Preliminary clinical outcomes of shoelace repair with internal brace for ulnar collateral ligament injuries with chronic avulsion bone fragments in student baseball players
Yasuhiro Mitsui, Kazuto Higuchi, Koji Hara, Ryunosuke Abe, Syuichiro Sakai, Toshihiko Yoshida

TL;DR
A new surgical technique for ulnar collateral ligament injuries in baseball players shows similar success with or without bone fragments.
Contribution
Demonstrates shoelace repair with internal brace is effective for UCL injuries with chronic avulsion bone fragments.
Findings
All patients returned to play with no significant differences in sports scores between groups.
No complications were observed in either group with or without bone fragments.
The technique is viable for young athletes with minimal ligament degeneration.
Abstract
Ulnar collateral ligament (UCL) repair with internal brace augmentation has demonstrated promising results. Traditionally, chronic avulsion bone fragments (BFs) at the UCL attachment site have been considered as indications for reconstruction. We applied a shoelace repair technique combined with internal bracing in student baseball players with and without such BFs. We hypothesized that favorable clinical outcomes could be achieved regardless of the presence of BFs. This study aimed to evaluate the clinical outcomes of shoelace repair with internal brace technique. Eighteen student baseball players who underwent shoelace repair with internal brace were included. Based on pre-operative radiographs and computed tomography scans, patients were classified into those with BFs (n = 8) and those without (n = 10). Post-operative outcomes were assessed and compared between the 2 groups using…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
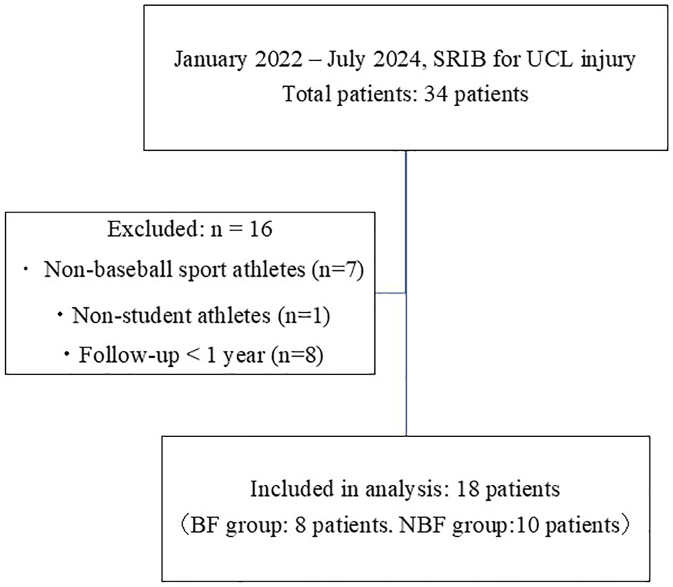 Figure 1
Figure 1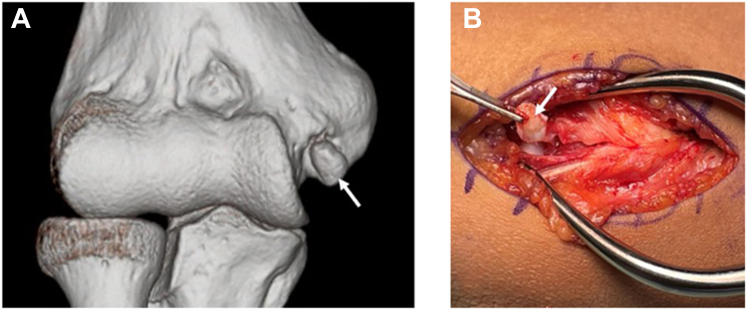 Figure 2
Figure 2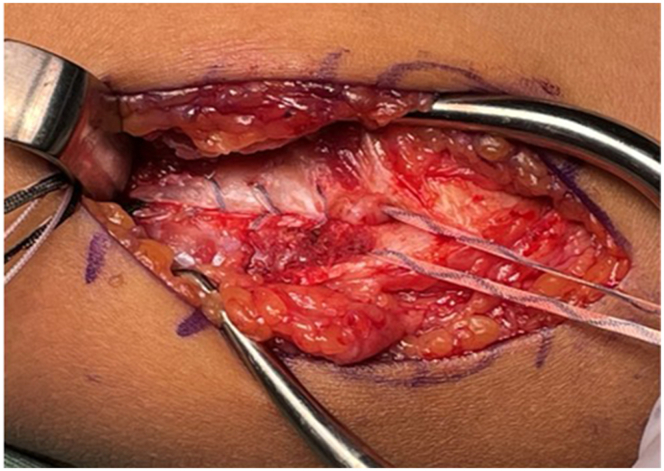 Figure 3
Figure 3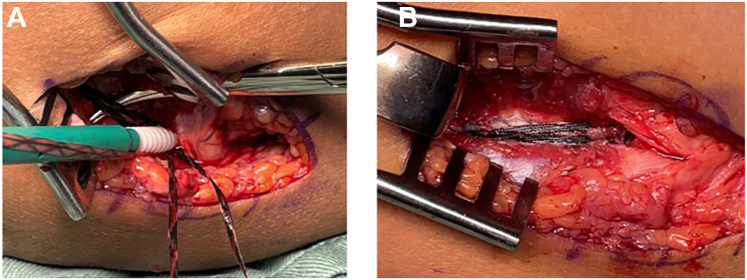 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSports injuries and prevention · Foot and Ankle Surgery · Knee injuries and reconstruction techniques
Ulnar collateral ligament (UCL) injury is one of the most severe throwing-related injuries affecting the upper extremity. In baseball players, it typically results from cumulative microtrauma due to repetitive throwing motions.3^,^9 In the United States, the number of UCL reconstruction surgeries significantly increased from 2007 to 2011, with the highest rates observed in baseball players aged 15-19 years, showing an average annual growth of about 9%.15 Furthermore, by 2025, the incidence of UCL reconstruction in this age group is projected to reach 14.5 per 100,000 individuals.7^,^22
