Integrating a Large Language Model to Streamline Nursing Handover Documentation Across Multiple Hospitals in Taiwan: Development and Implementation Study
Ray-Jade Chen, Mai-Szu Wu, Lung-Wen Tsai, Shy-Shin Chang, Shu-Tai Shen Hsiao, Yu-Sheng Lo

TL;DR
This study shows how integrating a large language model into nursing documentation systems can significantly reduce the time nurses spend on handover tasks across multiple hospitals in Taiwan.
Contribution
The novel contribution is the successful deployment of an LLM-integrated nursing information system across three hospitals, demonstrating measurable time savings and workflow efficiency.
Findings
LLM integration reduced per-patient handover documentation time from 3.45-4.32 minutes to 1.17-2.54 minutes.
Aggregate monthly time savings across three hospitals ranged from 474 to 981 hours.
Nurse verification was required to ensure accuracy and mitigate hallucinations in LLM-generated content.
Abstract
The global nursing shortage, exacerbated by heavy workloads and high turnover rates associated with the COVID-19 pandemic, continues to undermine care quality and nurse well-being. Although digital health technologies have enhanced coordination, improved communication, and reduced clinical errors in nursing practice, they have also increased nurses’ documentation burden. Advances in large language models (LLMs) and other generative artificial intelligence (GenAI) tools facilitate the generation of accurate reports from electronic medical records (EMRs), thereby streamlining documentation workflows, saving time, and reducing nurses’ workloads. Accordingly, integrating LLMs into electronic nursing documentation systems warrants further exploration. This study examines the integration of an LLM into an in-house nursing information system (NIS) implemented across 3 hospitals in Taiwan to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
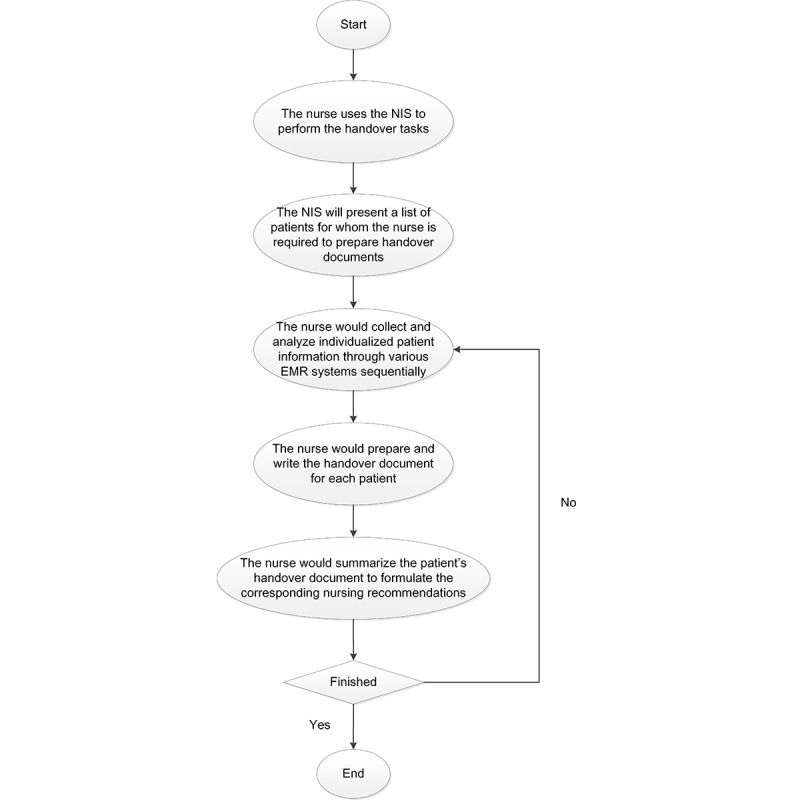 Figure 1
Figure 1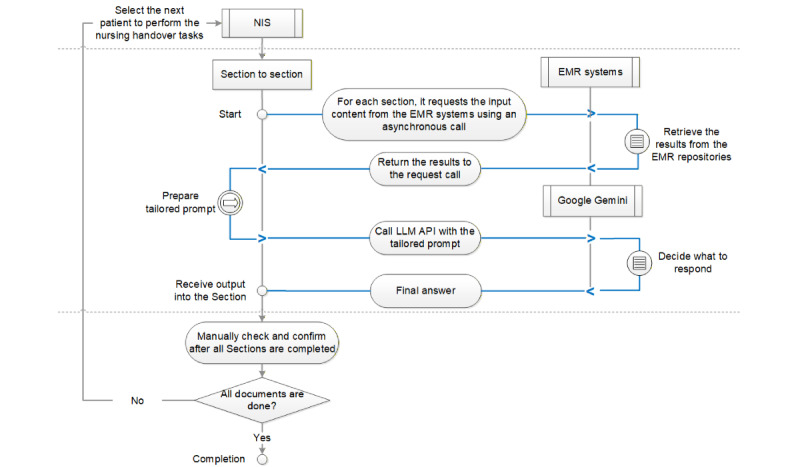 Figure 2
Figure 2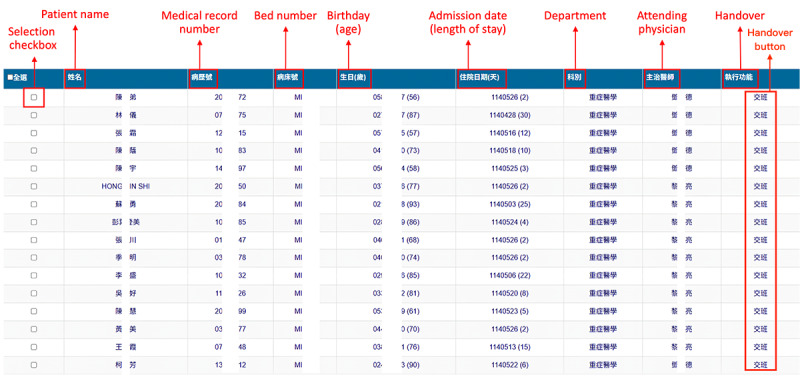 Figure 3
Figure 3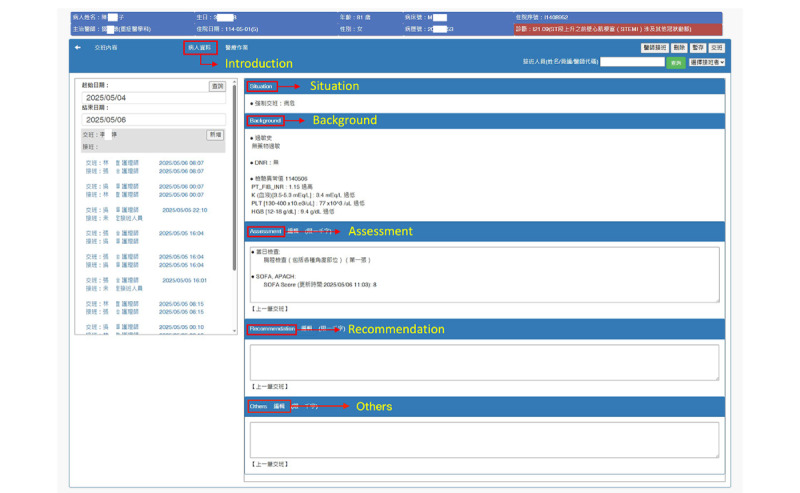 Figure 4
Figure 4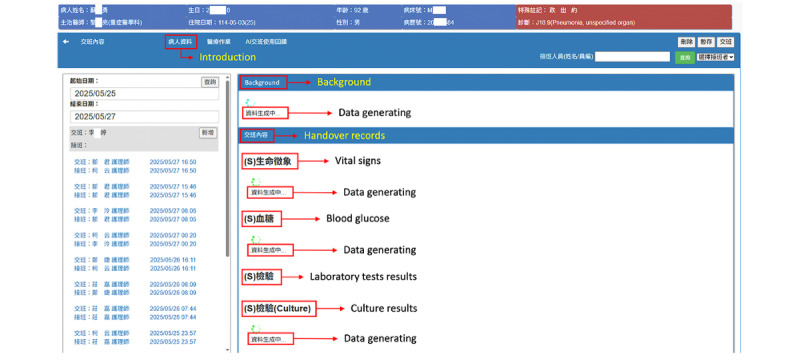 Figure 5
Figure 5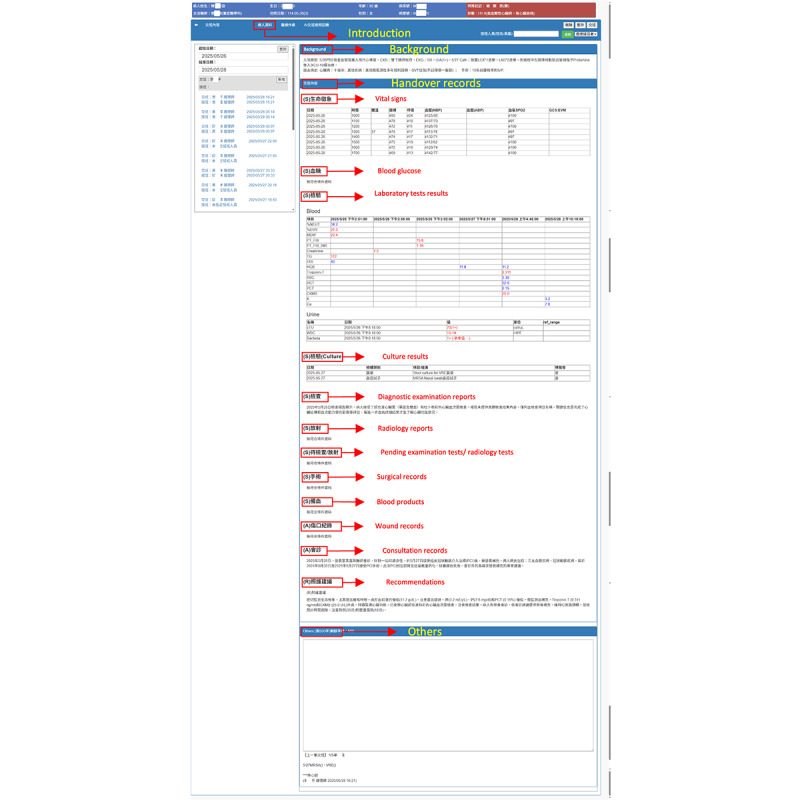 Figure 6
Figure 6| Components | Sections |
| Identity | Introduction |
| Situation | Vital signs, blood glucose, laboratory test results, culture results, diagnostic examination reports, radiology reports, pending diagnostic examination tests or radiology tests, surgical records, and blood products |
| Background | Admission reason, medical history |
| Assessment | Wound records, consultation records |
| Recommendations | A blank field for manual data entry |
| Others | A blank field for manual data entry |
| Components | Sections |
| Identity | Introduction |
| Handover recordsa | Vital signs, blood glucose, laboratory test results, culture results, diagnostic examination reports, radiology reports, pending diagnostic examination tests or radiology tests, surgical records, blood products, wound records, consultation records, and recommendations |
| Background | Admission reason, medical history |
| Others | A blank field for manual data entry |
| Components and sections | Electronic medical record source systems | Tailored prompts | ||
|
|
|
| ||
|
| Introduction | Inpatient system | The nursing information system already provides information (manual data entry is not necessary). | |
|
|
|
| ||
|
| Admission reason and medical history | Inpatient system and medical documentation system | Summarize admission details into a concise paragraph. Highlight the primary reason for admission and include key clinical details. | |
|
|
|
| ||
|
| Vital signs | Nursing information system | Extract and structure the following vital signs data from the past 8 hours from the provided data: date, time, temperature, pulse, respiration, blood pressure, oxygen level, and Glasgow Coma Scale values. Maintain chronological order. | |
| Blood glucose | Laboratory information system | Extract and structure blood glucose readings from the past 8 hours, including date, time, and measurement value. Organize the data in reverse chronological order. | ||
| Laboratory test results | Laboratory information system | Extract the following laboratory results from the past 48 hours: test item, value, and reference range. Mark abnormal values (H for high and L for low), and leave normal values unmarked. Organize the results chronologically and return them in a structured JSON format. | ||
| Culture results | Laboratory information system | Extract and structure key information from culture data within 6 days. For each data sample, identify and output the following fields in a structured format: collection date, specimen type, culture results, and status (completed or pending). | ||
