The effect of alienation on depression among Chinese caregivers of children with autism: family resilience as a moderator
Lin Zheng, Xin Liu

TL;DR
Chinese caregivers of children with autism experience higher depression due to alienation, but family resilience can reduce this risk.
Contribution
This study identifies specific family resilience factors that moderate the link between alienation and depression in Chinese caregivers of children with autism.
Findings
Alienation is strongly linked to depression in caregivers of children with autism.
Family resilience dimensions like communication and social support reduce the impact of alienation on depression.
Faith/spiritual beliefs also act as a buffer against depression caused by alienation.
Abstract
Caregivers of children with autism spectrum disorder (ASD) in China often encounter stigma and social isolation, which may heighten alienation and increase depression risk. Family resilience—the strengths and resources within the family system, may help protect caregiver mental health. This study examined the association between alienation and depression among Chinese caregivers of children with ASD and tested whether family resilience moderates this relationship. A cross-sectional survey of 205 caregivers in Jilin Province assessed alienation, depressive symptoms, and family resilience using validated Chinese instruments. Exploratory factor analysis was used to confirm the structure of the Family Resilience (FaRE) Questionnaire for this population. Hierarchical regression analyses examined the association between alienation and depression and the moderating effects of family…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
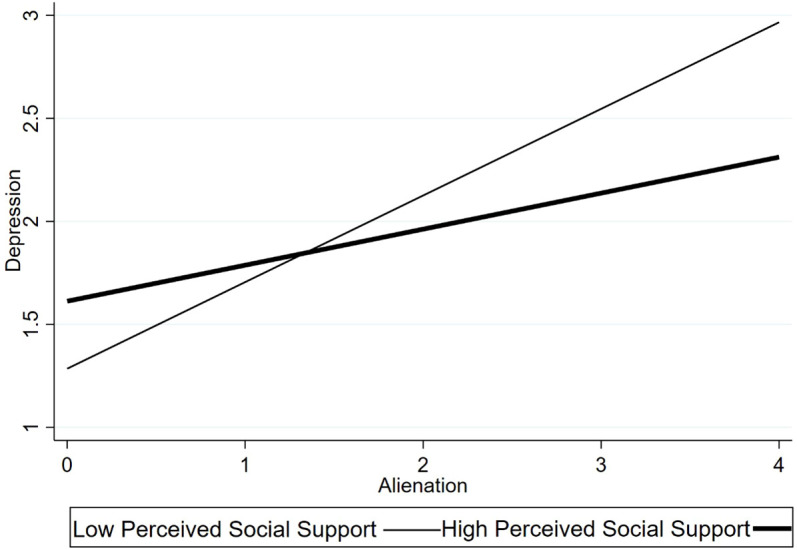 Figure 1
Figure 1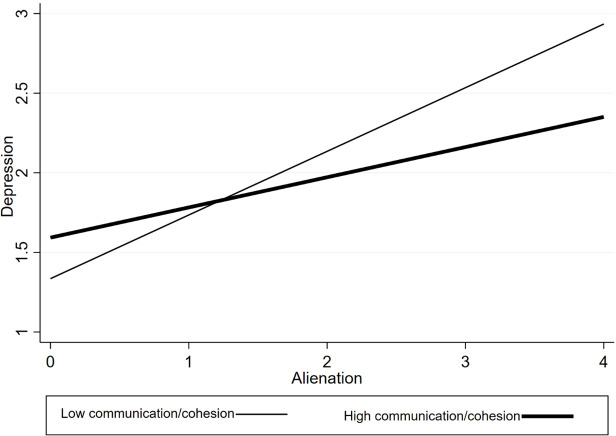 Figure 2
Figure 2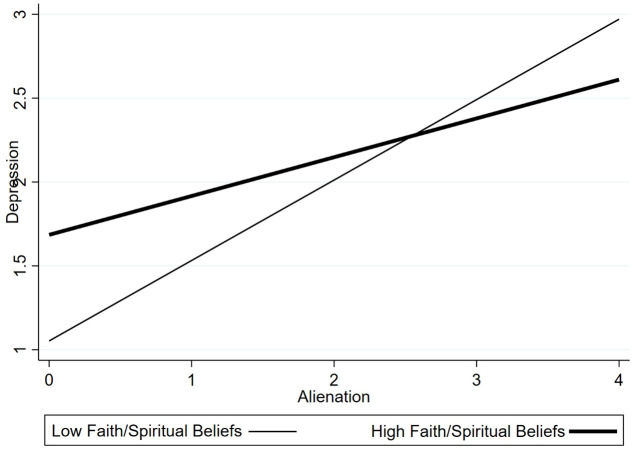 Figure 3
Figure 3| Test | Value | Criterion | |
|---|---|---|---|
| Kaiser–Meyer–Olkin (KMO) Measure of Sampling Adequacy | 0.953 | ≥ 0.60 | |
| Bartlett’s Test of Sphericity | Approx. Chi-square | 3948.813 | — |
| df | 190 | — | |
| p-value | <.001 | <.05 | |
| Continuous variables | ||||||
|---|---|---|---|---|---|---|
| Variable | Min | Max | M | SD | Skewness | Kurtosis |
| Age | 25 | 76 | 44.688 | 11.647 | .844 | 2.840 |
| Depression (CES-D mean score) | 1.000 | 3.905 | 2.129 | .859 | .286 | 1.759 |
| Alienation | 1.067 | 3.733 | 2.411 | .715 | -.019 | 2.038 |
| Family resilience (Communication/Cohesion) | 1.000 | 4.000 | 2.628 | .724 | -.331 | 2.463 |
| Family resilience (Social Support) | 1.000 | 4.000 | 2.750 | .672 | -.574 | 2.769 |
| Family resilience (Family Coping Ability) | 1.000 | 4.000 | 2.697 | .658 | -.498 | 3.290 |
| Family resilience (Faith/Spirituality) | 1.000 | 4.000 | 1.013 | .988 | .565 | 2.482 |
| Categorical variables | ||||||
| Variable | Category | N (%) | ||||
| Gender | Female | 165 (80.5%) | ||||
| Male | 40 (19.5%) | |||||
| Education | Junior high school or below | 100 (48.8%) | ||||
| High school or above | 105 (51.2%) | |||||
| Chronic illness | Yes | 88 (42.9%) | ||||
| No | 117 (57.1%) | |||||
| Variable | Group |
| Alienation | Depression | ||||
|---|---|---|---|---|---|---|---|---|
| M | SE | t/F | M | SE | t/F | |||
| Gender | Male | 40 | 2.129 | .124 | –.641 | 2.172 | .111 | –2.007* |
| Female | 165 | 2.217 | .060 | 2.416 | .049 | |||
| Age group | 20s | 5 | 2.057 | .801 | 1.27 | 2.480 | .511 | .97 |
| 30s | 79 | 2.152 | .790 | 2.361 | .667 | |||
| 40s | 59 | 2.350 | .768 | 2.467 | .626 | |||
| 50s | 34 | 2.010 | .770 | 2.198 | .639 | |||
| ≥ 60 | 28 | 2.272 | .694 | 2.398 | .712 | |||
| Education | Middle school or below | 100 | 2.330 | .074 | 2.406* | 2.496 | .068 | 2.760** |
