Electronic health records-related determinants of healthcare professionals' burnout and mitigation strategies: systematic review and meta-analysis
Yi Yang, Rui Shi, Zeng Wang, Jia Xu, Jiaxi Xie, Jialin Liu

TL;DR
This paper reviews how electronic health records contribute to burnout among healthcare workers and suggests ways to reduce it.
Contribution
A comprehensive multi-group analysis of EHR-related burnout and identification of key mitigation factors across healthcare professionals.
Findings
EHR use significantly increases the risk of occupational burnout (OR = 2.49).
Burnout rates vary by professional group, with physicians having the highest occurrence at 38.1%.
Poor EHR design and excessive documentation time are primary contributors to burnout.
Abstract
While the adoption of electronic health records (EHRs) has become widespread, it has been accompanied by a concurrent exacerbation of burnout among healthcare professionals. However, existing research has predominantly focused on single professional groups, lacking comprehensive multi-group analysis and the identification of key modifiable mitigation factors. Following the PRISMA guidelines, we systematically searched for relevant literature published between 2005 and 2025. A total of 41 studies, encompassing 54,443 healthcare professionals, were included. A meta-analysis was conducted to assess the association between EHR use and occupational burnout, with subgroup analyses performed to examine differences across various professional groups and assessment tools. Sensitivity analysis was conducted to reduce the bias. The use of EHRs was found to significantly associated with an…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
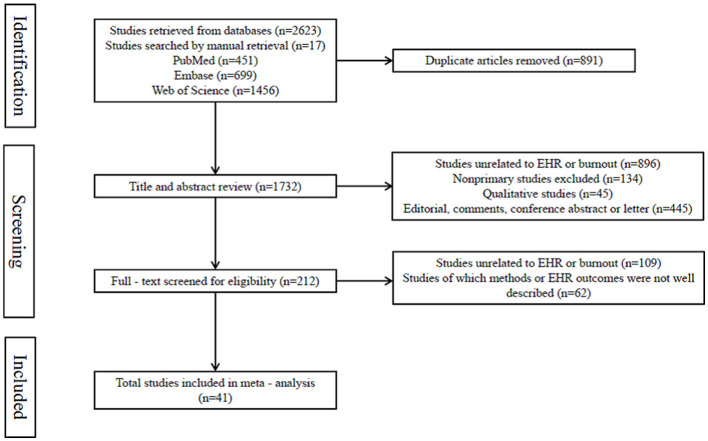 Figure 1
Figure 1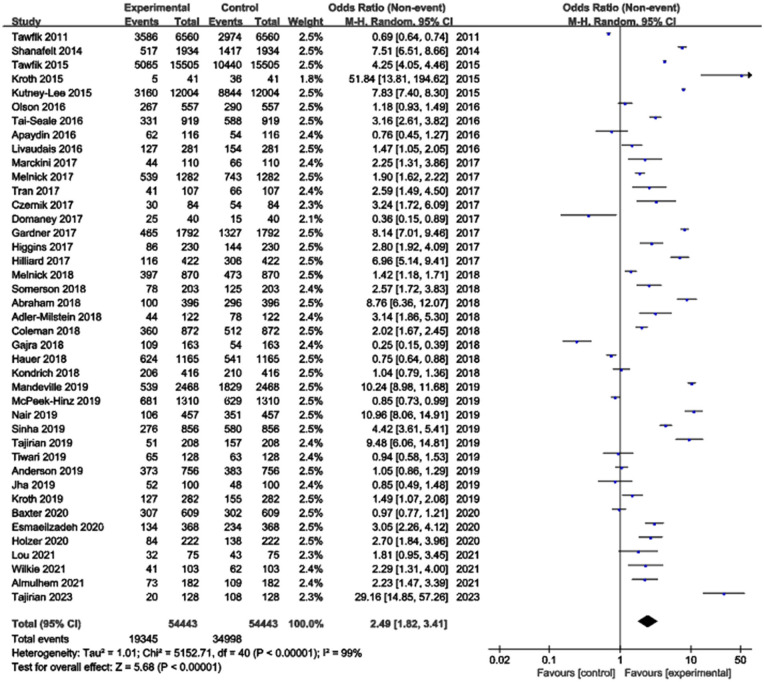 Figure 2
Figure 2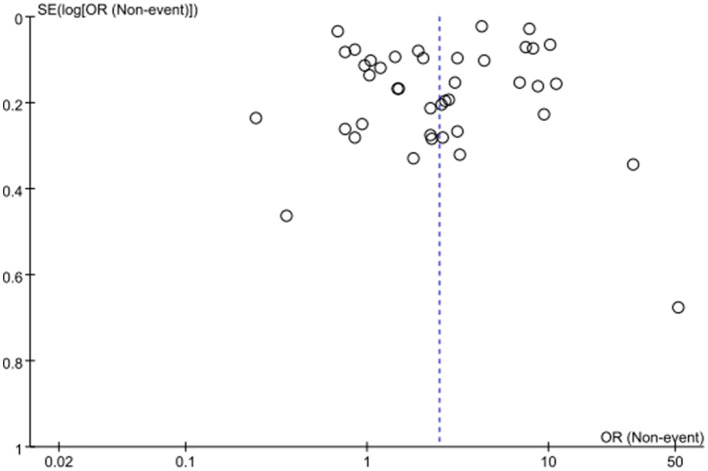 Figure 3
Figure 3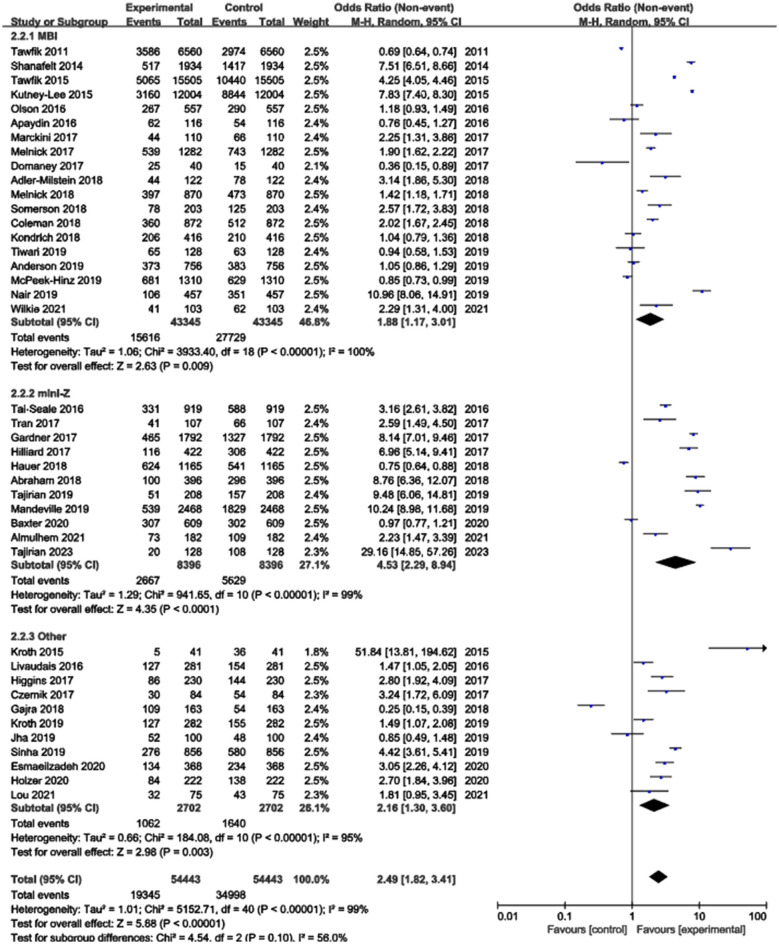 Figure 4
Figure 4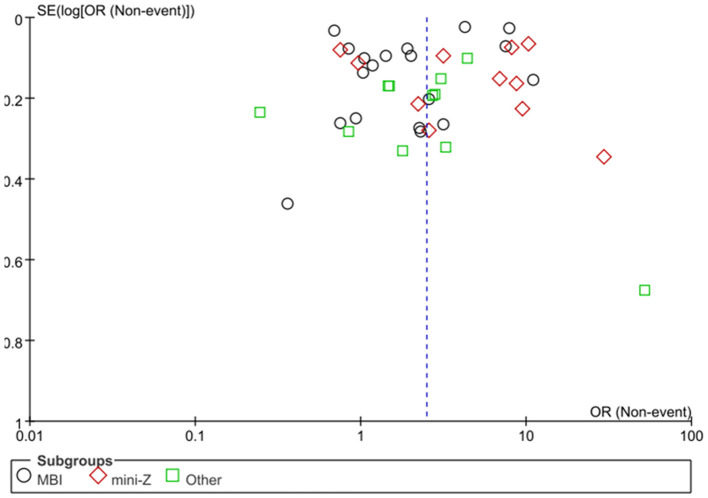 Figure 5
Figure 5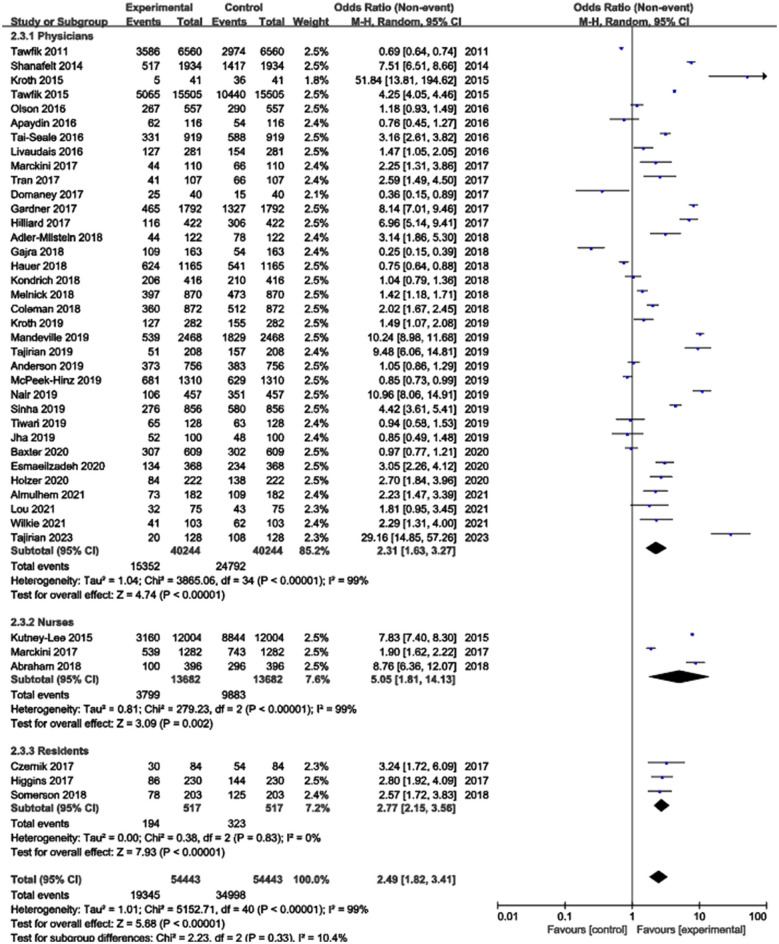 Figure 6
Figure 6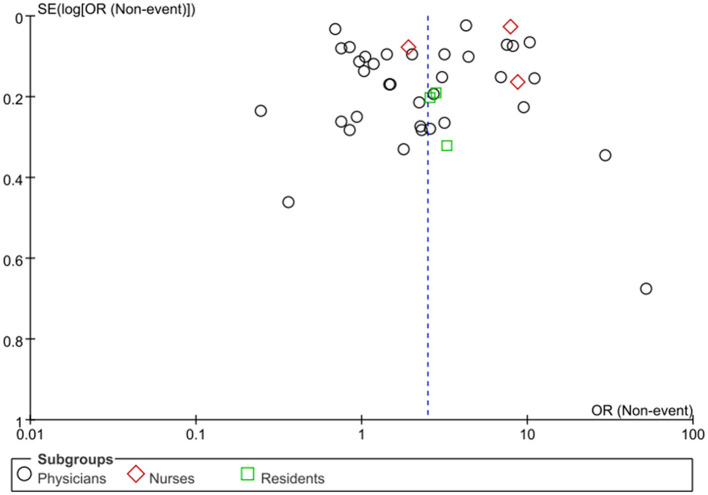 Figure 7
Figure 7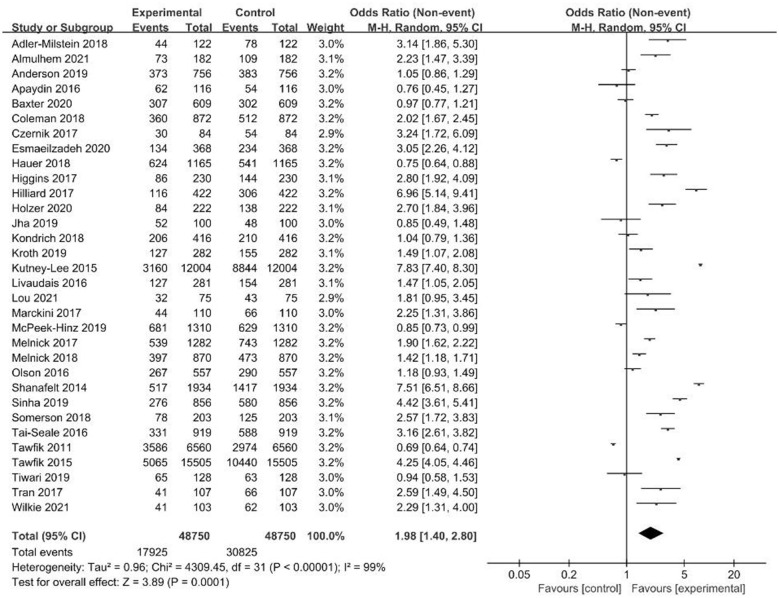 Figure 8
Figure 8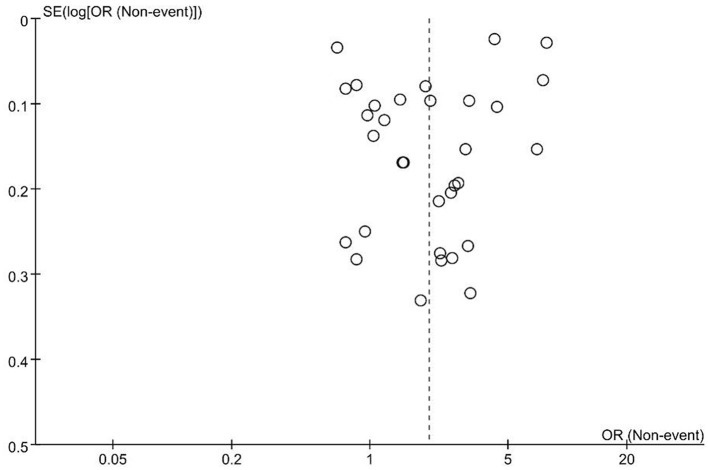 Figure 9
Figure 9|
|
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|---|---|
| Shanafelt et al. ( | 2016 | United States | Physicians and other clinician staff | 6,560 | 3,586 | 54.66 | MBI | 19.2 |
| Tawfik et al. ( | 2014 | United States | Physicians | 1,934 | 517 | 26.73 | MBI | 70 |
| Tawfik et al. ( | 2015 | United States | Physicians and other clinician staff | 1,5505 | 5,065 | 32.67 | MBI | 70.4 |
| Kroth et al. ( | 2015 | United States | Physicians | 41 | 5 | 12.00 | Other | Not reported |
| Kutney-Lee et al. ( | 2021 | United States | Nurses | 1,2004 | 3,160 | 26.30 | MBI | Not reported |
| Olson et al. ( | 2016 | United States | Physicians | 557 | 267 | 47.94 | MBI | 44 |
| Tai-Seale et al. ( | 2016 | United States | Physicians | 919 | 331 | 36.02 | mini-Z | 71.13 |
| Apaydin et al. ( | 2016 | United States | Physicians and other clinician staff | 116 | 62 | 53.45 | MBI | Not reported |
| Livaudais et al. ( | 2016 | United States | Physicians and other clinician staff | 281 | 127 | 45.20 | Other | 44 |
| Tran et al. ( | 2017 | United States | Physicians and other clinician staff | 107 | 41 | 38.32 | mini-Z | 56 |
| Marckini et al. ( | 2017 | Canada and United States | Physicians | 110 | 44 | 40.00 | MBI | 28.7 |
| Gardner et al. ( | 2017 | United States | Physicians | 1792 | 465 | 25.95 | mini-Z | 42.7 |
| Hilliard et al. ( | 2017 | United States | Physicians and other clinician staff | 422 | 116 | 27.49 | mini-Z | 39.3 |
| Higgins et al. ( | 2017 | United States | Residents | 230 | 86 | 37.39 | Other | Not reported |
| Czernik et al. ( | 2017 | United States | Residents | 84 | 30 | 35.71 | Other | 67 |
| Melnick et al. ( | 2017 | United States | Nurses | 1,282 | 539 | 42.00 | MBI | 9.9 |
| Domaney et al. ( | 2017 | United States | Psychiatry Residents and Faculty | 40 | 25 | 62.50 | MBI | Not reported |
| Hauer et al. ( | 2018 | United States | Physicians | 1,165 | 624 | 53.56 | mini-Z | 8.86 |
| Gajra et al. ( | 2018 | United States | Physicians | 163 | 109 | 67.00 | Other | Not reported |