Initial treatment options include cessation of throwing, physical therapy, and conservative approaches such as platelet-rich plasma therapy8^,^20 and extracorporeal shock wave therapy.20 If conservative management fails, surgical intervention is considered. The standard surgical treatment for UCL injury is ligament reconstruction using a tendon graft, which has demonstrated favorable outcomes.6^,^10^,^17^,^21^,^36 However, a major limitation of reconstruction is the prolonged recovery time, often resulting in the loss of 1 to 2 competitive seasons.32
Recently, UCL repair using internal brace (IB) augmentation with FiberTape (Arthrex, Naples, FL, USA) has garnered attention.5^,^14 Dugas et al14 reported that IB provided superior initial fixation strength compared with reconstruction in biomechanical studies. In addition, IB demonstrated comparable resistance to gapping and failure under high valgus torque.4^,^5 In clinical studies, Dugas et al12 performed IB repair in overhead athletes aiming for early return to play (RTP). Reconstruction was performed in cases with bone fragments (BFs) or severe ligament degeneration. They found comparable clinical outcomes, with IB offering a shorter time to RTP.
According to Savoie et al,31 younger overhead athletes typically exhibit less ligament degeneration than professionals, making them more suitable candidates for UCL repair rather than reconstruction. Based on this rationale, we considered that the shoelace repair with internal brace augmentation (SRIB) could also be effective in cases involving BFs. Traditionally, these cases have been considered indications for reconstruction, based on the assumption that primary repair is not feasible after fragment removal. This technique may allow for primary repair even after fragment excision, potentially expanding the indications for UCL repair. Since January 2022, we have performed SRIB in student baseball players with minimal ligament degeneration, based on magnetic resonance imaging (MRI), ultrasound, and intraoperative findings, regardless of the presence of BFs. Previous reports have indicated that valgus instability may occur following medial epicondyle avulsion fractures, regardless of whether bony union is achieved.16^,^27 Harada et al18 also reported that nonunion of medial epicondyle fragments may be associated with subsequent recurrence and other injuries. Untreated childhood avulsion injuries of the medial epicondyle may result in chronic BFs, increasing the risk of medial elbow pain and UCL insufficiency during adolescence.26 Therefore, addressing these chronic fragments during surgical repair may help prevent long-term dysfunction and further support the indication of SRIB in such cases.
