Evaluating the health economic impact of cefepime/enmetazobactam in complicated urinary tract infections in the German setting: a cost analysis from payer perspective
Johanna Röder, Sebastian M. Wingen-Heimann, Danila Seidel, Ann-Cathrine Froitzheim, Melina S. Kurte, Oliver Witzke, Maria J. G. T. Vehreschild, Oliver A. Cornely, Florian Kron

TL;DR
This paper evaluates the economic impact of two antibiotic treatments for complicated urinary tract infections in Germany, finding that one option may reduce long-term costs by lowering relapse rates.
Contribution
The study provides a novel health economic analysis comparing cefepime/enmetazobactam and piperacillin/tazobactam for cUTIs from a German payer perspective.
Findings
Cefepime/enmetazobactam had lower average treatment costs (€5,332.12) compared to piperacillin/tazobactam (€5,414.83).
Higher relapse rates are associated with increased treatment costs in the German healthcare system.
Cumulative cost differences at the population level could be substantial despite moderate per-patient differences.
Abstract
Complicated urinary tract infections (cUTIs) are ubiquitous, associated with healthcare resources, and demand effective antibiotic treatment to prevent clinical failure and relapse. Evidence on health economic implications of treatment options remains limited. Recent studies have shown that cefepime/enmetazobactam was superior to piperacillin/tazobactam regarding the combined endpoints clinical cure and microbiological eradication, the latter being closely linked to reduced relapse rates. Therefore, we perform a health economic evaluation of cefepime/enmetazobactam vs. piperacillin/tazobactam for cUTI from a German payer perspective. To assess monetary impacts of both therapies, we conducted a semi-structured literature review for costs of (relapsed) cUTI. Subsequently, we adjusted international costs to the German healthcare system using European price levels of the Organisation for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
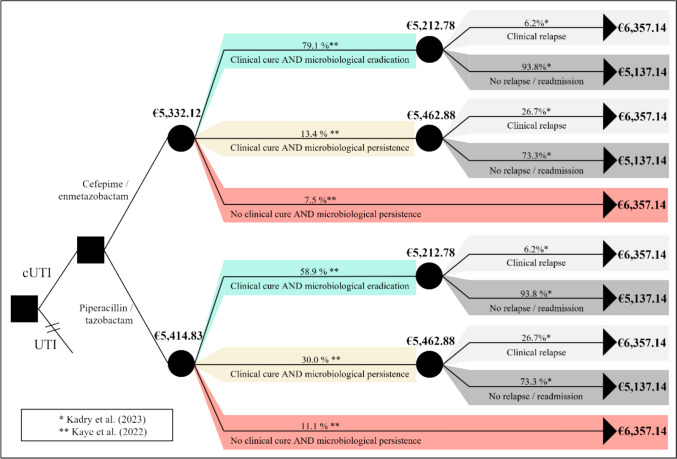 Figure 1
Figure 1- —FOM Hochschule für Oekonomie und Management gGmbH (3376)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Tract Infections Management · Antibiotics Pharmacokinetics and Efficacy · Pediatric Urology and Nephrology Studies
Introduction
Urinary tract infections (UTI) are among the most common bacterial infections and represent a major public health concern due to their high prevalence and significant impact on healthcare systems worldwide [1, 2, 3]. Particularly complicated urinary tract infections (cUTI), which are characterised by occurring in patients with structural or functional anomalies of the urogenital tract [4], or in combination with comorbidities, result in higher healthcare costs. However, limited research exists regarding the extent of the clinical and financial burden [1, 5, 6, 7]. Broad definitions and delimitations of cUTI limit comparability of studies, especially on an international scale [8]. Direct and indirect costs associated with cUTI arise from prolonged hospital stays, illness-related disability, additional diagnostic procedures, and the need for prolonged antimicrobial therapy [5]. These costs are further enhanced by emergence of multidrug-resistant bacterial pathogens, making cUTI treatment more difficult [2, 6, 9]. It is not uncommon for cUTIs to occur during an inpatient stay and, at up to 65%, they account for the largest proportion of nosocomial infections [5, 10]. Additionally, cUTI represent a reason for admission to hospital [11]. A cross-sectional multicenter study based on the National Emergency Department database in the United States has shown that almost two thirds of cUTI visits in the emergency department ended in hospitalisation. Of these, 44.9% were related to cUTI directly as main diagnosis, whereas 85.5% had cUTI as secondary diagnosis [12]. In light of these challenges, there is an urgent need for treatment strategies to address resistance but also to reduce relapse rates and, consequently, healthcare resource utilisation. However, health economic evaluations for this purpose are rare and not yet available for cUTI in Germany.