| High school or above | 105 | 2.075 | .076 | 2.247 | .059 | |||
| Chronic illness | No | 117 | 2.064 | .073 | -2.992** | 2.268 | .058 | –2.555* |
| Yes | 88 | 2.379 | .076 | 2.502 | .071 | |||
| Variable | Group |
| Communication/Cohesion | Social support | Family coping ability | Faith/Spirituality | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SE | t/F | M | SE | t/F | M | SE | t/F | M | SE | t/F | |||
| Gender | Male | 40 | 2.763 | .145 | 1.573 | 2.871 | .125 | 1.750 | 2.925 | .098 | 2.709** | 1.381 | .080 | –.216 |
| Female | 165 | 2.512 | .066 | 2.626 | .063 | 2.612 | .061 | 1.402 | .049 | |||||
| Age group | 20s | 5 | 2.1 | .778 | 1.21 | 2.567 | .401 | .82 | 2.933 | .279 | .73 | 1.4 | .652 | .83 |
| 30s | 79 | 2.643 | .856 | 2.673 | .761 | 2.65 | .718 | 1.307 | .492 | |||||
| 40s | 59 | 2.415 | .838 | 2.573 | .801 | 2.571 | .849 | 1.492 | .642 | |||||
| 50s | 34 | 2.706 | .84 | 2.882 | .858 | 2.765 | .815 | 1.417 | .743 | |||||
| ≥ 60 | 28 | 2.542 | .955 | 2.655 | .923 | 2.798 | .699 | 1.429 | .623 | |||||
| Education | Middle school or below | 100 | 2.493 | .087 | –1.095 | 2.585 | .086 | –1.543 | 2.597 | .081 | –1.398 | 1.565 | .069 | 3.978*** |
| High school or above | 105 | 2.625 | .083 | 2.759 | .072 | 2.746 | .069 | 1.238 | .045 | |||||
| Chronic illness | No | 117 | 2.554 | .082 | –.132 | 2.668 | .073 | –.12 | 2.755 | .074 | 1.812* | 1.397 | .055 | –.003 |
| Yes | 88 | 2.57 | .089 | 2.682 | .088 | 2.564 | .075 | 1.398 | .065 | |||||
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| Gender | 1 | ||||||
| Age | -.179* | 1 | |||||
| Education level | -.111 | -.131 | 1 | ||||
| Chronic illness status | -.095 | .035 | -.100 | 1 | |||
| Alienation | .148 | -.013 | -.191* | -.178* | 1 | ||
| Depression | .046 | .014 | -.167** | -.203** | .623*** | 1 | |
| Family resilience | -.140 | .033 | .103 | -.018 | -.437*** | -.314*** | 1 |
| Predictor | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| B (SE) | β | t | B (SE) | β | t | |
| Gender (female) | .092 (.137) | .047 | .67 | –.078 (.111) | –.040 | –.70 |
| Age | –.000 (.005) | –.004 | .05 | .000 (.004) | .006 | .10 |
| Education (high vs. low) | –.219 (.108) | –.142* | –2.03 | –.071 (.088) | –.046 | –.80 |
| Chronic illness (no vs. yes) | .300 (.107) | .193** | 2.80 | .135 (.088) | .087 | 1.54 |
| Alienation | .712 (.067) | .605*** | 10.56 | |||
| R² | .065 | .400 | ||||
| Adj. R² | .046 | .386 | ||||
| ΔR² | .340*** | |||||
| F | 3.47*** | 26.61*** | ||||
| Predictor | Communication & cohesion | Social support | Family coping ability | Faith/Spiritual beliefs | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B (SE) | β | t | B (SE) | β | t | B (SE) | β | t | B (SE) | β | t | |
| Gender (female) | –.045 (.108) | –.023 | –.42 | .061 (.112) | .031 | .55 | –.079 (.112) | –.041 | –.71 | –.075 (.109) | –.039 | –.69 |
| Age | .000 (0.005) | .009 | .09 | .000 (.004) | –.001 | –.02 | .000 (.004) | –.002 | –.02 | .000 (.004) | –.001 | –.02 |
| Education (high vs. low) | –.077 (0.105) | –.048 | –.73 | –.057 (.087) | –.037 | –.65 | –.057 (.087) | –.035 | –.60 | –.057 (.087) | –.035 | –.60 |
| Chronic illness (no vs. yes) | .111 (.086) | .071 | 1.29 | .112 (.087) | .072 | 1.28 | .128 (.092) | .096 | 1.39 | .150 (.096) | .109 | 1.73 |
| Alienation | .661 (.072) | .561*** | 9.14 | .692 (.072) | .588*** | 9.65 | .672 (.071) | .572*** | 9.48 | .705 (.067) | .599*** | 10.60 |
| Communication & Cohesion | –.079 (.053) | –.088 | –1.47 | |||||||||
| Social Support | –.043 (.057) | –.045 | –.77 | |||||||||
| Family Coping Ability | –.089 (.060) | –.088 | –1.49 | |||||||||
| Faith/Spiritual Beliefs | .023 (.073) | .018 | .32 | |||||||||
| Communication × Alienation | –.254 (.068) | –.204*** | –3.72 | |||||||||
