Anterior sternoclavicular joint disruption with ipsilateral medial clavicle fracture in an adolescent: case report and literature review
Ahmed Alabdali, Omar AlQattan, Hanan Ahmad, Malak Almutairi, Abdullah Al Jubori

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
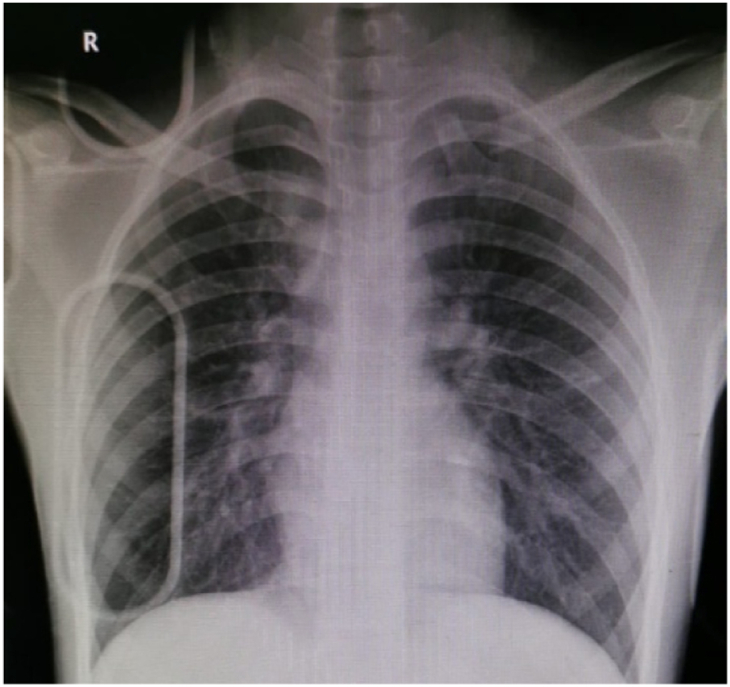 Figure 1
Figure 1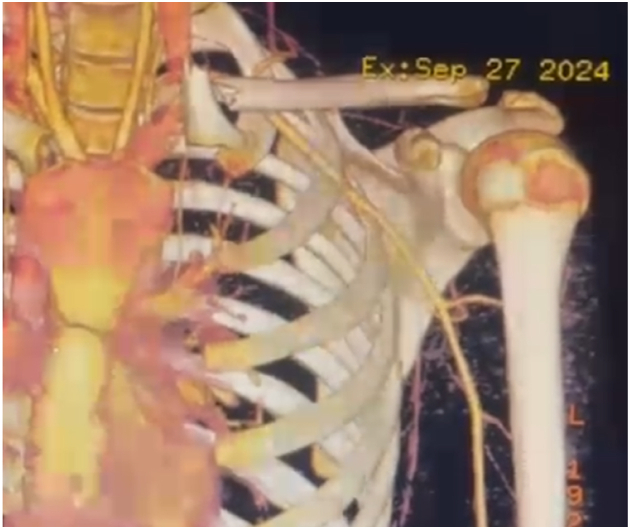 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5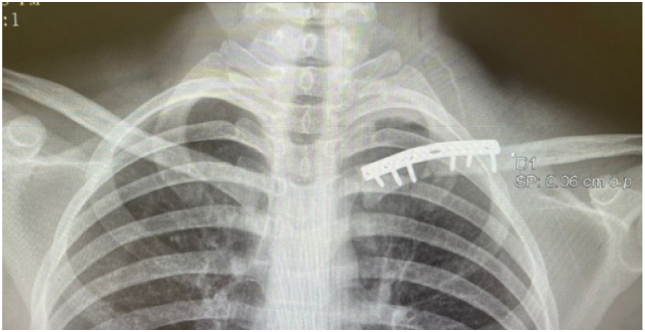 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder and Clavicle Injuries · Nerve Injury and Rehabilitation · Trauma Management and Diagnosis
Introduction
Dislocation of the sternoclavicular joint (SCJ) is a rare pathology in orthopedic trauma, with some studies reporting it accounts for less than 5% of all shoulder girdle injuries.18 In adults, these injuries typically occur as true dislocations following capsular and ligamentous disruption, whereas in skeletally immature patients whose medial clavicular physis is the last in the body to fuse, usually between 22 and 25 years of age, they often present as physeal fracture-dislocations or “pseudodislocations.” The anterior dislocation may result in ongoing pain and discomfort with some loss of function, while posterior dislocation carries far more serious potential complications due to possible injury to mediastinal structures.4^,^15^,^21 The incidence of physeal fractures of the medial clavicle is not well established, but this site is considered one of the rarest locations for physeal injury described in the literature.4 We report a rare case of anterior SCJ disruption with an associated ipsilateral clavicle fracture. Our goal with this report is to expand on the very limited data on SCJ disruption and ipsilateral clavicle fracture, thereby helping guide recognition and management in similar cases.
