A pathological classification for predicting recurrence and guiding adjuvant therapy in esophageal squamous cell carcinoma following neoadjuvant immunochemotherapy: a two-center cohort study
Jiaming Huang, Hongsheng Xie, Guiqing Zeng, Manhong Yao, Zhifeng Zhang, Zhekai Zhang, Qijun Zheng

TL;DR
This study proposes a new classification system to predict recurrence and guide treatment for esophageal cancer patients after immunochemotherapy.
Contribution
A novel pathological classification system based on tumor regression grade and ypN status to guide adjuvant therapy decisions in ESCC patients.
Findings
TRG and ypN status were identified as independent predictors of recurrence-free survival.
A subgroup (TRG0-1 ypN+) showed significant survival improvement with adjuvant therapy.
Four prognostic subgroups were defined based on TRG and ypN status.
Abstract
Neoadjuvant immunochemotherapy (nICT) has emerged as a promising treatment modality for locally advanced esophageal squamous cell carcinoma (ESCC). However, optimal post-nICT adjuvant strategies remain undefined, and a classification system that integrates both prognosis and recurrence patterns to guide treatment decisions is currently lacking. This retrospective study enrolled 283 patients with locally advanced ESCC who underwent nICT with R0 resection between January 2019 and December 2023 at two participating institutions. The primary endpoint was recurrence-free survival (RFS). Secondary endpoints included recurrence patterns, overall survival (OS), locoregional recurrence-free survival (LRFS), and distant metastasis-free survival (DMFS). Survival curves were generated using the Kaplan-Meier method. Propensity score matching was employed for group comparisons and a Cox proportional…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
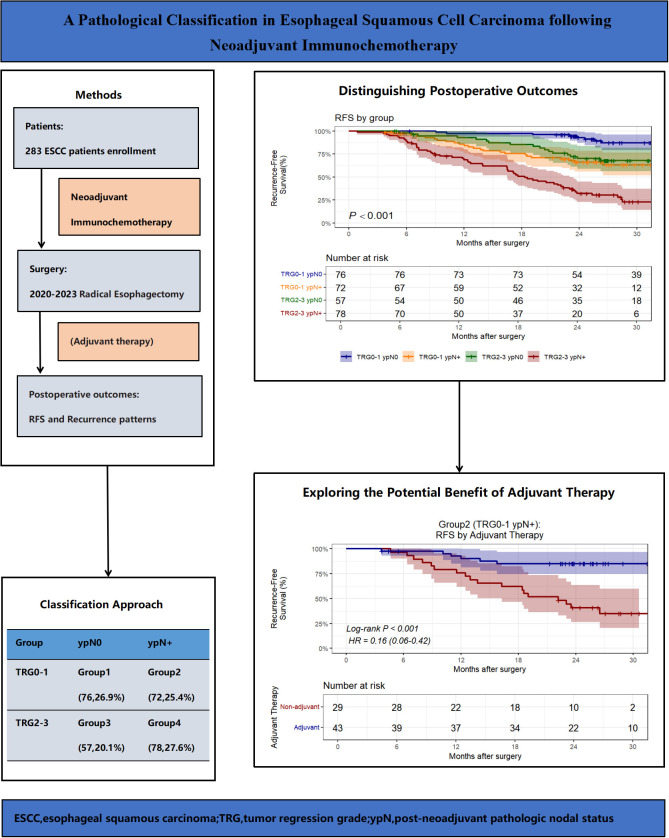 Figure 1
Figure 1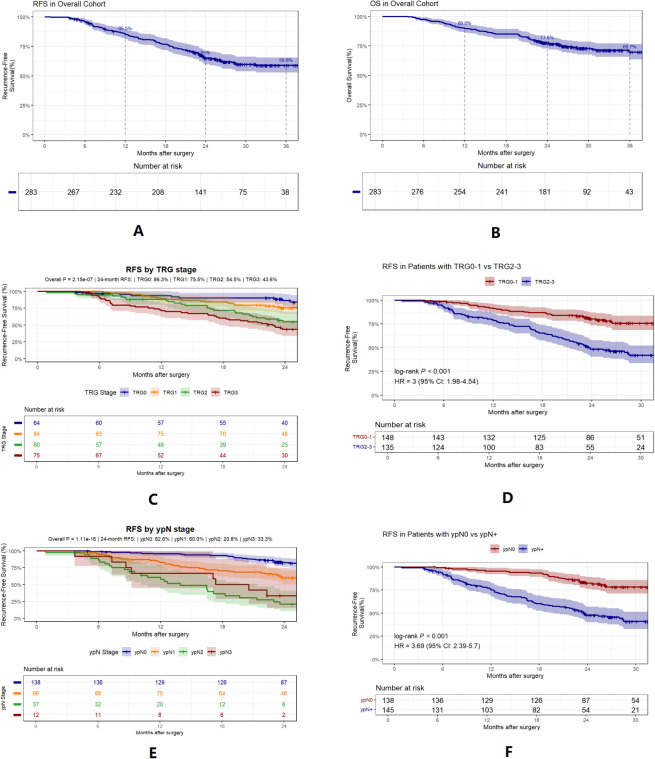 Figure 2
Figure 2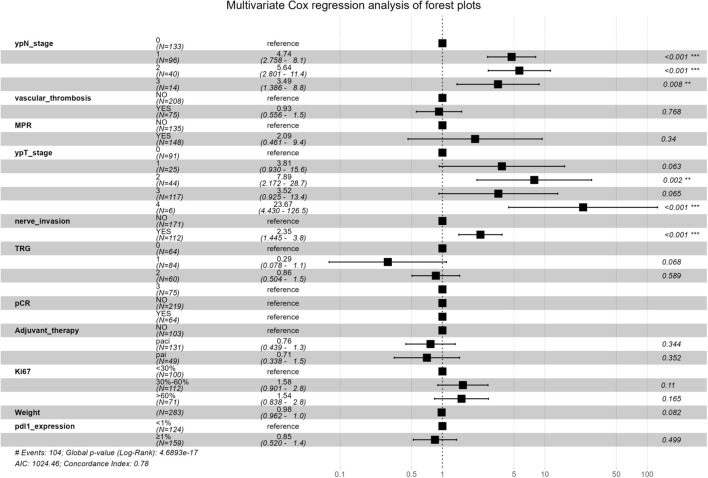 Figure 3
Figure 3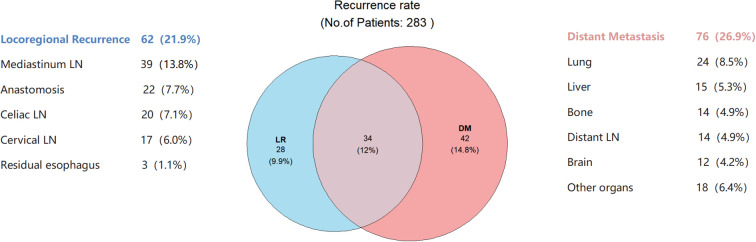 Figure 4
Figure 4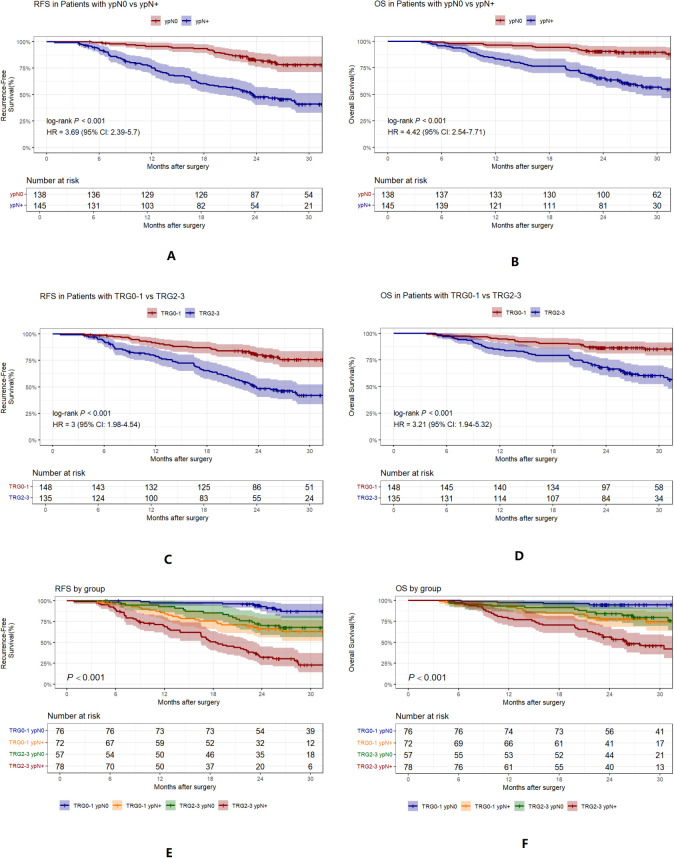 Figure 5
Figure 5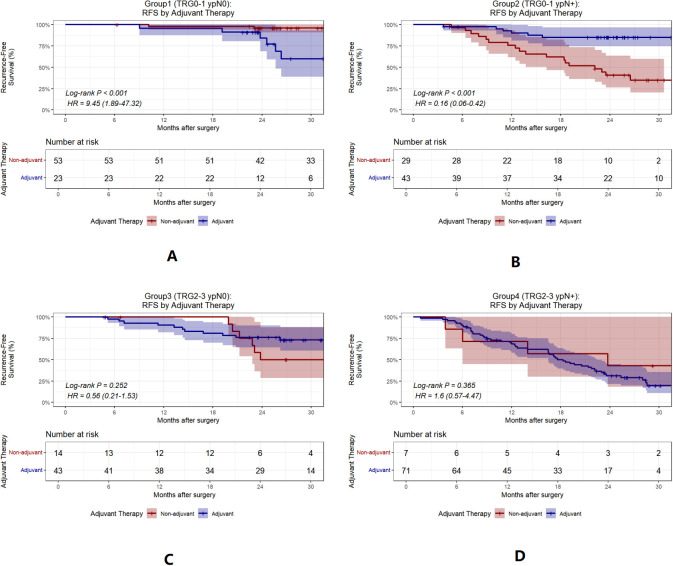 Figure 6
Figure 6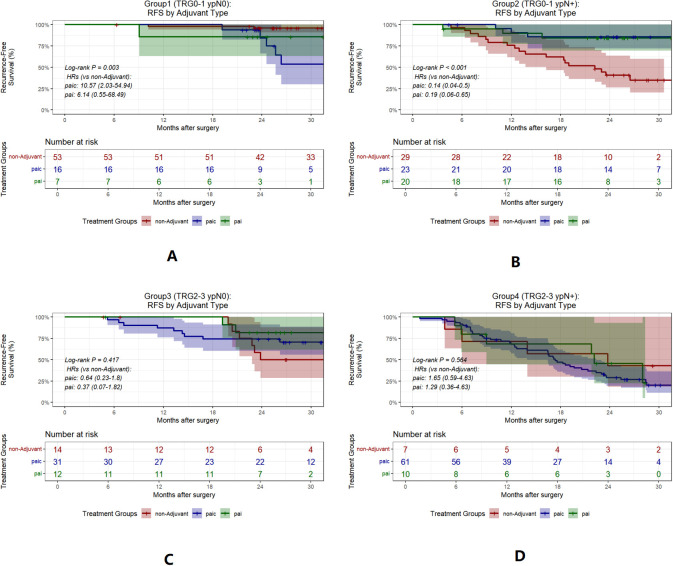 Figure 7
Figure 7| Characteristic | N = 283 |
|---|---|
| Sex, n (%) | |
| Female | 87 (30.7%) |
| Male | 196 (69.3%) |
|
| 67.2 ± 7.2 |
|
| 55.9 ± 10.1 |
|
| 162.4 ± 7.4 |
|
| 21.1 ± 3.3 |
|
| |
| Upper thoracic | 31 (11.0%) |
| Middle thoracic | 153 (54.1%) |
| Lower thoracic | 99 (35.0%) |
|
| 4.8 ± 1.9 |
|
| |
| Karelizumab | 138 (48.8%) |
| Tirelizumab | 39 (13.8%) |
| Srolizumab | 31 (11.0%) |
| Sindilizumab | 30 (10.6%) |
| Teraplizumab | 23 (8.1%) |
| Navulizumab | 22 (7.8%) |
| Neoadjuvant Chemotherapy, n (%) | |
| Paclitaxel* + Carboplatin | 156 (55.1%) |
| Paclitaxel* + Cisplatin | 109 (38.5%) |
| Other | 18 (6.4%) |
|
| |
| 2 | 175 (61.8%) |
| 3-4 | 108 (38.2%) |
| ypT stage, n (%) | |
| 0 | 91 (32.2%) |
| 1 | 25 (8.8%) |
| 2 | 44 (15.5%) |
| 3 | 117 (41.3%) |
| 4a | 6 (2.1%) |
| ypN stage, n (%) | |
| 0 | 133 (47.0%) |
| 1 | 96 (33.9%) |
| 2 | 40 (14.1%) |
| 3 | 14 (4.9%) |
| Tumor regression grade, n (%) | |