This study aimed to investigate the influence of BFs on the short-term post-operative outcomes of SRIB in student baseball players. We hypothesized that favorable clinical outcomes could be achieved regardless of the presence of BFs.
Materials and methods
Patient population
This study was approved by the relevant institutional review board (approval number 2502); all patients provided informed consent regarding participation and publication of the study. This study included patients diagnosed with UCL injury between January 2022 and July 2024. The inclusion criteria for UCL injury were: (1) tenderness along the UCL, (2) imaging findings on MRI or ultrasound indicating UCL injury, and (3) positive results on both the moving valgus stress test and milking test.
Surgical indications were as follows: (1) failure of conservative treatment for more than 3 months, (2) medial joint space widening of ≥2 mm in the affected elbow compared with the contralateral (uninjured) side on ultrasound performed under gravity stress (shoulder 90° abduction, elbow 90° flexion), and (3) cases requiring early return to sports. Exclusion criteria were: (1) athletes participating in sports other than baseball, (2) nonstudent (adult) athletes, and (3) patients with less than 1 year of post-operative follow-up. After applying these criteria, 18 patients were included in the final analysis (Fig. 1). Chronic avulsion BFs were defined as residual ossified fragments at the proximal or distal UCL attachment, clearly separated from the bone on radiographs or computed tomography.Figure 1. Flow diagram of patient selection. A total of 34 patients underwent SRIB for UCL injury between January 2022 and July 2024. After applying the inclusion and exclusion criteria, 18 student baseball players were included in the final analysis (8 with BFs and 10 without [NBF]). Excluded cases included adult athletes, nonbaseball players, and those with less than 1-year post-operative follow-up. SRIB, shoelace with internal brace; UCL, ulnar collateral ligament; BF, bone fragment; NBF, no bone fragment.
Image findings
UCL injury classification was performed using pre-operative MRI (1.5 T; Philips Medical Systems, Tokyo, Japan), based on the method described by Ramkumar et al.28^,^29 Proximal partial tears were classified as type 1A and complete tears as type 1B; midsubstance partial and complete tears as types 2A and 2B, respectively; and distal partial and complete tears as types 3A and 3B, respectively.
BFs were evaluated using pre-operative radiographs and computed tomography (Canon Medical Systems, Tokyo, Japan). Fragments located between the medial epicondyle and sublime tubercle were classified based on their relative position: those closer to the medial epicondyle were categorized as proximal, and those closer to the sublime tubercle as distal. Patients with BFs were classified as BF–positive, and those without BF as no bone fragment (NBF). All BF cases involved chronic avulsion-type BFs.
Operative technique
All procedures were performed by a single senior orthopedic surgeon specializing in elbow surgery (Y.M.). Surgery was performed through a muscle-splitting approach to allow direct visualization and assessment of the UCL. If significant ligament degeneration was observed intraoperatively, the procedure was converted to ligament reconstruction. One patient was converted to ligament reconstruction owing to severe ligament degeneration that was deemed unsuitable for repair; this case was excluded from the final analysis. The UCL was split along the direction of its fibers. When chronic avulsion-type BFs were present at the proximal or distal ligament attachment, they were often found embedded within the ligament substance. In our practice, SRIB is considered feasible when the avulsion BF is ≤ 1 cm; for larger fragments, ligament reconstruction is preferred. These fragments were carefully excised in a minimally invasive manner to preserve the structural integrity of the ligament. Although minor ligament defects were unavoidable due to the intraligamentous nature of the fragments, excessive resection was meticulously avoided, as a large defect could preclude the use of repair techniques (Fig. 2, A and B).Figure 2. Pre-operative and intraoperative images. (A) Pre-operative 3D-CT image showing a chronic avulsion-type bone fragment at the proximal UCL attachment site (white arrow). (B) Intraoperative image after splitting the UCL along the direction of its fibers, showing the excised proximal bone fragment (white arrow). 3D, three dimensional; CT, computed tomography; UCL, ulnar collateral ligament.