Case report
Initial assessment
A 15-year-old male presented initially to an outside hospital after he was involved in a high-speed road traffic accident with vehicle rollover. He was hemodynamically stable, alert, and oriented. He reported isolated pain localized to the left shoulder, without respiratory distress, dysphagia, neurological deficit, or signs of vascular compromise.
Plain radiographs demonstrated a medial clavicle fracture with associated SCJ disruption (Fig. 1). Computed tomography (CT) angiography of the SCJs confirmed anterior dislocation of the left SCJ with an associated medial clavicle fracture. The medial fragment was free-floating, rotated approximately 90° in the coronal plane, with its lateral aspect pointing superiorly and the sternal aspect directed inferiorly and anteriorly (Fig. 2). There was no evidence of compression of the great vessels.Figure 1. Initial anteroposterior chest radiograph demonstrating medial clavicle fracture with associated sternoclavicular joint disruption on the left side.Figure 2. Three-dimensional computed tomography (CT) angiographic reconstruction showing anterior dislocation of the left sternoclavicular joint and 90° rotation of the medial clavicle fragment without evidence of vascular compression.
The patient was referred to our institution for definitive management. On examination, he was neurovascularly intact with an obvious prominence and deformity over the left SCJ and overlying ecchymosis. No attempt at closed reduction had been made at the referring hospital, and no magnetic resonance imaging (MRI) was performed.
Decision-making
The decision for operative fixation of this injury pattern was made based on the severe displacement of the fracture and the apparent instability of the free-floating fragment. Consideration of a fixation construct spanning both the medial clavicle fracture and the SCJ was done, but ultimately decided against due to excessive soft tissue stripping needed for the spanning construct and the absolute need for future hardware removal of fixation spanning SCJ. The final pre-operative plan was for standard plating of the medial clavicle fracture and intraoperative assessment for any need for further fixation of the SCJ. The patient was booked and underwent the surgery 7 days after the initial injury.
Operative technique
Definitive management was performed with open reduction and internal fixation of the left medial clavicle fracture. The patient is in the beach chair position. The left clavicular region was prepped and draped in the usual sterile fashion. A cardiothoracic surgeon was on standby. A skin incision was made over the superior medial clavicle, followed by meticulous subcutaneous dissection, with identification and protection of the medial branch of the supraclavicular nerve.
The medial clavicle fracture was visualized, showing 90° rotation of the fragment consistent with CT findings (Fig. 3). Exposure of the clavicle was limited to only what was deemed necessary for the reduction of the clavicle fracture and for the placement of the plate; no attempt was made to expose the SCJ. Anatomical reduction was achieved with bone clamps and temporarily secured with a provisional K-wire (Fig. 4). Reduction of the clavicle fracture restored normal alignment of the SCJ on intraoperative fluoroscopy, showing reduction of the rotational element of the SCJ disruption on anterior–posterior views.Figure 3. Intraoperative exposure of the left medial clavicle showing the rotated free-floating fragment prior to reduction.Figure 4. Anatomical reduction achieved and provisionally secured with a K-wire under fluoroscopic guidance.