| Adler-Milstein et al. ( | 2018 | United States | Physicians | 122 | 44 | 36.07 | MBI | 37 |
| Somerson et al. ( | 2018 | United States | Residents | 203 | 78 | 38.42 | MBI | Not reported |
| Melnick et al. ( | 2018 | United States | Physicians | 870 | 397 | 45.63 | MBI | 69.6 |
| Coleman et al. ( | 2018 | United States | Physicians | 872 | 360 | 41.28 | MBI | 34.3 |
| Abraham et al. ( | 2018 | United States | Nurses | 396 | 100 | 25.25 | mini-Z | Not reported |
| Kondrich et al. ( | 2018 | Canada and United States | Physicians | 416 | 206 | 49.52 | MBI | 59.4 |
| Kroth et al. ( | 2019 | United States | Physicians and other clinician staff | 282 | 127 | 45.04 | Other | 44.1 |
| Tajirian et al. ( | 2019 | Canada | Physicians and trainee | 208 | 51 | 24.52 | mini-Z | 43.8 |
| Mandeville et al. ( | 2019 | United States | Physicians and other clinician staff | 2,468 | 539 | 21.84 | mini-Z | 39.5 |
| Tiwari et al. ( | 2019 | United States | Physicians and other medical staff | 128 | 65 | 50.8 | MBI | Not reported |
| Sinha et al. ( | 2019 | United States | Physicians | 856 | 276 | 32.24 | Other | 73 |
| Anderson et al. ( | 2019 | United States | Physicians and trainee | 756 | 373 | 49.34 | MBI | 9.2 |
| McPeek-Hinz et al. ( | 2019 | United States | Physicians | 1,310 | 681 | 52.00 | MBI | 3.3 |
| Nair et al. ( | 2019 | United States | Physicians | 457 | 106 | 23.19 | MBI | Not reported |
| Jha et al. ( | 2020 | United States | Physicians and other medical staff | 100 | 52 | 52.00 | Other | 55.9 |
| Esmaeilzadeh and Mirzaei ( | 2020 | Iran | Physicians and other medical staff | 368 | 134 | 36.41 | Other | Not reported |
| Holzer et al. ( | 2020 | United States | Physicians and trainee | 222 | 84 | 37.84 | Other | 16.2 |
| Baxter et al. ( | 2020 | United States | Physicians | 609 | 307 | 50.40 | mini-Z | 60.4 |
| Wilkie et al. ( | 2021 | Canada | Physicians | 103 | 41 | 39.80 | MBI | 40.9 |
| Almulhem et al. ( | 2021 | Saudi Arabia | Physician trainees | 182 | 73 | 40.10 | mini-Z | Not reported |
| Lou et al. ( | 2021 | United States | Physician trainees | 75 | 32 | 42.70 | Other | Not reported |
| Tajirian et al. ( | 2023 | Canada | Physicians | 128 | 20 | 15.60 | mini-Z | 50 |
|
|
|
|
|
|
|---|---|---|---|---|
| Tawfik et al. | Cross-sectional | NICU with ≥10 weekly admissions, nursing care workload, and patient mortality | Burnout recognition education; implementation of burnout interventions at the individual and institutional level | Using EHR outside working or at home; time on using EHR |
| Shanafelt et al. | Cross-sectional | Using CPOE female gender, emergency medicine, each additional hour per week | Assistant order entry; documentation support | Time spent on clerical tasks |
| Tawfik et al. | Cross-sectional | HIT frustration, difficulty in falling asleep | Supplemental EHR training; scribes to assist documentation; team-based documentation and inbox management; automating data-entry tasks | Frustrated or stressed by EHR |
| Kroth et al. | Cross-sectional | Inefficient user interfaces, unpredictable system response times, poor interoperability between systems and excessive data entry | HICT and clinic architectural and process redesign | Proficiency with EHR use; Sufficient time for documentation |
| Kutney-Lee et al. | Cross-sectional | Employing EHR systems with suboptimal usability | EHR usability | EHR adoption level and teaching status |
| Olson et al. | Cross-sectional | Poor control over workload, inefficient teamwork, lack of value alignment with leadership, and hectic-chaotic work atmosphere | Improve professional satisfaction; nonphysician order entry | Using EHR outside working or at home; insufficient documentation time |
| Tai-Seale et al. | Cross-sectional | Female gender and poor control over work schedule | Feeling highly valued; having good control over work schedule; working in a quiet or busy but reasonable environment; assist physician with email work; limit desktop medical work outside working hours (except in emergencies) | Using EHR outside working or at home; number of EHR system-generated in basket messages |