| 0 | 64 (22.6%) |
| 1 | 84 (29.7%) |
| 2 | 60 (21.2%) |
| 3 | 75 (26.5%) |
|
| 25.5 ± 11.0 |
|
| 64 (22.6%) |
|
| 148 (52.3%) |
|
| 112 (39.6%) |
|
| 75 (26.5%) |
| PD-L1 expression, n (%) | |
| <1% | 124 (43.8%) |
| ≥1% | 159 (56.2%) |
| Ki-67 index, n (%) | |
| <30% | 100 (35.3%) |
| 30%-60% | 112 (39.6%) |
| >60% | 71 (25.1%) |
| Recurrence pattern, n (%) | |
| No recurrence | 179 (63.3%) |
| LR | 28 (9.9%) |
| DM | 42 (14.8%) |
| LR+DM | 34 (12.0%) |
| Adjuvant therapy, n (%) | |
|
| 103 (36.4%) |
|
| 131(46.3%) |
|
| 49 (17.3%) |
| Pattern | Group1(TRG0-1 ypN0)(N=76) | Group2(TRG0-1 ypN+)(N=72) | Group3(TRG2-3 ypN0)(N=57) | Group4(TRG2-3 ypN+)(N=78) |
|
|---|---|---|---|---|---|
| Recurrence | 8 (10.5) | 25 (34.7) | 17 (29.8) | 54 (69.2) | < 0.001 |
| LR | 1 (1.3) | 9 (12.5) | 4 (7.0) | 14 (17.9) | 0.005 |
| DM | 4 (5.3) | 12 (16.7) | 7 (12.3) | 19 (24.4) | 0.009 |
| LR+DM | 3 (3.9) | 4 (5.6) | 6 (10.5) | 21 (26.9) | < 0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal Cancer Research and Treatment · Cancer Immunotherapy and Biomarkers · Colorectal and Anal Carcinomas
Introduction
Esophageal cancer is a highly prevalent gastrointestinal malignancy, ranked eighth in incidence and sixth in mortality among all cancers worldwide (1–3), that poses a significant threat to human health. In China, the incidence and mortality rates of esophageal cancer are among the highest globally, with squamous cell carcinoma accounting for over 90% of cases (4–8). Most patients are diagnosed at a locally advanced stage. The primary treatment