Preferences for implementing training program among primary care physicians in prescribing and deprescribing for patients with multimorbidity: a discrete choice experiment
Leyi Jiang, Yu Xia, Liyan Han, Ming Yan, Xinmei Zhou, Ruoxia Zhang, Yiting Lu, Jiaying Yu, Guifen Zhang, Lingyan Wu, Yi Guo, Yuling Tong, Zhijie Xu

TL;DR
This study identifies what primary care physicians in China prefer in training programs for prescribing and deprescribing in patients with multiple chronic conditions.
Contribution
The study introduces a discrete choice experiment to uncover PCPs' preferences for training program implementation features.
Findings
PCPs prioritize training frequency, session duration, and instructor composition in training programs.
Optimizing preferred attributes can increase acceptance of weekly training by up to 66.75%.
Autonomous enrollment and multidisciplinary mentoring are key to improving participation.
Abstract
Primary care physicians (PCPs) have great needs of receiving training and potential to improve their capacities of prescribing and deprescribing for patients with multimorbidity. However, limited studies focused on PCPs’ preferences for how training program is implemented. This study used a discrete choice experiment (DCE) to investigate PCPs’ preferences for implementing training program in prescribing and deprescribing for patients with multimorbidity. This study surveyed PCPs in eastern China from October 10 to December 5, 2024 using an electronic questionnaire. Eight attributes and levels in a DCE were identified based on implementation science theory: instructor composition, teaching model, training location, participant enrollment, session duration, training frequency, assessment methods, and theoretical basis of the course. DCE data were analyzed using a mixed logit model to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
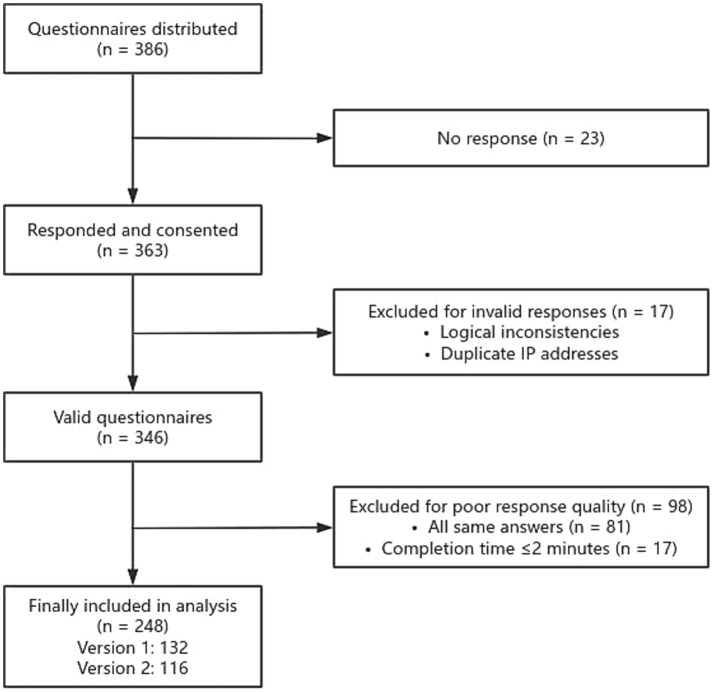 Figure 1
Figure 1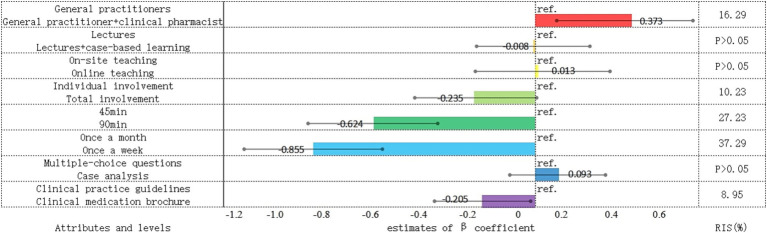 Figure 2
Figure 2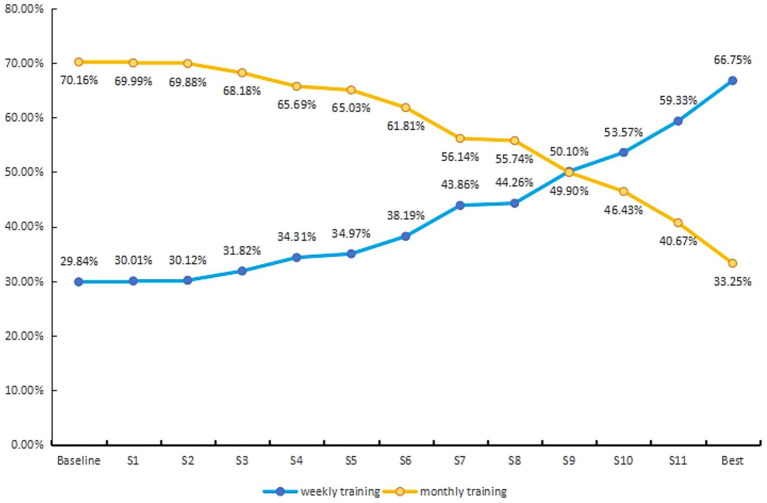 Figure 3
Figure 3| Attribute | Definition | Level | Code |
|---|---|---|---|
| Instructor composition | Professionals who offer courses; Structure of the teaching staff | a. General practitioners | 0 |
| b. General practitioner + clinical pharmacist | 1 | ||
| Teaching model | The model that the course is conducted | a. Lectures | 0 |
| b. Lectures + case-based learning | 1 | ||
| Training location | Whether the training is organized online or on-site | a. On-site teaching | 0 |
| b. Online teaching | 1 | ||
| Participant enrollment | Enrollment method of participants, i.e., the participants are involved individually or totally | a. Individual involvement | 0 |
| b. Total involvement | 1 | ||
| Session duration | Time required for a session | a. 45 min | 0 |
| b. 90 min | 1 | ||
| Training frequency | How often is each session conducted | a. Once a month | 0 |