| Social Support × Alienation | –.172 (.072) | –.133* | –2.40 | |||||||||
| Family Coping × Alienation | –.115 (.074) | –.086 | –1.55 | |||||||||
| Faith × Alienation | –.365 (.128) | –.156** | –2.84 | |||||||||
| R² | .443 | .419 | .414 | .424 | ||||||||
| Adj. R² | .423 | .398 | .383 | .404 | ||||||||
| F | 22.33*** | 20.27*** | 19.87*** | 20.74*** | ||||||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFamily and Disability Support Research · Resilience and Mental Health · Parental Involvement in Education
Introduction
1
Autism spectrum disorder (ASD) has shown a steady rise worldwide. In the United States, recent surveillance data indicate that about 1 in 36 eight-year-old children meets diagnostic criteria for ASD, reflecting a continued upward trend (1). China has reported similar increases; contemporary reviews estimate that approximately 0.26–1% of the population may be individuals with ASD, and newer meta-analyses suggest that prevalence among Chinese children approaches international levels (2, 3). As diagnoses rise, increasing numbers of families must undertake long-term caregiving, elevating concerns regarding the well-being of caregivers of children with ASD.
Terminology note: We use person-first language (e.g., “children with ASD”) throughout to emphasize individuals rather than diagnoses, consistent with bias-free and inclusive language guidance for scholarly writing (4). We acknowledge that preferences vary and that some autistic individuals and communities prefer identity-first language; future work should follow participants’ self-identified terminology where feasible.
From a diversity and equity perspective, caregivers of children with ASD in China remain under-represented in the international literature and may face structural barriers such as stigma and constraints in access to supports and services (5, 6). These inequities may place additional strain on families with limited resources or restricted access to formal services, increasing risks of social exclusion and poor mental health. Accordingly, examining alienation and resilience among Chinese caregivers can inform equity-oriented strategies to address inequities in caregiver mental health (7).
Against this backdrop of structural barriers and uneven support, caregivers of children with ASD frequently experience considerable psychological distress. Recent studies in China and abroad show high rates of stress, anxiety, and depression among these caregivers (8–15). Beyond intensive daily caregiving demands, many caregivers confront persistent stigma rooted in misconceptions about ASD (16, 17). Such stigma often takes the form of blame or disapproval, contributing to experiences of affiliate stigma or social exclusion (5, 18–23). Repeated exposure to stigmatizing interactions can foster social withdrawal and a sense of alienation, characterized by perceived disconnection from society and interpersonal relationships. This alienation may compound the emotional burden of caregiving and heighten vulnerability to deteriorating mental health.
A growing body of research links alienation and related constructs—such as internalized stigma, perceived discrimination, and chronic loneliness—to adverse psychological outcomes. Evidence from recent Chinese studies indicates that feelings of alienation are associated with elevated depressive symptoms even after accounting for other stressors (24). Among caregivers of individuals with developmental disabilities, stigma-related alienation similarly predicts poorer well-being and increased depression (25). Given that depressive symptoms affect an estimated 40–50% of caregivers of children with ASD worldwide (26), understanding how alienation contributes to depression is an urgent research priority.