A 4.75-mm absorbable SwiveLock anchor (Arthrex, Naples, FL, USA), loaded with 2 SutureTapes (1.3 mm; Arthrex, Naples, FL, USA) and one 2-0 FiberWire (Arthrex, Naples, FL, USA) (yielding 6 suture limbs in total), was inserted into the sublime tubercle regardless of tear location (proximal or distal) or the presence of BFs. The 2-0 FiberWire was used for distal ligament repair, whereas 2 of the 4 SutureTape limbs were used to perform a shoelace repair of the split UCL, applying adequate tension to restore ligament continuity (Fig. 3). The remaining 2 SutureTape limbs were used as an IB.Figure 3. Intraoperative image showing shoelace repair of the split UCL using 2 SutureTape (1.3-mm) limbs from the anchor placed in the sublime tubercle. The white-and-blue–striped tapes are SutureTapes used for the shoelace repair. UCL, ulnar collateral ligament.
All suture limbs were then fixed together using another 4.75-mm absorbable SwiveLock anchor, which was inserted at the inferior margin of the medial epicondyle corresponding to the isometric point of the ligament, with the elbow flexed at 60°. To avoid overtensioning of the IB limbs, a fine Pean clamp was inserted beneath them during fixation (Fig. 4, A and B).Figure 4. Final fixation using a second SwiveLock anchor at the medial epicondyle. (A) Pean clamp inserted under the internal brace to prevent overtensioning. (B) Shoelace repair with internal brace, final view. The black SutureTapes (1.3-mm) are used for the internal brace.
Post-operative rehabilitation
The elbow was immobilized with a splint for 1 week following surgery. Starting 1 week post-operatively, a hinged elbow brace was applied, and range of motion exercises were initiated, with both flexion and extension increased by 10° each week (total 20° per week). The brace was removed at 2 months post-operatively. The throwing program was initiated at 3 months post-operatively. RTP was typically targeted at 6 months for position players and 8 months for pitchers, depending on individual recovery.
Baseline and follow-up patient-reported and return-to-sport outcomes
Clinical outcomes were assessed using the Japan Orthopedic Association Sports (JOA Sports) score, Kerlan–Jobe Orthopedic Clinic (KJOC) Overhead Athletes Shoulder and Elbow score, and Disabilities of the Arm, Shoulder, and Hand (DASH) sports module score. RTP was defined as participation in at least one official game following surgery.
Post-operative competitive level was evaluated using the Conway scale,9 where:
- •“Excellent” indicated return to the same or higher competitive level for at least 12 months
- •“Good” indicated return to a lower competitive level than preinjury
- •“Fair” indicated return to recreational play
- •“Poor” indicated failure to return to sports
Statistical analyses
Statistical analyses were performed using R software (version 3.6.3, R Foundation for Statistical Computing, Vienna, Austria). Pre-operative and post-operative clinical outcomes were compared using paired t-test and Wilcoxon signed-rank test. Two-group comparisons between the BF and NBF groups for patient characteristics, clinical scores, and time to RTP were conducted using independent samples t-test and Mann–Whitney U test. Comparisons of UCL injury classification and Conway scale between groups were performed using Pearson chi-square test. A P value <.05 was considered statistically significant.
Results
Surgical cases and patient characteristics
A total of 34 patients underwent SRIB for UCL injury, of which 18 met the inclusion criteria and were included in this study (Fig. 4). Among them, 8 patients were classified into the BF group (proximal: 6 cases, distal: 2 cases), and 10 were classified into NBF group. Patient characteristics and comparisons between the BF and NBF groups are summarized in Table I. There were no significant differences between the BF and NBF groups in terms of age (17.0 ± 1.2 vs. 16.8 ± 2.3 years; P = .37), height (173 ± 0.8 vs. 172 ± 0.6 cm; P = .75), weight (71.5 ± 6.1 vs. 73.7 ± 9.9 kg; P = .59), body mass index (BMI) (24.7 ± 2.4 vs. 23.7 ± 1.1 kg/m^2^; P = .30), competition level (7 high school and 1 college student vs. 9 high school and 1 college student; P = .59), or player position (5 pitchers, 2 catchers and 1 infielders vs. 6 pitchers, 1 catchers, 2 infielders, and 1 outfielders; P = .66).Table IPatient characteristics.OutcomeBF (N = 8)NBF (N = 10)P valueAge (yr)17 ± 1.216.8 ± 2.3.37Height (cm)173 ± 0.8172 ± 0.6.75Weight (kg)71.5 ± 6.173.7 ± 9.9.59BMI (kg/m^2^)24.7 ± 2.423.7 ± 1.1.3Level.59 High school79 College11Position.66 Pitcher56 Catcher21 Infielder12 Outfielder01BMI, body mass index; BF, bone fragment; NBF, no bone fragment.
