Adolescents’ health and well-being into the COVID-19 pandemic: A two-wave prospective investigation– The HUNT study
Kirsti Kvaløy, Erik Reidar Sund, Tormod Rimehaug, Kristine Pape, Jo Magne Ingul, Vegar Rangul

TL;DR
This study examines how the mental health and well-being of Norwegian adolescents changed during the early years of the COVID-19 pandemic, with a focus on differences based on socioeconomic status.
Contribution
The study provides new insights into how adolescents' health and well-being changed during the pandemic, particularly highlighting differences based on gender and socioeconomic position.
Findings
Boys and girls reported increased loneliness during the pandemic, while mental distress increased only in boys.
Adolescents from low socioeconomic backgrounds experienced greater declines in health and well-being compared to those from high socioeconomic backgrounds.
Girls in low socioeconomic groups showed improved health and well-being during the study period, unlike boys.
Abstract
Using data on Norwegian adolescents, this study aimed to explore changes in mental health, quality of life, somatic health complaints and loneliness from before and one year into the COVID-19 pandemic, also considering the changes according to socioeconomic position (SEP). The study involved a cross-sectional comparative design with data from Young-HUNT4 (2017–2019) (n = 4347) and Young-HUNT COVID (May/June 2021) (n = 2033), aged 16–19 years. Additionally, longitudinal changes from Young-HUNT4 (n = 1565), aged 13–15 years, with follow-up in Young-HUNT COVID were explored. The impact of SEP was investigated through regression analyses and investigating prevalence changes in high and low SEP groups. In the cross-sectional comparison, boys and girls reported higher levels of loneliness and mental distress (boys only) into the pandemic compared to before, while general health and quality…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
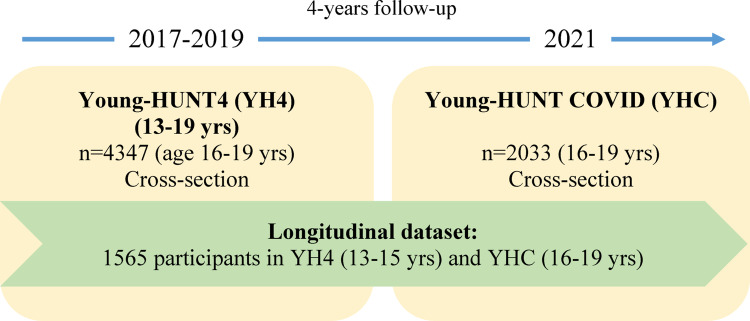 Figure 1
Figure 1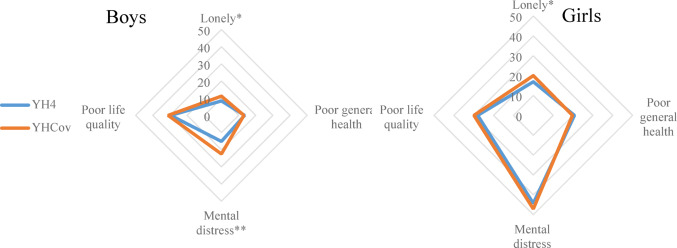 Figure 2
Figure 2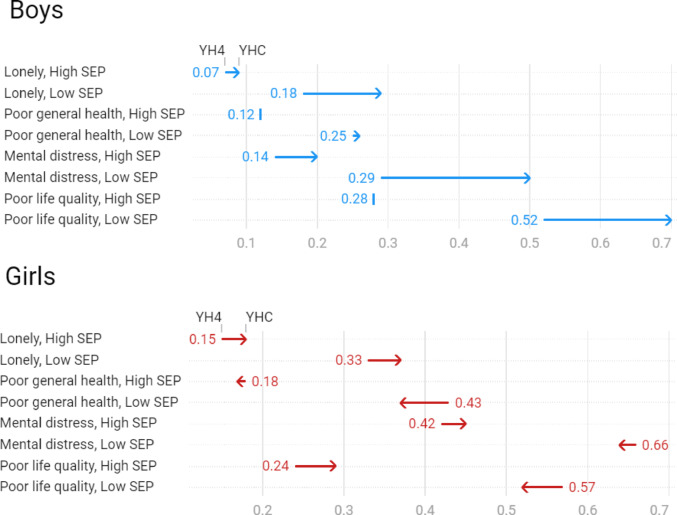 Figure 3
Figure 3- —NTNU Norwegian University of Science and Technology (incl St. Olavs Hospital - Trondheim University Hospital)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and Mental Health · Resilience and Mental Health · Psychological Well-being and Life Satisfaction
Introduction
Most countries in the world implemented full or partial school closures in the period from 2020 to 2021 related to the coronavirus disease 2019 (COVID-19) pandemic. To prevent further spread of the SARS-CoV-2 virus and adverse impacts on health in the population,* this resulted in social distancing and lockdown efforts that negatively affected health and well-being of children and adolescents. This growing recognition was* mostly based on cross-sectional investigations. The Young-HUNT COVID data collection in combination with earlier data collected prior to the COVID-19 pandemic from the same Norwegian adolescent population,* allowed* us to study this in a longitudinal perspective gaining potential general knowledge of underlying factors influencing the adverse health trends observed among today’s young people.