| Diagnostic examination reports | Examination information system | Summarize diagnostic findings from the past 24 hours, emphasizing significant abnormal results in Standard Mandarin. If such findings are unavailable, state “No examination reports available.” | ||
| Radiology reports | Radiology information system | Summarize key radiological findings from the past 24 hours, highlighting clinically relevant abnormalities in Standard Mandarin. If such findings are unavailable, state “No radiology reports available.” | ||
| Pending diagnostic examination tests or radiology tests | Patient schedule system | List upcoming diagnostic and radiology tests in the following format: procedure name and scheduled date. | ||
| Surgical records | Operating room system | Extract the following information from surgical records from the past 48 hours: procedure name, start time, end time, blood loss, and anesthesia method. If no records are available, state “No surgical records available.” | ||
| Blood products | Blood bank system | Extract the following information on blood product orders within 48 hours: order number, blood type and Rha factor, order date, product name, quantity ordered/used, and transfusion date. If such information is unavailable, state “No blood product records available.” | ||
| Wound records | Nursing information system | Extract the following wound assessment data: type, location, assessment date/time, and dimensions. If these data are unavailable, state “No wound assessment records available.” | ||
| Consultation records | Medical documentation system | Summarize consultation findings and recommendations in Standard Mandarin. If such information is unavailable, state “No consultation records available.” | ||
| Recommendations | Blank field | Generate comprehensive nursing care recommendations based on the provided data. Present recommendations as bullet points in only Standard Mandarin. Include information on priority interventions, monitoring requirements, preventive measures, and areas for special attention. | ||
|
|
|
| ||
|
| Others | Blank field for manual data entry | N/Ab | |
| Hospital and shift | September 24 | ||
| Number of shifts, n | Document completion time (minutes), mean (SD) | ||
|
|
|
| |
|
| Day | 12,418 | 4.10 (4.55) |
| Night | 12,203 | 4.32 (4.48) | |
| Overnight | 12,466 | 3.45 (3.82) | |
|
|
|
| |
|
| Day | 9379 | 4.26 (5.08) |
| Night | 10,547 | 3.70 (4.47) | |
| Overnight | 10,909 | 4.10 (5.29) | |
|
|
|
| |
|
| Day | 13,868 | 3.67 (4.31) |
| Night | 14,466 | 4.09 (4.25) | |
| Overnight | 14,201 | 3.81 (4.23) | |
| Hospital and shift | October 24 | November 24 | December 24 | ||||||||||||||||||||||||
| Number of shifts, n | Generative artificial intelligence time (seconds)a, mean (SD) | Manual time (minutes)b, mean (SD) | Document completion time (minutes)c, mean (SD) | Number of shifts, n | Generative artificial intelligence time (seconds), mean (SD) | Manual time (minutes), mean (SD) | Document completion time (minutes), mean (SD) | Number of shifts, n | Generative artificial intelligence time (seconds), mean (SD) | Manual time (minutes), mean (SD) | Document completion time (minutes), mean (SD) | ||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||
|
| Day | 12,043 | 17.0 (20.0) | 1.89 (2.23) | 2.17 (2.56) | 11,882 | 16.70 (19.60) | 1.85 (2.18) | 2.13 (2.50) | 12,510 | 17.00 (19.60) | 1.88 (2.17) | 2.17 (2.50) | ||||||||||||||
| Night | 11,928 | 19.6 (22.1) | 2.18 (2.45) | 2.50 (2.82) | 11,900 | 18.70 (22.10) | 2.08 (2.45) | 2.40 (2.82) | 12,740 | 19.80 (22.10) | 2.20 (2.45) | 2.54 (2.82) | |||||||||||||||
| Overnight | 11,918 | 19.0 (21.6) | 2.11 (2.40) | 2.43 (2.76) | 11,745 | 19.00 (21.60) | 2.11 (2.39) | 2.42 (2.75) | 12,642 | 18.60 (20.80) | 2.07 (2.31) | 2.38 (2.66) | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||
|
| Day | 8291 | 12.1 (17.9) | 1.34 (1.99) | 1.54 (2.29) | 8620 | 13.20 (19.50) | 1.47 (2.17) | 1.68 (2.50) | 8905 | 13.90 (19.80) | 1.55 (2.20) | 1.78 (2.53) | ||||||||||||||
| Night | 9612 | 12.5 (18.7) | 1.39 (2.08) | 1.60 (2.39) | 10,035 | 12.50 (18.70) | 1.38 (2.07) | 1.59 (2.39) | 10,190 | 12.50 (18.60) | 1.39 (2.06) | 1.60 (2.37) | |||||||||||||||
| Overnight | 9597 | 9.2 (14.6) | 1.02 (1.62) | 1.17 (1.86) | 9438 | 10.10 (15.40) | 1.12 (1.72) | 1.28 (1.97) | 9635 | 9.60 (15.10) | 1.07 (1.68) | 1.23 (1.93) | |||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
| |||||||||||||||
|
| Day | 13,103 | 14.8 (20.2) | 1.65 (2.24) | 1.89 (2.58) | 13,931 | 15.40 (20.70) | 1.71 (2.30) | 1.97 (2.65) | 13,875 | 15.30 (20.90) | 1.70 (2.33) | 1.96 (2.67) | ||||||||||||||
| Night | 15,317 | 15.7 (21.3) | 1.74 (2.36) | 2.01 (2.72) | 15,268 | 16.10 (21.50) | 1.79 (2.39) | 2.06 (2.75) | 16,040 | 16.50 (22.00) | 1.84 (2.45) | 2.11 (2.82) | |||||||||||||||
