Latissimus dorsi flap: a comprehensive systematic review of traditional and novel applications
María García-García, Belén Andresen-Lorca, Alessandro Thione, Pedro Alvedro-Ruiz, Arantxa Blasco-Serra, Eva M. González-Soler, Alfonso A. Valverde-Navarro

TL;DR
This paper reviews the traditional and new uses of the latissimus dorsi flap in reconstructive surgery, highlighting its versatility and evolving applications.
Contribution
The paper provides a comprehensive, indication-based synthesis of both traditional and emerging uses of the latissimus dorsi flap.
Findings
The LD flap is used for both coverage and functional reconstructions in multiple anatomical regions.
Functional applications include facial reanimation, limb motor restoration, and urologic reconstruction.
Free LD flaps are preferred for distant or complex reconstructions, while pedicled flaps are used for adjacent defects.
Abstract
The latissimus dorsi (LD) flap is among the most adaptable and extensively employed techniques in reconstructive surgery, providing a dependable solution for addressing a wide range of defects. Although traditionally employed for soft-tissue coverage, its indications have progressively expanded to include complex and functional reconstructions. The aim of this review was to provide a comprehensive, indication-based overview of both traditional and emerging applications of the LD flap reported in the literature. A systematic review was conducted in accordance with PRISMA guidelines, analysing published applications of the LD flap in reconstructive surgery. An initial search was performed up to July 30, 2024, and subsequently updated during manuscript revision to include studies published through January 10, 2026. Two independent reviewers examined the selected articles, individually…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
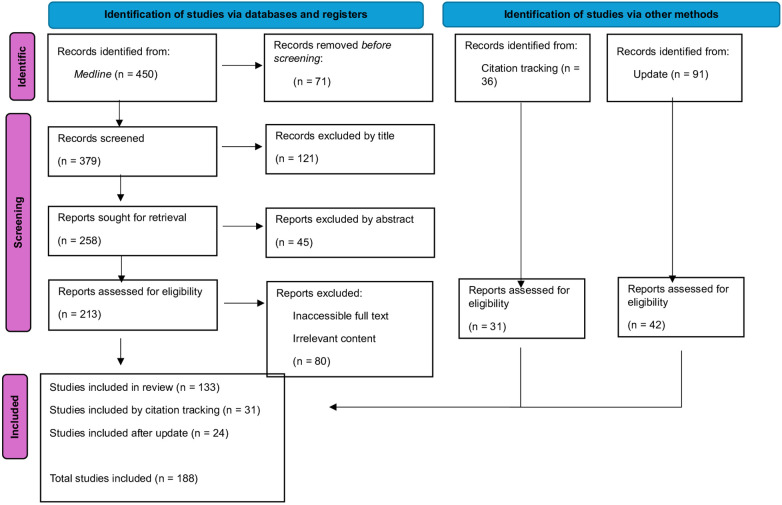 Figure 1
Figure 1| Author | Study design | Year of publication | Sample ( |
|---|---|---|---|
| Bianchi et al. ( | Case series | 1983 | 3 |
| Sabatier et al. ( | Case series | 1992 | 63 |
| Zimmermann et al. ( | Case report | 1993 | 1 |
| Yap et al. ( | Case report | 1994 | 1 |
| Papadopoulos et al. ( | Case series | 1994 | 12 |
| Allen et al. ( | Case series | 1994 | 12 |
| Bootz et al. ( | Case series | 1995 | 7 |
| Wallace and Roden ( | Case series | 1995 | 5 |
| Whetzel et al. ( | Case report | 1997 | 1 |
| Schultes et al. ( | Case report | 1998 | 1 |
| Park and Koh ( | Case report | 1998 | 1 |
| Bedini et al. ( | Case series | 2000 | 9 |
| Ihara et al. ( | Case series | 2000 | 12 |
| Dixon et al. ( | Case series | 2002 | 25 |
| Meiners ( | Case report | 2003 | 1 |
| De Smet et al. ( | Case report | 2004 | 1 |
| Germann et al. ( | Case report | 2006 | 1 |
| McConkey et al. ( | Case report | 2006 | 1 |
| Djordjevic et al. ( | Case series | 2006 | 30 |
| Perovic et al. ( | Case series | 2007 | 16 |
| Hierner et al. ( | Case series | 2009 | 14 |
| Gakis et al. ( | Case series | 2011 | 11 |
| Ozer et al. ( | Case report | 2011 | 1 |
| Phan et al. ( | Case series | 2011 | 8 |
| He et al. ( | Case series | 2012 | 11 |
| Kim et al. ( | Case series | 2012 | 20 |
| Kim et al. ( | Case report | 2012 | 1 |
| Gangurde et al. ( | Case series | 2012 | 3 |
| Qu et al. ( | Case series | 2012 | 6 |
| Nazerani et al. ( | Case series | 2012 | 7 |
| Hwang et al. ( | Case report | 2012 | 1 |
| Venkatramani et al. ( | Case series | 2013 | 19 |
| Biglioli et al. ( | Case series | 2013 | 17 |
| Karle et al. ( | Case series | 2013 | 3 |
| Tsai et al. ( | Case report | 2013 | 1 |
| Takushima et al. ( | Case series | 2013 | 351 |
| Patel et al. ( | Case report | 2014 | 1 |
| Trimaille et al. ( | Case report | 2014 | 1 |
| Vibhakar et al. ( | Case report | 2014 | 1 |
| Endara et al. ( | Case report | 2014 | 1 |
| Fujioka et al. ( | Case report | 2014 | 1 |
| Muramatsu et al. ( | Case series | 2014 | 4 |
| Hornez et al. ( | Case report | 2014 | 1 |
| Kim et al. ( | Case report | 2014 | 7 |
| Santanelli di Pompeo et al. ( | Case series | 2014 | 23 |
| Hillerup et al. ( | Case series | 2014 | 15 |
| Wilkman et al. ( | Case series | 2014 | 10 |
| Wormald et al. ( | Case series | 2014 | 15 |
| Horta et al. ( | Case report | 2015 | 1 |
| Okazaki et al. ( | Case series | 2015 | 4 |
| Gilleard et al. ( | Case report | 2015 | 1 |
| Tuncer et al. ( | Case report | 2015 | 1 |
| Cigna et al. ( | Case report | 2015 | 1 |
| Højvig y Bonde ( | Case series | 2015 | 135 |
| Jain et al. ( | Case report | 2015 | 1 |
| Kaur et al. ( | Case series | 2015 | 19 |
| Kesiktas et al. ( | Case series | 2015 | 12 |
| Longo et al. ( | Case series | 2015 | 5 |
| Miyamoto et al. ( | Case series | 2015 | 5 |
| Singh et al. ( | Case series | 2015 | 2 |
| Tan et al. ( | Case series | 2015 | 2 |
| Angrigiani et al. ( | Case series | 2015 | 45 |
| Bach et al. ( | Case series | 2015 | 7 |
| Nicoli et al. ( | Case report | 2016 | 1 |
| Rednam and Rinker ( | Case report | 2016 | 1 |
| Buchanan et al. ( | Case report | 2016 | 1 |
| Banys-Paluchowski et al. ( | Case report | 2016 | 1 |
| He et al. ( | Case series | 2016 | 12 |
| Ng et al. ( | Case report | 2016 | 1 |
| Amin et al. ( | Case report | 2016 | 1 |
| Bodin et al. ( | Case report | 2016 | 1 |
| Cadenelli et al. ( | Case report | 2016 | 1 |
| Ozcan Akcal et al. ( | Case series | 2016 | 2 |
| Correia Anacleto et al. ( | Case series | 2016 | 100 |
| Gao et al. ( | Case series | 2016 | 16 |
| Gencel et al. ( | Case series | 2016 | 6 |
| Hwang et al. ( | Case series | 2016 | 23 |
| Lü et al. ( | Case series | 2016 | 15 |
| Mutlu et al. ( | Case report | 2016 | 1 |
| Miyamoto et al. ( | Case series | 2016 | 2 |
| Homma et al. ( | Case report | 2017 | 1 |
| Azab and Alsabbahi ( | Case series | 2017 | 13 |
| Kamochi et al. ( | Case series | 2017 | 2 |
| Morice et al. ( | Case series | 2017 | 1 |
| Park et al. ( | Case series | 2017 | 4 |
| Tenekeci et al. ( | Case report | 2017 | 1 |
| Takahashi et al. ( | Case report | 2017 | 1 |
| Bodin et al. ( | Case series | 2017 | 9 |
| Ortmaier et al. ( | Case series | 2017 | 116 |
| Cook et al. ( | Case series | 2017 | 126 |
| De Runz et al. ( | Case series | 2017 | 122 |
| DeLong et al. ( | Case series | 2017 | 2,304 |
| Yuan et al. ( | Case series | 2017 | 25 |
| Papadakis et al. ( | Case report | 2017 | 1 |
| Vairinho et al. ( | Case report | 2018 | 1 |
| Beltrami et al. ( | Case series | 2018 | 2 |
| Kang et al. ( | Case series | 2018 | 2 |
| Ju et al. ( | Case series | 2018 | 7 |
| Marchesi et al. ( | Case series | 2018 | 12 |
| Lai et al. ( | Case report | 2018 | 1 |
| Voss et al. ( | Case series | 2019 | 3 |
| Barrientos et al. ( | Case report | 2019 | 1 |
| Fried et al. ( | Case report | 2019 | 1 |
| Wong et al. ( | Case report | 2019 | 1 |
| Tashiro et al. ( | Case series | 2019 | 6 |