for locally advanced ESCC involves neoadjuvant therapy followed by surgery (9–12), with options including neoadjuvant chemotherapy (nCT), neoadjuvant chemoradiotherapy (nCRT), and neoadjuvant immunochemotherapy (nICT). nICT has shown promise in the treatment of locally advanced ESCC (13), and its efficacy and safety have been demonstrated in several clinical trials (14). Although the pCR rate with nICT is lower than that with nCRT, R0 resection rates are comparable (15). Moreover, nICT may offer a superior long-term prognosis compared with nCRT (16–20), making it a suitable option for high-risk patients or those averse to radiotherapy.
However, the optimal adjuvant strategy following nICT and radical esophagectomy remains uncertain (21–25). With diverse options such as radiotherapy, chemotherapy, and immunotherapy, selecting the best postoperative treatment is controversial. Consequently, there is an urgent need for a classification system to aid postoperative prognostic assessment and to guide treatment decisions. Current stratification methods often rely on ypTNM staging combined with surrogate endpoints, such as pathological complete response (pCR) and major pathological response (MPR) (26–29). However, the prognostic discriminatory power of ypTNM can be diminished by the “downstaging” effect of neoadjuvant therapy. pCR and MPR are unidimensional metrics and thus fail to fully capture the multidimensional risk of recurrence. These methods are suboptimal for predicting postoperative recurrence and are insufficient for guiding treatment.