| Apaydin et al. | Cross-sectional | Managing unscheduled or same-day patients, lack of pharmacist support, administrative work, excessive overall workload, difficulty communicating with other professionals, inadequate care coordination, and answering patient emails | Interventions to facilitate provider-led quality improvement | Managing in-basket messages generated by EHR; responding to EHR alerts |
| Livaudais et al. | Cross-sectional | Negative perceptions of EHR | Perceiving positive effect of EHR in practice; technical support for EHR when using systems; EHR optimization program | Managing in-basket messages generated by EHR; poor EHR design; dealing with patient-call messages in systems |
| Tran et al. | Cross-sectional | Clinical full-time equivalents >0.9 and more incomplete messages in inbox | Perception positive attitudes about the effect of EHR or satisfied with EHR | Average additional 10 minutes spent on EHR after each visit; less efficient at completing EHR and inbox information |
| Marckini et al. | Cross-sectional | Female gender and dissatisfaction for clerical tasks | EHR optimization; improving physician efficiency; and job satisfaction | Managing in-basket messages generated by EHR; dissatisfaction with EHR |
| Gardner et al. | Cross-sectional | Primary care specialties, female gender, and reporting poor or marginal time for documentation | Perception positive attitudes about the effect of EHR or satisfied with EHR | Excessive data inputting in EHR; using EHR at home; frustrated with EHR |
| Hilliard et al. | Cross-sectional | High volume of patient call messages in the system and lack of control over workload | Copy and paste used in EHR documentation; assist with inbox tasks and create 2 administrative “desktops” | Using EHR outside working or at home; excessive data inputting in EHR; managing in-basket messages generated by EHR |
| Higgins et al. | Cross-sectional | Self-compassion, sleep disorder, lacking support from leaders, and poor control over schedules | Peer support, perceived appreciation and meaningfulness in work; maintaining values consistent with practice institution | Poor EHR usability; perception negative attitudes about the effect of EHR |
| Czernik et al. | Cross-sectional | Frustrated or stressed by EHR | Reducing the burden of documentation tasks; improving EHR usability; interventions to improve the EHR | Poor usability of EHR; information overload; degradation of medical documentation |
| Melnick et al. | Cross-sectional | lower emotional exhaustion scores, depersonalization scores, and overall rates of burnout | Standardized technical availability | Improving EHR usability |
| Domaney et al. | Cross-sectional | emotional exhaustion, depersonalization, and low sense of personal accomplishment | The total time spent using EHR per week is 22 hours | |
| Hauer et al. | Cross-sectional | Loss of practicing autonomy, female gender, frustrated with EHR, and increasing insurance and government regulation | Improve the functionality of EHR; enhance physician leadership and involvement; create a center for physician empowerment; create a physician health program | Using EHR outside workday |
| Gajra et al. | Cross-sectional | Variable reimbursement models, interactions with payers, and increasing treating and caring demands | Use advanced practice providers; hire additional administrative staff; invest in information technology | Excessive data inputting in EHR; frustrated or stressed by EHR; using EHR outside workday |
| Adler-Milstein et al. | Cross-sectional | Poor self-rated EHR skills | Improve EHR design; scribe or team documentation; reduce documentation requirements | Using EHR outside working or at home; time spent on EHR; system-generated in-basket messages (>114) per week |
| Somerson et al. | Cross-sectional | Working >80 hours per week, verbal abuse from faculty, educational debt, “scut” work >10 hours per week | Nursing support; duty-hour restrictions; improving EHR functionality and efficiency; adequate, personalized training and support; adequate social work support | Time spent on EHR per week; used EHR >20 hours per week |
| Melnick et al. | Cross-sectional | Practice location (academic medical center) and medical specialty | Improve EHR usability | Using EHR outside working or at home; poor EHR usability |