| Djordjevic et al. ( | Case series | 2019 | 129 |
| Dutra et al. ( | Case series | 2019 | 123 |
| Maselli et al. ( | Case series | 2019 | 7 |
| Mericli et al. ( | Case series | 2019 | 47 |
| Motono et al. ( | Case report | 2019 | 1 |
| Boonipat et al. ( | Case report | 2019 | 1 |
| Hallock ( | Case report | 2019 | 1 |
| Hamada et al. ( | Case report | 2019 | 1 |
| Li et al. ( | Case series | 2019 | 11 |
| Liu et al. ( | Case series | 2019 | 16 |
| Lohana et al. ( | Case series | 2019 | 120 |
| Matsumine et al. ( | Case series | 2019 | 2 |
| Özkan et al. ( | Case series | 2019 | 12 |
| Scaglioni and Giunta ( | Case series | 2019 | 5 |
| Khan et al. ( | Case report | 2020 | 1 |
| Menichini et al. ( | Case report | 2020 | 1 |
| Mughal et al. ( | Case series | 2020 | 11 |
| Chim et al. ( | Case series | 2020 | 42 |
| Dragos et al. ( | Case report | 2020 | 1 |
| Cha et al. ( | Case series | 2020 | 45 |
| De Lorenzi et al. ( | Case series | 2020 | 11 |
| Piat et al. ( | Case series | 2020 | 72 |
| Sakharpe et al. ( | Case report | 2020 | 1 |
| Xiao et al. ( | Case report | 2020 | 1 |
| Song et al. ( | Case series | 2020 | 2 |
| Bedarida et al. ( | Case series | 2020 | 8 |
| Ogawa et al. ( | Case report | 2021 | 1 |
| Ogawa et al. ( | Case series | 2021 | 3 |
| Münchow et al. ( | Case report | 2021 | 1 |
| Raymond et al. ( | Case series | 2021 | 18 |
| Ahmed et al. ( | Case series | 2021 | 25 |
| Casella et al. ( | Case series | 2021 | 23 |
| Couto-González et al. ( | Case series | 2021 | 95 |
| Alshammari et al. ( | Case report | 2021 | 1 |
| Valenti et al. ( | Case series | 2021 | 16 |
| Chang et al. ( | Case series | 2021 | 25 |
| Chang et al. ( | Case series | 2022 | 10 |
| Brunetti et al. ( | Case report | 2022 | 1 |
| Fraisse et al. ( | Case report | 2022 | 1 |
| Zhao et al. ( | Case report | 2022 | 1 |
| Zhang et al. ( | Case series | 2022 | 13 |
| Klein et al. ( | Case report | 2022 | 1 |
| Amendola et al. ( | Case report | 2022 | 1 |
| He et al. ( | Case series | 2022 | 72 |
| Miura et al. ( | Case report | 2022 | 1 |
| Feng et al. ( | Case series | 2022 | 20 |
| Yoo et al. ( | Case series | 2022 | 30 |
| Ozaniak et al. ( | Case report | 2022 | 1 |
| Zheng et al. ( | Case series | 2022 | 31 |
| Lee et al. ( | Case series | 2022 | 97 |
| Brambilla et al. ( | Case series | 2022 | 12 |
| Homsy et al. ( | Case series | 2022 | 126 |
| Katayama et al. ( | Case series | 2023 | 3 |
| Alessandri-Bonetti et al. ( | Case report | 2023 | 1 |
| Kagaya et al. ( | Case report | 2023 | 1 |
| Brunetti et al. ( | Case report | 2023 | 1 |
| Chen et al. ( | Case series | 2023 | 15 |
| Bota et al. ( | Case report | 2023 | 1 |
| Alonso-Rodriguez Piedra et al. ( | Case series | 2023 | 10 |
| Adamyan et al. ( | Case series | 2023 | 592 |
| Lellouch et al. ( | Case report | 2023 | 1 |
| Anghel et al. ( | Case report | 2023 | 1 |
| Olvera-Yarza et al. ( | Case report | 2023 | 1 |
| Yang et al. ( | Case report | 2023 | 1 |
| Kim et al. ( | Case report | 2023 | 1 |
| Thione et al. ( | Case series | 2023 | 2 |
| Jaffar et al. ( | Case series | 2023 | 26 |
| Sui et al. ( | Case series | 2023 | 53 |
| La Padula et al. ( | Case series | 2023 | 68 |
| Marque et al. ( | Case report | 2023 | 1 |
| D'Alessandro et al. ( | Case series | 2024 | 176 |
| Banys-Paluchowski et al. ( | Case series | 2024 | 140 |
| Bassiri Gharb et al. ( | Case series | 2024 | 10 |
| Fujioka and Koga ( | Case report | 2024 | 1 |
| Javeed et al. ( | Case series | 2024 | 184 |
| Trapero et al. ( | Case report | 2024 | 1 |
| Wu et al. ( | Case series | 2025 | 65 |
| Nasır ( | Case series | 2025 | 30 |
| Ahmed et al. ( | Case series | 2025 | 18 |
| Rodríguez et al. ( | Case report | 2025 | 1 |
| Mordovskiy et al. ( | Case series | 2025 | 32 |
| Panzenbeck et al. ( | Case series | 2025 | 52 |
| Fragomen et al. ( | Case report | 2025 | 1 |
| Author | Flap indication | Flap type | Recipient vessels | Reinnervation |
|---|---|---|---|---|
| Dixon et al. ( | Breast reconstruction after mastectomy | Pedicled (mini-flap) | – | No |
| Vibhakar et al. ( | Breast reconstruction after mastectomy and lymphadenectomy | Pedicled (+ lateral thoracic lymph nodes transfer) | – | No |
| Endara et al. ( | Breast reconstruction after mastectomy | Free | Internal mammary | No |
| Santanelli di Pompeo et al. ( | Breast reconstruction after mastectomy | Pedicled (+ fat graft) | – | No |
| Højvig y Bonde ( | Breast reconstruction after mastectomy | Pedicled | – | No |
| Kaur et al. ( | Breast reconstruction after mastectomy | Pedicled | – | No |
| Correia Anacleto et al. ( | Breast reconstruction after mastectomy | Pedicled (kite flap) | – | No |
| Banys-Paluchowski et al. ( | Thoracic wall reconstruction after male mastectomy | Pedicled | – | No |
| He et al. ( | Breast reconstruction in Poland syndrome | Pedicled chimeric (+ thoracodorsal artery perforator flap) | – | No |
| Cook et al. ( | Breast reconstruction after mastectomy | Pedicled | – | No |
| De Runz et al. ( | Breast reconstruction after mastectomy and RT | Pedicled | – | No |
| DeLong et al. ( | Breast reconstruction after mastectomy and RT | Pedicled | – | No |
| Yuan et al. ( | Breast reconstruction after partial or total mastectomy | Pedicled (laparoscopic) | – | No |
| Lai et al. ( | Breast reconstruction after lumpectomy | Pedicled (laparoscopic) | – | No |
| Lee et al. ( | Breast reconstruction after mastectomy | Pedicled (vertical and mini-flap) | – | No |
| Dutra et al. ( | Breast reconstruction after mastectomy and RT | Pedicled | – | No |
| Li et al. ( | Breast reconstruction after radionecrosis | Pedicled | – | No |
| Liu et al. ( | Breast reconstruction in Poland syndrome | Pedicled | – | No |
| Lohana et al. ( | Breast reconstruction after mastectomy | Pedicled (bilateral) | – | No |
| Maselli et al. ( | Breast reconstruction after mastectomy | Pedicled | – | No |
| Mericli et al. ( | Breast reconstruction after lumpectomy | Pedicled | – | No |
| Motono et al. ( | Breast and thorax reconstruction after tumoral excision | Pedicled | – | No |
| Cha et al. ( | Breast reconstruction after mastectomy | Pedicled (+ fat graft) | – | No |
| De Lorenzi et al. ( | Breast reconstruction after mastectomy | Pedicled | – | No |
| Piat et al. ( | Breast reconstruction after mastectomy | Pedicled (+ fat graft) | – | No |
| Sakharpe et al. ( | Breast reconstruction after mastectomy | Reverse pedicled based on intercostal arteries | – | No |
| Song et al. ( | Breast reconstruction after mastectomy | Pedicled (bilobed) | – | No |
| Ahmed et al. ( | Breast reconstruction after mastectomy | Pedicled (+ fat graft) | – | No |
| Casella et al. ( | Breast reconstruction after mastectomy | Pedicled (kite flap) | – | No |
| Couto-González et al. ( | Breast reconstruction after mastectomy | Pedicled (+ fat graft) | – | No |