| b. Once a week | 1 | ||
| Assessment methods | The way to measure participant learning outcomes after training, including multiple-choice questions and case analysis | a. Multiple-choice questions | 0 |
| b. Case analysis | 1 | ||
| Theoretical basis of the course | Main sources of pedagogical content in training courses and materials | a. Clinical practice guidelines | 0 |
| b. Clinical medication brochure | 1 |
| Training plan A | Training plan B | |
|---|---|---|
| Instructors composition | General practitioner | General practitioner + Clinical pharmacist |
| Teaching model | Lectures + Case-based learning | Lectures |
| Training location | Online teaching | On-site teaching |
| Participant enrollment | Individual involvement | Total involvement |
| Session duration | 90 min | 45 min |
| Training frequency | Once a week | Once a month |
| Assessment methods | multiple-choice questions | Case analysis |
| Theoretical basis of the course | Clinical practice guidelines | Clinical medication brochure |
| What is your choice? | ☑ | □ |
| Characteristics | Sub-groups | |
|---|---|---|
| Location | Suichang | 65 (26.2) |
| Daishan | 60 (24.2) | |
| Cixi | 60 (24.2) | |
| Kaihua | 46 (18.5) | |
| Hangzhou | 17 (6.9) | |
| Gender | Male | 125 (50.4) |
| Female | 123 (49.6) | |
| Age, y | ≤30 | 80 (32.3) |
| 31–40 | 71 (28.6) | |
| 41–50 | 66 (26.6) | |
| >50 | 31 (12.5) | |
| Duration of professional practice, y | ≤10 | 113 (45.6) |
| 11–20 | 80 (32.3) | |
| 21–30 | 36 (14.5) | |
| >30 | 19 (7.7) | |
| Scope of practice | General practice | 152 (61.3) |
| Clinical specialty | 64 (25.8) | |
| General practice plus clinical specialty | 32 (12.9) | |
| Professional title | Resident physician | 115 (46.4) |
| Attending physician | 79 (31.9) | |
| Associate chief physician | 38 (15.3) | |
| Chief physician | 16 (6.5) | |
| Educational background | High school or below | 43 (17.3) |
| Bachelor’s degree | 202 (81.5) | |
| Master’s degree or above | 3 (1.2) | |
| Participation in standardized residency training | Yes | 158 (63.7) |
| No | 90 (36.3) | |
| Involvement in family doctor contract services | Yes | 171 (69) |
| No | 77 (31) | |
| Geographical location of the institution | Rural | 162 (65.3) |
| Urban | 86 (34.7) | |
| Nature of the employing institution | General hospitals | 9 (3.6) |
| Township health center | 110 (44.4) | |
| Community health service center | 62 (25) | |
| Village clinic | 67 (27) | |
| Average daily patient encounters (patients/day) | ≤50 | 181 (73) |
| 51–100 | 55 (22.2) | |
| >100 | 12 (4.8) |
| Attributes and levels |
| 95%CI | SD | 95%CI | ||
|---|---|---|---|---|---|---|
| Lower | Upper | Lower | Upper | |||
| Instructors composition (Ref: General practitioner) | ||||||
| General practitioner + clinical pharmacist |
| 0.112 | 0.635 |
| 0.396 | 1.156 |
| Teaching model (Ref: lectures) | ||||||
