3 months |
| De Coninck et al., 2020 [ | 7 | Female | Mandible | Burkitt Lymphoma | No | Few months |
| Parker, William D, and Keith [ | 37 | Female | Mandible | Burkitt Lymphoma | No | NA |
| Riaz et al., 2021 [ | 3 | Male | Mandible | Burkitt Lymphoma | No | 20 days |
| Vardas et al., 2022 [ | 84 | Male | Maxilla | DLBCL | No | 15 days |
| Gante et al. 2022 [ | 44 | Male | Mandible | DLBCL | No | 4 months |
| Chait et al., 2023 [ | 7 | Male | Maxilla | Burkitt Lymphoma | No | NA |
| Vyas et al., 2024 [ | 60 | Male | Maxilla | DLBCL | No | 2 months |
| Shil et al., 2024 [ | 10 | Female | Maxilla | T‐LBL | No | 1 month |
| Polard et al., 2024 [ | 47 | Male | Maxilla | High grade B‐cell lymphoma | No | 2 years |
| Rezazadeh et al., 2024 [ | 18 | Female | Maxilla | DLBCL | No | 15 weeks |
| Gatt et al., 2024 [ | 32 | Male | Maxilla | HTLV1+ T‐cell lymphoma | No | 1 month |
| El Gaouzi et al., 2024 [ | 26 | Female | Maxilla/ mandible | Burkitt Lymphoma | No | 1 month |
| Papadopoulou et al., 2024 [ | 11 | Female | Mandible | Burkitt Lymphoma | No | 3 weeks |
| Wongpattaraworakul et al., 2025 [ | 61 | Male | Maxilla | DLBCL | Yes | NA |
| Wongpattaraworakul et al., 2025 [ | 68 | Female | Mandible | DLBCL | Yes | 4 months |
- —the Higher Education Personnel Improvement Coordination (CAPES), Ministry of Education
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphoma Diagnosis and Treatment · Oral and Maxillofacial Pathology · Sinusitis and nasal conditions
Introduction
1
Most periapical radiolucent lesions result from dental pulp necrosis and are classified as periapical lesions of endodontic origin [1]. In most cases, these lesions heal, and bone regeneration occurs after endodontic treatment [2]. However, the periapical region can also be affected by non‐endodontic lesions, which include a wide variety of pathologies such as cysts, benign and malignant tumors, fibro‐osseous lesions, and bacterial or fungal infections [1, 3]. The literature highlights that the clinical and radiographic similarity between endodontic and non‐endodontic lesions often complicates diagnostic differentiation, potentially leading to misdiagnosis and inappropriate treatment [4].
Among the lesions that may mimic endodontic pathologies, lymphomas should be considered in the differential diagnosis, particularly diffuse large B‐cell non‐Hodgkin lymphoma (DLBCL), the most common subtype of lymphoma affecting the oral cavity [3, 5]. Although lymphomas can involve the oral cavity and jawbones, their primary occurrence in these structures is rare, making definitive diagnosis challenging [5]. Patients with periapical lymphoma may present with signs and symptoms such as swelling, persistent pain, tooth mobility, and bone resorption, features often mistakenly attributed to endodontic diseases [6]. Additionally, these lesions may exhibit nonspecific radiographic characteristics, typically appearing as osteolytic areas with ill‐defined borders, which may delay diagnosis and negatively impact the patient's prognosis [7].
Given this scenario, the present case report describes a patient with DLBCL initially manifesting as a persistent periapical lesion in the anterior maxillary region. Moreover, we provide a comprehensive review of lymphomas occurring in the periapical region reported in English‐language literature. The literature review was conducted through a systematic search of the PubMed database, using combinations of terms related to diffuse large B‐cell non‐Hodgkin lymphoma (DLBCL), periapical lymphoma, malignant periapical lesions, and pathologies mimicking endodontic conditions. The search strategy was adapted according to the database indexing, with no restriction on publication date. Additionally, a manual search of the references of included studies was performed to identify further relevant articles. Duplicates were removed during the screening phase to ensure the inclusion of unique and pertinent studies for analysis. Two reviewers independently performed the initial screening of studies based on titles and abstracts, followed by full‐text reading. Any disagreements were resolved by a third reviewer. The Rayyan QCRI software was used for reference management, duplicate removal, and documentation of exclusion reasons. Data extraction was conducted by the first reviewer and subsequently verified by another, including the following information: author/year, age and gender of the population, diagnosis, performance of endodontic treatment, and time to diagnosis.