| Feng et al. ( | Breast reconstruction after mastectomy | Pedicled (laparoscopic) | – | No |
| Zheng et al. ( | Breast reconstruction after mastectomy | Pedicled (vertical) | – | No |
| Chen et al. ( | Breast reconstruction after mastectomy | Pedicled (Da Vinci) | – | No |
| D'Alessandro et al. ( | Breast reconstruction after mastectomy | Pedicled | – | No |
| Banys-Paluchowski et al. ( | Breast reconstruction after mastectomy | Pedicled | – | No |
| Javeed et al. ( | Breast reconstruction after mastectomy | Pedicled (fleur-de-lis flap) | – | No |
| Angrigiani et al. ( | Breast reconstruction after mastectomy | Pedicled Thoracodorsal Artery Perforator Flap (TDAP) | – | No |
| Brambilla et al. ( | Breast reconstruction after mastectomy | Pedicled TDAP (+ implants) | – | No |
| Homsy et al. ( | Breast reconstruction after mastectomy | Pedicled and Free TDAP | Internal mammary | No |
| Author | Flap indication | Flap type | Recipient vessels | Reinnervation |
|---|---|---|---|---|
| Sabatier et al. ( | Craniofacial reconstruction after tumoral excision | Pedicled | – | No |
| Wilkman et al. ( | Craniofacial reconstruction after tumoral excision | Pedicled | – | No |
| Papadopoulos et al. ( | Craniofacial reconstruction after tumoral excision | Free | Temporal superficial, facial or external carotid | No |
| Bootz et al. ( | Anterior cranial reconstruction after tumoral excision | Free | Facial or temporal superficial | No |
| Schultes et al. ( | Oral defect and tongue reconstruction after tumoral excision | Free | Facial | Yes (neurorrhaphy to lingual branch of facial nerve) |
| Kim et al. ( | Cranial reconstruction after infection or traumatic defect | Free | Temporal superficial | No |
| Kim et al. ( | Nasal reconstruction after osteomyelitis | Free | Facial | No |
| Biglioli et al. ( | Spheno-orbital reconstruction after tumoral excision | Free (+ rib bone graft) | Temporal superficial or cervical | No |
| Karle et al. ( | Jaw reconstruction after tumoral excision | Free chimeric (+ scapular flap + | Internal mammary | No |
| Hillerup et al. ( | Jaw reconstruction after osteonecrosis | Free (+ iliac bone graft) | Superior thyroid | No |
| Gilleard et al. ( | Craniofacial reconstruction after parotid abscess | Free | Facial | Yes (neurorrhaphy to buccal branch of facial nerve) |
| Longo et al. ( | Craniofacial reconstruction after tumoral excision | Free | Superior thyroid or facial | No |
| Singh et al. ( | Scalp reconstruction after tumoral excision | Free | Temporal superficial | No |
| Tan et al. ( | Scalp reconstruction after traumatic defect | Free | A-V loop (facial artery and vein; and small saphenous vein) | No |
| Mutlu et al. ( | Scalp reconstruction after tumoral excision | Free | Temporal superficial | No |
| Kamochi et al. ( | Orbitomaxillary reconstruction after tumoral excision | Free chimeric (+ scapular flap) | Facial | No |
| Morice et al. ( | Scalp reconstruction after traumatic defect | Free | Temporal superficial | No |
| Park et al. ( | Facial reconstruction after maxilectomy | Free chimeric (+ scapular flap) | Facial or temporal superficial | No |
| Tenekeci et al. ( | Scalp reconstruction after tumoral excision | Free | Temporal superficial | No |
| Barrientos et al. ( | Cerebrospinal fluid fistula coverage after tumoral excision and radiation | Free | A-V loop (facial artery and vein; and saphenous vein) | No |
| Fried et al. ( | Scalp reconstruction after tumoral excision | Free | Superior thyroid | No |
| Scaglioni and Giunta ( | Scalp reconstruction after tumoral excision | Free TDAP | Temporal superficial | No |
| Wong et al. ( | Facial reconstruction after arteriovenous malformation | Free (bilateral) | Facial | Yes (neurorrhaphy to zygomatic branch of facial nerve and hypoglossal nerve) |
| Voss et al. ( | Jaw reconstruction after tumoral excision | Free chimeric (+ scapular flap) | External carotid | No |
| Mughal et al. ( | Scalp reconstruction after tumoral excision | Free | Temporal superficial | No |
| Xiao et al. ( | Scalp reconstruction after tumoral excision | Free | Facial | No |
| Klein et al. ( | Facial reconstruction after maxillectomy | Free (+ rib bone graft) | Facial | No |
| Katayama et al. ( | Jaw reconstruction after tumoral excision | Free | A-V fistula (facial artery and vein) | No |
| Alessandri-Bonetti et al. ( | Scalp reconstruction after burn debridement | Pedicled | – | No |
| Bassiri Gharb et al. ( | Scalp reconstruction after tumoral excision or cerebrovascular accident | Free (+ rib bone graft) | External carotid, linguofacial trunk or occipital | No |
| Trapero et al. ( | Scalp reconstruction after arterio-venous malformation excision | Free chimeric (+ anterior serratus muscle) | Subscapular | No |
| Thione et al. ( | Neck and pharyngeal reconstruction after tumoral excision | Free | Inferior thyroid or lingual | No |
| Jaffar et al. ( | Head and neck reconstruction after tumoral excision | Free TDAP | Superior thyroid or facial | No |
| Rodríguez et al. ( | Mandibular reconstruction after tumoral excision | Pedicled chimeric (+ rib) | – | No |
| Author | Flap indication | Flap type | Recipient vessels | Reinnervation |
|---|---|---|---|---|
| Amin et al. ( | Axillary region reconstruction after tumoral excision | Pedicled | – | No |
| Wormald et al. ( | Axillary reconstruction after hidradenitis suppurativa | Pedicled TDAP | – | No |
| La Padula et al. ( | Axillary reconstruction after hidradenitis suppurativa | Pedicled TDAP | – | No |
| Chang et al. ( | Axillary and inguinal reconstruction after burn contracture | Free TDAP | Axillary and femoral | No |
| Miura et al. ( | Coverage of aortic prosthesis after omentopexy infection | Free (+ rectus abdominis muscle) | Transverse cervical | No |
| Bodin et al. ( | Thoracic wall reconstruction after tumoral excision | Free chimeric (+ anterior serratus muscle) | Contralateral thoracodorsal | No |
| Lü et al. ( | Thoracic wall reconstruction after tumoral excision | Pedicled (bilobed) | – | No |
| Papadakis et al. ( | Thoracic wall reconstruction after epirubicin extravasation | Pedicled | – | No |
| Vairinho et al. ( | Thoracic wall reconstruction after radionecrosis | Pedicled | – | No |
| Boonipat et al. ( | Thoracic wall reconstruction after tumoral excision | Pedicled (+ groin flap + | – | No |
| Hallock ( | Thoracic wall reconstruction after thoracotomy wound necrosis | Pedicled (+ serratus anterior muscle) | – | No |
| Khan et al. ( | Thoracic wall reconstruction after gunshot | Pedicled | – | No |
| Fraisse et al. ( | Thoracic wall reconstruction after epirubicin extravasation | Pedicled | – | No |
| Zhang et al. ( | Thoracic wall reconstruction after sternal wound necrosis | Pedicled | – | No |