Not all caregivers exposed to adversity experience poor mental health. Many demonstrate resilience when navigating the challenges of raising children with ASD. Family resilience refers to the processes through which families withstand, adapt to, and recover from stress (27). Conceptually, different dimensions of family resilience may buffer the psychological impact of alienation through distinct mechanisms. For example, communication and cohesion within the family may reduce the emotional consequences of alienation by fostering emotional connectedness and shared understanding, whereas perceived social support can counteract social withdrawal by extending supportive resources beyond the immediate family. Faith or spiritual beliefs may further promote meaning-making and optimism, helping caregivers cope with marginalizing experiences. Prior research has consistently shown that higher levels of family resilience are associated with better psychological adjustment among caregivers of children with ASD (28, 29).
This study examines whether family resilience mitigates the impact of alienation on depression among caregivers of children with ASD in China. We hypothesized that alienation would be positively associated with depressive symptoms (H1) and that specific dimensions of family resilience would moderate this association by weakening the relationship between alienation and depression (H2). Clarifying these relationships can deepen understanding of both risk and protective processes and inform interventions aimed at reducing caregiver isolation and strengthening family resilience in educational and community contexts.
Methods
2
Participants and procedure
2.1
The participants were primary caregivers of children with ASD recruited from community organizations, rehabilitation centers, and parent support groups in Jilin Province, Northeast China. From a diversity and equity perspective, access to ASD-related services and supports may vary across settings, and caregivers may rely on different combinations of formal and informal resources. This recruitment strategy therefore captures caregivers navigating varying levels of service accessibility and social inclusion. This design helps contextualize alienation as an equity-relevant psychosocial experience linked to differential opportunities for support and participation. Between June and August 2023, a total of 205 caregivers aged 22–76 years completed structured questionnaires. Researchers collaborated with local administrators to identify and invite eligible participants.
Eligible participants were primary caregivers (parents or grandparents) of a child formally diagnosed with ASD who had at least three months of continuous caregiving experience. This criterion was used to ensure that caregivers had sufficient exposure to daily caregiving demands and had moved beyond the initial adjustment period, allowing for more stable assessments of psychosocial experiences. To further ensure inclusion of caregivers actively involved in daily care, those not currently co-residing with their child were excluded. Each family contributed one caregiver, defined as the individual primarily responsible for the child’s daily care.
Among the respondents, 80.5% were female caregivers, 19.5% were male caregivers. Most caregivers were middle-aged, with approximately 39% in their 30s and 29% in their 40s. Educational attainment was moderate: 48.8% had junior high school education or below, while 51.2% had at least a high school education. Nearly 43% reported one or more chronic health conditions.
Participants completed the survey either on paper or online after providing written informed consent. The survey required approximately 10–15 minutes to complete, and researcher assistance was available if needed. The study protocol was approved by the Institutional Review Board of Jeonbuk National University, South Korea (IRB2023-06-003-002), as part of the author’s doctoral research project at Jeonbuk National University, where the study was initiated and overseen during the author’s PhD training. Data were collected in China through collaborating community organizations and service agencies with administrative permission from site leaders. The present manuscript reports a secondary analysis of this previously collected dataset; no additional recruitment or data collection was conducted for the current study. Participation was voluntary and anonymous, written informed consent was obtained, and no identifying information was collected. Questionnaires were considered valid if they (a) contained no substantial missing data on key study variables (alienation, depression, and family resilience) and core covariates, and (b) showed no obvious internal inconsistencies in basic demographic information. Based on these criteria, 205 of the 220 returned questionnaires were retained for analysis.
Given the exploration nature of the moderation analyses, the sample size (N = 205) is comparable to that used in prior studies examining caregiver psychological outcomes using hierarchical regression approaches. Although no formal a priori or post hoc power analysis was conducted, the sample size was considered adequate for exploratory modeling with multiple covariates, and the findings should be interpreted with appropriate caution.
Measures
2.2
Depression
2.2.1
Caregiver depressive symptoms were assessed using the 20-item Center for Epidemiologic Studies Depression Scale (CES-D), Chinese version. Items measure the frequency of depressive symptoms (e.g., sadness, hopelessness, sleep disturbance) experienced during the past week on a 4-point scale ranging from 0 (“rarely or none of the time”) to 3 (“most or all of the time”). Higher scores indicate greater depressive symptoms.
Although the CES-D is commonly reported using a summed total score (range=0–60) and associated cutoff values in prior research, all analyses in the present study were conducted using mean item scores. This approach was adopted to ensure consistency across study measures and to facilitate interpretation in regression and moderation analyses. The Chinese version of the CES-D has demonstrated strong psychometric properties in prior studies (30; 31). In the present sample, internal consistency was excellent (Cronbach’s α = 0.95).
Alienation
2.2.2
Caregivers’ sense of alienation was measured using a revised Chinese version of the Generalized Social Alienation Scale (GSAS), adapted by Yang (32) based on Jessor’s conceptualization of alienation (33). The scale assesses perceived social disconnection, isolation, and powerlessness (e.g., “I feel like I don’t really belong in society”).