To address these limitations, we developed a novel prognostic stratification model based on TRG and ypN status and explored the potential benefits of adjuvant therapy by analyzing postoperative pathological data and outcomes (Figure 1).
Overview of the study design, key findings, and implications.
Methods
The study was approved by the Ethics Committees of Jieyang People’s Hospital (No.2025062) and Shenzhen People’s Hospital and was conducted in accordance with the principles of the Declaration of Helsinki. The requirement for informed consent was waived due to the retrospective nature of the study.
Study design and patient population
This retrospective study included patients with locally advanced ESCC (cT1-2N1-3 M0 or cT3-4aN0-3 M0, according to criteria from the AJCC, 8th edition) who underwent R0 resection after receiving nICT at Jieyang People’s Hospital or Shenzhen People’s Hospital between January 2019 and December 2023.
Exclusion criteria were: a) history of other malignancies within 5 years; b) incomplete clinical or pathological data; c) non-squamous cell carcinoma or mixed histology; d) neoadjuvant therapy not involving chemotherapy combined with immune checkpoint inhibitors e) non-R0 resection; and f) death due to surgical complications or other causes within a 3-month perioperative period.
Study endpoints
The primary endpoint was recurrence-free survival (RFS), defined as the time from surgery to confirmed or highly suspected recurrence or death from any cause. The secondary endpoints included recurrence pattern, overall survival (OS), locoregional recurrence-free survival (LRFS), and distant metastasis-free survival (DMFS). All survival times were calculated starting from the date of surgery.
pCR was defined as ypT0N0M0 or ypTisN0M0, and MPR was defined as ≤10% residual tumor in the primary lesion, according to AJCC 8th edition criteria. Tumor regression grading (TRG) was assessed using AJCC 8th edition criteria: TRG0 (no residual tumor), TRG1 (single cells or rare small groups of cancer cells), TRG2 (more than single cells or rare small groups of cancer cells with evident tumor regression), and TRG3 (extensive residual tumor or no regression) (30, 31).
Treatment and follow-up
All tumors were deemed resectable or potentially resectable prior to treatment and patients received 2–4 cycles of nICT consisting of a taxane-platinum doublet combined with a PD-1/PD-L1 inhibitor. Following neoadjuvant therapy, 95.3% of the patients underwent McKeown esophagectomy and 25.6% underwent three-field lymphadenectomy. R0 resection was achieved in all surgeries, and postoperative radiotherapy was not routinely administered. Specific adjuvant treatment regimens were determined through multidisciplinary team discussions, considering the tumor stage (ypT, ypN), pCR/MPR status, patient age, performance status (PS) scores, and patient preferences. Adjuvant therapy was initiated within 1 to 2 months of surgery. In most cases, 2-4 cycles postoperative cycles of adjuvant chemotherapy were administered and adjuvant immunotherapy was maintained for 1 year. Patients of the two centers were followed up every three months for the first two years post-surgery and every six months thereafter. Follow-up examinations included enhanced CT of the neck, chest, and upper abdomen; tumor marker assays; and gastroscopy or PET-CT when indicated. No patients who were missing follow-ups/attritions were included in this study.
Definitions and location of recurrence
Recurrence patterns were categorized as locoregional recurrence (LR), distant metastasis (DM), or synchronous recurrence (LR+DM); the latter was defined as recurrences occurring within one month of each other. According to the AJCC 8th edition criteria, LR refers to recurrence at the anastomosis, residual esophagus, gastric conduit, or regional lymph nodes diagnosed via gastroscopy, PET-CT, enhanced CT, or biopsy. DM refers to lymph node or organ involvement outside the locoregional area, as confirmed by PET-CT, enhanced CT, or biopsy.