Global estimates said that up to 1.5 billion of the ones younger than 20 years were out of school in early 2020 and again in early 2021 related to the COVID-19 pandemic restrictions [1]. In Norway, all schools were mandatory closed down from March 12, 2020, and then there were dynamic changes throughout 2020 and 2021 that sometimes differed geographically [2]. Compared to many European countries, Norway is sparsely populated and has better social welfare benefit arrangements. These factors combined may have resulted in different conditions for the young people in Norway compared to other equivalent regions of the Western world.
Adolescence is a critical period in life concerning psychosocial development characterized by social transition regarding individual role, peer relationships and family cohesion [3]. This makes adolescents especially vulnerable to the disruptive changes imposed by the pandemic restrictions as mental distress seems to be associated with stress from social isolation [4–6]. Over the last decades there has been several reports of an increase in young people feeling unhappy, reporting mental distress [7–10], and loneliness [11]. How the COVID-19 pandemic interacted with these trends may have varied regionally and globally due to the differences in pandemic restrictions and dissimilarities in society and population [12]. According to the World Health Organization (WHO), the global prevalence of anxiety and depression increased by a massive 25% in the first year of the COVID-19 pandemic [13]. Most studies investigating the impact of the pandemic on mental health have described an increase in mental distress [1, 14–17], but not all [4–6].
Norway implemented a nationwide lockdown on March 12, 2020. This involved compulsory closure of schools and cancellation of organized sport activities. Within a few weeks after the first closure, which also encouraged restrictive social interactions, dynamic change in infection and insecurity regarding the consequences of the contagion, resulted in various restrictions throughout 2020 and 2021. Norwegian adolescents suffered from more restrictions than younger children with repeated and extended periods of home schooling and cancelled sports activities throughout the pandemic period [18]. Norwegian adolescents also experienced adverse mental health during the pandemic [18–20]. In the study by Hafstad et al., somatic health complaints were shown to increase ahead of and 15 months into the pandemic whereof girls appeared to be more affected than boys [18]. Other studies also report a more adverse effect on mental health in girls compared to boys [17, 21, 22]. Most studies published concerning the COVID-19 pandemic’s effect on adolescents have been based on cross-sectional data not being able to shed light on the longitudinal effects within the same group of individuals. Even if such studies are of immense benefit, the effect of ageing within adolescence is of uttermost importance to consider as shown in a previous Norwegian study [23].
The COVID-19 pandemic led to societal changes concerning the use of technologies; digital means of learning and communication, and an increase in screen time usage [1], which may have influenced the experience of loneliness [24]. Others have also suggested loneliness to be an important trigger of the increase in mental health problems, quality of life and somatic complaints during the pandemic [18, 24, 25]. An increase in loneliness among adolescents was observed even before the pandemic [11]. This could suggest that the trend might be a continuation of pre-existing patterns rather than solely a result of the pandemic. Furthermore, the age-typical developmental changes must also be controlled for to clarify the influence of the pandemic. However, it is important to consider that the pandemic might have exacerbated these trends due to increased social isolation and stress. The interplay of multiple contributing factors requires complex datasets that enable the necessary complex designs and analytic strategies to fully understand the dynamics at play.
Social inequality impact mental health acting as additional strain or protective factors affecting the influence of the COVID-19 pandemic on mental health and quality of life. Those with low socioeconomic status (families with low education levels or limited financial resources) may have been affected more [17], hence, important to address with special emphasis in a longitudinal setting like ours.
Based on current knowledge concerning the consequences of the COVID-19 pandemic on the adolescent population our hypothesis was that adolescent health and well-being deteriorated as an effect of the public measures that was imposed and that this was enhanced by low SEP. To study the potential consequences of the pandemic on Norwegian youth, we compared a cohort where data were collected before the pandemic outbreak (2017-19) and after the major close-down of the Norwegian society, combined with comparable cohort data collected in the same population a few decades earlier.