Items were rated on a 4-point Likert scale ranging from 1 (“strongly disagree”) to 4 (“strongly agree”), with higher scores indicating greater alienation. Mean item scores were used in all analyses. The revised adult version has demonstrated good psychometric properties in prior research on social estrangement and perceived discrimination (34). In the present study, the scale showed excellent internal consistency (Cronbach’s α = 0.94).
Family resilience
2.2.3
Family resilience was assessed using the Family Resilience Questionnaire (FaRE), originally developed by Faccio et al. (28) and translated and psychometrically validated in a Chinese sample (8, 35). The scale is grounded in a systemic resilience framework and assesses four theoretically distinct dimensions: (a) communication and cohesion, reflecting emotional connectedness and open family communication; (b) perceived social support, capturing both internal and external support resources; (c) family coping ability, indicating perceived competence in managing stress and adversity; and (d) faith/spiritual beliefs, reflecting shared belief systems and meaning-making processes. All items were rated on a 4-point Likert scale (1 = strongly disagree; 4 = strongly agree), with higher scores indicating greater family resilience.
Although a Chinese version has been validated (8), it has not been previously examined among caregivers of children with ASD; therefore, we conducted an exploratory factor analysis (EFA) to evaluate its factorial structure in the present sample. Bartlett’s test of sphericity was significant (χ² = 3948.81, p < 0.001), and the Kaiser–Meyer–Olkin (KMO) measure was 0.953, indicating excellent sampling adequacy. Principal axis factoring with varimax rotation was employed. Factors were retained based on eigenvalues greater than 1.0 and inspection of the scree plot.
Five items (Items 1, 8, 9, 10, and 17) were removed due to low factor loadings (< 0.63) or conceptual overlap. All retained items loaded strongly (≥ 0.63) on their intended factors and showed no substantial cross-loadings. The final 19-item solution preserved the original four-factor structure proposed by Faccio et al. The four subscales demonstrated strong internal consistency (Cronbach’s α = 0.88–0.92), and the overall scale showed excellent reliability (α = 0.96). The KMO and Bartlett’s test results are reported in Table 1.
Covariates
2.2.4
Several caregiver sociodemographic characteristics were included as covariates: gender (0 = male, 1 = female), age (years), education level (0 = junior high school or below, 1 = high school or above), and presence of a chronic health condition (0 = no, 1 = yes). These variables have been consistently associated with caregiver mental health outcomes in ASD research (29, 36) and were included to adjust for their potential confounding effects.
Data analysis
2.3
We first conducted descriptive analyses to summarize caregiver characteristics and the distributions of the main study variables. Independent t-tests and one-way ANOVAs were used to examine group differences in depression, alienation, and the family resilience subdimensions across key demographic categories (e.g., gender, education). Pearson correlations were then calculated among alienation, depression, and the resilience subdimensions to examine bivariate associations and assess potential multicollinearity. For descriptive purposes, an overall family resilience score was included in the correlation analyses to provide a general overview of bivariate associations. However, in the regression and moderation analyses, only the four resilience subdimensions were examined to avoid redundancy and multicollinearity and to maintain a clear focus on distinct family resilience processes.
To test the primary hypotheses, we estimated a series of hierarchical linear regression models. Depression was specified as the dependent variable and alienation as the main independent variable. Family resilience was examined as a moderator through separate moderated regression models for each of the four subdimensions (communication/cohesion, perceived social support, family coping ability, and faith/spiritual beliefs). No model was estimated for an overall resilience score, as the analytic focus was on the distinct dimensions.
Each regression analysis followed a three-model procedure. Model 1 included the control variables (caregiver gender, age, education, and chronic illness). Model 2 added the mean-centered main effects of alienation and the relevant resilience subdimension. Model 3 included the interaction term (Alienation × Resilience Subdimension). Mean-centering was used to reduce multicollinearity. Moderation effects were evaluated based on the significance of the interaction term and the change in R² from Model 2 to Model 3 (37).
For significant interactions, simple slope analyses were conducted to examine the association between alienation and depression at high and low levels of the moderator (± 1 SD from the mean). Significant interaction effects were also plotted for visualization (see Figures 1–3), and simple slope statistics are reported in the Results section.
Interaction between alienation and family communication/cohesion in predicting depression.
Interaction between alienation and perceived social support in predicting depression.
Interaction between alienation and faith/spiritual beliefs in predicting depression.
All analyses were performed using Stata 17.0. A two-tailed p < 0.05 was considered statistically significant. Multicollinearity diagnostics indicated no problematic collinearity among predictors (tolerance values > 0.70; variance inflation factors < 1.5). Regression assumptions were evaluated through inspection of residual-versus-fitted plots (linearity and homoscedasticity) and normal probability plots of standardized residuals, with no substantial deviations observed.
Results
3
Descriptive findings
3.1
Descriptive statistics for the study of variables and covariates are presented in Table 2.
Depression and alienation. Caregivers showed considerable variation in depressive symptoms. The mean CES-D item score was 2.13 (SD = 0.86), with higher values indicating greater depressive symptoms. Alienation levels were also relatively elevated to 2.41 (SD = 0.72), suggesting frequent experiences of social withdrawal or misunderstanding.