| Lectures + Case-based learning | −0.008 | −0.226 | 0.210 | −0.068 | −0.559 | 0.424 |
| Training location (Ref: on-site teaching) | ||||||
| Online teaching | 0.013 | −0.247 | 0.273 |
| 1.142 | 1.908 |
| Participant enrollment (Ref: individual involvement) | ||||||
| Total involvement |
| −0.470 | 0.000 |
| −1.082 | −0.387 |
| Session duration (Ref: 45 min) | ||||||
| 90 min |
| −0.875 | −0.374 |
| 0.526 | 1.188 |
| Training frequency (Ref: once a month) | ||||||
| Once a week |
| −1.121 | −0.589 |
| 0.820 | 1.518 |
| Assessment methods (Ref: multi-choice questions) | ||||||
| Case analysis | 0.093 | −0.092 | 0.278 | 0.330 | −0.160 | 0.820 |
| Theoretical basis of the course (Ref: clinical practice guideline) | ||||||
| Clinical medication brochure |
| −0.390 | −0.020 | −0.302 | −0.767 | 0.162 |
| Log-likelihood | −894.515 | Pseudo-R2 | 0.132 | |||
| AIC | 1,823.030 | RLH mean | 0.526 | |||
| BIC | 1,925.002 | |||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Disease Management Strategies · Pharmaceutical Practices and Patient Outcomes · Primary Care and Health Outcomes
Introduction
Primary care physicians (PCPs) serve as key gatekeepers within the healthcare system, particularly in the management of patients with multimorbidity through the provision of continuous, coordinated, and accessible care. The quality of their prescribing practices directly influences patient safety and the efficient use of healthcare resources. However, evidence suggests that the prevalence of potentially inappropriate medications among older adults in primary care settings in China is as high as 39% (1). PCPs continue to face substantial challenges in both prescribing and deprescribing medications for patients with multimorbidity (2). Clinical decision-making is often complicated by factors such as drug–drug interactions, cognitive biases, and treatment burden. Additional barriers include patient resistance to changes in existing treatment regimens, limited access to continuing medical education, and time constraints during patient encounters (3).
These challenges are compounded by the escalating burden of multimorbidity worldwide. As chronic diseases become more prevalent and populations continue to age, the presence of multiple chronic conditions within individuals has emerged as a critical public health challenge (4–6). In China, the prevalence of multimorbidity among older adults has demonstrated an increasing trend over recent years, rising to 43% in 2023 (7). Among individuals with multimorbidity, polypharmacy and inappropriate medication use are widespread concerns (1). An increase in the number of prescribed medications is associated with a higher risk of drug–drug interactions, drug-disease interactions, and medication errors, collectively termed medication-related problems, which pose substantial threats to patient safety with consequences ranging from functional decline to mortality (8–10).