Regarding the classification of UCL injuries, 5 patients in the BF group and 6 in the NBF group were classified as type 1A, whereas one patient in the BF group and none in the NBF group were classified as type 1B. No cases in either group were classified as types 2A or 2B.
Two patients in the BF group and one in the NBF group were classified as type 3A, whereas no patients in the BF group and 3 in the NBF group were classified as type 3B. There were no significant differences in UCL injury classification between the 2 groups (P = .23) (Table II).Table IIUCL injury classification.OutcomeBF (N = 8)NBF (N = 10)P valueUCL injury classification.23 1A56 1B10 2A00 2B00 3A21 3B03UCL, ulnar collateral ligament; BF, bone fragment; NBF, no bone fragment.
Pre-operative and post-operative clinical scores
The pre-operative and post-operative clinical outcomes of the 18 cases (pre-operative/post-operative: P value) are shown in Table III. Significant improvements were observed in the JOA sports score (30.5/90.5 points: P < .0001), DASH sports score (81.2/6.9 points: P < .0001), and KJOC score (40.3/85.3 points: P < .0001). The follow-up period for each group were: BF 22.8 months and NBF 21.5 months, with no significant difference between the 2 groups (P = .77).Table IIIPre-operative and post-operative clinical score.OutcomePre-operativePost-operativeP valueJOA sports score (points)30.5 ± 18.790.5 ± 11.5<.0001∗DASH sports score (points)81.2 ± 15.36.9 ± 13.2<.0001∗KJOC score (points)40.3 ± 15.285.3 ± 11.4<.0001∗JOA, Japan Orthopedic Association; DASH, disabilities of the arm, shoulder, and hand; KJOC, Kerlan–Jobe Orthopedic Clinic.∗P < .001.
In the BF group, the pre-operative and post-operative clinical outcomes (pre-operative/post-operative: P value) showed significant improvements in the JOA sports score (25.8/87.8 points: P = .0001), DASH sports score (79.6/7 points: P = .007), and KJOC score (39/85.6 points: P = .007).
In the NBF group, the pre-operative and post-operative clinical outcomes (pre-operative/post-operative: P value) showed significant improvements in the JOA sports score (35/85.8 points: P < .0001), DASH sports score (82.5/6.8 points: P = .003), and KJOC score (41.5/85.2 points: P < .0001).
In the post-operative clinical outcomes between the 2 groups (BF/NBF: P value), there were no significant differences in the JOA sports score (87.8/85.8 points: P = .73), DASH sports score (7/6.8 points: P = .74), or KJOC score (85.6/85.2 points: P = .93) (Table IV).Table IVPre-operative and post-operative clinical score of BF and NBF.OutcomeBF (N = 8)NBF (N = 10)P value (BF vs. NBF)Follow-up time (mo)22.8 ± 10.521.5 ± 7.3.77JOA sports score (points) Pre-operative25.8 ± 19.535.0 ± 17.5.31 Post-operative87.8 ± 10.985.8 ± 12.5.73 P value (pre-operative vs. post-operative).0001∗<.0001∗DASH sports score (points) Pre-operative79.6 ± 17.682.5 ± 14.0.71 Post-operative7.0 ± 10.26.8 ± 15.7.74 P value (pre-operative vs. post-operative).007†.003†KJOC score (points) Pre-operative39.0 ± 17.841.5 ± 13.8.64 Post-operative85.6 ± 9.985.2 ± 12.9.93 P value (pre-operative vs. post-operative).007†<.0001∗JOA, Japan Orthopedic Association; DASH, disabilities of the arm, shoulder, and hand; KJOC, Kerlan–Jobe Orthopedic Clinic; BF, bone fragment; NBF, no bone fragment.∗P < .001.†P < .01.