Statistical analysis
Categorical variables are presented as counts and percentages; continuous variables are expressed as mean ± standard deviation if normally distributed, or median and interquartile range otherwise. The Kaplan-Meier method was used to estimate the RFS and OS. Survival curves were compared using the log-rank test and pairwise comparisons were adjusted using the Bonferroni method. All analyses were performed using R software (version 4.4.3). Statistical significance was defined as a two-sided P value of < 0.05.
To reduce confounding in the assessment of adjuvant therapy, propensity score matching (PSM) was employed. The covariates included age, ypT stage, ypN stage, and TRG, which were selected a priori based on clinical relevance. A 1:1 nearest-neighbor matching algorithm with a caliper width of 0.2 was used without replacement. Covariate balance before and after matching was assessed using standardized mean differences.
Univariate and multivariate Cox proportional hazards models were used to identify factors associated with postoperative RFS in the entire cohort. Variables with P < 0.05 in univariate analysis, along with clinically relevant variables (e.g. adjuvant therapy), were included in the multivariate model. Stratification into risk groups was based on key prognostic factors identified by multivariate Cox modeling, considering clinical relevance.
Results
Patient characteristics and outcomes
In total, 283 patients were enrolled between January 2019 and December 2023 (Supplementary Figure A1). Table 1 summarizes baseline characteristics and treatments. The pCR and MPR rates for the entire cohort were 22.6% and 52.3%, respectively. Figure 2 shows RFS and OS curves for the total population.
Kaplan-Meier curves for survival outcomes. (A, B), RFS and OS in the overall cohort. (C, D), RFS stratified by tumor regression grade(TRG). (E, F), RFS stratified by post-neoadjuvant pathologic nodal status(ypN).
After PSM, 68 matched pairs were included in the overall assessment of the efficacy of adjuvant therapy. Covariates were well-balanced post-matching, as indicated by the standardized mean differences (Supplementary Figures A2, A3). The baseline characteristics were generally comparable between the matched cohorts (Supplementary Table A1). In the matched cohorts, no statistically significant difference in RFS was observed between the patients who received adjuvant therapy and those who did not (Supplementary Figures A4, A5).
Factors affecting postoperative recurrence
Univariate Cox regression analysis identified weight, TRG, pCR, MPR, ypT status, ypN status, nerve invasion, vascular thrombosis, pdl1 expression and Ki-67 as significant variables (Supplementary Figure A6, Supplementary Table A2). Multivariate analysis confirmed TRG and ypN stage as independent factors affecting RFS (Figure 3, Supplementary Table A3).
HR > 1 indicates that the factor is a risk factor for increased recurrence risk, HR < 1 indicates a protective factor. The dashed line (HR=1) is the reference line for no effect. MPR, major pathologic response; TRG, tumor regression grade; pCR, pathologic complete response.
Recurrence patterns and influencing factors
The median follow-up was 25.8 months (range 5.8–56.3 months). Recurrence occurred in 104 of the 283 patients (36.7%), with distant metastasis being the most common pattern (Figure 4).
Distribution of recurrence sites. The blue and light red circles represent patients with LR and DM, respectively; overlaps indicate synchronous recurrence. Side annotations show recurrence sites and case counts, with percentages indicating their proportion of the total cohort. LR, Locoregional recurrence; DM, distant metastasis; LN, lymph nodes.
Classification methods and postoperative outcomes
Further analysis showed that TRG status was highly correlated with RFS. For ease of analysis, TRG was divided into TRG0-1 and TRG2-3 (Figures 2C, D). Further analysis revealed that patients with ypN1, ypN2, or ypN3 stage disease had significantly worse RFS than those with ypN0 stage disease. However, the differences between ypN1 and ypN3 stages were not significant (Figures 2E, F). Consequently, ypN status was dichotomized into ypN0 and ypN+ for subsequent analyses.
Based on these findings and the clinical rationale, we proposed a classification method incorporating TRG and ypN status, dividing the patients into four subgroups: Group1 (TRG0-1 ypN0; n=76; 26.9%), Group 2 (TRG0-1 ypN+; n=72; 25.4%), Group 3 (TRG2-3 ypN0; n=57; 20.1%), and Group 4 (TRG2-3 ypN+; n=78; 27.6%) (Table 2). Figure 5 illustrates survival stratified by ypN status and TRG (A-D), and by the combined groups (E-F). Group 1 had the best prognosis, while Group 4 had the worst, and Groups 2 and 3 exhibited intermediate prognoses.