To address these challenges, the Chinese government has introduced a series of policies aimed at enhancing the quality of medical services as part of ongoing healthcare reforms (11). Among these initiatives, promoting rational drug use through professional training has been identified as a key strategy. Prior research indicates that well-designed training programs can significantly enhance prescribing accuracy and reduce the incidence of potentially inappropriate prescriptions (12, 13). However, training effectiveness depends not only on content but also on implementation formats that influence knowledge retention and participant engagement (14, 15). Accordingly, a comprehensive understanding of PCPs’ training preferences is essential for the development of a practical, effective, and sustainable competency-based training system.
Understanding PCPs’ implementation preferences is a prerequisite for designing interventions that achieve intended outcomes (16). Even expertly designed training content fails to improve practice if physicians do not participate or engage. From a theoretical perspective, training effectiveness depends on a causal chain in which implementation attributes influence participation decisions, participation enables knowledge acquisition, and knowledge translates into practice change (17). Within this chain, individual preferences function as the initial gateway determining whether training can exert any effect.
Equipped with concepts and tools from implementation science, this challenge can be systematically addressed. Defined as “the scientific study of methods to promote the systematic uptake of research findings and other evidence-based practices into routine practice” (18), implementation science offers theoretical frameworks and practical tools to identify and overcome barriers to implementation, adapt interventions to specific healthcare settings, and promote sustainable practice change (19). Rather than merely identifying what content PCPs wish to learn, we deconstruct training programs into discrete implementable attributes informed by implementation strategy frameworks. This approach enables quantification of preferences for specific design features and generates evidence for precise matching of implementation strategies to PCPs’ priorities (20). The significance therefore lies not only in describing preferences but in providing an empirical basis for designing theory-driven, contextually tailored interventions that can be systematically optimized and replicated.
However, research exploring PCPs’ preferences for how training programs should be implemented, particularly in prescribing and deprescribing for multimorbidity, remains limited. Existing studies have concentrated on content design and instructional method evaluation, with comparatively little attention to implementation preferences (13, 15, 21). This study utilizes a discrete choice experiment (DCE) to explore PCPs’ preferences regarding the implementation of training programs in prescribing and deprescribing for patients with multimorbidity. DCE is a multidimensional stated preference method that allows for the identification and quantification of participants’ trade-offs among competing attributes (22). DCE has been used to assess decision-making in areas ranging from disease screening to preferences for workforce incentives (23–25). By identifying the factors influencing PCPs’ preferences, this study aims to align training initiatives closely with their needs, potentially enhancing engagement and improving the feasibility and effectiveness of the programs.
Methods
This study employed a DCE to systematically investigate PCPs’ preferences regarding the implementation of training programs. DCE is particularly well-suited for this purpose, as it enables the quantification of the relative importance of multiple attributes by presenting respondents with realistic scenarios that require trade-offs between competing options (22). This multi-attribute decision-making framework aligns with the study’s objectives and supports the identification of optimal training configurations (26). Compared with traditional survey methods, which may struggle to capture the complexity of individual preferences with sufficient reliability and validity (27, 28), DCE provides a more robust and scientifically rigorous approach. In particular, the use of a mixed logit model facilitates accurate estimation of utility values while accounting for heterogeneity in respondent preferences across different training attributes.
This study involves human participants and was approved by the Second Affiliated Hospital of Zhejiang University School of Medicine Ethics Committee [approval no. (2024) Ethics Review Research no. (1485)], and the research was conducted in accordance with the principles outlined in the Declaration of Helsinki.
Study settings and population
Participants were recruited from 23 community health centers located in Hangzhou, Cixi, Daishan, Suichang, and Kaihua. Inclusion criteria were as follows: (a) licensed clinicians whose scope of practice includes general practice or internal medicine, and (b) those who had been employed at a community health center for at least 1 year. Physicians were excluded if they declined to provide informed consent or if they had no intention of participating in any future training programs.