Methods
Study populations
The population-based Trøndelag Health Study (HUNT) was initiated in 1984–1986 (HUNT1) and consists of three subsequent waves (HUNT2-4) conducted every 11th year (24, 25). In the HUNT Study, inhabitants (aged 13 +) of Trøndelag County in the central part of Norway have been invited to participate. The data collection from adolescents, the Young-HUNT Study (26, 27), was first carried out in 1995–1997 with the Young-HUNT1 Survey (YH1, n = 8980). It consisted of data from 13–19-year-olds where the youngest were invited to a follow-up, Young-HUNT2 (YH2, n = 2427), in 2000–2001. Cross-sectional data from new adolescent cohorts were collected in 2006–2008, Young-HUNT3 (YH3, n = 8199), and in 2017-19, Young-HUNT4 (YH4, n = 8066). The surveys were conducted at secondary schools lower and upper. Pupils completed a questionnaire during one school hour. Specially trained personnel visited all the schools for interviews, clinical measurements and collection of biological samples (YH3 and YH4).
The HUNT COVID Study was started in 2021 with the main purpose of studying risk factors, severity, and the consequences of the nationwide control measures on public health. Data from adolescents, the Young-HUNT COVID Survey (YHC), was conducted in May/June 2021. All pupils from the upper secondary schools in the whole Trøndelag County (n = 32) aged 16 + were invited. An electronic questionnaire was sent out mainly to be answered in one school hour. Many questions were the same as in YH4, but we also included questions specifically concerning the COVID-19 pandemic. Due to teachers’ strikes, cancelled exams and the closing–down of certain schools, participation rates, 16–19-year-olds, only reached 35% (n = 5034). In the same geographical region as YH4, participation rate was 40% (n = 1778).
The study samples included in the present study consisted of both cross-sectional data of YH4 and YHC, and longitudinal data from YH4 to YHC and YH1 to YH2. The cross-sectional data from 16–19-year-olds in YH4 (n = 4347, 51% girls) and YHC (n = 2033, 59% girls) were used to compare trends. In addition, the youngest participants (13–15-year-olds) from YH4 (n = 3719, 51% girls) were compared to the oldest (16–19-year-olds) YH4 (n = 4347, 51% girls) to investigate the effects of age on the health measures used.
Longitudinal analyses to study changes from YH4 to YHC comprised 1565 participants (61% girls). The longitudinal YH1 to YH2 dataset, used as comparison as the follow-up years in the two are comparable, consisting of 2399 participants (54% girls). For study designs, see Fig. 1 and S1.
Fig. 1. Flow chart of the study populations, Young-HUNT4, YH4 (2017–2019) and Young-HUNT COVID, YHC (2021); cross-sectional datasets (age 16–19 years) and a longitudinal dataset consisting of 1565 individuals participating at age 13–15 years and in a follow-up four years later at age 16–19 years
To assess the potential impacts of the low participation rate in the follow-up in YHC, participants in both waves were compared descriptively at the age of 13–15 years at baseline participation (YH4) (data not shown).
Study variables
Socioeconomic position (SEP) was deduced from the variable self-perceived family affluence measured using the single question ‘How well off do you think your family is compared to most others” with three response options that were dichotomized into 1) High (“About the same as most others”,* “*Better financial situation) and 2) Low (Worse financial situation). Loneliness was measured by the single question ‘Are you lonely?’ rated on a 5-point scale was dichotomized into 1) not lonely (Very rarely/Rarely/Sometimes lonely) and 2) lonely (Often/Very often). General health was measured by the question ‘How is your health at the moment?’ rated on a 4-point scale ranging from “Poor” to 4 “Very good” and further dichotomized into 1) Good/Very good and 2) Poor/Very poor. The 10-item Hopkins Symptom Checklist (HSCL-10), a shorter version of the longer SCL-25 scales [26], assessed symptoms of anxiety and depression (mental distress). The HSCL-10 is a widely used tool for measuring psychological distress and symptoms of depression. Studies have shown that HSCL-10 has good internal consistency [27], which makes it a reliable tool for assessing psychological distress over time.