| Coleman et al. | Cross-sectional | Work-related physical pain, work-home conflict, and younger age | Build personal resilience, enhance wellness; peer support; reduce administrative or EHR burden | Using EHR outside working or at home; increased EHR or documentation requirement |
| Abraham et al. | Cross-sectional | Intraorganizational factors | EHR with multifunctional; reduce high EHR workload; work with supportive colleagues; improve team communication | High EHR workload |
| Kondrich et al. | Cross-sectional | Feeling undervalued by patients, lacking superior support, little promotion chances, perceived unfair clinical working schedule, and nonacademic environment | Improve physician well-being | Feeling that the EHR detracts from patient care |
| Kroth et al. | Cross-sectional | Overall stress | Improve EHR design; clinician training; scribes to assist documentation; work at home boundaries; exercise, taking breaks | Information overloading; slow system response; excessive data inputting; fail to navigate quickly; note bloat; patient- clinician relationship interference; fear of missing something; billing oriented notes. |
| Tajirian et al. | Cross-sectional | Workflow issues | Reduce the administrative burden of EHR; improve EHR | Lower satisfaction and higher frustration with the EHR; poor intuitiveness and usability of EHR |
| Mandeville et al. | Cross-sectional | HIT-related stress and burnout and emergency medicine | Improved workflow | Daily frustration added by EHR; using EHR outside working or at home |
| Tiwari et al. | Cross-sectional | Lack of physical exercise and weekly working hours | Teamwork and working satisfaction; self-care training | Poor EHR usability; dissatisfaction with EHR |
| Sinha et al. | Cross-sectional | Interpersonal disengagement | Lower CLOC ratio (total CLOC time to allocated appointment time); well-established personal resources | Using EHR outside working |
| Anderson et al. | Cross-sectional | Female gender, younger age, shorter practicing years, and having children at home | Taking 20 days or more of vacation time | Using EHR at home; ≥2-hour patient administration |
| McPeek-Hinz et al. | Cross-sectional | The gender of the bed doctor | The local work culture | The time spent after work |
| Nair et al. | Cross-sectional | Working long hours, weekly number of nursing patients, practice environment, disinterested health systems, and dissatisfaction with remuneration | Caring for fewer patients per week | Using EHR outside working or at home; EHR requirements |
| Jha et al. | Cross-sectional | COVID-19 pandemic and in-house billing | Stay positive; improved EHR design | Documentation through EHR |
| Esmaeilzadeh and Mirzaei | Cross-sectional | Less direct communication with patients, inadequate training for using HIT, and increasing computerization at work | Positive perceptions of EHR; more policy and legal interventions to ensure meaningful use of EHR | Poor EHR usability; time spent entering data |
| Holzer et al. | Cross-sectional | Receive COVID-19 patients | Using EHR to streamline clinical care activities; physician task relief | Using EHR outside work; increased EHR workload |
| Baxter et al. | Cross-sectional | Medical conditions, expletives and/or profanity | NLP analyses of inbasket messages at scale | EHR inbox messages |
| Wilkie et al. | Cross-sectional | High workload and insufficient resources | Good leadership; prioritize work-life balance | Poor EHR usability |
| Almulhem et al. | Cross-sectional | Daily work increases the sense of frustration | Further research should be conducted to explore possible solutions | Remote EHR use |
| Lou et al. | Cross-sectional | The clinical workload of EHR | Mitigate sustained elevations of work responsibilities | Total EHR usage time, patient load, and chart review time |
| Tajirian et al. | Cross-sectional | Daily frustration | Streamlining prescription processes, enhancing search functionalities, and addressing system inefficiencies | Medication reconciliation and prescription processes; chart navigation and information retrieval; longitudinal medication history; technology infrastructure challenges. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsElectronic Health Records Systems · Artificial Intelligence in Healthcare and Education · Hospital Admissions and Outcomes