Sample size estimation in this study utilized the established rule-of-thumb formula developed by Johnson and Orme (29): n > 500c/(t × a), where n represents the minimum required sample size, c denotes the largest number of levels across all attributes, t indicates the number of choice sets presented to each respondent, and a signifies the number of alternatives per choice set. Application of this formula yielded a minimum required sample size of respondents per questionnaire version. With two questionnaire versions implemented, the aggregate minimum sample size was determined to be 166 respondents. To compensate for anticipated invalid or incomplete responses (estimated at 20%), the target sample size underwent appropriate adjustment, establishing a final recruitment objective of at least 208 PCPs meeting eligibility criteria.
The design of DCE
Attributes and levels
The identification and specification of training attributes and their corresponding levels represent the foundational and most critical step in designing a DCE, as they play a pivotal role in uncovering the factors that influence training preferences. To comprehensively identify the attributes relevant to PCPs’ preferences for implementing the training program, this study employed a multi-step process, including a systematic review of the literature, structured group discussions, and qualitative interviews.
Based on the relevant literatures (28, 30–32), an initial candidate pool was formed, comprising instructor composition, teaching model, training location, participant enrollment, session duration, training frequency, assessment methods, theoretical basis of the course, training depth, training scale, accreditation type, and incentive mechanisms. Secondly, a panel of eight experts comprising primary care physicians, clinical pharmacists, medical educators, and implementation science researchers evaluated these candidates in structured discussions. Attributes were prioritized based on their potential influence on physician participation and alignment with implementation science frameworks (33). Training depth, training scale, accreditation type, and incentive mechanisms were removed due to limited variability or lower relevance, yielding a preliminary set of eight attributes. Thirdly, semi-structured interviews with 20 primary care physicians recruited from two community health centers confirmed the relevance of these attributes; feedback led to simplified wording for participant enrollment and theoretical basis of the course, with no attributes removed.
Following attribute identification, the corresponding levels were determined. For quantitative attributes including session duration and training frequency, levels were selected to reflect common continuing medical education practices in China and to present meaningful contrasts. Session duration was set at 45 min versus 90 min, with 45 min representing a standard session length in Chinese medical education and 90 min corresponding to a typical lecture or workshop block (34). Training frequency was defined as once a month versus once a week, reflecting differences in both session interval and overall course timeline, which in turn influences curriculum design and content organization (35). For qualitative attributes, levels were derived from existing practice patterns and expert consensus, ensuring each level represented a realistic and distinguishable training feature. The relevance and comprehensibility of all levels were confirmed during the qualitative interviews. This process yielded eight key attributes for use in the discrete choice experiment, as presented in Table 1.
All attributes in the DCE were categorical with two levels and were dummy-coded. For each attribute, the reference level was coded as 0 and the alternative level as 1, enabling straightforward interpretation of coefficients as the change in utility associated with moving from the reference to the alternative level.
Experiment design and choice set construction
Following the identification of relevant attributes and levels for the DCE, different attribute levels were systematically combined to generate hypothetical training implementation scenarios. If all possible combinations were included, a full factorial design with 8 attributes, each having 2 levels, would result in 2^8^ = 256 unique training alternatives. Pairing these alternatives into binary choice sets would yield a total of 32,640 possible combinations (i.e., 256 × 255/2), which would be impractical to present to respondents. To manage this complexity while preserving experimental efficiency, a fractional factorial design (FFD) was employed to construct a manageable set of choice scenarios. The design aimed to meet two essential criteria: (1) independence of attributes and (2) balanced representation, ensuring that each attribute level appeared with equal frequency across the experiment.
We used the orthogonal design function in IBM SPSS Statistics 25 to generate 12 distinct training implementation profiles that satisfied these criteria. A level-shifting approach was then applied to construct choice sets: for each profile, a second option was generated by incrementally shifting attribute levels (with wrap-around adjustment), creating paired alternatives. This process produced 12 binary choice sets. To minimize respondent fatigue and cognitive burden, the 12 choice sets were randomly divided into two versions of the questionnaire, with each version containing 6 DCE questions.