In our dataset, the internal consistency was satisfactorily with a Cronbach’s alpha of 0.92 in both YH4 and YHC. Each item was rated on a four-point Likert scale ranging from 1 (‘Not bothered’) to 4 (‘Very much bothered’). As with previous evaluations of the score [28], participants who had responded to more than eight of the ten questions were also included [29], (n = 154 YH4, and n = 37 in YHC). An average item score of ≥ 1.85 was used to identify symptoms of mental distress, following suggestions from Strand et al. [28].
The instrument ILC - Inventory of Life Quality [30] was used for measuring quality of life. The ILC-28-score is a reliable way of measuring life quality [30]. The translated Norwegian version used here is validated [31]. The score contains seven questions with answers on a 5-point Likert scale from “Very good” to “Very poorly”. The coded responses are summarized in a sumscore from 0 to 28, where 0 is high and 28 is low quality of life [30, 32]. In our dataset, the internal consistency was satisfactorily with a Cronbach’s alpha of 0.85 in both YH4 and YHC. ILC was also dichotomized with sex-specific upper 25% percentile cut-offs, ≥ 11 in girls and ≥ 8 in boys.
Statistics
Differences between the two study samples (YH4 and YHC) were tested by Pearson’s Chi-square tests for categorical variables and T-tests for continuous variables. The Friedman test was used for the longitudinal analyses. The results are shown in either means with standard errors or as proportions, number of participants and percentages. Two-tailed p-values < 0.05 were considered statistically significant. To explore the association between self-perceived family affluence (proxy for SEP) and various health outcomes and whether these differed pre- and into the pandemic, regression analyses were performed as binary logistic for the categorical outcomes (loneliness and general health) and linear regression for continuous outcomes (mental distress and life quality). These were performed adjusted for sex and age (Model 1) and in addition for survey participation (YH4 and YHC) (Model 2). Estimated effects are presented as Odds ratios (ORs) and standardized betas (Bs), both with 95% confidence intervals and p-values. Difference between YH4 and YHC concerning SEP was additionally tested by calculating prevalence ratios and differences. To analyse drop-off statistics, YH4 participants that were invited but did not take part in the YHC follow-up (830 boys and 703 girls) where compared to the ones that did participate. Statistically, boys did not differ, but the non-participant girls reported slightly lower life quality (measured with ILC) at YH4 than their peers. To confirm our findings in the longitudinal analyses, we additionally used STATA specifying random effects panel models to examine changes in outcomes across survey waves and between sexes, including interaction terms for wave and sex. Analyses were restricted to participants who participated in both YH4 and YHC, and standard errors were clustered at the individual level. For self-perceived family affluence, loneliness and self-reported general health, we applied logistic regression (xtlogit) and report predicted probabilities (as percentages) using the margins postestimation command. For HSCL-10 and ILC, we used linear regression (xtreg) and estimated marginal means using the margins command. To assess sex-specific changes from YH4 to YHC, we used the lincom command. These analyses were run in two models where the second was adjusted for time-varying age.
Results
Girls participated in higher rates compared to boys in YHC (59%) in contrast to YH4 (51%), and the adolescents were slightly older, 17.7/17.8 and 17.5 years, YHC and YH4 respectively (Table 1). In both surveys, the prevalence of loneliness, poor general health, mental distress and life quality were higher in girls than in boys. Loneliness was more prevalent in YHC compared to YH4 in both boys and girls (8.4% vs. 11.2% in boys and 16.9% vs. 20% in girls), which represent a negative change of 2.8% in boys and 3.1% in girls. Interestingly, only boys and not girls reported poorer metal health from pre- to-pandemic conditions (Table 1; Fig. 2). This represented an increase in the HSCL-10 sumscore of 1.12 units. Perception of SEP (self-perceived family affluence) seemed to be unchanged comparing pre-pandemic with pandemic data (Table 1).
Table 1. Characterisation and sex-stratified comparison of the Young-HUNT4, YH4 (2017–2019) and Young-HUNT COVID, YHC (2021) cross-sectionsVariablesYH4YHCP value YH4YHCP* value Boys (n = 2135)Boys (n = 828)Girls (n = 2212)Girls (n = 1205)Age: Mean, SD17.5 (1.0)17.7 (0.9)< 0.00117.5 (0.9)17.8 (0.9)< 0.001Family affluence: Low, n (%)176 (8.4)80 (9.7)0.252244 (11.1)140 (11.7)0.648Loneliness: Often/Very often, n (%)171 (8.4)90 (11.2)0.021362 (16.9)237 (20)0.025General health: Poor/Very poor, n (%)286 (13.5)108 (13.1)0.758455 (20.7)237 (19.7)0.493HSCL-10 sumscore, SD14.24 (5.0)15.36 (6.0)< 0.00119.46 (7.4)19.6 (7.1)0.536ILC sumscore, SD5.65 (4.2)5.84 (4.4)0.3697.99 (4.6)8.32 (4.8)0.073T-test for continuous and Pearson Chi square for categorical variables. Missing in YH4: Family affluence (self-perceived) (n = 60), Loneliness (n = 165), General health (n = 31), HSCL (n = 284), ILC (n = 403). Missing in YHC: Family affluence (self-perceived) (n = 10), Loneliness (n = 43), General health (n = 4), HSCL (n = 83), ILC (n = 563).