Definitive fixation was achieved with a superiorly placed 2.7 mm reconstruction plate, secured with 3 bicortical screws on each side of the fracture (Fig. 5). No additional fixation or suturing of any ligaments was done to the SCJ. Wound closure was in standard layered fashion of fascia over clavicle, platysma, subcutaneous tissue, and skin. Final intraoperative imaging confirmed satisfactory hardware placement and reduction of both the fracture and the SCJ (Fig. 6).Figure 5. Definitive fixation using a superiorly placed 2.7 mm reconstruction plate secured with 3 bicortical screws on each side of the fracture.Figure 6. Post-operative anteroposterior radiograph demonstrating satisfactory hardware placement and restoration of sternoclavicular joint alignment.
Post-operative course and follow-up
Post-operatively, the patient's arm was immobilized in a sling for one week, followed by a gradual return to active range of motion as tolerated. At the 1-week follow-up, forward flexion was 90°. By the 6-week review, the patient achieved forward flexion to 160°, abduction to 150°, and full functional use without pain. At 3 months, he had a full and symmetrical range of motion of the left shoulder compared with the contralateral side, with no tenderness over the SCJ and no radiographic evidence of loss of reduction or hardware complications. At the final follow-up (6 months), he remained asymptomatic, had returned to unrestricted activities, and radiographs confirmed complete union of the fracture with maintained joint congruity.
Discussion
Causes and mechanism of injuries
The most common cause of SCJ injury is road traffic accidents, followed by sports-related trauma. The mechanism is often classified into direct and indirect forces. Indirect forces are applied to the shoulder and transmitted to the SCJ.16 Combined injuries usually result from an amalgamation of multiple forces, as a single force would likely dissipate after causing one injury. This was the case in our patient, who sustained a rollover road traffic accident.
Dislocation vs. physeal injury
The medial clavicular physis does not begin ossification until approximately 18 years of age and does not fuse till around 25 years of age. SCJ dislocations in skeletally immature patients may not be a true dislocation but a physeal fracture sometimes termed pseudodislocation.10 This distinction is clinically significant. In true dislocations, there is disruption of the SCJ capsule and often associated injury to the costoclavicular and interclavicular ligaments, depending on whether the displacement is anterior or posterior.7 In contrast, physeal injuries may preserve these ligamentous attachments, as the periosteum and attached ligaments remain intact and avulse with the metaphyseal fragment.4 In skeletally immature patients with physeal injuries, a substantial degree of remodeling can be expected, which may make nonoperative management (“skillful neglect”) a viable option in certain anterior injuries. However, posterior injuries whether true dislocations or displaced physeal fractures carry the risk of serious mediastinal complications and often require urgent reduction.15 There are some rare reports of misdiagnosed chronic dislocation later being found to be pseudodislocation nonunions.5
Imaging
Due to the anatomical location of the SCJ, it is difficult to accurately assess the direction of injury on standard radiographs, and CT scanning is often required. CT angiography provides the added advantage of evaluating for associated vascular compromise. MRI is valuable for assessing ligamentous integrity and for differentiating true dislocations from pseudodislocations.10 Some surgeons do not routinely perform MRI, as the definitive nature of the injury can often be determined intraoperatively.11
Treatment
Because of the rarity of this specific injury pattern, the available evidence regarding its management is limited to case reports.