| Zhao et al. ( | Thoracic wall reconstruction after tumoral excision | Pedicled (+ rectus abdominis muscle + | – | No |
| Yang et al. ( | Thoracic wall reconstruction after radionecrosis | Pedicled | – | No |
| Beltrami et al. ( | Scapular region reconstruction after tumoral excision | Pedicled (+ scapular prosthesis) | – | No |
| Kang et al. ( | Sacral reconstruction after pressure ulcer | Reverse turnover pedicled based on posterior intercostal arteries | – | No |
| Park and Koh ( | Ischiosacral reconstruction after pressure ulcer | Free | Superior gluteal | No |
| Phan et al. ( | Sacral reconstruction after pressure ulcer | Free (+ serratus anterior muscle) | Inferior gluteal | No |
| He et al. ( | Ischial reconstruction after pressure ulcer | Free | Superior gluteal | No |
| Chang et al. ( | Sacral reconstruction after pressure ulcer | Free | Gluteal | No |
| Cigna et al. ( | Lumbosacral region reconstruction after tumoral excision | Pedicled (supercharged with inferior gluteal artery) | – | No |
| Tuncer et al. ( | Lumbosacral region reconstruction after tumoral excision | Free | A-V loop (thoracodorsal artery and vein; and saphenous vein) | No |
| Miyamoto et al. ( | Lumbosacral region reconstruction after tumoral excision | Free (flow-through) | Rectal superior (scapular circumflex and anterior serratus as T segment) | No |
| Hamada et al. ( | Lumbosacral region reconstruction after tumoral excision | Reverse pedicled based on lumbar arteries (supercharged with anterior serratus artery) | – | No |
| Menichini et al. ( | Lumbosacral region reconstruction after tumoral excision | Reverse pedicled based on anterior serratus artery | – | No |
| Brunetti et al. ( | Lumbosacral region reconstruction after tumoral excision | Pedicled chimeric (+ fascio-cutaneous propeller flap) | – | No |
| Author | Flap indication | Flap type | Recipient vessels | Reinnervation |
|---|---|---|---|---|
| Fujioka et al. ( | Abdominal wall and pelvis reconstruction after tumoral excision | Free chimeric (+ anterior serratus muscle) | Deep femoral | No |
| Hornez et al. ( | Abdominal wall reconstruction after traumatic explosion | Pedicled | – | No |
| Bodin et al. ( | Abdominal wall reconstruction after tumoral excision | Free | Deep inferior epigastric | Yes (spontaneous) |
| Brunetti et al. ( | Abdominal wall reconstruction after tumoral excision | Free | Deep inferior epigastric | Yes (spontaneous) |
| Lellouch et al. ( | Abdominal wall reconstruction after enterocutaneous fistula | Free | Superficial femoral | No |
| Ahmed et al. ( | Abdominal wall repair after massive ventral hernia | Free | Deep inferior epigastric | No |
| Author | Flap indication | Flap type | Recipient vessels | Reinnervation |
|---|---|---|---|---|
| Allen et al. ( | Coverage of distal leg traumatic amputation | Free chimeric (+ scapular flap) | Posterior tibial | No |
| Germann et al. ( | Dorsum of foot reconstruction after tumoral excision in newborn | Free (+ tendon transfer) | Anterior tibial | No |
| Hierner et al. ( | Coverage of knee after arthroplasty | Free | Superficial femoral | No |
| Hwang et al. ( | Reconstruction of distal leg after Marjolin ulcer excision | Free (use of pedicle as a T-junction to facilitate fibular free flap) | Anterior tibial | No |
| Nazerani et al. ( | Reconstruction of knee after traumatic defect | Free (+ rib bone graft) | Popliteal | No |
| Patel et al. ( | Coverage of distal leg traumatic amputation and extensor muscle resection | Free chimeric (+ anterior serratus muscle + | Anterior tibial | Yes (neurorrhaphy to deep peroneal nerve) |
| Venkatramani et al. ( | Reconstruction of knee after traumatic defect | Free | Descending genicular | No |
| Jain et al. ( | Reconstruction of knee after traumatic defect | Free | Anterior tibial | No |
| Miyamoto et al. ( | Reconstruction of distal leg after tumoral excision | Free (flow-through) | Anterior tibial and posterior tibial (scapular circumflex as T segment) | No |
| Gao et al. ( | Reconstruction of distal leg after traumatic defect | Free (flow-through) | Posterior tibial (scapular circumflex and subscapular as T segment) | No |
| Gencel et al. ( | Reconstruction of distal leg after electrical burn debridement | Free (cross flow-through) | Contralateral posterior tibial (scapular circumflex, subscapular and anterior serratus as T segment) | No |
| Hwang et al. ( | Reconstruction of leg after tibial open fracture | Free (+ iliac bone graft) | Anterior tibial or posterior tibial | No |
| Rednam and Rinker ( | Reconstruction of leg after tibial open fracture | Free | Anterior tibial | Yes (neurorrhaphy to motor branch of soleus nerve) |
| Tashiro et al. ( | External hemipelvectomy reconstruction after tumoral excision | Free (flow-through) | Deep inferior epigastric (scapular circumflex as T segment) | Yes (spontaneous) |
| Chim et al. ( | Leg, ankle and foot reconstruction after traumatic defect | Free | Anterior tibial or posterior tibial | No |
| Dragos et al. ( | Reconstruction of knee after traumatic defect | Free (anterior serratus muscle (+ rib bone graft) | Posterior tibial | No |
| Münchow et al. ( | Coverage of knee after infected arthroplasty | Free | A-V loop (common femoral artery and vein; and contralateral great saphenous vein) | No |
| Raymond et al. ( | Coverage of knee after arthroplasty | Free | Superficial femoral | No |
| Amendola et al. ( | Reconstruction of leg and foot after traumatic defect | Free chimeric (+ scapular flap + | Descending branch of lateral femoral circumflex and anterior tibial | No |
| He et al. ( | Reconstruction of knee, leg, ankle and foot after traumatic defect or tumoral excision | Free | Descending branch of lateral femoral circumflex, descending genicular, lateral superior genicular, popliteal, anterior tibial, posterior tibial, medial sural, peroneal | No |
| Kagaya et al. ( | Coverage of Lisfranc stump in patients with chronic ischemia | Free | Arterialized vein (superficial femoral artery bypass to great saphenous vein) | No |
| Sui et al. ( | Leg, knee and foot reconstruction after trauma, tumoral excision and burn scar | Free TDAP (+ latissimus dorsi muscle) | Medial gluteal, superficial femoral, posterior tibial or anterior tibial | No |
| Fragomen et al. ( | Lower limb reconstruction and lymphedema treatment | Free chimeric (+ fasciocutaneous flap + | Posterior tibial | No |
| Author | Flap indication | Flap type | Recipient vessels | Reinnervation |
|---|---|---|---|---|
| Meiners et al. ( | Shoulder reconstruction after infection of neuropathic shoulder | Pedicled | – | No |
| Ozer et al. ( | Elbow reconstruction after open fracture and loss of soft tissue | Pedicled (+ rib bone graft) | – | No |
| Qu et al. ( | Elbow and arm reconstruction after traumatic defects | Pedicled | – | No |