Fig. 2. Proportions (%) of participants reporting loneliness, poor general health, poor life quality and mental distress in the two cross-sections: Young-HUNT4, YH4 (2017–2019) and Young-HUNT COVID, YHC (2021) in boys and girls. * P value < 0.05, ** P value < 0.001 indicating statistically significant difference between YH4 and YHC
In a combined YH4/YHC dataset, regression analyses demonstrated that low SEP negatively affected all the selected outcome variables (Table S1). To explore whether the impact of SEP on health and well-being changed during the pandemic, sex-stratified prevalence ratios were calculated (Table S2). In the high SEP group, the prevalence of poor general health and life quality stayed unchanged in boys and nearly unchanged in girls, while the other two outcomes deteriorated. In the low SEP group, all the outcomes worsened in boys, while loneliness was the only one that developed adversely in girls (Fig. 3).
Fig. 3. Sex-specific prevalence of loneliness, poor general health, mental distress and poor life quality in the Young-HUNT4, YH4 (2017–2019) and Young-HUNT COVID, YHC (2021) cross-sections stratified on socioeconomic position (SEP - family affluence). Lonely (Often/Very often), Poor mental health (Poor/Very poor), Mental distress (HSCL-10 ≥ 1.85), Poor life quality (ILC, sex-specific 25% upper percentile cut-offs; ≥ 8 in boys and ≥ 11 in girls)
Following the younger adolescents (13–15-year-olds) longitudinally (from 2017 to 2019 to May/June 2021) displayed a different pattern than the one observed comparing the cross-sections (YH4 and YHC). In both sexes, self-reported low family affluence (4.7–8.1% in boys and 6.9–10.8% in girls), loneliness (5.5–9.0% in boys and 12.1–20.4% in girls) and mental distress (HSCL-10 caseness) (14.3–24.3% in boys and 34.5–52.0% in girls) increased. Poorer health (11.6–19.5%) and lower life quality (ILC) (mean (SD) 7.3 (4.6) to 8.36 (4.8)) were only observed in girls (Table 2).
Table 2. Characterisation and sex-stratified comparison of the Young-HUNT4, YH4 (2017–2019) and Young-HUNT COVID, YHC (2021) longitudinal dataset (n = 1565)VariablesBoys (n = 605)Girls (n = 960)YH4YHCP value YH4YHCP* value Age: Mean, SD14.6 (1.0)17.8 (0.9)14.6 (1.0)17.9 (0.9)Family affluence: Low, n (%)28 (4.7)49 (8.1)0.00666 (6.9)103 (10.8)< 0.001Loneliness: Often/Very often, n (%)32 (5.5)53 (9.0)0.024113 (12.1)192 (20.4)< 0.001General health: Poor/Very poor, n (%)64 (10.7)69 (11.4)0.513111 (11.6)187 (19.5)< 0.001HSCL-10 sumcore, SD14.00 (6.9)15.43 (5.9)< 0.00117.66 (6.9)20.48 (7.4)< 0.001ILC sumscore, SD5.47 (4.2)5.84 (4.4)0.1267.30 (4.6)8.36 (4.8)< 0.001Friedman test. Missing: Family affluence (self-perceived) (n = 20), Loneliness (n = 47), General health (n = 13), HSCL-10 (n = 77), ILC (n = 116)
To confirm and examine these results, additionally analyses examining changes across survey waves (YH4 and YHC) and between sexes, including interaction terms for wave and sex specifying random effects panel models, were performed. The results (Model 1) agreed very well with our previous findings, except for boys reporting poorer life quality (ILC) over time (see Table S3).