Clinical trial data have demonstrated that the novel β-lactam/β-lactamase inhibitor combination cefepime/enmetazobactam is non-inferior and superior in efficacy to piperacillin/tazobactam for treating cUTI and acute pyelonephritis caused by gram-negative bacteria [13]. The combined measure of clinical cure and microbiological eradication showed that more patients achieved favourable outcomes with cefepime/enmetazobactam. Microbiological eradication was defined as the reduction of qualifying baseline pathogens to less than 10^3^ CFU/mL in urine [13]. The composite outcome of both clinical cure and microbiological eradication to determine therapeutic success is commonly used by the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA) [27, 28]. Kadry et al. showed that microbiological eradication in particular is an indicator of the overall success of the antibiotic therapy, i.e. also considering relapse rates [14]. Patients who met the criteria for clinical cure without microbiological eradication at follow-up after completing antibiotic therapy were with an adjusted odds ratio of 5.51 more likely to experience clinical failure compared to those who achieved both clinical cure and microbiological eradication [14].
In this study, the health economic impact of using cefepime/enmetazobactam instead of piperacillin/tazobactam for the treatment of cUTI is evaluated from a payer’s perspective, with a particular focus on reducing relapse rates and hospital readmissions, and the subsequent impact on healthcare resource utilisation and costs in Germany.
Methods
The following step-by-step approach was used for the health economic evaluation to assess the monetary impact for the treatment of cUTI patients with cefepime/enmetazobactam:
-
I.Cost evaluation for cUTI The cost assessment for cUTI in Germany was conducted based on a semi-structured literature review by using the literature database PubMed. Relevant sources were analysed to estimate the average cost per patient on an inpatient level.
-
II.Cost evaluation for relapse of cUTI in GermanyThe costs associated with relapses of cUTI were also derived from a semi-structured literature research with PubMed, followed by a conversion of costs into the German healthcare context via an international comparison of price levels of the Organisation for Economic Cooperation and Development (OECD).
-
III. Comparative health economic analysis of cefepime/enmetazobactam vs. piperacillin/tazobactam for cUTI in GermanyThe results from step I and step II served as the foundation for the comparative health economic evaluation for the two antibiotic regimes cefepime/enmetazobactam versus piperacillin/tazobactam for the treatment of cUTI. The comparison accounted for the cUTI relapse rate, incorporating primary outcome and recurrence rates as reported in previous studies [13, 14]. By integrating these probabilities into the cost framework, a comprehensive assessment of the total healthcare expenditures associated with each treatment strategy was performed from a healthcare payer’s perspective.
-
IV.Validation of simulated cost data in GermanyTo ensure the robustness of the cost estimates, a final verification step was conducted using publicly available inpatient data from all German hospitals, completed by cost data from cost-accounting hospitals for the year 2023. According to § 21 Hospital Remuneration Act (Krankenhausentgeltgesetz (KHEntG) inpatient case data is reported quarterly to the Institute for Hospital Remuneration system (InEK). The data contained case information on diagnoses, procedures and outsourced German Diagnosis Related groups (aG-DRGs) in an anonymised and aggregated form and is accessible via the database InEK Data Browser [15]. Twenty-five queries consisting of principal diagnosis and secondary diagnoses (Supplementary Table 8) based on the inclusion criteria of Kaye et al. [13] were performed, to create an equivalent study (queries 1-25). Procedural codes (OPS) for complex treatment for colonisation or infection with multidrug-resistant pathogens were further queried (Supplementary Table 9). Another query (query 26) combines the main diagnosis for urinary tract infections (N39.0) according to ICD-10-GM with relevant secondary diagnoses and an ICD specific multidrug-resistant pathogens. Supplementary Table 10 shows the composition of all 26 performed queries, including all diagnostic and procedure codes according to the International Statistical Classification of diseases 10 German Modification (ICD-10-GM) 2023 [16] and the German procedure classification system 2023 [17].