| Ng et al. ( | Elbow reconstruction after tumoral excision | Free | Brachial | No |
| Kim et al. ( | Multiple digit reconstruction after traumatic defects or infection | Free (+ iliac bone grafts) | Radial y dorsal radial | No |
| Kesiktas et al. ( | Coverage of transhumeral stump after electric burn debridement | Pedicled | – | No |
| Cadenelli et al. ( | Shoulder and arm reconstruction after tumoral excision | Pedicled | – | No |
| Anghel et al. ( | Coverage of high transhumeral stump after high-energy trauma | Pedicled | – | Yes (neurorrhaphy to ulnar and median nerve) |
| Olvera-Yarza et al. ( | Coverage of axillary region after hidradenitis suppurativa debridement | Pedicled | – | No |
| Marchesi et al. ( | Coverage of axillary region after hidradenitis suppurativa debridement | Pedicled | – | No |
| Author | Flap indication | Flap type | Recipient vessels | Reinnervation |
|---|---|---|---|---|
| Perovic et al. ( | Phalloplasty in congenital aphallia, iatrogenic and traumatic amputations | Free | Femoral | Yes (neurorrhaphy to ilioinguinal nerve) |
| Adamyan et al. ( | Phalloplasty in gender affirming surgery (female to male) | Free | Deep epigastric | Yes (neurorrhaphy to motor branch of obturator nerve) |
| Djordjevic et al. ( | Phalloplasty in gender affirming surgery (female to male) | Free | Femoral | Yes (neurorrhaphy to ilioinguinal nerve) |
| Djordjevic et al. ( | Phalloplasty in congenital aphallia | Free | Femoral | Yes (neurorrhaphy to ilioinguinal nerve) |
| Gakis et al. ( | Functional detrusor myoplasty in patients with bladder acontractility caused by lower motor neuron lesion | Free | Inferior epigastric | Yes (neurorrhaphy to 12th intercostal nerve) |
| Rednam and Rinker ( | Functional reconstruction of posterior compartment of leg after traumatic defect | Free | Tibioperoneal trunk | Yes (neurorrhaphy to soleus branch of tibial nerve) |
| Patel et al. ( | Restoration of ankle dorsiflexion after traumatic defect | Free | Anterior tibial | Yes (neurorrhaphy to deep peroneal nerve) |
| Anghel et al. ( | Restoration of flexion and extension of arm after high transhumeral amputation | Pedicled | – | Yes (neurorrhaphy to radial nerve and median nerve) |
| Fujioka and Koga ( | Functional reconstruction of trapezius muscle after tumoral excision | Pedicled | – | Yes (neurorrhaphy to accessory nerve) |
| Nicoli et al. ( | Functional triceps reconstruction after tumoral excision | Free (supercharged) (+ groin flap + | Radial | Yes (neurorrhaphy to cubital nerve) |
| Trimaille et al. ( | Restoration of wrist and finger flexion and extension after congenital Volkmann contracture | Free | Radial | Yes (neurorrhaphy to median nerve) |
| Horta et al. ( | Phrenic nerve neurotization for restoring physiological motion in congenital diaphragmatic hernia | Pedicled | - | Yes (neurorrhaphy to phrenic nerve) |
| Gilleard et al. ( | Craniofacial reconstruction after parotid abscess | Free | Facial | Yes (neurorrhaphy to buccal branch of facial nerve) |
| Takushima et al. | Facial reanimation after tumor excision, Bell's palsy, trauma or stroke | Free | Facial | Yes (neurorrhaphy to buccal branch of contralateral facial nerve) |
| Okazaki et al. ( | Facial reanimation after tumoral excision or congenital cause | Free (bilobed) (+ fascia lata graft) | Facial | Yes (neurorrhaphy to buccal branch of facial nerve; and masseteric branch of mandibular nerve) |
| Homma et al. ( | Facial reanimation after tumoral excision | Free (bilobed) (+ fascia lata graft) | Facial | Yes (neurorrhaphy to masseteric branch of mandibular nerve) |
| Matsumine et al. ( | Facial reanimation after tumoral excision or traumatic defect | Free chimeric (+ anterior serratus muscle) | Facial | Yes (neurorrhaphy to buccal branch of facial nerve and masseteric branch of mandibular nerve) |
| Wong et al. ( | Facial reanimation after arteriovenous malformation excision | Free | Facial | Yes (neurorrhaphy to zygomatic branch of facial nerve) |
| Ogawa et al. ( | Facial reanimation after tumoral excision | Free chimeric (+fascio-adipo-cutaneous flap + | Facial | Yes (neurorrhaphy to buccal branch and zygomatic branch of facial nerve) |
| Yoo et al. ( | Facial reanimation after tumoral excision or traumatic defect | Free | Facial | Yes (neurorrhaphy to masseteric branch of trigeminal nerve and facial nerve) |
| Bedarida et al. ( | Facial reanimation after tumoral excision or trauma | Free TDAP | External carotid | Yes (neurorrhaphy to trunk and distal branches of facial nerve) |
| Panzenbeck et al. ( | Facial reanimation after congenital Moebius syndrome | Free (bilateral) | Facial | Yes (neurorrhaphy to masseteric, hypoglossal or accessory nerves) |
| Ogawa et al. ( | Oral depressor muscles reinnervation after tumoral excision | Free chimeric (+ fascio-adipo-cutaneous flap) | Facial and superior thyroid | Yes (neurorrhaphy to marginal branch and buccal branch of facial nerve) |
| Wu et al. ( | Functional tongue reconstruction after tumoral excision | Free TDAP | Facial | Yes (neurorrhaphy to hypoglossal nerve) |
| Mordovskiy et al. ( | Functional tongue and suprahyoid muscles reconstruction after tumoral excision | Free chimeric (+ serratus anterior muscle) |
| Yes (neurorrhaphy to hypoglossal nerve) |
| Author | Flap indication | Flap type | Recipient vessels | Reinnervation |
|---|---|---|---|---|
| Marque et al. ( | Phalloplasty in gender affirming surgery (female to male) | TDAP | Inferior epigastric | No |
| Nasır ( | Phalloplasty in gender affirming surgery (female to male), congenital aphallia and traumatic amputations | Free | Superior femoral or common femoral | No |
| Gangurde et al. ( | Thoracic wall reconstruction after Jarcho-Levin syndrome | Pedicled | – | No |
| Tsai et al. ( | Bronchopleural fistula collapse | Pedicled | – | No |
| Zimmermann et al. ( | Closure of acute bronchial stump after pneumonectomy | Pedicled | – | No |
| Yap et al. ( | Repair of thoracic oesophageal perforation | Pedicled | – | No |
| Bianchi et al. ( | Diaphragmatic hernia restoration in newborns | Reverse pedicled | – | No |
| Wallace and Roden ( | Diaphragmatic hernia restoration in newborns | Reverse pedicled | – | No |
| Whetzel et al. ( | Diaphragmatic hernia restoration in kids | Reverse pedicled | – | No |
| Bedini et al. ( | Diaphragmatic reconstruction after pneumonectomy | Reversed pedicled | – | No |
| McConkey et al. ( | Diaphragmatic reconstruction after tumoral excision | Pedicled | – | No |
| Buchanan et al. ( | Functional pectoral muscle reconstruction in Poland syndrome | Pedicled | – | No |
| Muramatsu et al. ( | Functional deltoid muscle reconstruction after tumoral excision | Pedicled | – | No |
| De Smet et al. ( | Functional deltoid muscle reconstruction after irreparable axillary lesion | Pedicled | – | No |