Kaplan-Meier curves for RFS and OS, stratified by TRG, ypN, and group. (A, B), RFS and OS by ypN0 vs ypN+. (C, D), RFS and OS by TRG0-1 vs TRG2-3. (E, F), RFS and OS by group. TRG, tumor regression grade.
Efficacy of adjuvant therapy by group
To evaluate how this classification informs adjuvant therapy, we reanalyzed treatment outcomes by subgroup. In Group 2, adjuvant therapy was associated with significantly improved RFS (HR = 0.16, 95% CI 0.06–0.42, P<0.001)(Figure 6). We further analyzed the differences in postoperative adjuvant treatment modalities and found that both postoperative adjuvant immunochemotherapy and postoperative adjuvant immunotherapy benefited group 2 (TRG0-1 ypN+) (Figure 7).
Kaplan-Meier curves for RFS by adjuvant therapy in each group. (A–D), RFS by adjuvant vs non-adjuvant therapy in groups 1 to 4. Non-adjuvant, No adjuvant therapy; adjuvant, postoperative adjuvant immunochemotherapy or postoperative adjuvant immunotherapy. TRG, tumor regression grade.
Kaplan-Meier curves for RFS by adjuvant type in each group. (A–D), RFS by paic, pai vs non-adjuvant therapy in groups 1 to 4. Non-adjuvant, No adjuvant therapy; paic, postoperative adjuvant immunochemotherapy; pai, postoperative adjuvant immunotherapy. TRG, tumor regression grade.
Discussion
nICT has transformed the management of locally advanced ESCC; however, the postoperative recurrence risk and adjuvant strategies remain unclear. This study developed and validated a simple binary classification system based on TRG and ypN status to aid postoperative prognostic assessment and guide adjuvant therapy. Lin et al. (32) also reported the use of MPR and ypN status to predict recurrence risk after nICT. Compared to MPR, TRG offers a more detailed reflection of the tumor response to nICT. Biologically, TRG and lymph node responses are correlated with distinct processes, both of which are associated with a poor prognosis. This combination provides a more comprehensive assessment of the efficacy of neoadjuvant therapy efficacy (31). In our propensity-matched cohort, adjuvant therapy did not confer a survival benefit on the overall population, suggesting limitations of the current empiric adjuvant regimens. However, as this was a retrospective study where adjuvant therapy was primarily administered to patients with high-risk features, the observed benefits could be limited, and the results should be interpreted cautiously.
Current post-nICT decisions rely heavily on ypTNM staging and surrogate endpoints, such as pCR/MPR (28, 29, 33). However, the prognostic power of ypTNM is often attenuated by neoadjuvant “downstaging”, and although the unidimensional metrics pCR and MPR (34–36)identify favorable responders, they are insufficient for comprehensively assessing recurrence risk (24, 37, 38). Our study confirmed that TRG and ypN status are mutually independent prognostic predictors. TRG can reflect the effect of primary tumor lesions, and the ypN status can reflect changes in lymph nodes after nICT. TRG 0-1 corresponds to an MCR, indicating high treatment efficacy, whereas TRG 2-3 indicates poor or no pathological response. A combination of these factors revealed profound tumor heterogeneity. Group 1 (TRG0-1 ypN0) represented a “favorable response” cohort, sensitive to systemic therapy with no nodal residue; their excellent prognosis suggests that a “watch-and-wait” approach may be most appropriate, avoiding overtreatment. Group 4 (TRG2-3 ypN+) constituted a “high-risk subgroup”, combining primary resistance with metastatic potential, clearly defining an ultra-high-risk group warranting exploration of intensive adjuvant therapies (e.g., novel ADC agents, combined radiotherapy). In Group 2 (TRG0-1 ypN+), adjuvant therapy significantly improved RFS (HR = 0.16, 95% CI 0.06–0.42, P<0.001), indicating that this subgroup derived substantial benefit, potentially extending the gains of immunotherapy. Group 3 (TRG2-3 ypN0) had an intermediate prognosis and did not benefit from postoperative adjuvant therapy. Recurrence risks in this group might stem from localized micrometastases or hematogenous spread; tailoring adjuvant strategies (e.g. targeted radiotherapy to the primary site or modified systemic therapy) could be beneficial, but requires validation in larger studies.