Data collection
The direct cost data underlying this study was obtained from Vallejo-Torres et al. [18] and consisted of unit costs for length of stay (LOS), diagnostic tests (DIAG), treatment procedures (TREAT), antibiotic therapy (ATB), and costs after discharge for readmissions and outpatient visits (DISCH). The study presented three cost scenarios for cUTI patients. Scenario 1 includes costs for diagnosis and treatment, and the length of stay in the hospital. The second scenario considers in addition the costs of antibiotic therapy. The third scenario furthermore considers costs incurred after the actual discharge with respect to readmissions and additional outpatient visits after relapse. The scenarios two and three were used for the following cost analysis and transferred to the German healthcare system.
International comparison of healthcare values
For international comparison of healthcare values, a methodology developed by the OECD was used. Because price levels vary markedly between Germany, Spain, and other European countries, Koechlin et al. [19] and Lorenzoni et al. [20] developed an approach of converting national currency values into one common European price level. For this study, the Spanish cost values for cUTI treatment as published by Vallejo-Torres et al. [18] were converted to German cost values via the common European price level as presented in Table 1. This applied methodology ensures the transferability of cost values to the German healthcare system.Table 1. Cost value conversion Spain–Germany for three scenarios based on OECD price levelSpain [18]OECD-Level 2017GermanyLOS + DIAG + TREAT€5,241.00€6,239.29€4,991.43LOS + DIAG + TREAT + ATB€5,394.00€6,421.43**€5,137.14LOS + DIAG + TREAT + ATB + DISCH€6,675.00€7,946.43€6,357.14**Bold values indicate the resulng costs used for the decision treeLOS - length of stay, DIAG - diagnostic tests, TREAT - treatment procedures, ATB - antibiotic therapy, DISCH - costs after discharge for readmissions and outpatient visitsSpain’s healthcare price level is 84% of the OECD average, whereas Germany’s is 80%. For example, €100 spent on healthcare services in Spain corresponds to €95.24 in Germany when adjusted for OECD price levels
Decision tree
For the comparative cost analysis for cUTI in Germany, a decision tree model was constructed. Literature-based and converted cost values (Table 1) were incorporated as well as probabilities for “clinical cure AND microbiological eradication” (composite endpoint), probabilities for “clinical cure AND microbiological persistence”, probabilities for “No clinical cure AND microbiological persistence” (Table 2) from Kaye et al. [13], and probabilities for “clinical relapse” and “no relapse/readmission” (Table 3) from Kadry et al. [14] to calculate overall cUTI treatment costs for cefepime/enmetazobactam versus piperacillin/tazobactam. Relapse rates are conditional on microbiological outcome and were applied equally to both drugs due to lack of drug-specific evidence [14].Table 2. Probabilities I for decision-tree based on Kaye et al. [13]Clinical cure AND microbiological eradicationClinical cure AND microbiological persistenceNo clinical cure AND microbiological persistence*∑Cefepime/enmetazobactam79.1%13.4%7.5%100%Piperacillin/tazobactam58.9%30.0%11.1%100%Table 3. Probabilities II for decision tree based on Kadry et al. [14]Clinical relapse/readmissionNo relapse/readmission∑*Clinical cure AND microbiological eradication6.2%93.8%100%Clinical cure AND microbiological persistence26.7%73.3%100%No clinical cure AND microbiological persistence100%0%100%
Sensitivity analysis
Sensitivity analysis to control for variation in probabilities was conducted based on the approach by Kadry et al. [14]. Supplementary Table 11 shows the modified probabilities used for the sensitivity analysis.