| Overnight | 15,053 | 13.7 (19.6) | 1.52 (2.18) | 1.74 (2.50) | 15,337 | 14.10 (20.60) | 1.57 (2.29) | 1.80 (2.64) | 15,030 | 15.60 (22.40) | 1.74 (2.49) | 2.00 (2.86) | |||||||||||||||
| Outcome | Factor | Wald chi-square statistic ( | |
| Generative artificial intelligence document generation time | Month | 5.74 (2) | .06 |
| Manual timea | Month | 5.74 (2) | .06 |
| Document completion timeb | Month | 5.74 (2) | .06 |
| Generative artificial intelligence document generation time | Shift | 10.39 (2) | .006 |
| Manual time | Shift | 10.39 (2) | .006 |
| Document completion time | Shift | 10.39 (2) | .006 |
| Generative artificial intelligence document generation time | Hospital | 52.85 (2) | <.001 |
| Manual time | Hospital | 52.85 (2) | <.001 |
| Document completion time | Hospital | 52.85 (2) | <.001 |
| Outcome | Factor | β (seconds) | 95% CI | |
| Generative artificial intelligence document generation time | Intercept | 15.09 | 14.26 to 15.92 | <.001 |
| Generative artificial intelligence document generation time | Hospital: TMUHa vs SHHb | 3.05 | 1.80 to 4.31 | <.001 |
| Generative artificial intelligence document generation time | Hospital: WFHc vs SHH | –3.47 | –4.72 to –2.23 | <.001 |
| Manual timed | Intercept | 100.60 | 95.05 to 106.15 | <.001 |
| Manual time | Hospital: TMUH vs SHH | 20.35 | 11.97 to 28.72 | <.001 |
| Manual time | Hospital: WFH vs SHH | –23.16 | –31.45 to –14.88 | <.001 |
| Document completion timee | Intercept | 115.69 | 109.31 to 122.07 | <.001 |
| Document completion time | Hospital: TMUH vs SHH | 23.40 | 13.77 to 33.03 | <.001 |
| Document completion time | Hospital: WFH vs SHH | –26.64 | –36.16 to –17.11 | <.001 |
| Generative artificial intelligence document generation time | Month: December vs October | .56 | 0.09 to 1.04 | .02 |
| Manual time | Month: December vs October | 3.75 | 0.58 to 6.92 | .02 |
| Document completion time | Month: December vs October | 4.31 | 0.66 to 7.95 | .02 |
| Generative artificial intelligence document generation time | Shift: night vs day | 1.05 | –0.24 to 2.34 | .11 |
| Manual time | Shift: night vs day | 6.99 | –1.61 to 15.60 | .11 |
| Document completion time | Shift: night vs day | 8.04 | –1.85 to 17.93 | .11 |
| Generative artificial intelligence document generation time | Month: November vs October | .16 | –0.23 to 0.55 | .41 |
| Manual time | Month: November vs October | 1.09 | –1.50 to 3.69 | .41 |
| Document completion time | Month: November vs October | 1.26 | –1.73 to 4.24 | .41 |
| Generative artificial intelligence document generation time | Shift: overnight vs day | –.69 | –2.45 to 1.07 | .44 |
| Manual time | Shift: overnight vs day | –4.59 | –16.34 to 7.15 | .44 |
| Document completion time | Shift: overnight vs day | –5.28 | –18.79 to 8.22 | .44 |
| Outcome | Factor | β (seconds) | 95% CI | |
| Document completion timea | Intercept | 118.01 | 112.21 to 123.81 | <.001 |
| Document completion time | Preb vs Postc | 63.48 | 53.81 to 73.16 | <.001 |
| Document completion time | Taipei Medical University Hospital vs Shuang Ho Hospital | 19.10 | 10.34 to 27.85 | <.001 |
| Document completion time | Wan Fang Hospital vs Shuang Ho Hospital | –25.67 | –34.42 to –16.92 | <.001 |
| Document completion time | Night vs day | 6.44 | –2.35 to 15.22 | .15 |
| Document completion time | Overnight vs day | –5.98 | –17.99 to 6.03 | .33 |
| Hospital and shift | October 24 | November 24 | December 24 | ||||||||
| Number of documents with revisionsb, n | Number of documentsc, n | Revision rated, % | Number of documents with revisions, n | Number of documents, n | Revision rate, % | Number of documents with revisions, n | Number of documents, n | Revision rate, % | |||
|
|
|
|
|
|
|
|
|
|
| ||
|
| Day | 8164 | 12,043 | 67.79 | 8001 | 11,882 | 67.34 | 8343 | 12,510 | 66.69 | |
| Night | 9162 | 11,928 | 76.81 | 9000 | 11,900 | 75.63 | 9267 | 12,740 | 72.74 | ||
| Overnight | 9551 | 11,918 | 80.14 | 9744 | 11,745 | 82.96 | 10,830 | 12,642 | 85.67 | ||
|
|
|
|
|
|
|
|
|
|
| ||
|
| Day | 4215 | 8291 | 50.84 | 5334 | 8620 | 61.88 | 5562 | 8905 | 62.46 | |
| Night | 7684 | 9612 | 79.94 | 6000 | 10,035 | 59.79 | 6178 | 10,190 | 60.63 | ||
| Overnight | 7804 | 9597 | 81.32 | 6960 | 9438 | 73.74 | 7810 | 9635 | 81.06 | ||
|
|
|
|
|
|
|
|
|
|
| ||
|
| Day | 9717 | 13,103 | 74.16 | 9717 | 13,931 | 69.75 | 9554 | 13,875 | 68.86 | |
| Night | 11,886 | 15,317 | 77.60 | 11,886 | 15,268 | 77.85 | 11,861 | 16,040 | 73.95 | ||
| Overnight | 11,884 | 15,053 | 78.95 | 11,884 | 15,337 | 77.49 | 11,759 | 15,030 | 78.24 | ||
| Hospital | October 24, hours (full-time equivalent)b | November 24, hours (full-time equivalent)b | December 24, hours (full-time equivalent)b | Average, hours (full-time equivalent)b |
| Taipei Medical University Hospital | 113-273 (0.71-1.71) | 115-276 (0.72-1.72) | 117-282 (0.73-1.76) | 115-277 (0.72-1.73) |