This study aims to emphasize the importance of recognizing the key characteristics of malignant periapical lesions, particularly lymphoma, by general practitioners and endodontists, as well as the necessity of establishing a differential diagnosis with lesions of endodontic origin.
Case Report
2
A 44‐year‐old male was referred to the Oral Medicine service for evaluation of an intraosseous lesion in the maxillary region. According to the patient's history, the initial evaluation and treatment were performed by an external private dentist approximately 60 days earlier, after the onset of intense pain in the upper left lateral incisor. At that time, a periapical radiograph was obtained, showing a diffuse radiolucent area in the periapical region of tooth #7. Clinical assessment included pulp vitality testing, which was negative, supporting the indication for endodontic treatment. Root canal therapy was then performed by the same provider. Following the endodontic procedure, the patient developed gingival edema and palatal swelling, and the same dentist carried out periodontal scaling and root planning associated with photobiomodulation therapy. Only after persistence and progression of the signs and symptoms was the patient referred to the Oral Medicine service for further investigation and management. His medical history included systemic hypertension, treated with BenicarAnlo. The patient denied alcohol, tobacco, or any other significant habits.
Upon physical examination, the patient appeared to be in good general health, with stable vital signs. However, facial asymmetry was observed in the left maxillary region. Intraoral examination revealed fibroelastic swelling in the anterior region of the left maxilla, resulting in a reduced maxillary vestibular fornix, with a purplish hue and a telangiectatic surface. In the interproximal region between central and lateral incisors, a reduction in the interdental papilla was observed, creating a “black space.” Additionally, a volume increase of approximately 1.5 cm was noted along the midline of the hard palate, with a smooth surface, a mucosa‐like color, and no tenderness upon palpation. The central and lateral incisors, canine and first premolar exhibited grade II mobility, with no fistulas or purulent discharge. Oral hygiene was adequate, and no odontogenic infectious foci were identified. A panoramic radiograph showed an imprecise radiolucent area on the periapical region of these teeth. Computed tomography (CT) scan revealed a hypodense lesion; with ill‐defined borders with involvement of the left maxillary sinus and the inferior portion of the nasal cavity, with important bone destruction (Figure 1) (Supplementary Material).
Initial clinical and radiographic aspects. (A‐B) Initial clinical examination revealing mild facial asymmetry due to a localized swelling in the upper left lip region (yellow arrow). (C) Intraoral swelling in the anterior region of the left maxilla, resulting in a reduced maxillary vestibular fornix, with a purplish hue and a telangiectatic surface. A decrease in the interdental papilla is observed in the interproximal region between teeth lateral and central incisors (yellow arrow). (D) Swelling along the midline of the hard palate. (E) Periapical radiograph demonstrating a diffuse radiolucent area at the periapex of tooth #7. (F) Panoramic radiograph showing a poorly defined radiolucent image in the periapical region of teeth. Tooth lateral incisor presents previous endodontic treatment. (G) Axial slice of computed tomography (CT) revealing an expansile hypodense lesion in the anterior maxillary region, associated with cortical bone disruption. (H) Coronal CT reconstruction demonstrating hypodensity in the left maxillary sinus and the inferior portion of the nasal cavity, associated with bone destruction. (I) Sagittal CT reconstruction showing satisfactory endodontic treatment of tooth lateral incisor, associated with bone destruction, cortical disruption, and root resorption.
Based on the clinical history and imaging findings, the main differential diagnoses included malignancy, particularly lymphoma or sarcoma. Fine needle aspiration (FNA) and incisional biopsy were performed under local anesthesia. For the incisional biopsy, a vestibular incision was made in the anterior maxilla, in the region of the left central and lateral incisors. A fragment of soft tissue was removed and submitted for histopathological analysis. Despite dental mobility, no extractions were required. The procedure was completed without complications, and postoperative healing was satisfactory. The smear obtained from the FNA revealed a representative sample showing large, round cells with frequent mitotic figures suggestive of lymphoma. Histopathological examination of the biopsy specimen revealed fibrous connective tissue densely infiltrated by mononuclear lymphocytes. Immunohistochemical analysis subsequently showed positivity for LCA, CD20, PAX5, CD10, and BCL‐6 in more than 30% of the cells, and BCL‐2 in fewer than 30% of the cells. A high proliferative index was identified (Ki‐67: 80%). CD3 and MUM‐1 antibodies were negative (Figure 2). Based on these findings, a diagnosis of Diffuse Large B‐Cell Non‐Hodgkin Lymphoma was established. The immunohistochemical panel is summarized in Table 1.