Questionnaire
The questionnaire consisted of two main sections (see Supplementary File 1). The first section collected information on PCPs’ demographic characteristics and work-related information, including variables such as age, educational background, practice location, and clinic workload. The second section comprised six DCE questions. Each choice task presented respondents with two hypothetical training program alternatives, characterized by varying levels of key attributes, such as course format, training location, course duration, and training frequency.
To enhance respondents’ comprehension of the DCE, the questionnaire included detailed descriptions of each attribute and its corresponding levels. A sample DCE question was provided prior to the main choice tasks to familiarize participants with the format and structure of the experiment. This introductory example aimed to ensure clarity and reduce potential misunderstandings during the selection process. Table 2 presents the sample question included in the questionnaire.
Data collection
Data collection for this study was conducted over a three-month period, from October 10 to December 5, 2024, across multiple regions in eastern China, including Hangzhou, Cixi, Daishan, Suichang, and Kaihua. A mixed approach combining both convenience and purposive sampling techniques was employed to ensure broad and diverse participation while targeting specific demographic groups relevant to the study’s objectives.
The survey was administered using Questionnaire Star,1 an online survey platform operated by Changsha Ranxing Information Technology Co., Ltd. This platform was selected for its comprehensive functionality, including features for survey distribution, data collection, and analysis. The use of an online platform allowed for efficient outreach across a wide geographical area. Upon creation of the questionnaire, an online link was generated through Questionnaire Star, which facilitated the distribution process. The health administrators of each community health centers were contacted to help promote the survey and encourage participation.
To ensure the quality and reliability of the responses, several measures were incorporated into the survey’s design. First, a minimum time engagement requirement of 90 s was set before respondents could submit their responses to discourage rushed answers and ensure that participants consider each question carefully. Second, the survey was structured to require completion of all items before submission, and if any questions were left unanswered, an error message would prompt the respondent to fill in the required fields. Third, the survey included built-in response validation for key demographic questions, such as age and education level, to avoid inconsistencies or erroneous data entries. Fourth, to minimize the potential for careless or low-quality responses, screening questions were embedded within the survey to identify disengaged respondents. Moreover, the collected data were exported for cleaning and analysis, during which research assistants reviewed and flagged any anomalies or questionable responses for exclusion.
Statistical analysis
The analytical procedure comprised two sequential phases. Demographic characterization was conducted using descriptive statistics via IBM SPSS Statistics 25.0. The DCE data underwent primary analysis through a mixed logit model implemented in Stata 17.0. The model was estimated using maximum simulated likelihood with 500 Halton draws. Consistent with random utility theory, the analytical framework presumes that respondents select alternatives offering maximum perceived utility. The utility function for each choice alternative is expressed as:
where U_ntj_ denotes the total utility of alternative j for individual n in choice task t. This utility function incorporates two components: (1) V_ntj_, the systematic utility component determined by observable attributes, and (2) ε_ntj_, the stochastic error term capturing unobservable factors. The systematic utility component V_ntj_ is specified as:
where β_k_ represents the coefficients corresponding to attributes X_ktj_, which denote the attribute levels for alternative j in choice task t. Attribute levels underwent appropriate coding prior to analysis, with specific coding specifications detailed in Table 1. The coefficient β_k_ provides information regarding both preference direction (through its sign) and preference intensity (through its magnitude) for the corresponding attribute level (25). Detailed specifications of the coding scheme, parameter distributions, and the exact model syntax are provided in Supplementary File 2.
To facilitate intuitive comprehension of attribute importance, Relative Importance Scores (RIS) were calculated. These scores derive from the maximum utility differential between attribute levels, weighted by their corresponding coefficients. Statistical significance of attribute coefficients (p-values) was systematically incorporated into RIS calculations to ensure valid interpretability of attribute importance hierarchies (24, 36).