Our data further confirm that the predominant failure pattern after nICT is distant metastasis rather than local recurrence. This contrasts with the higher local recurrence rates after nCRT and emphasizes that the core objective of any post-nICT adjuvant strategy should be to intensify systemic control. Our classification model, particularly the efficacy of adjuvant therapy in Group 2, likely reflects the successful systemic eradication of micrometastases, thereby reducing distant recurrence.
The limitations of this study include its retrospective design, limited sample size (particularly in certain subgroups), and the inability to assess postoperative radiotherapy, as it was not routinely performed. Furthermore, the median follow-up duration was only 25.8 months, which is relatively short for a definitive oncological prognosis. These limitations necessitate cautious interpretation of the results. Future prospective multicentre studies are warranted to validate this classification model.
In summary, the TRG-ypN binary classification system effectively differentiated the prognosis of patients with ESCC after nICT and identified subgroups likely to benefit from adjuvant therapy. Although its clinical utility requires further prospective validation, this study offers a framework for personalized postoperative management.
Conclusion
Our classification system based on TRG and ypN status effectively stratified the prognosis of patients with ESCC following nICT and identified specific populations, such as TRG0-1 ypN+ patients, who may benefit from postoperative adjuvant therapy, thereby providing a valuable basis for individualized treatment decisions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wu Y He S Cao M Teng Y Li Q Tan N . Comparative analysis of cancer statistics in China and the United States in 2024. Chin Med J (Engl). (2024) 137:3093–100. doi: 10.1097/CM 9.0000000000003442, PMID: 39654104 PMC 11706596 · doi ↗ · pubmed ↗
- 2Wilson BE Wright K Sengar M Sullivan R Pearson SA Barton MB . Analysis of 2023 World Health Organization cancer Essential Medicines List and concordance with resource-stratified guidelines. J Natl Cancer Inst. (2025) 117:2010–20. doi: 10.1093/jnci/djaf 100, PMID: 40408185 PMC 12505124 · doi ↗ · pubmed ↗
- 3Qi L Sun M Liu W Zhang X Yu Y Tian Z . Global esophageal cancer epidemiology in 2022 and predictions for 2050: A comprehensive analysis and projections based on GLOBOCAN data. Chin Med J (Engl). (2024) 137:3108–16. doi: 10.1097/CM 9.0000000000003420, PMID: 39668405 PMC 11706580 · doi ↗ · pubmed ↗
- 4Diao X Guo C Jin Y Li B Gao X Du X . Cancer situation in China: an analysis based on the global epidemiological data released in 2024. Cancer Commun (Lond). (2025) 45:178–97. doi: 10.1002/cac 2.12627, PMID: 39659114 PMC 11833671 · doi ↗ · pubmed ↗
- 5Collatuzzo G Abe SK Rahman MS Parvin R Inoue M Boffetta P . Estimating the burden of cancer attributable to tobacco in Bangladesh in 2020. J Cancer Policy. (2025) 45:100614. doi: 10.1016/j.jcpo.2025.100614, PMID: 40619062 · doi ↗ · pubmed ↗
- 6Al-zahrani SA Morgan E Zahwe M Fouad H Bray F . Burden of five major types of gastrointestinal cancer in the Eastern Mediterranean Region. BMJ Open Gastroenterol. (2025) 12. doi: 10.1136/bmjgast-2024-001577, PMID: 39971587 PMC 11840892 · doi ↗ · pubmed ↗
- 7Zhou J Sun K Wang S Chen R Li M Gu J . Associations between cancer family history and esophageal cancer and precancerous lesions in high-risk areas of China. Chin Med J (Engl). (2022) 135:813–9. doi: 10.1097/CM 9.0000000000001939, PMID: 35026773 PMC 9276202 · doi ↗ · pubmed ↗
- 8Yang CS Chen XL . Research on esophageal cancer: With personal perspectives from studies in China and Kenya. Int J Cancer. (2021) 149:264–76. doi: 10.1002/ijc.33421, PMID: 33270917 PMC 8141013 · doi ↗ · pubmed ↗