Microscopic analysis demonstrating connective tissue infiltrated by neoplastic cells. (A) Fine‐needle aspiration (FNA) smear revealing large, round cells with frequent mitotic figures. (B) Hematoxylin‐eosin staining showing atypical lymphoid cells with hyperchromatic nuclei and atypical mitotic activity. Immunohistochemical staining demonstrating positivity for (C) LCA, (D) CD20, (E) PAX5, (F) CD10, (G) BCL‐6 (>30%), (H) BCL‐2 (<30%), and (I) a high proliferative index with Ki‐67 expression at 80%.
Following the diagnosis, the patient was referred to an oncology service. During disease staging, a positron emission tomography‐computed tomography (PET/CT) scan demonstrated a hypermetabolic lesion in the left maxilla, with bone destruction and invasion into the inferior portion of the nasal cavity and ipsilateral maxillary sinus. In addition, other two lesions were identified in the proximal third of the right humerus and in the left cervical lymph node (Figure 3). The disease was classified as Ann Arbor stage IV A, with R‐IPI (Revised‐International Prognostic Index): 2 GOOD 80% 4Y PFS and CNS‐IPI (Central Nervous System‐International Prognostic Index): intermediate. The patient underwent six cycles of chemotherapy using the R‐CHOP regimen (Rituximab, Cyclophosphamide, Hydroxydaunorubicin, Vincristine sulfate, and Prednisone).
PET scan findings. (A) Whole‐body 18F‐FDG PET/CT scan revealing increased radiotracer uptake in the maxilla, right humerus, and left cervical lymph node. (B) PET/CT scan demonstrating a hypermetabolic lesion in the left maxilla, associated with bone destruction and invasion of the inferior portion of the nasal cavity and the ipsilateral maxillary sinus. (C) Hypermetabolic medullary lesion in the proximal third of the right humerus. (D) Hypermetabolic lesion in the left cervical lymph node.
Eighteen months after completing the treatment, intraoral physical examination revealed intact and normochromatic oral mucosa, with no clinical signs of disease. Only a scar was observed in the maxillary vestibular sulcus, consistent with the previous biopsy, and the gingival black space in the interproximal region between central and lateral incisors had been restored. No dental mobility was observed. A panoramic radiograph and cone‐beam computed tomography (CBCT) scan showed new bone formation in the anterior region of the left maxilla. The PET/CT scan demonstrated complete remission of the lesions (Figure 4). The patient continues to undergo regular clinical and imaging surveillance, monitored by the Oral Medicine and Oncology teams.
Clinical and radiographic assessment 18 months post‐treatment. (A‐B) Intraoral examination revealed intact, normochromatic oral mucosa, with no signs of swelling. The gingival “black space” in the interproximal region between central and lateral incisors had been successfully restored. (C) Panoramic radiograph demonstrating complete bone neoformation in the maxilla. (D‐F) Cone‐beam computed tomography (CBCT) scan confirming new bone formation in the anterior region of the left maxilla. (G‐I) PET/CT scan showing complete disease remission, with no evidence of hypermetabolic lesions in the maxilla, humerus, or cervical lymph node.
The literature review identified 75 cases of lymphomas involving the periapical region (Table 2). Patient age ranged from 3 to 84 years, with a mean of 43,13 years. Regarding gender distribution, 32 patients were female, and 42 were male. The mandible was the most frequently affected site, accounting for 43 cases, while two patients presented simultaneous lesions in both the maxilla and mandible. The most prevalent subtype was diffuse large B‐cell lymphoma (DLBCL), representing 37 cases. Endodontic treatment was performed in 30 cases, whereas 16 underwent tooth extraction prior to the definitive lymphoma diagnosis.
Discussion
3
This case report describes a rare presentation of diffuse large B‐cell lymphoma (DLBCL) initially manifesting as a persistent periapical lesion in the anterior maxilla, mimicking an endodontic pathology. The diagnostic complexity in distinguishing between endodontic and non‐endodontic periapical lesions is emphasized. Although the majority periapical radiolucencies are of endodontic origin and respond favorably to conventional root canal treatment, persistent cases should raise suspicion of an underlying malignancy [2].
Malignant non‐endodontic periapical lesions are rare diagnoses [3]. A literature review identified 30 distinct non‐endodontic pathological entities that mimicked inflammatory periapical lesions, with malignancies, including primary and metastatic tumors, accounting for 45.1% of cases [74]. However, a retrospective analysis of periapical biopsy specimens reported a lower incidence, with only 3.26% of cases classified as malignant [6].