Results
Decision tree
For Spain, cost values of €5,394 without a clinical relapse and €6,675 with a clinical relapse for the treatment of cUTI were reported in the literature [18]. The conversion using the OECD price levels of 84% for Spain and 80% for Germany resulted in costs of €5,137.14 for the treatment of cUTI without a relapse and €6,357.14 for cases with a relapse in Germany (Fig. 1, calculations in Supplementary Table 7). The resulting costs for cases with clinical relapse and those without relapse were assumed to be independent of the selected antibiotic therapy in this model, as published literature does not provide robust evidence for differences in relapse-related costs between cefepime/enmetazobactam and piperacillin/tazobactam. Considering the probabilities of clinical relapse and non-relapse, this results in the following costs for the two different scenarios cefepime/enmetazobactam and piperacillin/tazobactam of the decision tree model. To determine the costs to be compared, the decision tree must be viewed from right to left; the total costs result from the multiplication of case costs with the respective probabilities.Fig. 1. Decision Tree cUTI treatment and associated costs with cefepime/enmetazobactam vs. piperacillin/tazobactam. Relapse rates are conditional on microbiological outcome and were applied to both drugs due to lack of drug-specific evidence
Cefepime/enmetazobactam
In patients who undergo treatment with cefepime/enmetazobactam, clinical cure AND microbiological eradication is reached with a probability of 79.1%. Assuming that a clinical relapse occurs in 6.2% and no relapse in 93.8% of these cases, this results in average composed costs for therapy of €5,212.78 for the composite endpoint. Clinical cure AND microbiological persistence are achieved in 13.4% of cases, with the assumption of clinical relapse occurring with a probability of 26.7% and non-relapse with a probability of 73.3%. This results in average treatment costs of €5,462.88. However, 7.5% of all cases treated with cefepime/enmetazobactam did not meet clinical cure nor microbiological eradication, resulting in treatment costs of €6,357.14 within this group with a probability of 100%. This results in average treatment costs of €5,332.12 for cefepime/enmetazobactam.
Piperacillin/tazobactam
Patients treated with the comparator piperacillin/tazobactam reach the composite endpoint clinical cure AND microbiological eradication in 58.9% of cases. Probabilities for the assumption of clinical relapse (6.2%) and no relapse (93.8%) remain equal, resulting in average composed costs of €5,212.78. Clinical cure AND microbiological persistence are observed in 30.0% of all cases with treatment of piperacillin/tazobactam. Probabilities of 26.7% for clinical relapse and 73.3% for no relapse result in average costs of €5.462,88. No clinical cure AND microbiological persistence is met by 11.1% of patients treated with piperacillin/tazobactam, equally to treatment costs of €6,357.14 for this group. Overall, average treatment costs for piperacillin/tazobactam amount to €5,414.83 without further differentiation of clinical relapse and no relapse.
Results verification
We performed 26 individual queries via the InEK DataBrowser to obtain data for the German healthcare setting. The resulting DRGs were matched with the average costs per DRG from the InEK DataBrowser—Data Delivery Costs DRG 2023 grouped by 2025 (DRG Report Browser). The queries can be clustered as shown below.
Queries 1–25
A total of 169 cases (queries 1–25) met the inclusion criteria for cUTI derived from Kaye et al. [13]. Due to data protection regulations, a number of cases smaller than four is not displayed in the InEK DataBrowser. This results in 77 cases for further analysis, whereas 92 cases were excluded. Forty of all included cases were assigned to DRG L63B with an average LOS of 13.4 days (Table 4). The remaining 37 cases were assigned to DRG L63A with an average LOS of 19.9 days (Table 5). This results in an average DRG- costs of €5,312.12 per case with DRG L63B, and €7,809.39 per case for the higher-rated DRG L63A for the accounting year 2023. Both groups were within the average length of stay of the respective DRG-group, ensuring no further surcharges or deductions from the DRG-fee. Due to the separation of the nursing budget from the DRG, personnel costs for nursing were not included.Table 4. Verification—DRG costs L63B for cUTI in GermanyaG-DRGDesignationQuery No.CasesAverageLOSStandard deviation LOSCumulated LOSL63BInfections of the urinary organs without certain highly complex treatment, with certain complex treatment or with extremely