The observed discrepancy between the YH4 compared to the YHC cross-sections with the YH4-follow-up longitudinal sample could be due to age, as older adolescents tend to report more adverse health than younger adolescents do. To investigate this, differences in the younger and older age groups (13–15 vs. 16–19-year-olds) of the YH4 (total sample, n = 8066) was explored (Table S4). As presumed, we could confirm that in both sexes older compared to younger adolescents reported more loneliness, poorer general health, and higher mental distress. These findings were confirmed in Model 2 using random effects models adjusting for the variation in age due to time between YH4 and YHC (see Table S3).
In addition, the same age-related trend of adverse self-reported health was seen when comparing longitudinal data from an earlier Young-HUNT follow-up survey (n = 2399); baseline in 1995-97 (YH1) with follow-up four years later in 2000-01(YH2) (see FigS1 and Table S5). For the earlier Young-HUNT survey dataset (YH1 with follow-up in YH2), adolescents in the age range 16–19 years in YH1 (not participating in the YH2 follow-up) was compared to YH2 participants to evaluate differential trends over time in that five-year period. In general, no adverse developments were observed concerning loneliness, general and mental health, although girls were slightly lonelier in 1995–1997 (YH1), than in 2000–2001 (YH2) (see Fig S2).
Discussion
Most studies have shown that health protection efforts during the COVID-19 pandemic such as repeated quarantine, confinement and lockdowns have negatively affected especially mental health in children and adolescents [33]. Even so, countries and geographical regions were subject to variations in the capacity to handle the situation and strictness in measurements, which would affect the populations differently. Norway represents a wealthy society with well-organized social benefit arrangements; hence restrictions were most probably less intrusive compared to some of the other populations which other studies were based on. In addition, our study population inhabit a rural area in Norway not as densely populated as the ones represented in many other COVID-19 focused studies.
In our study, data from the same region in Norway were collected pre-pandemic (2017–2019) and again well into the pandemic (May/June 2021) which gave us the unique possibility of studying factors related to the pandemic in the same adolescent population over time. The main findings of our study based on primarily two cross-sections of 16–19-year-olds living in the same area previously and under the COVID-19 pandemic were generally that the adolescents were not affected as negatively as could be expected; general health, quality of life and the adolescents’ perception of family affluence seemed to have stayed unchanged. The rise in loneliness observed also before the pandemic, however, seemed to have continued into the pandemic. Interestingly, only boys and not girls reported poorer mental health from the time before the pandemic compared to into the pandemic, which is the opposite of what others have shown and deviate from the negative trends identified before the pandemic where girls compared to boys reported the most adverse development [9, 10, 34].
In contrast to the findings in the two cross-section, adverse general and mental health, quality of life and loneliness were identified longitudinally at the two time points pre-pandemic (2017–2019) and four years later into the pandemic at follow-up (May/June 2021) in a dataset consisting of 1565 individuals. Independent of the pandemic, the same negative development was observed in an earlier Young-HUNT based longitudinal dataset from 1995 to 1997 with follow-up in 2000–2001. Our suggestion is that the adverse health developments seen in the longitudinal sample spanning the period pre-pandemic into the pandemic is not a result of the pandemic restrictions, but rather a consequence of the increase in age from early until later adolescence as have been evident from other longitudinal studies [23, 35].
There has been a constant rise in loneliness observed globally over the last 20 years among young people with special emphasis on females [11]. The same trend has been identified in Norway [36, 37]. Young individuals are especially vulnerable to loneliness as they are in a state of social, psychosocial and cognitive transition from childhood to adulthood [38]. The increased loneliness prevalence causes public health concerns, as it is associated with risk factors such as suicidal behaviour [39, 40], social anxiety and depression [41] as well as future adult psychological illness and poor health outcomes [42]. It is therefore of immense importance to investigate whether the restrictions during the pandemic gave further rise in loneliness, with the associated adverse consequences for health and well-being. There is a suggestion that this negative trend is linked to the parallel rise in digital media usage such as social media and smart phones [11] which seems to have been further strengthened during the COVID-19 pandemic [43–45].
In our study, loneliness was more prevalent during the pandemic compared to prior to the pandemic in both sexes. This is in line with another Norwegian study, which show that loneliness had increased linearly from 2014 into the pandemic in 2021 [20]. Contrary to this, Hansen et al., identified no additional adverse change in loneliness during the pandemic in young Norwegian adults (18–24 years [46]. This was suggested to be because adolescents’ relationships with parents and peers during the pandemic did not seem to deteriorate [20].