| Wan Fang Hospital | 163-307 (1.02-1.92) | 166-314 (1.04-1.96) | 160-302 (1.00-1.89) | 163-308 (1.02-1.92) |
| Shuang Ho Hospital | 198-381 (1.24-2.38) | 203-391 (1.27-2.44) | 201-387 (1.25-2.42) | 201-386 (1.25-2.41) |
| Total | 474-962 (2.96-6.01) | 484-981 (3.02-6.13) | 478-970 (2.99-6.07) | 479-971 (2.99-6.07) |
| Hospital and measure | October 24 | November 24 | December 24 | Overall (October to December) | |
|
|
|
|
|
| |
|
| Allocated generative artificial intelligence cost, US $a | 630.18 | 688.92 | 848.02 | 2167.11 |
| Time saved (hours)b, range | 113-273 | 115-276 | 117-282 | 345-831 | |
| Equivalent labor value (US $10/hour), range | 1130-2730 | 1150-2760 | 1170-2820 | 3450-8310 | |
| Net labor valuec (US $), range | 499.82-2099.82 | 461.08-2071.08 | 321.98-1971.98 | 1282.89-6142.89 | |
|
|
|
|
|
| |
|
| Allocated generative artificial intelligence cost, US $ | 493.14 | 544.74 | 630.12 | 1667.99 |
| Time saved (hours), range | 163-307 | 166-314 | 160-302 | 489-923 | |
| Equivalent labor value (US $10/hour), range | 1630-3070 | 1660-3140 | 1600-3020 | 4890-9230 | |
| Net labor value (US $), range | 1136.86-2576.86 | 1115.26-2595.26 | 969.88-2389.88 | 3222.01-7562.01 | |
|
|
|
|
|
| |
|
| Allocated generative artificial intelligence cost, US $ | 747.75 | 828.36 | 985.75 | 2561.87 |
| Time saved (hours), range | 198-381 | 203-391 | 201-387 | 602-1159 | |
| Equivalent labor value (US $10/hour), range | 1980-3810 | 2030-3910 | 2010-3870 | 6020-11,590 | |
| Net labor value (US $), range | 1232.25-3062.25 | 1201.64-3081.64 | 1024.25-2884.25 | 3458.13-9028.13 | |
|
|
|
|
|
| |
|
| Allocated generative artificial intelligence cost, US $ | 1871.07 | 2062.02 | 2463.89 | 6396.97 |
| Time saved (hours), range | 474-961 | 484-981 | 478-971 | 1436-2913 | |
| Equivalent labor value (US $10/hour), range | 4740-9610 | 4840-9810 | 4780-9710 | 14,360-29,130 | |
| Net labor value (US $), range | 2868.93-7738.93 | 2777.98-7747.98 | 2316.11-7246.11 | 7963.03-22,733.03 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHospital Admissions and Outcomes · Nursing Diagnosis and Documentation · Electronic Health Records Systems
Introduction
The global nursing shortage has been exacerbated by several factors and remains a critical challenge for health care systems, threatening health care quality and access [1,2]. The COVID-19 pandemic has increased nursing workloads, resulting in increased patient acuity, greater infection control demands, and longer working hours—all of which have contributed to nurses experiencing physical exhaustion, moral distress, and mental health challenges [3,4]. Moreover, the pandemic worsened the nursing shortage, with 100,000 nurses leaving the US health care workforce during the pandemic and an additional 900,000 planning to exit by 2027 [5]. This shortage has compromised care quality and increased burnout and turnover risks. According to the World Health Organization (WHO), although the global nursing workforce grew from 27.9 million in 2018 to 29.8 million in 2023, a shortage of 5.8 million nurses persists, which is projected to decrease to 4.1 million by 2030 [6].
Although Taiwan experienced early success in controlling the COVID-19 pandemic, the pandemic exposed structural problems within the country’s nursing sector. Nursing shortages, particularly in intensive care and emergency departments, persisted during the late-pandemic and postpandemic periods. High turnover rates and uneven workloads contributed to increased work-related stress [7]. Furthermore, interviews with public health nurses revealed that frequent changes in temporary assignments and information systems during the pandemic exacerbated fatigue and created additional challenges for frontline nurses [8].
The ongoing digital transformation in health care has rendered digital technologies essential to nursing practice. Studies have indicated that the adoption of digital tools by health care professionals improves care quality, enhances patient participation in their own care [9,10], fosters better coordination among health care professionals [11], reduces medication errors and adverse events [12,13], and improves documentation accuracy [14,15]. However, this shift has led to more time being spent on indirect tasks, particularly activities related to maintaining electronic medical records (EMRs), including data collection, entry, and confirmation [16]. Documentation accounts for a considerable portion of nurses’ work time, and this burden is exacerbated by high patient turnover [17] and the use of multiple recording systems [18,19]. A systematic review revealed that nurses spend between 13% and 31% of their work time on documentation [20]; thus, considering nurses’ heavy workloads, reducing documentation time has become a critical issue in nursing.