Closed reduction
Closed reduction of isolated physeal injuries can be successful, particularly if performed within 48 hours. It should be considered in all isolated physeal injuries, especially in posterior injuries, where there have been reports of severe complications such as pneumothorax, injury to the great vessels, tracheal injury, esophageal compression leading to dysphagia, and death.18 However, closed reduction maneuvers are described primarily for isolated SCJ injuries, not for combined injuries such as in our case, where a free-floating fragment was present. In such cases, there is a theoretical risk that attempted closed reduction could displace the fragment posteriorly, potentially resulting in catastrophic complications. There is a report of an ipsilateral SCJ dislocation with clavicle fracture in which closed reduction was attempted and failed, but no serious complication occurred.19
Operative fixation
A meta-analysis on SCJ dislocation identified irreducible posterior SCJ dislocation as an indication for open surgical treatment, while irreducible anterior dislocation in a healthy, active patient was considered a relative indication, based on clinical outcomes.17 Another meta-analysis focusing solely on posterior SCJ injuries in the adolescent population aimed to compare the outcomes of open and closed treatment methods. However, due to limited follow-up and significant variability in the techniques employed, the authors concluded that a formal statistical comparison was not possible.18
Regarding operative indications for isolated clavicle fractures in adolescents, a recent review states that the only absolute indications for surgery are open fractures, fractures with skin tenting, and major venous or arterial injury. Most other injuries are managed conservatively.13
Literature review
Review of the literature for ipsilateral SCJ disruption, whether in the adult or pediatric population, with associated clavicle fracture yielded a few results. Various treatment methods were implemented with generally good results (Table I).Table ILiterature review of ipsilateral sternoclavicular joint disruption or dislocation with clavicle fracture.Title (Yr)AuthorsThe injuriesImagingOpen vs. closed reductionFixation methodFollow-upComplicationsSternoclavicular physeal fracture. (2008)11Lampasi et al.14-yo boy; medial clavicle physeal fracture + adjacent clavicle fractureRadiographs + 3D CTOpen reduction (no closed attempt reported)Clavicle plating (reconstruction plate) + periosteal suture7 mo; full ROM, returned to sportsNone reportedAnterior SCJ dislocation with clavicle fracture (2013)9Khalid et al.17-yo male; anterior SCJ dislocation + mid-shaft clavicle fractureX-ray/CTOpen reductionClavicle plating + SCJ fusionHealed, but limited ROM compared to contralateralLimited ROM notedFracture and retrosternal SC dislocation (1978)8Kanoksikarin and Wearne19-yo male; clavicle fracture + posterior SCJ dislocationNot specifiedOpen reductionPin fixation + SCJ capsular repair17 mo; full ROM, returned to sportsNone notedSCJ disruption + clavicle fracture (2010)20Tompkins et al.9-yo boy; SCJ disruption + clavicle fractureX-ray/CTOpen reductionFiber-Wire transosseous suture6 mo; full ROM, returned to sportsNone notedEpiphyseal separation + clavicle fracture (1984)12Lemire and Rosman15-yo boy; epiphyseal separation + adjacent clavicle fractureX-ray/CTOpen reductionFigure-of-8 sutures through lateral fragment + periosteal suturing1 yr; returned to normal activityNot reportedHook-plate fixation case series (2022)23Zhang et al.17 patients >16 yo; proximal clavicle fracture + SCJ dislocationX-ray + CTOpen reduction (hook-plate applied)Hook-plate into sternum + screws into clavicle; in posterior cases a spacer/cap is added at the hook endNot reported; assumed unionTwo patients had complications (internal fixation failure; fracture nonunion)Medially displaced fracture-dislocation (2023)1Afifi et al.18-yo male; medial clavicle fracture + posterior SCJ disruptionCT (rotated fragment noted)Open reductionClavicle plating + figure-of-8 tape arthrodesis5 mo; healed, returned to trainingNone reportedAnterior SCJ dislocation + clavicle fracture (2021)14Reuter et al.45-yo male; clavicle fracture + anterior SCJ dislocationX-ray + CTOpen reductionTransosseous SCJ suture + clavicle locking plate12 weeks; healed, returned to pre-injury activityNone reportedTransosseous + plating in teens (2018)3Barrera-Ochoa et al.13- and 15-yo; medial clavicle fracture + posterior SCJ dislocationX-ray + CTOpen reductionTransosseous SCJ suture + clavicle plateFirst patient at 24 mo, second at 13 mo: both full ROMNone notedSCJ suture only (female, age 50) (2019)22Yadav et al.50-yo female; SCJ dislocation only (clavicle fracture implicit but not fixed)X-ray + CTOpen reductionTransosseous SCJ suture only6 mo; fracture healed, SCJ stable, full ROMNone reportedAdditional reports (1992; 1999)6Hardy; Allen and ZielinskiVarious ages with combined injuriesNot specifiedLikely openVariesFollow-up varies-Meta-analysis cautioning on K-wire use (2014)2Allen Jr BWarning about pin/K-wire complications————-SCJ, sternoclavicular joint; ROM, range of motion; 3D, three-dimensional; CT, computed tomography; yo, year-old.