In a recent review of studies concerning mental health in Europe during the COVID-19 pandemic, a general increase in mental health problems related to the pandemic was observed [47–49], although the findings are mixed [33]. By late 2020, i.e. after the most intrusive lock-down period, the increase appeared to have slowed down probably due to less fear and uncertainty amongst people. In our study, one of the most interesting findings was that only boys and not girls reported poorer mental health from the time before the pandemic compared to June 2021. This is in disagreement with the findings from a Finish study [50] and other Norwegian studies [18, 20] where mental distress seemed to worsen more in girls compared to boys. These discrepancies despite common Nordic conditions presumably being quite homogenous may be due to lack of total comparability concerning degree of urbanity. As mentioned, the population of the northern part of Trøndelag representing the sample in our study lack large cities, whilst the other Norwegian sample referred to [20] is nationally representative; hence with more participants inhabiting urban and more densely populated areas. A study that nicely describes the impact of different lockdown trajectories is the one by Meyer and colleagues where data are collected from two Australian states, Victoria, and Queensland [51].
We found based on the cross-sectional comparison of the 16–19-year-olds pre- and under the COVID-19 pandemic that general health, quality of life and the adolescents’ perception of family affluence seemed to have stayed unchanged. This could be because the restrictions in general did not have such negative effects on health as would be expected, or that the most stringent restrictions had been lifted at the point of data collection (May/June 2021) and conditions had normalised. As shown in a Dutch study, levels of loneliness, general mental health and life satisfaction declined initially in the pandemic but then improved to previous levels when restrictions were more relaxed [52]. This has also been shown by others who have suggested that the decline is a result of increased resilience in the population who adapted to the situation [53] and also were influenced by the positive effects of collective solidarity [54].
The fact that general health and life satisfaction stayed unchanged probably also depended on the adolescents perceiving their household financial situation to be the same as before. Financial decline related to the pandemic has in previous studies been shown to have negative impacts on physical and mental health in adolescents [55, 56], whereof several demonstrate that girls’ mental health was more adversely affected than boys’ in more vulnerable socioeconomic situations during the pandemic [57, 58].
In general, girls seem to be more prone to develop mental health problems than boys and factors influencing this are suggested to involve imposed expectations, social roles [59] and stronger stress reactivity [60]. Even if the proportion of girls compared to boys were shown to report adverse health and well-being generally, girls in our study did not develop negatively in the COVID-19 pandemic period. In fact, girls in the low SEP group seemed to be better off than before the pandemic. Family support and school contentment is important for mental health and well-being [61] and school pressure and coping in daily life are causes of poor life satisfaction and mental health [62, 63], also pinpointed by many adolescent girls themselves in Norway. As the effect of school pressure most probably changed in the pandemic period, it is tempting to speculate on the potential positive influence on girls this may have had. In a British survey, one-third of the students (aged 8–18) reported improvement in their mental wellbeing during the first COVID-19 lockdown and these were more likely than their peers to report improvement concerning factors such as school, relational, and lifestyle [6]. The authors suggest the reduction in school stress or learning systems during the pandemic to be better suited for some. Another issue interesting to emphasise related to our findings is the worrying trend of school refusals and “flight” from public schools among children and adolescents in Norway which has increased after the pandemic [64] and the mechanisms related to this [65]. Even if the pandemic resulted in disadvantages such as enhanced outsideness and reduced social skills [64], it is tempting to speculated whether life outside the school atmosphere also were beneficial for some adolescents.
In conclusion, our study indicate that the pandemic did not lead to a decline in the overall health and quality of life in adolescents, except for the increase in loneliness in both sexes and mental distress among boys. In general, girls appeared to cope better than boys, with health and life quality even showing improvement among girls from families with lower socioeconomic position. Understanding the contextual factors that contributed to this positive development and finding ways to sustain this situation beyond the pandemic is crucial for preventing further deterioration of mental health and well-being among adolescents in the future.
Strengths and limitations
The major strength of this study is the ability to compare the situation concerning adolescents’ health and well-being prior to and into the pandemic in the same population. The HUNT Study is a large population-based study largely representative of Norwegians [66, 67], although it does not include large city inhabitants. The population is relatively homogenous, with a low migration rate. Nearly everyone attends the same public schools and benefits from the same welfare and public health services although it may vary marginally between municipalities. The observed negative mental health and loneliness trends [9, 37] agree with both national and global circumstances [11, 20, 68].