Large language models (LLMs), a category of artificial intelligence (AI) tools, perform deep learning with millions or billions of parameters on extensive data to generate human-like text [21]. LLM platforms, such as ChatGPT (OpenAI), Gemini (Google LLC), and Llama (Meta Platforms, Inc.) [22,23], are applied in various domains, including text generation, question answering, translation, and creative content creation. Moreover, large multimodal models have been developed to process several types of data, such as text, images, video, and audio, thereby broadening the application potential of generative AI (GenAI) tools [24,25]. In health care, LLMs and other GenAI tools enable coherent text generation for tasks such as drug discovery, personalized medicine, radiology diagnosis, automated clinical documentation, medical research, and health information consultation [26-34]. These tools are driving advancements in diverse health care applications; however, ensuring the accuracy, reliability, and fairness of the generated results remains critical [35].
AI applications in nursing are rapidly expanding, and AI tools have the potential to become essential parts of nursing practice [36,37]. By integrating clinical data with language generation tools, GenAI systems can improve documentation quality, support clinical decision-making, and reduce administrative workload. Additionally, these systems can considerably shorten documentation time and enhance handover efficiency by rapidly producing consistent records, thereby allowing nurses to devote more time to patient care and ultimately improving the quality and safety of health care delivery [38,39].
To explore the potential of incorporating LLMs into electronic nursing documentation systems, this study integrated an LLM into an in-house nursing information system (NIS) to reduce the time and effort required for nursing handover documentation. We evaluated the LLM-integrated NIS by comparing the time spent by nurses on nursing handover documentation before and after integration. We additionally conducted a preliminary cost-effectiveness assessment and quantified the revision rate of GenAI-generated drafts before final submission.
Methods
Settings
This study was conducted at Taipei Medical University (TMU), which operates 3 hospitals: Taipei Medical University Hospital (TMUH), Wan Fang Hospital (WFH), and Shuang Ho Hospital (SHH). The combined capacity of these hospitals is 2675 acute beds (TMUH: 735; WFH: 761; SHH: 1179), and they handle a total of over 400,000 outpatient visits per month. Owing to nursing shortages, operational capacity decreased to 2195 acute beds as of May 2025 (TMUH: 608; WFH: 576; SHH: 1011). Nursing workflows are supported by an in-house NIS managed by the TMU Center of Digital Innovation and Development.
Google Gemini
We selected a HIPAA (Health Insurance Portability and Accountability Act)-compliant enterprise instance of Gemini 1.5 Pro (Google LLC) for integration into the in-house NIS. Gemini 1.5 Pro is a mid-sized multimodal LLM optimized for a broad range of reasoning tasks and can generate text output in response to diverse inputs, including text, image, video, and audio. Moreover, it offers capabilities for output streaming, conversational interactions, and system-level instruction handling. The model can be used to conduct various language-related tasks, such as text generation, text editing, code generation, problem-solving, recommendation generation, information extraction, and data generation [40].
Conventional Workflow in Nursing Handover Documentation
In hospitals across Taiwan, nursing schedules are typically structured around 3 daily shifts, and nurses are required to complete handover documentation twice per day. The nursing handover document follows the WHO-endorsed ISBAR (Identify, Situation, Background, Assessment, Recommendation) framework structured into 5 key components [41].
Figure 1 illustrates the conventional workflow for nursing handover documentation with the in-house NIS. Initially, the NIS displays a list of patients requiring handover documentation. Subsequently, nurses collect and analyze individualized patient information using various EMR systems. They then sequentially write a nursing handover document for each patient. Finally, the documented handover information is manually summarized to formulate the corresponding nursing recommendations for each patient.
In general, nurses prepare handover documents for 5-7 patients per shift, and senior nurses estimated an average completion time of approximately 5 minutes per patient. Accordingly, each nurse dedicates approximately 1 hour to complete patient handover tasks; this time frame includes both the documentation process and the subsequent verification and explanation of patient details to the receiving nurse.
Conventional workflow for nursing handover documentation using the in-house nursing information system (NIS) at Taipei Medical University. EMR: electronic medical record.
Prompt Design for Nursing Handover Documentation
A multidisciplinary team of nursing specialists and information technology professionals collaboratively outlined the key components of the nursing handover document, as defined in the existing EMR systems. Each component was divided into several sections, which were systematically evaluated to assess the extracted content and identify potential problems. The most critical problem identified was related to the manual collection, verification, transcription, and integration of patient data from various EMR systems. Thus, we reorganized the structure of the nursing handover document. Tables 1 and 2, respectively, present the sections of the original and revised (for the LLM-integrated NIS) nursing handover documents across 5 key components according to the ISBAR framework.
We developed section-specific prompts to support nurses’ use of the LLM, targeting 4 tasks: (1) extracting information from the provided input, (2) summarizing input text, (3) interpreting or translating text (eg, English to Mandarin), and (4) formatting content based on the input. When executed, these prompts generate draft content for the corresponding handover sections. Prompt development followed an iterative, human-in-the-loop process: draft prompts were repeatedly tested using deidentified EMRs, and outputs were reviewed by nursing professionals for clinical relevance, completeness, and adherence to the intended structure. Feedback-informed refinements were made to prompt wording, section constraints, and output formatting until the drafts were suitable for routine handover use. All prompts instructed the LLM to use only the provided input and to avoid introducing new values, assumptions, or inferences. No patient identifiers or personally identifiable information was transmitted to the LLM.
For example, in the laboratory results section, the NIS queried the laboratory information system to retrieve each patient’s test results and corresponding reference ranges from the preceding 48 hours. A tailored prompt was then sent via the LLM application programming interface (API) to identify abnormal results by comparing values with reference ranges and to present the extracted abnormalities in a structured table. Table 3 summarizes the tailored prompts by section and the corresponding EMR source systems, including the inpatient system, medical documentation system, NIS, laboratory information system, examination information system, radiology information system, patient schedule system, operating room system, and blood bank system.
Interactions Between the NIS and the LLM in the Designed Workflow for Nursing Handover Documentation
Google Gemini 1.5 Pro offers an API that provides access to its LLM, which was integrated into the in-house NIS to automatically generate nursing handover documents.
Figure 2 illustrates the integrated workflow of the LLM-integrated NIS. For each section of the nursing handover document, the NIS sends a request to the relevant EMR system to retrieve patient data through asynchronous calls. The retrieved data and the corresponding tailored prompt are then used as input to call the LLM API. Upon receiving the LLM response, the NIS organizes the content and formats it according to the appropriate style for each section. The final output generated by the NIS is a structured and comprehensive handover document that can be manually reviewed and validated by nursing staff.
Integrated workflow for the large language model (LLM)–integrated nursing information system (NIS). API: application programming interface; EMR: electronic medical record.
Log Data Collection and Analysis of the Nursing Handover Document in the NIS
In this study, log data from the LLM-integrated NIS, implemented in October 2024, were used to conduct a preliminary pre-post comparison of nursing handover document completion times. Handover document completion time was defined as the interval from when a nurse selected a patient by clicking the handover button, through manual entry before GenAI integration or automatic draft generation after integration, to final confirmation, when the nurse completed review and revision and clicked the “Confirm” button for that patient.