Family resilience. Across the four family resilience dimensions, mean scores were 2.63 for communication/cohesion, 2.75 for perceived social support, 2.70 for family coping ability, and 1.01 for faith/spiritual beliefs. Overall, caregivers reported moderate levels of family functioning across most domains, whereas faith/spiritual beliefs were notably lower on average. The subsequent results are summarized in Tables 3–5. The corresponding analyses are reported in Table 3, with additional results presented in Tables 4, 5.
Alienation as a predictor of caregiver depression
3.2
Alienation as a predictor of caregiver depression. Table 6 presents hierarchical regression models predicting caregiver depressive symptoms. In Model 1, which included only the control variables, the model explained a modest but statistically significant proportion of variance in depression (F (4, 200) = 3.47, p < 0.01, R² = 0.07). Caregivers with lower educational attainment and those with chronic illness reported higher levels of depressive symptoms, whereas gender showed a marginal association and age was not statistically significant.
In Model 2, the inclusion of alienation significantly improved model fit. Alienation was positively and significantly associated with depressive symptoms (p < 0.001), and the explained variance increased substantially relative to Model 1 (ΔR², p < 0.001), indicating that higher alienation was associated with higher levels of caregiver depression after adjusting for sociodemographic covariates.
Moderating effect of family resilience subdimensions
3.3
Moderation by family resilience subdimensions. Separate moderated regression models were estimated for each family resilience subdimension (Table 7). Across all models, alienation remained significantly associated with depressive symptoms. Significant interaction effects were observed for three subdimensions—communication/cohesion, perceived social support, and faith/spiritual beliefs—indicating that these family processes moderated the association between alienation and depression. In contrast, the interaction between alienation and perceived family coping ability was not statistically significant.
Resilience subdimensions
3.4
Communication and cohesion
3.4.1
The interaction between alienation and family communication/cohesion was statistically significant (β =–0.204, p <0.001). Simple slope analyses (Figure 1) indicated that the association between alienation and depressive symptoms was stronger among caregivers reporting lower levels of family cohesion (p < 0.001), whereas this association was weaker among those with higher cohesion (p< 0.05). These findings indicate that family communication and emotional cohesion moderate the association between alienation and caregiver depression.
Perceived social support
3.4.2
The interaction between alienation and perceived social support was statistically significant (β =–0.133, p <0.05). Simple slope analyses (Figure 2) indicated that the association between alienation and depressive symptoms was stronger at lower levels of perceived social support (p < 0.001), whereas this association was attenuated, though still positive, at higher levels of support (p= 0.01). These findings indicate that perceived social support moderates the association between alienation and depressive symptoms.
Perceived family coping ability
3.4.3
The interaction between alienation and perceived family coping ability was not statistically significant (β =–0.086, p = 0.22). Alienation remained significantly associated with depressive symptoms, whereas the interaction term did not reach statistical significance. These results indicate that perceived family coping ability did not moderate the association between alienation and caregiver depression.
Faith/spiritual beliefs
3.4.4
The interaction between alienation and faith/spiritual beliefs was statistically significant (β =–0.156, p <0.01). Simple slope analyses (Figure 3) showed that among caregivers reporting higher levels of faith/spiritual beliefs, the association between alienation and depressive symptoms was weak and not statistically significant (p > 0.10). In contrast, among caregivers with lower levels of faith/spiritual beliefs, alienation was significantly associated with higher depressive symptoms (p< 0.001). These findings indicate that faith/spiritual beliefs moderate the association between alienation and caregiver depression.
Summary
3.5
Across the four moderation models, three family resilience subdimensions—communication/cohesion, perceived social support, and faith/spiritual beliefs—significantly moderated the association between alienation and depressive symptoms. In contrast, perceived family coping ability did not show a significant moderating effect. Across all models, alienation remained significantly associated with caregiver depressive symptoms. The effects of the control variables were consistent with earlier models, with lower education and chronic illness associated with higher depressive symptoms, gender showing a marginal association, and age not significantly related to depression.
Discussion
4
This study examined how alienation relates to depressive symptoms among Chinese caregivers of children with ASD and whether specific components of family resilience mitigate this association. Consistent with the study hypotheses, alienation was strongly associated with higher levels of depressive symptoms, and three family resilience subdimensions—communication/cohesion, perceived social support, and faith/spiritual beliefs—demonstrated significant buffering effects. Together, these findings highlight alienation as a salient psychosocial risk factor associated with caregiver depression and underscore the importance of distinct family processes in shaping caregivers’ psychological adjustment within the present cultural context.
Consistent with prior research on stigma, social exclusion, and caregiver well-being, caregivers who reported higher levels of alienation also reported substantially higher depressive symptoms (24, 25, 38). Alienation reflects experiences of being misunderstood, marginalized, or socially excluded, and the internalization of such experiences may undermine emotional well-being by reducing perceived belonging and support. In the Chinese context, these associations may be shaped by uneven public understanding of ASD and by the social expectations placed on families, which can intensify caregivers’ sense of isolation while they manage demanding caregiving responsibilities. The present findings suggest that alienation is not merely a secondary burden but a central correlation of caregivers’ depressive symptoms.