Introduction
With the accelerating process of digitalization in healthcare, the electronic health record (EHR) has become an indispensable tool in modern medical systems. Its value in enhancing healthcare quality, optimizing clinical workflows, and promoting information sharing has been widely recognized (1–3). However, the widespread adoption of EHRs is also accompanied by a series of potential issues, among which the exacerbation of professional burnout among healthcare personnel is a significant concern. Professional burnout not only reduces the efficiency of healthcare services and compromises patient safety but also leads to increased turnover rates among healthcare professionals, posing a severe challenge to the stability of the healthcare system (4–6).
Currently, numerous studies have explored the association between EHRs and professional burnout among healthcare personnel, but existing research has several limitations. Most studies focus on a single group of healthcare professionals (such as physicians or nurses), lacking a holistic analysis of multiple groups (including physicians, nurses, technicians, administrative staff). This makes it difficult to comprehensively reveal the commonalities and differences in how EHRs contribute to burnout across different professional roles. For example, one report including only physicians stated that spending excessive time on documentation and workflows is a primary cause of professional burnout (7). Another study on family physicians showed that approximately 25% were highly dissatisfied with the usability and satisfaction of their EHR system (8). For Advanced Practice Registered Nurses (APRNs), 50.3% strongly indicated that EHRs increased their daily frustration, contributing to professional burnout (9). On the other hand, existing research has largely been confined to phenomenological descriptions and associative analyses (10, 11), lacking a systematic identification of the modifiable key factors contributing to EHR-related burnout. Additionally, research on effective mitigation strategies for EHR-related burnout is scarce and fragmented. One study offered practical suggestions for addressing EHR-related burnout only within a Canadian healthcare organization (12), while mitigation strategies targeting professional burnout across multiple groups of healthcare personnel are particularly insufficient.
This study employs systematic review and meta-analysis to synthesize global research findings. For the first time, it incorporates multiple groups of healthcare personnel into a unified analytical framework to systematically evaluate the impact of EHRs on professional burnout, clarify the strength of this association, analyze differences across various job roles and identify key risk factors. The findings will provide evidence-based insights for EHR system optimization and for healthcare institutions in developing mitigation strategies for professional burnout, offering a scientific basis for optimizing EHR applications and alleviating burnout among healthcare professionals.
Methods
Protocol and registration
This systematic review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Definition of burnout
In this study, the definition of professional burnout is primarily based on the Maslach Burnout Inventory-Human Services Survey (MBI-HSS) (10, 13). This instrument assesses burnout across three dimensions: emotional exhaustion, depersonalization, and reduced personal accomplishment. Using the definition of burnout from the original study. The specific criteria for high levels of burnout in each dimension were defined as follows: a score of ≥27 for high emotional exhaustion, a score of >10 for high depersonalization, and a score of < 33 for low personal accomplishment. Additionally, some studies in our review defined burnout using alternative instruments, such as the Stanford Physician Well-being Survey (14) or the mini-Z. We categorized the included studies based on the measurement tool and the specific definition of burnout they employed.