| Bota et al. ( | Functional deltoid muscle reconstruction after trauma | Pedicled | – | No |
| Ortmaier et al. ( | Mobility restoration of rotator cuff in combination with humeral arthroplasty | Pedicled | – | No |
| Valenti et al. ( | Mobility restoration of rotator cuff in combination with humeral arthroplasty | Pedicled | – | No |
| Alonso-Rodriguez Piedra et al. ( | Mobility restoration of rotator cuff in combination with humeral arthroplasty | Pedicled | – | No |
| Kim et al. ( | Reconstruction of chronic seroma pocket in axillary fossa | Pedicled | – | No |
| Vibhakar et al. ( | Breast reconstruction and lymphedema treatment | Pedicled (bilateral) (+ lateral thoracic nodes transfer) | – | No |
| Azab and Alsabbahi ( | Restoration of elbow flexion after traumatic defect | Pedicled | – | No |
| Ozaniak et al. ( | Restoration of elbow flexion after tumoral excision | Pedicled | – | No |
| Alshammari et al. ( | Restoration of elbow flexion after traumatic defect | Pedicled | – | No |
| Ihara et al. ( | Restoration of flexion and extension of fingers after traumatic defects | Pedicled | – | Yes (spontaneous) |
| Takahashi et al. ( | Restoration of finger extension after traumatic defects | Pedicled | – | Yes (spontaneous) |
| Ozcan Akcal et al. ( | Functional foot reconstruction after traumatic defects | Free chimeric (+ scapular flap) | Anterior tibial and posterior tibial | No |
| Ju et al. ( | Chronic osteomyelitis treatment in lower limb | Free (+ iliac bone graft) | Anterior tibial and posterior tibial | No |
| Fragomen et al. ( | Lower limb reconstruction and lymphedema treatment | Free chimeric (+ fasciocutaneous flap + | Posterior tibial | No |
| Biglioli et al. ( | Spheno-orbital reconstruction after tumoral excision | Free (+ rib bone graft) | Temporal superficial or cervical | No |
| Park et al. ( | Maxillary reconstruction after tumoral excision | Free chimeric (+ scapular flap) | Facial or temporal superficial | No |
| Kamochi et al. ( | Orbitomaxillary reconstruction after tumoral excision | Free chimeric (+ scapular flap) | Facial | No |
| Özkan et al. ( | Functional lower lip reconstruction after tumoral excision of traumatic defect | Free | Facial or superior thyroid | Yes (spontaneous) |
| Thione et al. ( | Pharyngeal reconstruction after tumoral excision | Free | Inferior thyroid or lingual | No |
| Bach et al. ( | Oral and pharyngeal reconstruction after tumoral excision | Free TDAP | Thyroid or facial | No |
| Rodríguez et al. ( | Mandibular reconstruction after tumoral excision | Pedicled chimeric (+ rib) | – | No |
| Location | Coverage | Functional non-innervated | Functional innervated |
|---|---|---|---|
| Breast | Breast reconstruction (internal mammary vessels as receptors) | – | |
| Head and neck | Coverage of skull base, scalp and craniofacial region following tumor resection, infection, trauma or osteonecrosis | Functional pharyngeal and lower lip reconstruction following trauma or tumor | Functional reconstruction of floor of mouth, tongue and cervicofacial region following tumor resection and infection |
| Thorax and back | Coverage of chest wall, axilla, scapula, lumbosacral or ischiosacral region following tumor resection, pressure ulcer or infection | Coverage of aortic prosthesis following infection and extended thoracic wall and lumbosacral region | – |
| Abdomen and pelvis | Coverage of abdominal wall following tumor resection, ventral hernias or entero-cutaneous fistulas | Functional abdominal wall reconstruction following tumor resection or trauma | Neo-phalloplasty (gender affirmation surgery or traumatic and congenital amputations) |
| Lower limb | Coverage of thigh, knee, leg and foot following trauma, infection, tumor resection, chronic or burns | Functional stump, knee and foot reconstruction following trauma, chronic osteomyelitis and tumor resection | Restoration of ankle dorsiflexion and posterior compartment function following traumatic amputations |
| Upper limb | Coverage of arm, elbow and fingers following tumor resection, trauma or infection | Functional elbow and hand reconstruction with skeletal components | Restoration of elbow flexion, wrist flexion and extension following tumor resection and Volkmann's contracture |
| Location | Coverage | Functional non-innervated | Functional innervated |
|---|---|---|---|
| Breast | Breast reconstruction after mastectomy or lumpectomy; volume replacement combined with implants, expanders or fat grafting | – | |
| Head and neck | Coverage of scalp and craniofacial region following tumoral resection or burns | Maxilla reconstruction following tumoral excision | – |
| Thorax and back | Coverage of chest wall, axilla, scapula and posterior trunk following tumoral resection, or tissue necrosis (secondary to extravasation, radionecrosis, pressure sores) | Repair of congenital diaphragmatic hernia or post-oncologic defects, closure of bronchopleural fistulae, repair of esophageal perforation and chest reconstruction in Poland and Jarcho-Levin syndromes | Diaphragm reinnervation following congenital diaphragmatic hernia and reinnervation of shoulder after tumoral resection |
| Abdomen and pelvis | Coverage of abdomen and pelvis following trauma | – | – |
| Lower limb | – | – | – |
| Upper limb | Coverage of shoulder, arm and elbow following trauma, burns, infection, hidradenitis or tumoral resection | Functional repair of shoulder and upper limb following tumor or trauma | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReconstructive Surgery and Microvascular Techniques · Reconstructive Facial Surgery Techniques · Nerve Injury and Rehabilitation
Introduction
The latissimus dorsi (LD) flap is one of the most versatile and widely utilized options in reconstructive surgery, offering a reliable solution for virtually any type of defect. It employs the latissimus dorsi muscle, a broad, flat muscle located in the posterior thorax, which is primarily supplied by the thoracodorsal artery and vein, branches of the subscapular system, and innervated by the thoracodorsal nerve (1).
First introduced in 1906, the LD flap was initially used for breast reconstruction following mastectomy (2). Over time, its applications have expanded significantly, making it a cornerstone in reconstructive surgery. The flap provides a well-vascularized, pliable, and durable tissue, which can reconstruct defects in multiple anatomical regions, including the head and neck, chest wall, upper and lower extremities, back and pelvis. Additionally, the LD flap has been proven valuable in both functional and aesthetic reconstruction, with modifications such as innervated flaps for restoring muscle function and perforator-based techniques for minimizing donor site morbidity.