A key contribution of this study lies in identifying specific dimensions of family resilience that moderate the association between alienation and depression. In line with our analytic focus, moderation effects were examined for each resilience subdimension rather than for an overall composite. Communication and cohesion showed the strongest buffering effect, indicating that families characterized by open communication and emotional connectedness may provide caregivers with supportive environments in which concerns can be shared and validated, thereby reducing the emotional impact of alienation (27, 39). Perceived social support similarly attenuated the alienation–depression association, suggesting that connections with extended family, peers, and community networks may compensate for feelings of social disconnection. Faith or spiritual beliefs constituted a third buffering dimension; shared belief systems and meaning-making processes may help caregivers reinterpret marginalizing experiences and sustain emotional equilibrium in the context of elevated alienation. These patterns are consistent with intervention- and practice-oriented literature suggesting that strengthening caregiver/family resilience and enhancing accessible support networks may improve caregiver adjustment and well-being (40–44).
In contrast, perceived family coping ability did not significantly moderate the relationship between alienation and depression. Coping efficacy may be more closely related to managing practical caregiving challenges than to buffering the relational and emotional dimensions of alienation. Additionally, the relatively low coping scores observed in this sample may have limited variability, reducing the likelihood of detecting interaction effects. These findings underscore that family resilience is multidimensional and that relational and meaning-oriented processes may be particularly relevant for caregivers’ emotional well-being.
Practical implications
4.1
The findings have several practical implications for practice and policy. Interventions aimed at reducing caregiver depression may benefit from explicitly addressing alienation through stigma-reduction efforts, inclusive community initiatives, and peer support programs that foster a sense of belonging. At the family level, strengthening communication, cohesion, and social support networks may help mitigate the psychological consequences of alienation. Meaning-focused or culturally grounded approaches may be especially relevant for caregivers who draw on spiritual or belief-based frameworks for support. Consistent with the strong association between alienation and depressive symptoms, addressing caregiver alienation represents a potentially important intervention target. Community-based initiatives may benefit from actively challenging stigma, enhancing public understanding of ASD, and promoting social inclusion of families of children with ASD (5, 45). Public education efforts and non-stigmatizing practices within health and social services may help reduce blaming attitudes and foster more supportive community environments.
Second, building peer support networks appears to be an important strategy. Whether delivered in person or online, peer groups can provide validation, shared experiences, and practical guidance, thereby counteracting feelings of isolation. Incorporating structured peer support into caregiver mental health programs may be particularly beneficial, as lower levels of alienation are associated with fewer depressive symptoms.
Third, strengthening family resilience offers a meaningful pathway for supporting caregiver mental health. Interventions may target the specific resilience components identified in this study. Programs that enhance communication and cohesion—by facilitating open emotional expression, collaborative problem-solving, and mutual support—may be especially impactful. Family-based psychoeducation or therapeutic approaches can help reinforce these relational processes while supporting families in managing stress.
Fourth, enhancing broader social support and service navigation represents another important direction (46). Practitioners can connect families to community resources, parent-mentor networks, and supportive organizations, and can assist caregivers in developing help-seeking and social networking skills. For caregivers who already draw on spiritual or meaning-focused frameworks, interventions that cultivate shared beliefs, purpose, or meaning may help sustain optimism and reduce vulnerability to alienation. Importantly, such approaches should be culturally sensitive and aligned with families’ existing values; even in non-religious families, encouraging shared narratives of growth, solidarity, or collective strength may serve similar supportive functions.
Given that communication/cohesion, perceived social support, and faith/spiritual beliefs emerged as the most salient moderators in this study, interventions that prioritize emotional and relational strengthening may be more effective for addressing depressive symptoms than approaches focused solely on practical coping skills. Ideally, comprehensive programs should integrate relational support with problem-focused strategies to provide holistic assistance for caregivers of children with ASD.
Importantly, these implications are equity-oriented: accessible, low-threshold community and family supports (e.g., anti-stigma initiatives, peer networks, and family-centered guidance) may reduce psychological burdens without requiring high-cost resources or specialized services. Prioritizing inclusive and culturally responsive support opportunities for under-served caregiver groups may help address inequities in caregiver mental health linked to differential access to services and social participation.
Limitations and future research
4.2
This study has several limitations. First, the cross-sectional design precludes causal inference. Although our framework posits that alienation contributes to depression and that family resilience buffers this association, the relationships may be reciprocal (e.g., depressive symptoms may increase social withdrawal and undermine family communication or perceived support). Longitudinal designs are therefore needed to establish temporal ordering and to test potential bidirectional dynamics among alienation, family resilience, and depression.
Second, all measures relied on caregiver self-report, which may introduce common method variance and response biases. Future work should strengthen measurement validity using multi-informant data and complementary assessment modalities (e.g., clinical evaluation of depression, observational indicators of family interaction, or objective indices of social connectedness).
Third, the sample was drawn from a single province in Northeast China and was recruited largely through community organizations and service agencies, which may limit generalizability and may overrepresent families already connected to support resources. In addition, although the FaRE demonstrated strong psychometric performance after item reduction, it was originally developed in the context of physical illness and may not fully capture autism-specific resilience processes. Replication in more diverse settings and with ASD-tailored resilience measures is warranted.