There are several limitations to the study, one being that data is based on self-report. Another drawback is the low participation rate in the Young-HUNT COVID Survey. As the variations in the school’s participation rates were due to the randomness of teachers that were on strike, regional lockdowns, and flexible times at school because of cancelled exams, reduced representativeness is not likely an important issue. In addition, confirming main coincident characteristics in the baseline study (YH4) age-groups 13–15 years, comparing with non-participants in the follow-up (Young-HUNT COVID), precluded the presence of selection bias and strengthened our findings. In our study, the cut-off level defining statistically significant findings was set to p-value < 0.05. However, if we were to compensate for potential type I errors due to multiple hypotheses tested, a cut-off value could have been set to 0.01 (Bonferroni Corrections accounting for five main hypotheses 0.05/5 = 0.01, α_new_ = α_original_/n). This would result in the observed increase in loneliness from Young-HUNT4 to Young-HUNT COVID not being present anymore. However, the increased prevalence concerning loneliness is still of interest as our study is primarily a descriptive one.
Anyhow, the influence due to variation in lockdown measures would be difficult to precisely account for as different regions and municipalities implemented different types of lockdown measures. At some points nationwide lockdown were declared, whereas some regions advocated for social distancing and limitations on gatherings rather than legally enforcing a lockdown.
In this study, SEP was measured by a question concerning self-perceived family affluence. Most studies using subjective SEP demonstrate a positive impact of higher SEP on better health outcomes in youth [69]. Interestingly, this association has also been shown to be reciprocal, i.e. that mental distress could negatively affect the subjective perception of SEP [70], but this direction of association depends on the health outcome. Concerning self-rated health for instance, the observed direction of association seems to be that SEP affects later health and not vice versa [71]. An alternative measure of SEP could have been the objective measure of parental education, which would in our case require family linkage through Statistics Norway. Using parental or family SEP as a proxy for adolescent SEP in predicting health outcomes may however be debatable since adolescents’ own perception of social status seem to impact health the most [72]. Even so, based on their meta-analysis findings, Quon and McGrath recommend incorporating both subjectively and objectively measured SEP in combination to better understand mechanisms underlying health disparities.
A limitation in our study could be that such a complex experience as loneliness was assessed by a single question both in YH4 and YHC. Although, it has been shown that single-item measures are reliable, correlate highly with multi-item scales and are useful measures of loneliness [73].
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Twenge JM. Increases in Depression, Self-Harm, and, Suicide Among US (2020) Adolescents After 2012 and Links to Technology Use: Possible Mechanisms. Psychiatr Res Clin Pract.;2(1):19–25. Epub 20200909. 10.1176/appi.prcp.20190015. Pub Med PMID: 36101887; Pub Med Central PMCID: PMCPMC 917607010.1176/appi.prcp.20190015 PMC 917607036101887 · doi ↗ · pubmed ↗
- 2WHO (2022) COVID-19 pandemic triggers 25% increase in prevalence of anxiety and depression worldwide. https://www.who.int/news/item/02-03-2022-covid-19-pandemic-triggers-25-increase-in-prevalence-of-anxiety-and-depression-worldwide [updated 2 March]PMC 999805735414629 · pubmed ↗
- 3von Soest T, Kozák M, Rodríguez-Cano R, Fluit DH, Cortés-García L, Ulset VS et al (2022) Adolescents’ psychosocial well-being one year after the outbreak of the COVID-19 pandemic in Norway. Nat Hum Behav.;6(2):217–28. Epub 20220120. 10.1038/s 41562-021-01255-w. Pub Med PMID: 3505864410.1038/s 41562-021-01255-w 35058644 · doi ↗ · pubmed ↗
- 4Guazzini A, Pesce A, Gino F, Duradoni M (2022) How the COVID-19 Pandemic Changed Adolescents’ Use of Technologies, Sense of Community, and Loneliness: A Retrospective Perception Analysis. Behav Sci (Basel).;12(7). Epub 20220713. 10.3390/bs 12070228. Pub Med PMID: 35877298; Pub Med Central PMCID: PMCPMC 931152810.3390/bs 12070228 PMC 931152835877298 · doi ↗ · pubmed ↗
- 5Potrebny T, Nilsen SA, Bakken A, von Soest T, Kvaløy K, Samdal O et al (2024) Secular trends in mental health problems among young people in Norway: a review and meta-analysis. Eur Child Adolesc Psychiatry. Epub 20240216. 10.1007/s 00787-024-02371-4. Pub Med PMID: 3836339110.1007/s 00787-024-02371-4PMC 1180584638363391 · doi ↗ · pubmed ↗