To support subsequent analyses and system optimization, step-level log data were collected across the full handover documentation workflow. We retrospectively extracted NIS logs from September 2024 (preintegration) and from October-December 2024 (postintegration) for the 3 TMU-managed hospitals. To reduce the influence of extreme values, log data with handover document completion times exceeding 20 minutes were excluded from the analyses. In addition, we logged both the automatically GenAI-generated handover draft and the final nurse-confirmed version to preliminarily quantify the document revision rate. As nurse identifiers were unavailable, we used hospital × shift as the clustering unit and applied robust (sandwich) SEs to account for within-cluster correlation.
Ethical Considerations
This retrospective study of deidentified NIS logs was approved by the TMU-Joint Institutional Review Board (TMU-JIRB; approval number N202506094). All data were deidentified to protect participant privacy and confidentiality, and no personally identifiable information was collected or disclosed. The TMU-JIRB waived the requirement for informed consent. All images included in the manuscript were reviewed to ensure that no individual participants or users could be identified. The hospitals also conduct routine qualitative and quantitative medical record audits, providing organizational accountability and quality assurance for AI-assisted documentation.
Results
Descriptive Statistics of Nursing-Related Factors for the Examined Hospitals
From September 1 to December 31, 2024, we collected NIS log data from the 3 hospitals during daily nursing handovers across 3 shifts (day, night, and overnight). At TMU, nursing handover documents must be prepared for most inpatients; however, certain patient categories are exempt from this requirement. These categories include patients undergoing postoperative observation, day hospitalization, and 1-day chemotherapy at TMUH; nursing home residents and day-care patients at WFH; and day-care, psychiatric ward, nursing home, and postpartum home care patients at SHH.
During the 4-month study period, the number of nurses working across the 3 daily shifts ranged from 501 to 524 at TMUH, 468 to 489 at WFH, and 862 to 892 at SHH. Monthly inpatient case volumes ranged from 7477 to 7733 at TMUH, 5406 to 5977 at WFH, and 8872 to 9814 at SHH. The mean monthly length of stay was 4.7-4.9 days at TMUH, 4.7-5.1 days at WFH, and 4.9-5.0 days at SHH. Across all shifts, total monthly shift counts ranged from 35,527 to 37,892 at TMUH, 27,500 to 30,835 at WFH, and 42,535 to 44,945 at SHH. Multimedia Appendix 1 summarizes descriptive statistics for the 3 hospitals included in this study.
Comparison of the Original and GenAI-Assisted Nursing Handover Documentation Functions in the NIS
In accordance with the workflow shown in Figure 1, the LLM-integrated NIS initially displays a table listing patients, enabling nurses to generate handover documents sequentially by clicking a selection checkbox (Figure 3). Each row presents key patient attributes, including the patient’s name, medical record number, bed number, birth date and age, admission date and length of stay, department, and attending physician. The table also includes a handover button to initiate the nursing handover process.
Figure 4 depicts the nursing handover documentation interface in the original NIS, displayed when a nurse selects a patient and initiates the handover process. Nurses complete 5 handover sections: Introduction (auto-populated; no manual entry required), Situation, Background, Assessment, and Recommendation and Other information.
Figure 5 depicts the revised nursing handover document in the LLM-integrated NIS. In contrast to the original NIS, selecting a patient for handover triggers an API call to the LLM. After the response is returned, the LLM-integrated NIS automatically populates draft content for each handover section. Nurses then review, revise, and confirm the draft. Once finalized, the nurse clicks “Confirm” to submit the handover document for that patient (Figure 6).
Screenshot of the patient list interface used by nurses to perform handover tasks in the nursing information system.
Screenshot of the Identify, Situation, Background, Assessment, Recommendation interface used for nursing handover tasks in the original nursing information system.
Screenshot of the revised nursing handover document in the large language model–integrated nursing information system.
Screenshot of a complete nursing handover document automatically generated by the large language model–integrated nursing information system.
Analysis of NIS Log Data for Pre-LLM Integration
Table 4 presents detailed NIS log data from September 2024 for TMUH, WFH, and SHH, including the number of shifts and the mean (SD) of handover document completion time per patient for each shift. Before LLM integration, nurses often had to pause documentation to gather additional patient information or respond to unplanned clinical events (eg, bedside care, family inquiries, or urgent clinical duties). Accordingly, the NIS included a draft-save function that allowed handover content to be temporarily stored and completed later.
A total of 110,457 shift-level handover logs were analyzed (TMUH: 37,087; WFH: 30,835; and SHH: 42,535), representing large-scale real-world clinical operations. Across hospitals and shifts, the mean handover document completion time per patient ranged from 3.45 (SD 3.82) to 4.32 (SD 4.48) minutes. At TMUH, mean completion times were 4.10 (SD 4.55) minutes (day shift), 4.32 (SD 4.48) minutes (night shift), and 3.45 (SD 3.82) minutes (overnight shift). At WFH, the corresponding values were 4.26 (SD 5.08), 3.70 (SD 4.47), and 4.10 (SD 5.29) minutes, respectively, whereas at SHH they were 3.67 (SD 4.31), 4.09 (SD 4.25), and 3.81 (SD 4.23) minutes, respectively.
Although only 1 month of preintegration log data were available, these results provide a preliminary baseline of nursing handover documentation performance against which the impact of subsequent GenAI-assisted workflows can be quantitatively evaluated.
Analysis of NIS Log Data for LLM Responses
Table 5 summarizes shift-level log data from October to December 2024 for TMUH, WFH, and SHH, including the number of shifts, mean GenAI document generation time per patient, mean nurse manual (review-revision-confirmation) time per patient, and mean overall document completion time per patient. SHH had the highest shift volume (43,473 in October to 44,945 in December) and the largest monthly patient volume (8872-8989; Multimedia Appendix 1), with mean overall completion times ranging from 1.74 (SD 2.5) to 2.11 (SD 2.82) minutes. WFH recorded the lowest shift volume (27,500-28,730) and the shortest mean overall completion times (mean 1.17, SD 1.86 minutes to mean 1.78, SD 2.53 minutes) while managing 5746-5977 patients per month (Multimedia Appendix 1). TMUH showed intermediate shift volume (35,890-37,892) and patient volume (7477-7733; Multimedia Appendix 1), with mean overall completion times of 2.13 (SD 2.5) to 2.54 (SD 2.82) minutes.
We further conducted analyses using joint Wald tests to assess whether hospital, shift, and month were associated with statistically significant differences. As individual nurse identifiers were not available in the log data, clustering at the nurse level was not feasible. Therefore, we defined the clustering unit as hospital × shift, and the corresponding results are presented in Table 6.
In Table 6, joint Wald tests indicated that all 3 outcomes (GenAI time, manual time, and document completion time) differed significantly across hospitals and shifts (hospital: Wald χ^2^2=52.85, P<.001; shift: Wald χ^2^2=10.39, P=.006). By contrast, the effect of month was not statistically significant (Wald χ^2^2=5.74, P=.057).
Moreover, we used generalized estimating equations (GEEs) to account for within-cluster correlation arising from the clustered and longitudinal structure of the data. Separate GEE models were fitted for GenAI time, manual time, and document completion time. Each model included month, shift, and hospital as categorical covariates and used an exchangeable working correlation structure with robust SEs; thus, estimates represent population-averaged (system-level) effects rather than individual-level effects. Table 7 reports the population-averaged GEE results for GenAI time, manual time, and document completion time (β and SE). Relative to SHH, TMUH had longer times across all outcomes (GenAI time: β=3.05; manual time: β=20.35; document completion time: β=23.40; all P<.001), whereas WFH had shorter times (GenAI time: β=−3.47; manual time: β=−23.16; document completion time: β=−26.64; all P<.001). December (vs October) was associated with small increases across outcomes (P=.02), whereas November (vs October; P=.41) and shift (P=.44) were not statistically significant.