Despite its widespread use, the indications, advantages, and limitations of the LD flap continue to evolve and grow. While some surgeons favor it due to its reliable vascularity and large surface area, concerns related to donor site morbidity, muscle atrophy, and functional impairment (3–5) have led to ongoing refinements in surgical techniques [such as muscle-sparing flaps (6–8)]. Innovations such as robot-assisted (9–12) and endoscopic (6, 13, 14) harvest, fat grafting (15–17), neuromuscular reinnervation, and the use of chimeric or hybrid flaps have further expanded its reconstructive potential.
This systematic review aims to provide a comprehensive analysis of all applications of the latissimus dorsi flap in reconstructive surgery. By compiling its described uses across different anatomical regions and surgical contexts, we seek to highlight the versatility, benefits, and evolving role of this flap in modern microsurgical reconstruction. Through this work, we aspire to offer a comprehensive guide for both novice and experienced surgeons, that will serve as a reference to easily review all possible applications of this versatile flap in reconstructive surgery. Organized by anatomical regions, this guide should assist and inspire surgeons when in search of reconstructive options facing a specific defect.
Material and methods
Search strategy
We conducted a systematic review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and AMSTAR 2 (18) guidelines on the published uses of the latissimus dorsi flap in reconstructive surgery.
One electronic database (Medline) was queried from June 4, 2024 to July 30, 2024 using the following research strategy: [superficial back muscles/surgery(MeSH Terms)] AND ([surgery, plastic(MeSH Terms)] OR [Plastic Surgery Procedures(MeSH Terms)]). In response to the peer-review process, the literature search was subsequently updated to include newly published studies, with the final search performed on January 10, 2026. Relevant additional articles identified through this update were incorporated into the final analysis and tables.
Inclusion and exclusion criteria
We included all articles meeting the following criteria: articles published in English, Spanish or French (languages spoken by both reviewers), with full-text freely available or retrievable via our institution's library (Hospital La Fe), published in indexed journals, on common and original indications of the latissimus dorsi flap in reconstructive surgery.
We excluded publications in conferences or congresses, letters to the editor, press releases, editorials, comments, reviews and cohort studies. In such a way, only case-series were collected, as the purpose of our study was to compile only the reported indications the flap had been used for and not comparing or contrasting it with other reconstructive methods.
Data extraction and evaluation
Both reviewers independently revised the selected articles, individually extracting the relevant data, which was later combined and contrasted. The following data was collected: author, defect location and indication, flap type (pedicled or free), recipient vessels and presence or absence of reinnervation.
The methodological quality and risk of bias of the included case reports and case series were assessed using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Case Reports. This checklist evaluates key aspects such as the clarity of the clinical presentation, the appropriateness of the interventions and outcomes reported, follow-up duration, and ethical considerations. Each included study was appraised independently by two reviewers, with disagreements resolved through discussion or consultation with a third reviewer.
Given the purely descriptive aim of this review, no statistical analysis was performed. Instead, the published indications of the latissimus dorsi flap were systematically compiled and organized to allow readers to appreciate the breadth and versatility of its reported applications.
Results
Our search yielded 450 articles. Initial screening reduced the sample to 379 publications. After reading all titles and abstracts and applying our exclusion criteria, only 213 articles were selected. Finally, following full-text reading, 133 articles were included in our review. Citation tracking identified an additional 31 relevant studies, resulting in 164 articles included from the initial search. During the revision of the manuscript, the literature search was updated to include newly published studies. From this update, 24 additional articles deemed most relevant to the scope of the review were incorporated into the final analysis and tables, bringing the total number of included full-text articles to 188. Figure 1 represents the PRISMA flow diagram. The results of the quality assessment for each included study are summarized in the Supplementary Material (Supplementary Table S1).
PRISMA flow diagram. This figure shows the number of records identified, screened, and included in the systematic review, along with reasons for exclusion at each stage, following PRISMA 2020 guidelines.
Table 1 (with results sorted by publication date) summarizes the characteristics of the 188 selected articles, which included 76 case reports and 112 case series. Although most studies consisted of single-case reports or small series, several large retrospective series were also identified, reflecting the predominantly descriptive nature of the available evidence. All studies had been conducted in the last 40 years, with the oldest dating back to 1983 and the most recent to 2025.
Based on anatomical location, the included articles were categorized into six major reconstructive domains: breast reconstruction (39 articles), head and neck reconstruction (34 articles), thorax and back reconstruction (28 articles), abdominal and pelvic reconstruction (6 articles), lower limb reconstruction (23 articles), and upper limb reconstruction (10 articles).
Regarding its reconstructive purpose, 25 articles described functional applications of the innervated latissimus dorsi flap, while 35 articles reported non-innervated flap reconstructions used with a functional purpose. Moreover, 10 of the functional reconstructions mentioned (5 innervated and 7 non-innervated) had a double purpose, involving both defect coverage and functional restoration.
Breast reconstruction represented the most frequently reported indication for the LD flap. The flap was primarily employed for oncologic breast reconstruction following mastectomy or lumpectomy, particularly in patients undergoing radiotherapy and/or chemotherapy. Most reconstructions were performed using pedicled flaps, often combined with implants, tissue expanders, or fat grafting to achieve adequate breast volume in either immediate or delayed settings. Free flaps were less commonly reported in breast reconstruction; when used, the internal mammary vessels were the most frequently selected recipients. Notably, across all reviewed studies, no cases of voluntary or involuntary reinnervation of the LD flap were reported in the context of breast reconstruction. Detailed characteristics of breast reconstruction cases are summarized in Table 2.
The LD flap has been extensively used in head and neck reconstruction for a wide spectrum of defects involving the scalp, skull base, orbit, mandible, maxilla, floor of the mouth, tongue, and pharynx. Indications included oncologic resections, trauma, post-burn contractures, infections, and cerebrospinal fluid fistulas. Both pedicled and free flaps were described, although the latter predominated in this region. Recipient vessels commonly included branches of the external carotid system, such as the facial, superficial temporal, superior and inferior thyroid, and occipital arteries. In complex cases, arteriovenous loops or fistulas were used to facilitate microvascular anastomosis. Functional reinnervation was selectively reported, particularly in facial reanimation and tongue reconstruction. These data are detailed in Table 3.
In thoracic and posterior trunk reconstruction, the LD flap was used to address a wide range of defects involving the chest wall, axilla, scapular region and lumbosacral area. Both pedicled and free flaps were employed, either ipsilateral or contralateral to the defect. Multiple technical modifications were reported, including bilobed, reverse-flow, and supercharged designs, as well as chimeric constructs incorporating the serratus anterior, rectus abdominis, pectoralis major, or groin flaps. Pressure ulcer reconstruction of the sacral and ischial regions was also described, predominantly using free LD flaps anastomosed to gluteal vessels. These reconstructions are summarized in Table 4.
The LD flap was less frequently reported for abdominal and pelvic reconstruction but was used for complex abdominal wall and pelvic defects following trauma or extensive oncologic resections, including pelvic exenteration. Free, pedicled, and chimeric flaps were described, often incorporating the serratus anterior muscle. In this subgroup, several reports documented spontaneous or intentional flap neurotization with recovery of voluntary muscle contraction. Details are provided in Table 5.
Lower extremity reconstruction with the LD flap encompassed defects from the pelvis to the foot, including the thigh, knee, leg, ankle, and foot. Indications included trauma, tumor resection, infection, chronic ischemia, and limb salvage procedures. Free flaps were predominantly used, either as standalone flaps or in chimeric configurations with scapular or serratus anterior components. To extend pedicle length and optimize reach, the thoracodorsal axis was frequently augmented using circumflex scapular or subscapular branches in flow-through or “T” configurations. Functional reinnervation was selectively reported for restoration of ankle dorsiflexion or posterior compartment function. These applications are detailed in Table 6.