severe CC, without complex treatment for pathogens requiring isolation, without extremely severe CC. [27]11112.005.691323512.602.06634516.0010.688011811.255.6190161115.558.501714013.4536L63B – Arithmetic mean costs aG-DRG 2023 grouped by 2025, [26]€5,312.12Standard deviation costs aG-DRG L63A€2,767.51aG-DRG - outsourced German Diagnosis-Related Group, LOS - length of stayTable 5Verification—DRG-remuneration L63A for cUTI in GermanyaG-DRGDesignationQuery No.CasesAverage LOSStandard deviation LOSCumulated LOSL63AInfections of the urinary organs with certain highly complex treatment or with extremely severe CC, with complex treatment for pathogens requiring isolation. [27]11220.5014.1924641019.609.7119611617.178.0910316921.449.621933719.9738L63A – Arithmetic mean costs aG-DRG 2023 grouped by 2025 [26]€8,686.43Standard deviation costs aG-DRG L63A€3,751.82aG-DRG - outsourced German Diagnosis-Related Group, LOS - length of stay
Query 26
Query 26 was based on the main diagnosis for urinary tract infections (N39.0) combined with relevant secondary diagnoses and further ICD codes for specific multidrug-resistant pathogens. We received a total of 114 cases in this query. 17 cases were excluded by data protection regulation. 46 cases (40.32%) resulted in the two previously stated DRGs L63B (32 cases) and L63A (14 cases) corresponding to average treatment costs of €5,312.12 for L63B and €8,686.43 for L63A, respectively. Four additional DRGs were found (L63E, L64B, L74Z, L44Z), associated with aG-DRG costs between €1,900.34 and €7,130.87 for the average LOS resulting from the query (Table 6).Table 6. Verification query 26 for cUTI in GermanyaG-DRGDesignationCasesaG-Costs aG-DRG 2023 grouped by 2025Standard deviation costs aG-DRGL63BInfections of the urinary organs without certain highly complex treatment, with certain complex treatment or with extremely severe CC, without complex treatment for pathogens requiring isolation or with complex treatment for pathogens requiring isolation, without extremely severe CC32€5,312.12€2,767.51L63EInfections of the urinary organs without extremely severe CC, without moderate / complex / highly complex treatment, without complex treatment for pathogens requiring isolation. treatment, without complex treatment for pathogens requiring isolation, without certain severe infections, age >5 and <18 years, without severe CC or age >17 and <90 years31€2,277.84€1,044.99L63AInfections of the urinary organs with certain highly complex treatment or with extremely severe CC, with complex treatment for pathogens requiring isolation14€8,686.43€3,751.82L64BOther diseases of the urinary organs with extremely severe or severe CC or specific diagnosis, more than one day of hospitalisation or urethrocystoscopy, except for congenital malformation, age >2 years9€1.917,49€783.09L74ZCertain diseases and disorders of the urinary organs with para-/tetraplegia6€2,544.50€1,274.27L44ZGeriatric early rehabilitation complex treatment for diseases and disorders of the urinary organs5€6,546.29€2,039.51Arithmetic mean costs and standard deviation based on Data delivery Costs DRG 2023 grouped by 2025 (‘DRG Report Browser’) [26]
Sensitivity analysis
The sensitivity analysis was based on the sensitivity analysis of Kadry et al. (2023) who stratified participants by reported reasons for clinical failure, resulting in different probabilities: 5.1% (compared to 6.2%) of concordant successes (clinical cure, microbiological eradication) were clinical failures defined as relapses, whereas 17.5% of discordant failures (clinical cure, microbiological persistence) resulted in relapses. Considering these probabilities, result tendency remains robust leading to average composed costs of €5,306.47 for treatment with cefepime/enmetazobactam compared to €5,373.25 for piperacillin/tazobactam treatment. Supplementary Tables 11 and 12 and Supplementary Fig. 2 show the corresponding probabilities, calculations and the resulting decision tree.
Discussion
To our knowledge, this is the first study analysing the financial effects of cUTI with and without relapses in Germany, comparing the impact of the two antibiotics cefepime/enmetazobactam and piperacillin/tazobactam within an economic evaluation. The results of this study highlight the health economic impact of treating cUTI with cefepime/enmetazobactam compared to piperacillin/tazobactam from the payer perspective in Germany. By incorporating literature-based cost values and clinical trial probabilities for relapse rates into a decision tree, we modelled the potential healthcare resource utilisation and financial burden associated with cUTI treatment strategies.