Comparison of NIS Log Data Before and After LLM Integration
Using NIS logs from the preintegration period (September 2024) and the postintegration period (October-December 2024), we compared handover document completion time. Table 8 reports population-averaged GEE estimates for document completion time (seconds). Document completion time was significantly longer preintegration than postintegration (β=63.48 seconds; 95% CI 53.81-73.16; P<.001), and the overall period effect was significant (χ^2^1=165.24; P<.001). Relative to SHH, completion time was longer at TMUH (β=19.10 seconds; 95% CI 10.34-27.85; P<.001) and shorter at WFH (β=−25.67 seconds; 95% CI −34.42 to −16.92; P<.001). Shift effects were not statistically significant (night vs day, P=.15; overnight vs day, P=.33).
Revision Rate of GenAI-Generated Handover Drafts
Using NIS logs from October to December 2024, we examined revisions of GenAI-generated handover drafts by hospital and shift. Table 9 presents, for each hospital-shift stratum, the number of patient-level handover documents in which nurses revised the GenAI-generated draft (number of documents with revisions), the total number of patient-level handover documents (number of documents), and the corresponding revision rate (number of documents with revisions/number of documents, %).
Revisions were common across hospitals and months. At TMUH, revision rates were higher during night (9267/12,740-9162/11,928, 72.74%-76.81%) and overnight shifts (9551/11,918-10,830/12,642, 80.14%-85.67%) than during day shifts (8343/12,510-8164/12,043, 66.69%-67.79%). At WFH, day-shift revision rates increased from nearly 50% (4215/8291, 50.84%) in October to over 60% (5334/8620-5562/8905, 61.88%-62.46%) in November-December, whereas night-shift revision rates decreased from nearly 79% (7684/9612, 79.94%) in October to nearly 60% (6000/10,035-6178/10,190, 59.79%-60.63%) thereafter; overnight-shift revision rates remained high (6960/9438-7804/9597, 73.74%-81.32%). At SHH, revision rates were relatively stable, with day shifts at 68.86%-74.16% (9554/13,875-9717/13,103) and night and overnight shifts at 73.95%-78.95% (11,861/16,040-11,884/15,053).
Estimated Time Savings in Handover Documentation Before and After LLM Integration
Nurses at TMUH, WFH, and SHH estimated that they typically completed handover documentation for 5-7 patients per shift when using the original NIS. Based on the available preintegration logs (limited to 1 month), the average documentation completion time ranged from 3.45 (SD 3.82) to 4.32 (SD 4.48) minutes per patient across hospitals and shifts (Table 4). Postintegration logs from October to December 2024 (Table 5) further characterized workflow performance by decomposing document completion time into GenAI generation time and nurse review-revision-confirmation time; the average overall completion time per patient ranged from 1.17 (SD 1.86) to 2.54 (SD 2.82) minutes. Taken together, these figures suggest a potential absolute reduction of approximately 0.91-3.15 minutes per patient ([3.45-2.54]/3.45-[4.32-1.17]/4.32, 26%-73% relative reduction). Moreover, using monthly patient volumes and the observed reduction in per-patient completion time, the LLM-integrated workflow corresponds to estimated savings of approximately 470-980 hours per month across the 3 hospitals (Table 10). Full-time equivalent (FTE) is a standard unit used to express workload or staffing capacity as the work time of 1 full-time worker over a specified period. FTE equivalents were calculated assuming 160 nursing work hours per FTE-month. At TMUH, the projected reduction was approximately 113-282 hours per month (equivalent to 0.7-1.8 FTE/month, assuming 160 working hours per FTE). At WFH, the estimated savings were approximately 160-314 hours per month (1.0-2.0 FTE/month). At SHH, which had the highest patient volume, the estimated savings were approximately 198-387 hours per month (1.2-2.4 FTE/month).
Cost-Effectiveness of GenAI-Assisted Handover Documentation
Preliminary GenAI token cost-effectiveness was evaluated by comparing GenAI operating expenditures with estimated nursing time savings (Table 11). Monthly patient volume was used to approximate documentation time saved, and nursing time was valued at US 493-US 322 to US 970 to US 1024 to US 4740-US 1871-US 2276-US 6396.97, with an estimated 1436-2913 hours saved, yielding an overall net labor value of US 22,733.
Discussion
Principal Findings
In this study, we integrated Google Gemini 1.5 Pro into the in-house NIS of TMU Health to improve the efficiency of nursing handover documentation across 3 hospitals in Taiwan. In the LLM-integrated workflow, a nurse initiates handover by selecting a patient, after which the LLM-integrated NIS retrieves relevant patient data and submits section-specific, tailored prompts to the LLM. The LLM generates draft content for each handover section, and the compiled document is returned to the LLM-integrated NIS for nurse review, revision, and finalization. This integration streamlines handover documentation by reducing manual data entry and supporting a more efficient routine workflow.
The LLM-integrated NIS retains the functionalities of the original in-house NIS, thereby enabling seamless incorporation of the LLM into the existing nursing handover documentation workflow. Nurses remain familiar with the system interfaces, obviating the need for adaptation and minimizing challenges related to digital skills training and system usability. Furthermore, nurses can readily interact with the LLM-integrated NIS and access the generated content, ensuring that the system does not interrupt workflow [42,43]. Consequently, nurses can maintain their focus on patient care while benefiting from the time-saving features of the LLM, ultimately improving both clinical and operational outcomes.
Across 3 TMU Health hospitals, postintegration NIS logs showed shorter per-patient handover documentation completion times than the limited 1-month preintegration baseline, corresponding to an estimated reduction of 0.91-3.15 minutes per patient ([3.45-2.54]/3.45-[4.32-1.17]/4.32, 26%-73%). When scaled by monthly patient volumes (Table 10), this reduction translated to approximately 470-980 hours saved per month across hospitals (approximately 0.7-1.8 FTE/month, assuming 160 working hours per FTE). A preliminary token cost evaluation suggested that GenAI operating expenditures (US 986 per hospital per month) were modest relative to the estimated labor or opportunity value of nursing time freed for clinical work, yielding a positive net labor value across October-December 2024 (Table 11). Overall, these findings suggest that GenAI-assisted handover documentation may reduce documentation burden and return clinically meaningful nursing time that could be redirected to direct patient care, which is particularly relevant in the context of nursing workforce shortages.
Safety Considerations and Hallucination Mitigation
Hallucinations are a well-recognized limitation of GenAI, particularly in clinical documentation tasks in which factual accuracy is critical [44-46]. During initial development and testing of the LLM-integrated NIS, we observed occasional hallucinations when the LLM was used to extract and structure vital signs from NIS inputs; for example, the model sometimes generated an average body temperature that was not explicitly documented in the source record. To mitigate hallucination risk, we implemented multiple safeguards. First, we iteratively refined prompts to restrict the LLM to reformatting and summarizing only the provided input and to prohibit the introduction of new values or inferences. Second, we required nurse review, correction, and confirmation before finalizing each handover note, thereby adding an additional verification layer. Despite these measures, we considered the residual risk of LLM-generated structured vital-sign outputs to be clinically unacceptable. Accordingly, we discontinued LLM-based structuring of vital signs and instead directly displayed the patient’s vital signs in the NIS. By contrast, the LLM appeared more reliable for extracting and synthesizing narrative information (eg, abnormal findings and clinically relevant descriptions) from radiology and examination reports, in which the task emphasized highlighting salient text rather than generating or imputing numeric values.