Upper extremity reconstruction included defects of the shoulder, arm, elbow, forearm, hand, and digits. Both pedicled and free LD flaps were reported, occasionally combined with bone grafts for skeletal reconstruction. Recipient vessels most commonly included the brachial and radial arterial systems. In selected cases, targeted muscle reinnervation using median, ulnar, or radial nerves was described, particularly in reconstructions aiming to restore elbow or arm function and to reduce neuropathic pain. These data are summarized in Table 7.
Tables 8, 9 specifically summarize functional reconstructions using innervated and non-innervated LD flaps, respectively. Innervated flaps were most frequently employed for facial reanimation, urologic indications such as phalloplasty (in gender affirmation surgery as well as traumatic and congenital amputations) and detrusor myoplasty, upper and lower limb motor restoration and diaphragmatic reconstruction. Non-innervated flaps were primarily used when passive functional support or dynamic stabilization was sufficient, such as in diaphragmatic, shoulder, elbow, and pharyngeal reconstruction.
Discussion
The latissimus dorsi flap remains a a cornerstone of reconstructive surgery owing to its reliable vascular anatomy, long and adaptable pedicle, and broad arc of rotation. These characteristics allow the flap to be harvested as pedicled or free and to be configured in chimeric, bilobed, reverse-flow, or supercharged designs, thereby substantially expanding its reconstructive versatility.
Across the literature, the LD flap has demonstrated value not only as a robust coverage option but also as a powerful tool for functional reconstruction, in both innervated and non-innervated forms, depending on the clinical objective. Nevertheless, despite this broad applicability, its use consistently follows recognizable indication-based patterns related to flap design and reconstructive goals.
As a general concept, pedicled flaps are predominantly described for defects located within their arc of rotation, most commonly involving the breast, chest wall, back, shoulder, and proximal upper extremity. In contrast, free flaps are more frequently reported for distant, extensive, or complex defects, including head and neck reconstruction, distal upper and lower extremity defects, abdominal wall and pelvic reconstruction.
Innervated, often bilobed or chimeric, LD flaps are primarily indicated when active functional restoration is required. Across multiple anatomical regions, targeted neurorrhaphy has enabled recovery of voluntary muscle contraction, thereby extending the role of the LD flap well beyond static coverage. Dynamic facial reanimation emerges as the most frequently reported functional indication, reflecting the favourable muscle excursion of the muscle and its compatibility with facial, masseteric, and hypoglossal nerve branches. In the upper extremity, innervated flaps have been successfully applied for reconstruction of major functional units, including elbow extension, forearm flexion and extension, and targeted muscle reinnervation following amputation, demonstrating the adaptability of the flap in restoring motor control and reducing neuropathic pain. Similarly, in the lower extremity, reinnervated flaps have contributed to the restoration of ankle and foot function following traumatic or oncologic defects. Beyond musculoskeletal reconstruction, innervated flaps have been described in visceral and dynamic reconstructions, such as detrusor myoplasty, neo-phalloplasty, diaphragmatic and pharyngeal reconstruction, and abdominal wall restoration.
By contrast, non-innervated LD flaps remain highly relevant when passive functional support or durable structural restoration is sufficient. Their predominant use as pedicled flaps in breast and thoracic reconstruction and as free flaps in craniofacial reconstruction reflects their reliability and acceptable outcomes.
Lastly, muscle-sparing and perforator-based flaps, including TDAP, are preferentially described in situations where minimization of donor-site morbidity is a primary concern, particularly in breast and trunk reconstruction. Their use reflects an evolving reconstructive philosophy that prioritizes functional preservation while maintaining reliable soft-tissue coverage.
Tables 10, 11 are organized according to flap transfer modality, distinguishing between pedicled and free latissimus dorsi flaps, and further stratified by innervated and non-innervated designs within each category. This structure provides a clear and practical overview of the reported indications, allowing surgeons to readily identify reconstructive strategies that have been described for specific anatomical regions and functional objectives. This framework is intended as a descriptive guide based on the existing literature, rather than a prescriptive algorithm, and aims to support indication-driven decision-making rather than subjective preference.
Several limitations of this qualitative systematic review must be acknowledged. The available evidence is largely derived from case reports and case series, with significant heterogeneity in indications, flap design, nerve selection, and outcome assessment. Objective functional metrics and long-term follow-up are inconsistently reported, precluding quantitative comparison or meta-analysis. Future studies specifically designed to compare reconstructive strategies—ideally through well-structured cohort studies or dedicated systematic reviews—would be valuable to further define optimal flap selection across different clinical scenarios. Nevertheless, the consistency of reliable reconstructive and functional outcomes across a wide range of anatomical regions supports the continued clinical relevance and adaptability of the LD flap in contemporary reconstructive surgery.
Conclusion
In conclusion, the latissimus dorsi flap remains a cornerstone of reconstructive surgery, demonstrating versatility across multiple anatomical regions. Whether used for oncologic, traumatic, or congenital defect reconstruction, it can be employed in multiple configurations, pedicled or free, reinnervated or not, attaining optimal functional and aesthetic outcomes. Its applications continue to evolve, with advancements in microsurgical techniques and functional restoration enhancing its role in complex defect reconstruction.
Our work is the first of its kind to describe and compile all the reported applications of the latissimus dorsi flap published in literature to date, serving as a reference for surgeons to review whenever considering whether the latissimus dorsi flap might be a possible solution for any defect they may be confronted with.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Netter FH. Atlas of Human Anatomy. Philadelphia, PA: Elsevier Health Sciences. (2010).
- 2Tansini I. Sopra il mio nuovo processo sli amputazione della mammella. Gaz Med Ital. (1906) 15:141–2.
- 3Lee K-T Lee YJ Kim A Mun G-H. Evaluation of donor morbidity following single-stage Latissimus dorsi neuromuscular transfer for facial reanimation. Plast Reconstr Surg. (2019) 143:152e–64e. 10.1097/PRS.000000000000516830325893 · doi ↗ · pubmed ↗
- 4Lee K-T Mun G-H. A systematic review of functional donor-site morbidity after latissimus dorsi muscle transfer. Plast Reconstr Surg. (2014) 134:303–14. 10.1097/PRS.000000000000036524732650 · doi ↗ · pubmed ↗
- 5Rindom MB Gunnarsson GL Lautrup MD Christensen RD Tos T Hölmich LR Shoulder-related donor site morbidity after delayed breast reconstruction with pedicled flaps from the back: an open label randomized controlled clinical trial. J Plast Reconstr Aesthet Surg. (2019) 72:1942–9. 10.1016/j.bjps.2019.07.02731515191 · doi ↗ · pubmed ↗
- 6Lee J Jung JH Kim WW Park CS Lee RK Park HY. Endoscopy-assisted muscle-sparing Latissimus dorsi muscle flap harvesting for partial breast reconstruction. BMC Surg. (2020) 20:192. 10.1186/s 12893-020-00853-132854673 PMC 7450551 · doi ↗ · pubmed ↗
- 7Cook J Waughtel J Brooks C Hardin D Hwee YK Barnavon Y. The muscle-sparing Latissimus dorsi flap for breast reconstruction: a retrospective review of 126 consecutive flaps. Ann Plast Surg. (2017) 78:S 263–8. 10.1097/SAP.000000000000103628525414 · doi ↗ · pubmed ↗
- 8Chim H Cohen-Shohet R Mc Laughlin MM Ehanire T. Function-sparing free split latissimus dorsi flap for lower-extremity reconstruction: five-year consecutive single-surgeon series. J Bone Joint Surg Am. (2020) 102:1714–23. 10.2106/JBJS.20.0002232598120 · doi ↗ · pubmed ↗