Search strategy
A systematic literature search was conducted in PubMed, Embase, and Web of Science for relevant English-language articles published between January 1, 2005, and July 31, 2025. To retrieve literature on EHR systems, the following search terms were used: “electronic health record,” “EHR,” “EMR,” “computerized physician order entry,” “CPOE,” “clinical decision support system,” and “CDSS.” For the concept of burnout, the terms “burnout,” “burn-out,” “alert fatigue,” and “exhaustion” were employed. To define our study population, a range of healthcare professionals was considered, including “physicians,” “doctors,” “medical staff,” “nurses,” “clinicians,” “medical student,” and “healthcare professional.” These terms were combined using Boolean logic. The detailed search strategy is available in Supplementary Table 1.
Inclusion and exclusion criteria
Inclusion criteria
Studies that assessed EHR-related burnout using MBI-HSS, mini-Z, or other self-report measures.Studies that examine the use of general EHR systems or specific supportive systems, such as CPOE.Studies that evaluated burnout among healthcare professionals and their individual psychological responses to EHR systems.
Exclusion criteria
Duplicate publications.Literature not relevant to EHRs or occupational burnout.Non-original research articles, including qualitative studies, editorials, commentaries, conference abstracts, and letters.Studies with an unclear description of the methodology or an unclear definition of EHR-related outcomes.
Data extraction and synthesis
To ensure the integrity and reliability of the data, enhance the efficiency of data extraction, and minimize subjective bias, two reviewers with different professional backgrounds independently performed the study selection (inclusion and exclusion process), quality assessment, and data extraction. The following data were extracted from the eligible studies: first author, publication year, country, study design, total sample size, and study outcomes. The primary outcome was whether professional burnout occurred among physicians, nurses, or residents as reported in cross-sectional studies.
Risk of bias assessment
Two reviewers assessed the completeness, verifiability, and quality of the included studies using the Joanna Briggs Institute (JBI) checklist (15) (Supplementary Table 2) and the Newcastle-Ottawa Scale (NOS) (16).
Statistical analysis
Literature screening was performed using EndNote X9 software, and meta-analysis was conducted using Review Manager 5.4 software. Heterogeneity was assessed using the I^2^ statistic, with statistical significance set at P < 0.05. If no significant statistical heterogeneity was present (I^2^ < 50%), a fixed-effect model was used to pool the results; otherwise (I^2^ ≥ 50%), a random-effects model was employed (16). Continuous variables were summarized using the mean and standardized mean difference (SMD), while rates were extracted for categorical variables. For cross-sectional studies, the effect size measure was the OR value for burnout and its corresponding 95% confidence interval (CI). We further conducted subgroup analyses based on the burnout assessment tools and different groups of healthcare professionals. Publication bias was assessed using a funnel plot. After excluding outliers, small studies, and high risk-of-bias studies, sensitivity analysis was conducted to reduce the bias.
Results
Literature search and study selection
A total of 2,640 articles were identified through a combination of database searches and manual retrieval. The database search was conducted across PubMed, Embase, and Web of Science, supplemented by 17 articles found through manual searching. After an initial screening of titles and abstracts, 1,520 articles were excluded for the following reasons: 896 were unrelated to EHRs or professional burnout; 134 were not original research articles; 45 were qualitative studies; and 445 were editorials, conference abstracts, or letters. The remaining 212 articles underwent full-text review, which led to the further exclusion of 171 articles: 109 were found to be unrelated to EHRs or professional burnout upon full-text assessment, and 62 had unclear methodology or an undefined EHR-related outcome. Ultimately, 41 studies met the inclusion criteria and were included in the meta-analysis for the subsequent evaluation of the impact of EHRs on professional burnout among various groups of healthcare professionals (Figure 1).
Study selection process.
Characteristics of the included studies
The final analysis included 41 studies, published between 2005 and 2025, conducted across regions in Canada, the United States, Iran, and Saudi Arabia. These studies collectively comprised 54,443 healthcare professionals. The sample sizes of the included studies varied considerably, ranging from 40 to 15,505 participants, with response rates ranging from 3.3% to 71.13%. The most used assessment tool for burnout was the MBI-HSS, which was utilized in 19 of the 41 studies (46.3%). Additionally, 11 studies (26.8%) employed the mini-Z burnout assessment (Table 1).
Meta-analysis of included studies
The meta-analysis examining the association between EHR use and burnout risk included 41 studies with a total of 54,443 healthcare professionals. The heterogeneity test indicated substantial heterogeneity among the studies (I^2^ = 99%), leading to the application of a random-effects model. The results demonstrated that EHR use was significantly associated with an increased risk of professional burnout, with a pooled Odds Ratio (OR) of 2.49 (95% CI: 1.82–3.41, p < 0.00001) (Figure 2). Publication bias was assessed using a funnel plot, which revealed no significant publication bias. The points in the funnel plot were symmetrically distributed, and there was no statistically significant evidence of publication bias (Figure 3). Detailed results of the quality evaluation are presented in Supplementary Table 3.
Meta-analysis of the association between EHR use and professional burnout.
Funnel plot for publication bias.
Subgroup analysis based on burnout assessment tools
Three distinct burnout assessment tools were identified among the included studies: the MBI-HSS, the mini-Z, and other instruments. Due to the presence of significant heterogeneity within each subgroup (I^2^ > 50%), a random-effects model was applied for all analyses. The subgroup analysis revealed that the occurrence rate of burnout was highest in studies using other tools (39.3%), followed by those using the MBI-HSS (36.0%) and was lowest in studies employing the mini-Z (31.8%) (Figure 4). However, these differences in occurrence rate among the three assessment methods were not statistically significant (p = 0.10). Publication bias was assessed using funnel plots, which showed a symmetrical distribution of points, suggesting no significant publication bias (Figure 5).
Subgroup analysis based on burnout calculation methods.
Funnel plot for publication bias.
Subgroup analysis based on healthcare professional populations
The included studies were categorized into three primary groups based on the study population: physicians, nurses, and residents. Given the significant heterogeneity observed within each of these subgroups (I^2^ > 50%), a random-effects model was utilized for all meta-analyses. The subgroup analysis confirmed a significant association between EHR use and professional burnout across all three populations. Specifically, the pooled OR was 2.31 (95% CI: 1.63–3.27, p < 0.00001) for physicians, 2.77 (95% CI: 2.15–3.56, p < 0.00001) for residents, and 5.05 (95% CI: 1.81–14.13, p = 0.002) for nurses (Figure 6). While the numerical OR values suggest a potentially stronger association among nurses, the differences between these population subgroups were not statistically significant (p = 0.33).