It should be noted many authors are against pin or K-wire fixation in SCJ dislocations due to the possible complication of pin migration that has led to death in some cases.18
Conclusion
Ipsilateral SCJ disruption with clavicle fracture is rare, particularly in adolescents. Our case of a 15-year-old male treated with open reduction and rigid fixation of the medial clavicle using a reconstruction plate achieved stable SCJ alignment without direct joint fixation and resulted in full functional recovery. This case adds to the limited literature and supports the role of rigid clavicular fixation as a safe and effective treatment option in similar presentations.
Disclaimers:
Funding: No funding was disclosed by the authors.
Conflicts of interest: The authors, their immediate families, and any research foundations with which they are affiliated have not received any financial payments or other benefits from any commercial entity related to the subject of this article.
Patient consent: Obtained.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Afifi M.F.A.Waldmann S.Pisano A.A rare rotated, medially displaced fracture-dislocation of the medial clavicle–case report and review of the literature Trauma Case Rep 48202310096710.1016/j.tcr.2023.100967 PMC 1071944938098810 · doi ↗ · pubmed ↗
- 2Allen B.Jr.Zielinski C.Posterior fracture through the sternoclavicular physis associated with a clavicle fracture: a case report and literature review Am J Orthop (Belle Mead, NJ)28199959860010541148 · pubmed ↗
- 3Barrera-Ochoa S.Nuñez J.H.Domenech-Fernandez P.Bergua-Domingo J.M.Knorr J.Soldado F.Medial third clavicular fracture in combination with a posterior sternoclavicular dislocation in skeletally immature patients: 2 cases of a new proximal clavicular injury JSES Open Access 22018979910.1016/j.jses.2017.12.00930675574 PMC 6334882 · doi ↗ · pubmed ↗
- 4Beckmann N.Crawford L.Posterior sternoclavicular Salter-Harris fracture-dislocation in a patient with unossified medial clavicle epiphysis Skeletal Radiol 4520161123112710.1007/s 00256-016-2399-227107998 · doi ↗ · pubmed ↗
- 5Brinker M.R.Simon R.G.Pseudo-dislocation of the sternoclavicular joint J Orthop Trauma 1319992222251020625610.1097/00005131-199903000-00012 · doi ↗ · pubmed ↗
- 6JRH.Complex clavicular injury in childhood J Bone Joint Surg Br 741992154173224810.1302/0301-620X.74B 1.1732248 · doi ↗ · pubmed ↗
- 7Jaggard M.K.Gupte C.M.Gulati V.Reilly P.A comprehensive review of trauma and disruption to the sternoclavicular joint with the proposal of a new classification system J Trauma Acute Care Surg 66200957658410.1097/TA.0b 013e 31817 fd 96b 19204537 · doi ↗ · pubmed ↗
- 8Kan OK Sikarin S.Wearne W.Fracture and retrosternal dislocation of the clavicle Aust New Zealand J Surg 481978959627635710.1111/j.1445-2197.1978.tb 05816.x · doi ↗ · pubmed ↗