The RTP duration was 7.5 months for the BF group and 8 months for the NBF group, with no significant difference (P = .58). Based on the Conway scale, 7 cases in the BF group were classified as excellent, 1 as good, and none as fair or poor, whereas 8 cases in the NBF group were classified as excellent, 2 as good, and none as fair or poor. No significant difference was observed between the 2 groups (P = .67) (Table V). These results suggest that favorable clinical outcomes and RTP can be achieved using SRIB regardless of the presence of BFs. No perioperative or post-operative complications were observed with SRIB in either group.Table VReturn-to-sports competitive performance between bone fragment + or –.OutcomeBF (N = 8)NBF (N = 10)P valueTRP (mo)7.5 ± 2.28.0 ± 1.6.58Conway scale Excellent78.67 Good12 Fair00 Poor00TRP, time to return to play; BF, bone fragment; NBF, no bone fragment.
Discussion
To the best of our knowledge, this is the first clinical study to compare short-term clinical outcomes of SRIB in student baseball players with and without chronic avulsion BFs. Our results demonstrated no significant differences in clinical outcomes between patients with and without BFs, suggesting the feasibility of SRIB as a surgical option in such cases.
Since Dr Frank Jobe first reported on UCL reconstruction in 1974, it has become the gold standard for the treatment of UCL injuries.10^,^17^,^21^,^36 In contrast, UCL repair was first performed by Norwood et al24 in 1981 for athletes with UCL injuries, and they reported satisfactory outcomes. However, a comparative study evaluating post-operative outcomes of reconstruction vs. repair in overhead athletes reported a RTP rate of 68% for reconstruction and 50% for repair. Among professional athletes, the RTP rate was 75% for reconstruction and 29% for repair, indicating superior outcomes with reconstruction.9
In 2006, Argo et al2 reported performing UCL repair on female athletes, including overhead athletes, with a 94% RTP rate at their preinjury competitive level. Similarly, Savoie et al31 reported an RTP rate of 93%. These favorable outcomes were attributed to the inclusion of student athletes, who are believed to exhibit less ligament degeneration compared with professional athletes.19^,^22^,^35 Since then, advancements in surgical techniques, such as the use of IB and more selective surgical indications, have resulted in RTP rates of 87%-96%, which are comparable to those achieved with reconstruction.1^,^12^,^13^,^25^,^29^,^30 Consistent with previous findings, the present study demonstrated favorable clinical outcomes in student baseball players undergoing SRIB, with all patients successfully returning to competitive play.
Among student athletes with UCL injuries, some present with lesions or avulsion of the medial epicondyle that originated around the age of 10 years, leading to valgus instability and the need for surgical intervention.32 In such cases, UCL reconstruction is often indicated in the United States.11^,^13^,^31 This is due to shortening of the UCL and degenerative changes around the BF, which make primary repair infeasible.23^,^34 However, reconstruction typically requires 11.6-16.8 months for RTP,6^,^10^,^17^,^21^,^36 resulting in the loss of one to 2 competitive seasons.33 Moreover, many high school athletes may be hesitant to undergo surgery owing to the prolonged recovery period required before returning to competition.19 One of the advantages of UCL repair is that it allows preservation of the native anatomy and sensory function.1
Considering these factors, we adopted SRIB for student baseball players seeking early RTP, regardless of the presence of BFs. Uchida et al35 reported that in shoelace repair, passing the suture tape through the distal UCL enables the tendon complex—including the UCL and flexor–pronator muscles—to converge at the medial epicondyle, thereby restoring the dynamic stabilizing mechanism. Although Uchida et al35 reported the technical feasibility of SRIB for chronic avulsion injuries, no clinical outcome data were presented, limiting its clinical applicability. The present study addresses this gap by directly comparing outcomes with and without BFs. In particular, the shoelace pattern may enhance not only longitudinal but also transverse tensioning of the ligament, which could further enhance medial elbow stability through improved dynamic muscle function, consistent with the role of the flexor–pronator group as described by Hoshika et al19 This technique has been considered useful in managing UCL instability associated with Little League elbow. In the present study, SRIB was employed in all cases, and no significant differences were observed between the BF and NBF groups in clinical outcomes, RTP duration, or Conway scale scores.