Limitations
First, only 1 month of preintegration log data were available, limiting the robustness of the baseline for manual handover documentation and constraining pre-post comparisons. Accordingly, the preintegration results should be interpreted as a preliminary benchmark for estimating the potential impact of subsequent GenAI-assisted workflows. Second, the NIS log schema was not sufficiently granular to support several secondary analyses. Specifically, we could not quantify technical reliability indicators (eg, connection failures, API time-outs, error returns, failed generations, or regeneration attempts), nor could we stratify performance by patient complexity (eg, intensive care unit vs general ward) or clinical acuity proxies such as length of stay. Consequently, the reported time and cost estimates reflect system-level averages and may mask heterogeneity in performance for complex cases or under high-load conditions. Third, we did not conduct a formal natural language processing evaluation of generated text quality using standard metrics or a gold-standard reference set [47,48]. Although nursing professionals reviewed and verified the LLM-generated handover content as part of routine workflow, the absence of quantitative natural language processing evaluation limits comparability with prior summarization studies and precludes objective assessment of section-level content fidelity. Fourth, although we quantified the revision rate of GenAI-generated drafts, we did not classify edit types (eg, corrections vs clarifications vs additions) or examine the reasons underlying nurse modifications. Therefore, we could not determine which content areas most frequently required changes or whether revisions primarily reflected model limitations, workflow preferences, or patient- and context-specific factors. Fifth, we did not conduct a formal usability or user experience evaluation. Specifically, we did not administer validated instruments (eg, the System Usability Scale or Technology Acceptance Model) or conduct structured interviews to assess nurses’ perceived workload, trust in GenAI outputs, or overall satisfaction, limiting conclusions about user acceptability beyond log-based performance metrics.
Future Directions
Our preliminary findings suggest that LLMs can support rapid, automated generation of nursing handover documents; however, nurse review and revision remain necessary before finalization. First, future work will expand the NIS logging framework to capture reliability and workflow metrics (eg, time-outs, error codes, retries, regeneration events, and editing behaviors) and enable more granular performance evaluation, including downstream operational outcomes such as nursing overtime hours. Second, we will compare LLM-generated drafts with nurse-finalized handovers to characterize error patterns, quantify revision types, and inform iterative prompt and model refinement. These analyses will be guided by predefined quality indicators and evaluation frameworks (eg, quantitative and qualitative ISBAR-based assessments) in future studies. Collectively, these data will support improvements in factual accuracy and the development of additional safeguards, including rule-based checks and retrieval-augmented generation strategies [49]. Third, to evaluate usability and acceptance, we will incorporate standardized instruments and structured qualitative feedback to assess nurse-perceived usability, trust, cognitive load, and workflow impact alongside log-derived efficiency outcomes. Fourth, to improve transferability, we will evaluate interoperability in settings with different EMR architectures and develop a configurable prompt-and-template layer (eg, leveraging HL7/FHIR [Health Level 7/Fast Healthcare Interoperability Resources] where available) to reduce site-specific customization. Specifically, we aim to reduce institution-specific effort related to data mapping; integration with source systems (eg, laboratory information system/radiology information system/examination information system); authentication and authorization; local handover templates and documentation policies; and network or operational configurations. In parallel, we will preserve and further validate transferable components, including ISBAR-aligned section prompts, the human-in-the-loop workflow (draft generation with nurse review-revision-confirmation), safety safeguards (eg, prompt constraints and use of source-of-truth structured data), and a log-based evaluation framework for efficiency, revision behavior, and reliability metrics. Finally, we will assess generalizability to other clinical documentation workflows, including automated note drafting and radiology report generation.
Conclusions
In this study, we integrated an LLM into an existing NIS to generate nursing handover documents in routine practice without modifying the user interface or disrupting established workflows. Across 3 hospitals within TMU Health, GenAI-assisted handover documentation was associated with reduced per-patient documentation completion time in real-world use. A preliminary cost-effectiveness analysis suggested that GenAI operating expenditures were modest relative to the estimated labor value of nursing time freed for clinical work from October to December 2024. To mitigate hallucination risk, particularly for structured numeric data, we constrained prompts and embedded nurse review, editing, and confirmation within the workflow. Overall, these findings support the operational feasibility of integrating GenAI into hospital documentation workflows while retaining human verification. Future work will expand NIS logging to quantify reliability and editing metrics, compare LLM-generated drafts with nurse-finalized documents to identify error patterns and inform prompt and model refinement, and evaluate interoperability and generalizability to other clinical documentation tasks.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Oulton JA The global nursing shortage: an overview of issues and actions Policy Polit Nurs Pract 20060873 Suppl 34S 39S 10.1177/1527154406293968170716937/3_suppl/34S 17071693 · doi ↗ · pubmed ↗
- 2MarćM Bartosiewicz A Burzyńska J Chmiel Z Januszewicz PA nursing shortage - a prospect of global and local policies Int Nurs Rev 20190366191610.1111/inr.124733003984930039849 · doi ↗ · pubmed ↗
- 3Qureshi SM Bookey-Bassett S Purdy N Greig MA Kelly H Neumann WP Modelling the impacts of COVID-19 on nurse workload and quality of care using process simulation P Lo S One 20221710 e 0275890 10.1371/journal.pone.027589036228015 PONE-D-21-3072436228015 PMC 9560613 · doi ↗ · pubmed ↗
- 4Ribeiro OMPL Coimbra VMO Pereira SCDA Faria ADCA Teles PJFC Rocha CGD Impact of COVID-19 on the environments of professional nursing practice and nurses' job satisfaction Int J Environ Res Public Health 202212161924 ijerph 192416908 10.3390/ijerph 19241690836554789 ijerph 192416908 PMC 977954136554789 · doi ↗ · pubmed ↗
- 5NCSBN research projects significant nursing workforce shortages and crisis National Council of State Boards of Nursing 2026-01-26 https://www.ncsbn.org/news/ncsbn-research-projects-significant-nursing-workforce-shortages-and-crisis
- 6State of the world's nursing report 2025: investing in education, jobs, leadership and service delivery World Health Organization 2026-01-26 https://www.who.int/publications/i/item/9789240110236
- 7Liao Z Sun S Clarissa C Aviles L Lin C Kao CT Shih Y Lo Y Chen LA Exploring the challenges of Taiwanese nurses in the COVID-19 post-pandemic era J Formos Med Assoc 202411123 Suppl 3S 215S 222 10.1016/j.jfma.2024.03.02038570237 S 0929-6646(24)00181-538570237 · doi ↗ · pubmed ↗
- 8Wu F Sun J Wu H Su M Lin C The experiences of public health nurses during the COVID-19 in Taiwan: a qualitative study Nurs Open 202401111 e 2091 10.1002/nop 2.20913826827838268278 PMC 10784424 · doi ↗ · pubmed ↗