Building on these limitations, future research should extend our findings in several directions. Methodologically, longitudinal and mixed-method designs (including qualitative interviews or social network approaches) could provide a more nuanced account of caregivers’ lived experiences of alienation and support and clarify how resilience processes develop over time. Analytically, moderation could be probed more precisely using the Johnson–Neyman technique, which identifies the range(s) of the moderator for which the focal association is statistically significant (i.e., the region of significance) and complements conventional simple-slope probing (e.g., at ±1 SD). Theoretically, additional factors—particularly child characteristics such as ASD symptom severity, functional level, and challenging behaviors—should be examined as potential contributors to caregiver alienation and depression and as potential contingencies in resilience processes (47, 48). Finally, it may be useful to further differentiate alienation into interpersonal, societal, and self-related components to identify which facets are most strongly linked to depressive symptoms.
Importantly, intervention implications derived from this work require empirical evaluation. Controlled trials are needed to test whether multi-component programs that reduce caregiver alienation (e.g., stigma-reduction, inclusive community practices, peer support) and strengthen key resilience processes (communication/cohesion, social support, and meaning-focused coping) can reduce caregiver depression beyond standard care.
Conclusion
5
This study highlights the psychosocial challenges faced by caregivers of children with ASD and identifies both risk processes and moderating resilience mechanisms associated with their mental health. Alienation—characterized by experiences of social disconnection, marginalization, and stigma—was strongly associated with depressive symptoms, underscoring the importance of considering the broader social context surrounding autism in addition to the clinical needs of children.
The findings also suggest potentially protective processes within families. Although not all aspects of family resilience operated similarly, three subdimensions—communication/cohesion, perceived social support, and faith/spiritual beliefs—demonstrated significant buffering effects on the association between alienation and depression. Families characterized by open communication, emotional closeness, supportive networks, and shared belief systems appeared to provide environments that helped caregivers manage the psychological burden of social exclusion.
Taken together, the results point to two complementary avenues for supporting caregiver well-being. Reducing external stressors—such as stigma, misinformation about ASD, and limited community inclusion—may help alleviate feelings of alienation. Strengthening internal family resources, particularly relational and meaning-centered processes, may further support caregivers in coping with the challenges of raising a child with ASD. Interventions may benefit from integrating both approaches by addressing societal attitudes while also enhancing family-level resilience capacities.
Ultimately, caregiver depression in the context of ASD is not only an individual mental health concern but also a social one. This study provides evidence of a strong association between alienation and depressive symptoms, while highlighting specific family resilience processes that function as meaningful buffers. Supporting caregivers in feeling more connected—to their families, communities, and sources of meaning—remains an important goal for promoting sustained well-being among caregivers of children with ASD.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Maenner MJ Warren Z Williams AR Amoakohene E Bakian AV Bilder DA . Prevalence and characteristics of autism spectrum disorder among children aged 8 years — Autism and developmental disabilities monitoring network, 11 sites, United States 2020. MMWR Surveill Summ. (2023) 72:1–14. doi: 10.15585/mmwr.ss 7202 a 1, PMID: 36952288 PMC 10042614 · doi ↗ · pubmed ↗
- 2Cubells JF . Prevalence of autism spectrum disorders in China. Shanghai Arch Psychiatry. (2013) 25:176–8. doi: 10.3969/j.issn.1002-0829.2013.03.008, PMID: 24991154 PMC 4054547 · doi ↗ · pubmed ↗
- 3Dai Q Xu X Wang H Zhao Z Zhang X Zhou A . Prevalence of autism spectrum disorder in Chinese children from 2010 to 2016: A meta-analysis. Chin J Child Health Care. (2017) 25:1243–8.
- 4American Psychological Association . Publication manual of the american psychological association 7th ed. Washington, DC: American Psychological Association (2020).
- 5Ng CSM Ng SSL . A qualitative study on the experience of stigma for Chinese parents of children with autism spectrum disorder. Sci Rep. (2022) 12:19550. doi: 10.1038/s 41598-022-23978-0, PMID: 36379973 PMC 9666461 · doi ↗ · pubmed ↗
- 6Zhang P Wang M Feng S . Identifying research hotspots in mental health for parents of children with autism spectrum disorder: A bibliometric perspective. Humanities Soc Sci Commun. (2025) 12:1881. doi: 10.1057/s 41599-025-06152-5, PMID: 39310270 · doi ↗
- 7Zheng L Long C Choi W . The effect of social activities on the alienation and family resilience of Chinese caregivers for children with autism: A latent class analysis. Front Psychiatry. (2024) 15:1406073. doi: 10.3389/fpsyt.2024.1406073, PMID: 38895029 PMC 11184502 · doi ↗ · pubmed ↗
- 8Li F Tang Y Li F Fang S Liu X Tao M . Psychological distress in parents of children with autism spectrum disorder: A cross-sectional study based on 683 mother–father dyads. J Pediatr Nurs. (2022) 65:e 49–55. doi: 10.1016/j.pedn.2022.02.006, PMID: 35249769 · doi ↗ · pubmed ↗