Our analysis reveals that relapse/readmission for cUTI has a direct financial impact and leads to significant increase in healthcare costs. Based on the semi-structured literature review, the average cost of treating a cUTI without relapse/readmission is €5,137.14, compared to €6,357.14 for cUTI with relapse/readmission from a payer’s perspective in Germany. Treatment costs are also influenced by the choice of antibiotic, as differences in drug efficacy can affect the likelihood of relapse and the duration of therapy. On average, treating a cUTI with cefepime/enmetazobactam results in costs of €5,332.12, while treatment with piperacillin/tazobactam results in €82.71 higher costs, when accounting for all outcome contingencies.
These findings are generally reflected in our decision-tree model and validation. Costs for more severe cases of cUTI were estimated at €8,686.43, whereas less severe cases amounted to €5,312.12. However, while the model supports the general trends observed in the literature, these findings should be interpreted with caution, as the aggregated aG-DRG case data used for modelling did not allow for the specific distinction between clinical relapse and cases without relapse/readmission. Consequently, the resulting cost estimates may be conservative, potentially underestimating the true economic burden, as relapse-related readmissions and resulting long-stay outlier payments are not fully captured.
Although the per-patient cost difference between cefepime/enmetazobactam and piperacillin/tazobactam is relatively small, its implications may be more relevant when considered at population level. Between 2022 and 2024, approximately 240,000–280,000 patients in Germany were hospitalised annually with cUTI/otherwise-defined UTI as the main reason for admission (ICD-10-GM N30-N39, Other diseases of the urinary system) [15, 21, 22]. Assuming all were treated with cefepime/enmetazobactam instead of piperacillin/tazobactam, potential annual cost savings could range from €19.9 million to €23.1 million. These theoretical estimates represent an upper-bound scenario and should be interpreted with caution, as only a subset of patients would be eligible for treatment with a reserve antibiotic. Nonetheless, even with these constraints, these results suggest that substantial population-level savings are possible, highlighting the potential economic relevance of broader adoption in clinical practice. This consideration may become even more relevant when extrapolating to larger healthcare systems.
Previous studies have shown that microbiological persistence, even after initial clinical cure, increases the risk of later treatment failure [14]. Therefore, initiation with effective antimicrobial therapy, leading to both clinical cure and microbiological eradication, is crucial to minimize the risk of relapse and subsequent hospital readmission. Our results add an important economic dimension to the clinical perspective by showing that relapses are associated with notably higher healthcare costs. As shown in the model, the higher efficacy of cefepime/enmetazobactam in achieving both clinical and microbiological success translates into both improved patient outcomes and reduced healthcare expenditures from a payer perspective.
From a health economic perspective, our analysis highlights the importance of choosing antibiotics that not only address antimicrobial resistance but also minimize indirect costs, such as prolonged hospital stays and additional diagnostic interventions. The decision tree model provides a structured approach to quantifying these economic effects on a case basis, offering valuable insights for healthcare payers in Germany. Given the increasing prevalence of multidrug-resistant pathogens, treatment strategies that effectively reduce relapse rates can help mitigate the long-term financial burden on the healthcare system.
It should be noted that our analysis set its focus on quantifying the economic burden for the treatment of cefepime/enmetazobactam compared to piperacillin/tazobactam broken down to a case-based level for Germany. Hereby, the focus is set on cUTI as the main diagnosis. However, cUTI as a secondary diagnosis and hospital-acquired infection poses a significant share as demonstrated by Zilberberg et al. [12]. Due to the heterogeneity of cUTI cases and limitations of the InEK Data Browser as data source, it was not possible to derive an overall German picture from our aggregated data source. The expansion of the analysis to cover the broader cUTI population should be addressed in future analyses.
Finally, it needs to be stressed that the favourable evaluation of cefepime/enmetazobactam compared to piperacillin/tazobactam with respect to health economic aspects is only one of many factors that need to be taken into account in a clinical context. From an antimicrobial stewardship perspective [23], the replacement of piperacillin/tazobactam by cefepime/enmetazobactam in the absence of multidrug-resistant bacteria is not acceptable and needs to be taken into account during further discussions. In this line of thought, it would be very valuable to extend the health economic analysis to further drugs with a comparable activity spectrum.