Lymphomas account for approximately 5% of malignant neoplasms in the head and neck region, with half of these affecting the oral and maxillofacial structures [5]. Lymphomas are classified into two main categories based on histopathological characteristics, with non‐Hodgkin lymphoma (NHL) accounting for approximately 90% of cases, while Hodgkin lymphoma (HL) represents the remaining 10% [75, 76]. The different lymphoma subtypes are identified according to their cellular origin, including B‐cell lymphomas (BCL), T‐cell lymphoid tumors (TCL), natural killer/T‐cell lymphomas (T/NK‐NHL), and HL [77].
In our review, diffuse large B‐cell lymphoma (DLBCL) accounted for approximately 50% of the reported cases. This is the most prevalent subtype, including among periapical lymphomas [78, 79]. DLBCL, not otherwise specified (NOS), is an aggressive neoplasm characterized by large B‐cells arranged in a diffuse growth pattern [80]. Despite its aggressive behavior, DLBCL NOS is potentially curable and associated with a high survival rate (SR), particularly with early diagnosis and appropriate treatment [81]. A retrospective analysis of patients with DLBCL in the head and neck region revealed a 3‐year survival rate of 59.26%, with poor prognosis and increased risk of disease‐related mortality were observed exclusively in patients over 80 years old [75].
DLBCL, NOS involves extranodal sites in approximately 40% of cases, with the gastrointestinal tract being the most frequently affected, followed by bones, testes, spleen, thyroid, liver, kidneys, and adrenal glands [80]. In the head and neck, the most commonly involved site is the Waldeyer's ring, followed by the paranasal sinuses and oral cavity [76, 80]. Within the oral cavity and jawbones, the gingiva is the primary site of occurrence, though the palate is also a frequent location for early‐stage oral DLBCL, NOS [81]. Findings from our review demonstrated a higher frequency of mandibular involvement compared to the maxilla, with the mandible affected in over 57% of the cases analyzed.
When DLBCL NOS involves the jawbones, its clinical presentation is often nonspecific, mimicking endodontic, periodontal, and other osteolytic lesions [3, 5]. A systematic review evaluating leukemia and lymphoma cases that mimicked periapical lesions and led to endodontic treatment revealed that pain was present in 16.8% of cases, while edema was the most common clinical manifestation, affecting 35.8% of cases, followed by dental mobility (30.5%) [4]. The present case exhibited all these features, further complicating the initial diagnosis.
Although periapical lesions of neoplastic origin may share clinical features with endodontic pathologies, specific characteristics favor a malignant etiology. These include minimal caries, dental mobility without periodontal disease, regional paresthesia, cervical lymphadenopathy, and a lack of response to appropriate endodontic therapy [5, 27]. Neurological symptoms should prompt clinicians to investigate malignancy, as sensory disturbances, including numbness of the lips, tongue, cheek, and infraorbital region, often result from structural compromise of the mandibular canal, infraorbital nerve canal, or pterygopalatine fossa [82].
Radiographic assessment is fundamental in the diagnostic process. High‐quality radiographs and computed tomography (CT) scans are essential for accurately evaluating lesions and identifying subtle features that aid in differential diagnosis [79]. Lymphomas affecting the jaws are frequently associated with teeth, leading to root resorption and displacement. Additional radiographic findings include jaw expansion, locally destructive osteolytic lesions with poorly defined margins, and frequent cortical disruption [5, 79]. Ill‐defined lesion margins, uncommon in dental infections, may serve as radiographic indicators of malignancy [4, 78]. Additional radiographic patterns include a “moth‐eaten” appearance, lamellar periosteal bone formation, widening of the mandibular canal, irregular periodontal ligament space enlargement, and alterations in tooth spacing [5].
In cases of maxillary lymphoma, tumor progression may extend into adjacent anatomical structures, such as the maxillary sinus, hard palate, orbit, nasal cavity, pterygopalatine fossa, and infraorbital nerve canal [82]. In the present case, imaging demonstrated significant maxillary expansion with invasion into the maxillary sinus and nasal cavity, a pattern characteristic of aggressive neoplastic behavior. The presence of extensive bone destruction in these regions further reinforced the malignant nature of the lesion.
Similar to the present case, the literature indicates that periapical lymphomas are frequently misdiagnosed, as malignancy indicators are often overlooked, likely due to limited awareness that malignant neoplasms can mimic periapical conditions [4]. Studies show that nearly 49% of periapical lymphomas are initially mistaken for inflammatory periapical pathologies, leading to inappropriate endodontic treatment [5]. This finding supports the results of the review, which identified that 40% of misdiagnosed periapical lymphomas underwent endodontic treatment. This diagnostic delay can negatively impact prognosis and increase mortality rates [3, 4]. According to our findings, the time to definitive diagnosis ranged from 15 days to 2 years. In the current case achieved definitive diagnosis within approximately 3 months, emphasizing the importance of early suspicion.