Subgroup analysis based on healthcare professional populations.
From a descriptive standpoint, the overall burnout prevalence observed within each population was 38.1% for physicians, 37.5% for residents, and 27.8% for nurses. We emphasize that these prevalence figures represent the absolute burden of burnout within each cohort, whereas the pooled ORs specifically reflect the strength of association between EHR use and burnout risk. A funnel plot assessment suggested no significant evidence of publication bias (Figure 7).
Funnel plot for publication bias.
Main causes of burnout and proposed solutions
We have summarized the factors contributing to burnout among healthcare professionals related to EHR use in Table 2. Poor design and usability of the EHR system were identified as the primary contributing factors. Furthermore, spending excessive time on EHR-related tasks outside of working hours, suboptimal EHR design, redundant alerts, and cumbersome workflows were also identified as key drivers of burnout for healthcare professionals. Among the 41 included studies, 20 specifically mentioned workload factors as a significant exacerbating element of this issue. Additionally, several effective measures to mitigate burnout were proposed. These include optimizing EHR design, increasing the use of scribes to assist with documentation, providing targeted training for clinicians, and implementing mandatory rest periods.
Sensitivity analysis
To ensure the robustness of our findings, a sensitivity analysis was conducted by excluding nine studies identified as outliers, small-scale, or having a high risk of bias. This analysis encompassed 48,750 healthcare professionals, with a descriptive burnout prevalence of 36.8% (17,925/48,750). Despite significant heterogeneity (I^2^ = 99%), the random-effects model confirmed that the association between EHR use and increased risk of occupational burnout remained significant (OR = 1.98, 95% CI: 1.40–2.80, p < 0.00001) (Figure 8). No significant publication bias was observed (Figure 9). These results demonstrate that the association is stable and not driven by external factors such as study quality or size. The persistent high heterogeneity likely reflects clinical and methodological variations across studies, such as diverse study populations and burnout assessment instruments.
Sensitivity analysis.
Funnel plot for publication bias.
Discussion
EHR is a comprehensive system for storing patient health information in a digital format. It is designed to be accessible across healthcare institutions and updated in real-time, encompassing the full lifecycle of patient data-including medical history, diagnoses, medications, and laboratory results. The primary goals of EHR implementation are to enhance healthcare quality, optimize service workflows, and promote information coordination. However, poor design and suboptimal application of EHRs can also increase the documentation burden and contribute to burnout among healthcare professionals (4, 17, 18). Burnout is characterized by three core dimensions: emotional exhaustion, depersonalization (or cynicism), and a reduced sense of personal accomplishment (19). This condition not only leads to decreased work efficiency and lower quality care but also places a significant physical and psychological strain on healthcare workers (20, 21). Our meta-analysis reveals a significant association between EHR use and an increased risk of burnout. Furthermore, it uncovers variations in burnout occurrence rates when assessed by different instruments and across different healthcare populations. However, these differences were not statistically significant, suggesting that EHR-related burnout is a pervasive issue affecting multiple groups within the healthcare workforce. Nevertheless, the implementation of targeted, modifiable mitigations tailored to specific healthcare populations has the potential to reduce the incidence of burnout.
MBI-HSS is one of the most widely used instruments for assessing occupational burnout, particularly among healthcare professionals (22). Our subgroup analysis indicated that studies utilizing the MBI-HSS reported a relatively high occurrence rate of burnout. This can likely be attributed to the MBI-HSS's comprehensive, three-dimensional assessment of burnout, which measures emotional exhaustion, depersonalization, and reduced personal accomplishment (22). Each dimension of the scale has well-defined, objective cutoff values, which helps to mitigate the subjective bias inherent in self-reported burnout. In contrast, mini-Z is a brief assessment tool that typically focuses on core burnout symptoms, such as emotional exhaustion and job satisfaction. Due to its limited number of items, it may have lower sensitivity in identifying mild burnout during rapid screening, potentially leading to the relatively lower occurrence rates it reports (23). Other tools included in our analysis comprised non-standard assessment instruments, such as the Stanford Physician Wellness Survey and various custom-designed questionnaires. These tools often have broader assessment scopes and may conflate general work-related fatigue with the specific syndrome of burnout, which could contribute to an inflation of the reported occurrence rates. Although there were numerical differences in the occurrence rates across the three tools, these differences were not statistically significant, indicating that occupational burnout is prevalent regardless of the assessment tool used.
This study confirms through Meta-analysis that the use of EHR is significantly associated with an increased risk of occupational burnout among healthcare workers (OR = 2.49), which was also supported by the results of sensitivity analysis (OR = 1.98). This finding is highly consistent with the results of Wu et al. (13) (OR = 2.43), collectively revealing the robustness of EHR as a driver of occupational burnout. Of particular note is that our analysis, as well as the study by Wu et al., clearly indicates that the time spent on EHR-related tasks outside of working hours is a key and quantifiable risk factor for burnout. Evidence from case-control studies suggests that performing more than 6 h of EHR charting work outside of working hours significantly increases the risk of burnout (24). This “invisible overtime” not only erodes the personal time of healthcare workers, directly leading to emotional exhaustion, but also blurs the boundaries between work and life, serving as one of the core mechanisms triggering occupational burnout.
In terms of the occurrence of EHR-related occupational burnout, the rate among physicians was slightly higher than that among residents and nurses, although the difference across these three groups was not statistically significant. This suggests that the impact of EHRs on burnout is a pervasive issue across multiple healthcare professional groups, with flaws in EHR system design and the significant number of additional hours spent on these systems being common contributing factors. Previous systematic reviews have indicated that research on EHR-related burnout has predominantly focused on physicians (5). As the primary decision-makers in patient care, physicians are required to use EHRs to perform high-frequency and complex documentation tasks, such as recording patient histories, entering orders, and writing progress notes. This demanding and burdensome documentation workload also diminishes physicians' satisfaction with the EHR, a finding consistent with the research of Shanafelt et al. (25). Our review summarizes that a primary cause of burnout among physicians is the excessive time spent on EHRs, which can amount to over 20 additional hours per week and is often completed outside of regular working hours (e.g., at night or on weekends). This form of “invisible overtime” directly exacerbates emotional exhaustion. Furthermore, mandatory, non-essential fields and repetitive alerts within EHR systems can undermine a physician's sense of personal accomplishment, thereby amplifying feelings of burnout. These factors may represent the core reasons for their slightly higher occurrence rate (26). For residents, the need to cope with high-intensity rotating schedules, in addition to spending extra time on EHR-related tasks, is a likely contributor to increased occupational burnout, which aligns with conclusions from prior studies (27, 28). Nurses, in contrast, primarily use EHRs to document the nursing process, a task set that is relatively more standardized and less complex than the comprehensive documentation required of physicians. This may partially account for their lower observed burnout occurrence. However, research indicates that the daily frustrations caused by the EHR and insufficient time for documentation remain key factors contributing to burnout among nurses (9).