Limitations
This study has several limitations. The model relies on probabilities from Kaye et al. [13], who predominantly enrolled patients from Eastern Europe. Eastern Europe is a region that is assumed to have comparatively higher rates of ESBL-producing pathogens than Western Europe [24, 25], which may have influenced treatment outcomes. In the study by Kadry et al. [14], relapse rates were primarily assessed at end of treatment, whereas our evaluation focused on day 14 outcomes, when intergroup differences were most evident. Due to the lack of alternative evidence, we assumed identical relapse probabilities for both drugs. These aspects should be considered when interpreting our results.
Additionally, our model relies on international cost data (Spain) extracted from literature, which are applied to the German healthcare setting. This is only possible by assuming that in general, the standard of care of cUTI in Spain is comparable to Germany and differs only by the different price levels [19, 20], which may not fully capture the variability seen in real-world clinical settings. This may allow both an over- and underestimation for both scenarios cUTI with and without clinical relapse/readmission.
While the decision tree approach provides a transparent framework for health economic evaluation, it does not account for dynamic factors such as patient-specific characteristics or drug resistance patterns that may influence treatment outcomes. Due to the chosen perspective, no indirect costs (e.g. illness-related disability) were taken into account in our analysis, so we assume a conservative approach and the total costs for cUTI may be higher than shown in this study. Future research should aim to validate these findings with real-world healthcare data and incorporate more granular cost analyses preferably by a bottom-up cost data approach.
In conclusion, this study provides strong evidence supporting the health economic and clinical benefits of cefepime/enmetazobactam over piperacillin/tazobactam for the treatment of cUTI in Germany. By reducing relapse rates and associated healthcare costs, this novel antibiotic regimen represents a promising option for optimizing resource allocation and improving patient care outcomes.
Conclusion
This study is the first to provide a health economic evaluation of cefepime/enmetazobactam in the treatment of cUTI from the German payers’ perspective. The use of cefepime/enmetazobactam for cUTI led to slightly reduced costs compared to piperacillin/tazobactam due to higher microbiological eradication probabilities and consequently lower relapse/readmission rates on a case level but might lead to substantially reduced costs from a population level. Further research on cUTI and its treatment options or another perspective for health economic evaluation is needed to gain deeper insights.
Conflict of interests
J.R., S.M.W.H., D.S., A.C.F., M.S.K., and F.K. are independent employees of VITIS Healthcare Group and received research funding from Advanz Pharma Germany GmbH. S.M.W.H. has received research and travel grants from Astellas, Merck, and Tillotts; research grants from Basilea, Gilead, and 3 M; travel grants from Pfizer; and lecture honoraria from Astellas, Merck, and Tillotts. O.W. has received research grants, speaker fees or travel grants from Amgen, Alexion, Astellas, AstraZeneca, Basilea, Biotest, Bristol-Myers Squibb, Correvio, Chiesi, Gilead, GSK, Hexal, Janssen, Dr. F. Köhler Chemie, MSD, Novartis, Roche, Pfizer, Sanofi, TEVA and UCB. O. Witzke is a member of the DGfN, DTG, RWGIM, DGMI and a member of the executive board of the DGI. M.J.G.T.V. has received speaker fees from Merck/MSD, 3 M, Ferring, Astellas, Uniklinik Karlsruhe, Uniklinik Köln, Akademie für Infektionsmedizin, Klinikum Essen, Pfizer, Universitätsklinikum Heidelberg, Uniklinik Frankfurt, Landesärztekammer Hessen, Janssen, Institute