This case underscores the necessity of considering malignancies in the differential diagnosis of persistent periapical lesions [4, 27]. Accurate clinic radiographic correlation, combined with histopathological evaluation, is essential for timely and precise diagnosis [79]. A thorough understanding of periapical malignancies and close collaboration among endodontists, pathologists, and oral medicine specialists are crucial for early diagnosis and improved patient outcomes.
Author Contributions
L.T.M.Q.C.: Conceptualization, Writing – original draft, Writing – review & editing; J.C.R.: Conceptualization, Investigation; I.S.P.F.: Investigation; S.M.P.L.: Investigation; A.R.S.‐S.: Investigation; P.A.V.: Investigation; M.A.L.: Conceptualization, Project administration, Writing – review & editing.
Funding
This work was supported in part by the Higher Education Personnel Improvement Coordination (CAPES), Ministry of Education, Brazil (Finance code 001—Grant number 88887.962729/2024‐00).
Conflicts of Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Ethics Statement
The study was conducted in accordance with the ethical principles established by the Institutional Research Ethics Committee, ensuring compliance with current ethical and scientific guidelines.
Clinical Study Registration
This study is a case report with a literature review and does not involve a clinical trial or prospective clinical study. Therefore, a Clinical Study Registration Number is not applicable.
Supporting information
Supporting Information: scd70162‐sup‐0001‐figure.png
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1T. Kosanwat , S. Poomsawat , and J. Kitisubkanchana , “Non‐Endodontic Periapical Lesions Clinically Diagnosed as Endodontic Periapical Lesions: A Retrospective Study Over 15 Years,” Journal of Clinical and Experimental Dentistry 13, no. 6 (2021): e 586–e 593, 10.4317/jced.57957.34188765 PMC 8223148 · doi ↗ · pubmed ↗
- 2K. Karamifar , A. Tondari , and M. A. Saghiri , “Endodontic Periapical Lesion: An Overview on Etiology, Diagnosis and Current Treatment Modalities,” European Endodontic Journal 5, no. 2 (2020): 54–67, 10.14744/eej.2020.42714.32766513 PMC 7398993 · doi ↗ · pubmed ↗
- 3L. F. Schuch and C. C. Vieira , “Uchoa Vasconcelos AC. Malignant Lesions Mimicking Endodontic Pathoses Lesion: A Systematic Review,” Journal of Endodontics 47 (2021): 178–188, 10.1016/j.joen.2020.08.023.32918962 · doi ↗ · pubmed ↗
- 4M. de Queiroga IS , V. Z. Drumond , L. G. Abreu , et al., “Leukemia and Lymphoma Mimicking Periapical Conditions Resulting in Endodontic Treatment: A Systematic Review,” Journal of Endodontics 51 (2025): 106–117, 10.1016/j.joen.2024.11.005.39577766 · doi ↗ · pubmed ↗
- 5H. Mortazavi , M. Baharvan , and K. Rezaeifar , “Periapical Lymphoma: Review of Reported Cases in the Literature,” Journal of Stomatology Oral and Maxillofacial Surgery 121 (2020): 404–407, 10.1016/j.jormas.2020.01.006.32035143 · doi ↗ · pubmed ↗
- 6C. C. Vieira , F. G. Pappen , L. B. Kirschnick , et al., “A Retrospective Brazilian Multicenter Study of Biopsies at the Periapical Area: Identification of Cases of Nonendodontic Periapical Lesions,” Journal of Endodontics 46 (2020): 490–495, 10.1016/j.joen.2020.01.003.32061420 · doi ↗ · pubmed ↗
- 7J. M. Dolan , A. De Graft‐Johnson , N. Mc Donald , B. B. Ward , T. J. Phillips , and S. M. Munz , “Maxillary and Mandibular Non‐Hodgkin Lymphoma With Concurrent Periapical Endodontic Disease: Diagnosis and Management,” Journal of Endodontics 43 (2017): 1744–1749, 10.1016/j.joen.2017.04.001.28734649 · doi ↗ · pubmed ↗
- 8L. Eisenbud , J. Sciubba , R. Mir , and S. A. Sachs , “Oral Presentations in Non‐Hodgkin's Lymphoma: A Review of Thirty‐One Cases. Oral Surgery,” Oral Medicine and Oral Pathology 57 (1984): 272–280, 10.1016/0030-4220(84)90183-X.6584818 · doi ↗ · pubmed ↗