This systematic review identifies several potentially modifiable factors that are associated with a reduced risk of EHR-related burnout. However, it is important to note that these strategies are derived primarily from cross-sectional studies and represent observational associations or author recommendations rather than interventions validated by randomized controlled trials (RCTs). Among the proposed measures, the deployment of medical scribes currently holds the most observational support across multiple studies for reducing physician documentation burden. EHR interface optimization and workflow improvements are frequently recommended to enhance efficiency but lack validation through controlled trials. Additionally, while AI/NLP-based documentation assistance shows promise, it remains largely at the expert recommendation stage with emerging pilot data. For physicians, the deployment of dedicated medical scribes or digital documentation solutions has been associated with reduced documentation burden and may be a promising strategy. Furthermore, optimizing the EHR user interface and navigation may enhance workflow efficiency and professional satisfaction (5). For residents, strengthening EHR-specific training has been proposed to lower adaptation barriers and foster a greater sense of mastery and accomplishment, potentially mitigating early-career burnout (29). For nursing staff, developing intuitive, user-friendly nursing documentation modules and streamlining communication workflows have been proposed as potentially beneficial approaches to alleviate daily frustrations caused by EHR interactions (30). Additionally, advancements in artificial intelligence (AI) and natural language processing (NLP) hold promise for automating documentation tasks (31), such as summarizing clinical conversations, drafting clinical notes, and intelligently prioritizing inbox messages (32). However, the application of NLP is not without limitations, such as challenges related to data imbalance (33). Future prospective cohort studies and RCTs are warranted to establish the causal effectiveness and long-term impact of these proposed strategies.
This systematic review has several limitations. First, while the high observed heterogeneity is not uncommon in meta-analyses of occurrence rate, it suggests potential variations in methodologies, definitions of “burnout,” and cultural contexts across the included studies. A random-effects model was used for the pooled analysis in this study because of the extremely high heterogeneity. Although the pooled estimate cannot be interpreted as a single, unified quantitative reference value, it nonetheless demonstrates a clear and statistically meaningful directional trend. In the sensitivity analyses, the direction of the pooled effect size remained consistent, indicating coherence in the overall trend of the study outcomes. Importantly, the high degree of heterogeneity did not alter the direction of the study's main conclusions. Second, the current body of research is predominantly concentrated in North America, which may limit the generalizability of our findings to other healthcare systems. Furthermore, most of the studies were cross-sectional in design, which precludes the establishment of definitive causal relationships. Future research should prioritize prospective cohort studies to better establish causality. There is also a need for greater focus on non-physician groups, particularly nurses and other allied health professionals, as their patterns of EHR interaction and unique sources of stress remain understudied. Finally, evaluating the effectiveness of various targeted mitigations for these specific populations represents a critical next step for the field. In the future, we will undertake actual research in this direction.
Conclusion
This systematic review and meta-analysis demonstrate that EHR use is significantly associated with an increased risk of occupational burnout across multiple healthcare professional groups, including physicians, nurses, and residents. Primary contributing factors identified include poor EHR design, excessive documentation time demands, and heavy administrative burdens. Targeted mitigation strategies, such as EHR system optimization and the deployment of medical scribes, show potential in reducing burnout among physicians. For nursing staff, developing intuitive documentation modules and streamlining communication workflows may help alleviate occupational stress. These findings provide a critical evidence base for healthcare institutions to optimize EHR implementation and develop tailored interventions. Future prospective studies and RCTs are essential to validate the causal effectiveness of these proposed mitigation approaches.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Huber MT Highland JD Krishnamoorthi VR Tang JW. Utilizing the electronic health record to improve advance care planning: a systematic review. Am J Hosp Palliat Care. (2018) 35:532–41. doi: 10.1177/104990911771521728627287 · doi ↗ · pubmed ↗
- 2Gatiti P Ndirangu E Mwangi J Mwanzu A Ramadhani T. Enhancing healthcare quality in hospitals through electronic health records: a systematic review. J Health Informatics Dev Ctries. (2021) 15:11–25.
- 3Woldemariam MT Jimma W. Adoption of electronic health record systems to enhance the quality of healthcare in low-income countries: a systematic review. BMJ Health Care Inform. (2023) 30:e 100704. doi: 10.1136/bmjhci-2022-10070437308185 PMC 10277040 · doi ↗ · pubmed ↗
- 4Tajirian T Stergiopoulos V Strudwick G Sequeira L Sanches M Kemp J . The influence of electronic health record use on physician burnout: cross-sectional survey. J Med Internet Res. (2020) 22:e 19274. doi: 10.2196/1927432673234 PMC 7392132 · doi ↗ · pubmed ↗
- 5Alobayli F O'Connor S Holloway A Cresswell K. Electronic health record stress and burnout among clinicians in hospital settings: a systematic review. Digit Health. (2023) 9:20552076231220241. doi: 10.1177/2055207623122024138130797 PMC 10734365 · doi ↗ · pubmed ↗
- 6Budd J. Burnout related to electronic health record use in primary care. J Prim Care Community Health. (2023) 14:21501319231166921. doi: 10.1177/2150131923116692137073905 PMC 10134123 · doi ↗ · pubmed ↗
- 7Kruse CS Mileski M Dray G Johnson Z Shaw C Shirodkar H. Physician burnout and the electronic health record leading up to and during the first year of COVID-19: systematic review. J Med Internet Res. (2022) 24:e 36200. doi: 10.2196/3620035120019 PMC 9015762 · doi ↗ · pubmed ↗
- 8Holmgren AJ Hendrix N Maisel N Everson J Bazemore A Rotenstein L . Electronic health record usability, satisfaction, and burnout for family physicians. JAMA Netw Open. (2024) 7:e 2426956. doi: 10.1001/jamanetworkopen.2024.2695639207759 PMC 11362862 · doi ↗ · pubmed ↗