Merieux, Forum für medizinische Fortbildung GmbH, Universitätsklinikum Freiburg, Berliner Dialyseminar, ADKA, Falk Foundation, St Johannes Hospital, DiaLog Service, CED Service, Ärztekammer Niedersachsen, St Josef Hospital, Limbach Gruppe SE, SUMIT OXFORD Ltd, EUMEDICA, KIT Kongress, Tillotts Pharma, Helios Kliniken, Lahn-Dill Kliniken, Gilead, and Klinikum Leverkusen. O.A.C. has received grants or contracts from iMi, iHi, DFG, BMBF, Cidara, DZIF, EU-DG RTD, F2G, Gilead, Med-Pace, MSD, Mundipharma, Octapharma, Pfizer and Scynexis, received consulting fees from Abbvie, AiCuris, Basilea, Biocon, Cidara, Seqirus, Gilead, GSK, IQVIA, Janssen, Matinas, MedPace, Menarini, Molecular Partners, MSG-ERC, Mundipharma, Noxxon, Octapharma, Pardes, Partner Therapeutics, Pfizer, PSI, Scynexis, Seres, Elion Therapeutics and Melinta, received payment or honoraria from Abbott, Abbvie, Akademie für Infektionsmedizin, Al-Jazeera Pharmaceuticals/Hikma, amedes, AstraZeneca, Deutscher Ärzteverlag, Gilead, GSK, Grupo Biotoscana/United Medical/Knight, Ipsen Pharma, Medscape/WebMD, MedUpdate, MSD, Moderna, Mundipharma, Noscendo, Paul-Martini-Stiftung, Pfizer, Sandoz, Seqirus, Shionogi, streamedup!, Touch Independent and Vitis, received payment for expert testimony from Cidara, and participated on a Data Safety Monitoring Board or Advisory Board for Boston Strategic Partners, Cidara, IQVIA, Janssen, MedPace, PSI, Pulmocide, Shionogi, The Prime Meridian Group, Vedanta Biosciences, AstraZeneca and Melinta.
Ethics approval
Ethics approval is not required for this study in accordance with local or national guidelines.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 274 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Carreno JJ, Tam IM, Meyers JL, Esterberg E, Candrilli SD, Lodise TP. Longitudinal, nationwide, cohort study to assess incidence, outcomes, and costs associated with complicated urinary tract infection. Open Forum Infect Dis. 2019. 10.1093/ofid/ofz 446.10.1093/ofid/ofz 536PMC 695678131951222 · doi ↗ · pubmed ↗
- 2Institut für das Entgeltsystem im Krankenhaus. Fallpauschalen-Katalog 2023 [Flat rate catalogue 2023]. 2022. Available from: https://www.g-drg.de/ag-drg-system-2023/fallpauschalen-katalog/fallpauschalen-katalog-20232.
- 3US Department of Health and Human Services; Food and Drug Administration; Center for Drug Evaluation and Research. Complicated Urinary Tract Infections: Developing Drugs for Treatment: Guidance for Industry. 2018. Available from: https://www.fda.gov/media/71313/download. Accessed 26 Feb 2025
- 4In EK Daten Browser—Unterjährige Datenlieferung DRG Januar bis Dezember 2023 [In EK Data Browser—in year data supply DRG January to December 2023. Available from: https://datenbrowser.inek.org/DRG 202401. Accessed 10 Feb 2025.
- 5Bundesinstitut für Arzneimittel und Medizinprodukte. 2023. ICD-10-GM Internationale statistische Klassifikation der Krankenheiten und verwandter Gesundheitsprobleme, German Modification [ICD-10-GM International Statistical classification of Diseases, German Modification]. Available from: https://www.bfarm.de/EN/Code-systems/Classifications/ICD/ICD-10-GM/_node.html. Accessed 11 Mar 2025
- 6Bundesinstitut für Arzneimittel und Medizinprodukte. 2023. Operationen- und Prozedurenschlüssel Version 2023 [German Procedure Classification Version 2023]. Available from: https://klassifikationen.bfarm.de/ops/kode-suche/htmlops 2023/index.htm. Accessed 15 Jan 2025.
- 7In EK Daten Browser—Unterjährige Datenlieferung DRG Januar bis Dezember 2022 [In EK Data Browser—in year data supply DRG January to December 2022]. Available from: https://datenbrowser.inek.org/DRG 202301. Accessed 5 Dec 2025
- 8In EK Daten Browser—Unterjährige Datenlieferung DRG Januar bis Dezember 2024 [In EK Data Browser—in year data supply DRG January to December 2024]. Available from: https://datenbrowser.inek.org/DRG 202501. Accessed 5 Dec 2025.