This study has some limitations. First, the sample size was small. Second, only short-term outcomes were assessed, and long-term follow-up is warranted. Third, no biomechanical analysis of the shoelace repair technique was conducted. In addition, the assessment of ligament quality during surgery was based on the subjective intraoperative judgment of the operating surgeon, which may have introduced selection bias. Furthermore, potential selection bias due to intraoperative conversion to reconstruction may limit the generalizability of our findings. Moreover, the high RTP rate observed in this cohort may partly reflect the inclusion of highly motivated student athletes with relatively mild degeneration, potentially introducing selection bias. Therefore, the present findings should be interpreted as preliminary clinical evidence, and the absence of significant differences between groups should be viewed cautiously given the limited sample size and statistical power.
Taken together, these findings suggest that SRIB may be considered a viable option for carefully selected young athletes with chronic avulsion BFs, although further prospective studies with larger cohorts are warranted to confirm its long-term effectiveness. Future studies incorporating biomechanical validation and larger, more diverse cohorts are warranted to establish the long-term efficacy of SRIB, especially in athletes with advanced degeneration or higher levels of competition. These findings may help refine surgical decision-making in young athletes with UCL injuries, expanding the indications for repair-based techniques beyond traditional boundaries.
Conclusion
SRIB was performed in student baseball players with and without chronic avulsion BFs, and post-operative outcomes were comparable between the groups. These findings suggest that SRIB may be a viable and safe surgical option in carefully selected young athletes with adequate tissue quality, thereby providing a balance between stability and early RTP.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Anvari A.Fathi A.Bolia I.K.Piatt E.Hasan L.K.Haratian A.Utilization of internal bracing in elbow medial UCL stabilization: from biomechanics to clinical application and patient outcomes Orthop Res Rev 13202120120810.2147/ORR.S 32189034703328 PMC 8541765 · doi ↗ · pubmed ↗
- 2Argo D.Trenhaile S.W.Savoie F.H.3rd Field L.D.Operative treatment of ulnar collateral ligament insufficiency of the elbow in female athletes Am J Sports Med 34200643143710.1177/036354650528124016282580 · doi ↗ · pubmed ↗
- 3Azar F.M.Andrews J.R.Wilk K.E.Groh D.Operative treatment of ulnar collateral ligament injuries of the elbow in athletes Am J Sports Med 28200016231065353810.1177/03635465000280011401 · doi ↗ · pubmed ↗
- 4Bernholt D.L.Lake S.P.Castile R.M.Papangelou C.Hauck O.Smith M.V.Biomechanical comparison of docking ulnar collateral ligament reconstruction with and without an internal brace J Shoulder Elbow Surg 2820192247225210.1016/j.jse.2019.04.06131351903 · doi ↗ · pubmed ↗
- 5Bodendorfer B.M.Looney A.M.Lipkin S.L.Nolton E.C.Li J.Najarian R.G.Biomechanical comparison of ulnar collateral ligament reconstruction with the docking technique versus repair with internal bracing Am J Sports Med 4620183495350110.1177/036354651880377130403369 · doi ↗ · pubmed ↗
- 6Cain E.L.Andrews J.R.Dugas J.R.Wilk K.E.Mc Michael C.S.Walter J.C.2nd Outcome of ulnar collateral ligament reconstruction of the elbow in 1281 athletes: results in 743 athletes with minimum 2-year follow-up Am J Sports Med 3820102426243410.1177/036354651037810020929932 · doi ↗ · pubmed ↗
- 7Camp C.L.Conte S.D’Angelo J.Fealy S.A.Ahmad C.S.Effect of predraft ulnar collateral ligament reconstruction on future performance in professional baseball: a matched cohort comparison Am J Sports Med 4620181459146410.1177/036354651875829829543498 · doi ↗ · pubmed ↗
- 8Chauhan A.Mc Queen P.Chalmers P.N.Ciccotti M.G.Camp C.L.D'Angelo J.Nonoperative treatment of elbow ulnar collateral ligament injuries with and without platelet-rich plasma in professional baseball players: a comparative and matched cohort analysis Am J Sports Med 4720193107311910.1177/036354651987630531589470 · doi ↗ · pubmed ↗