Furthermore, scenario analysis was implemented to evaluate how attribute level modifications influence predicted choice probabilities. Predicted probabilities were calculated using the mean coefficient estimates from the mixed logit model, reflecting the preferences of an average respondent. We established a baseline scenario in which the weekly training option was assigned the low-preference level for all attributes, while the monthly option was assigned the low-preference level for all attributes except training frequency. For each attribute k, we then constructed an improved scenario by switching only that attribute in the weekly option to its high-preference level, leaving the monthly option unchanged. The utility for each option was calculated as described above. The probability of choosing the weekly option was then calculated using the binary logit formula:
Results
Participant characteristics
The electronic questionnaires were distributed to 386 PCPs, and 363 PCPs responded and agreed to participate (response rate: 94.0%). After excluding 17 questionnaires with invalid responses, including logical inconsistencies in age and work experience and duplicate IP addresses, 346 valid questionnaires were retained. Of these 346 valid questionnaires, 81 were excluded due to providing uniform responses across all choice sets, indicating a lack of engagement or potential misunderstanding of the DCE tasks. An additional 17 respondents were excluded for completing the questionnaire in under 2 min, suggesting insufficient response quality. After applying these exclusion criteria, data from 248 PCPs (71.7%) were retained for analysis. The two versions of the questionnaire received responses from 132 and 116 participants, respectively. The detailed screening process is illustrated in Figure 1. No statistically significant differences were found in the demographic characteristics between the two groups (p > 0.05), indicating comparability across versions.
Questionnaire screening flow diagram.
Participants ranged in age from 23 to 61 years, with a mean age of 37.7 years. The length of clinical practice varied from 1 to 42 years, with an average of 13.7 years. Most respondents specialized in general practice (61.3%), held the professional title of physician (46.4%), had attained a bachelor’s degree (81.5%), and were practicing in rural areas (65.3%). A majority had completed standardized residency training (63.7%) and were involved in family physician contracting services (69%). The average daily number of patients served by PCPs was 44. Detailed demographic characteristics of the participants are presented in Table 3. The demographic characteristics of our sample aligned broadly with those reported for primary care physicians in national health statistics, indicating an acceptable level of representativeness (37).
Preferences of PCPs for training implementation
The preference model was based on a total of 2,976 choice observations collected from 248 respondents. Sensitivity analyses compared the main analytic sample (n = 248, after excluding low-quality responses) with the full sample (n = 346). The direction of preferences for all attributes remained consistent between the two models. However, coefficients for significant attributes were substantially larger in the main analysis (e.g., training frequency: β = −0.86 vs. −0.35; session duration: β = −0.62 vs. −0.33), and model fit improved (McFadden’s pseudo-R^2^ increased from 0.046 to 0.132). Moreover, the preference for multidisciplinary instructors became statistically significant only after exclusion, while assessment method lost significance. These findings indicate that low-quality responses introduce noise and attenuate true preference estimates, supporting the validity of our exclusion criteria in reducing bias (see Supplementary Table 1 for full results).
Results from the mixed logit model indicated that five out of eight attributes demonstrated statistically significant effects relative to their respective reference levels, as detailed in Table 4. Based on the magnitude of their statistical significance, the attributes were ranked in the following order of importance: training frequency (37.29%), session duration (27.23%), instructor composition (16.29%), participant enrollment (10.23%), and theoretical basis of the course (8.95%). Besides, the teaching model, location, and assessment methods did not exhibit statistically significant effects on preferences (p > 0.05).
Among all factors, the training frequency emerged as the most influential determinant, with a relative importance score of 37.29%. Compared to a monthly training schedule, a weekly frequency significantly reduced preference among PCPs, nearly doubling the decline in utility (β = −0.86; 95% CI: −1.12 to −0.59). The second most influential factor was training duration, with a relative importance score of 27.23%; shorter sessions were clearly preferred over longer ones (β = −0.62; 95% CI: −0.87 to −0.37). Additionally, a collaborative instructional model involving both general practitioners and clinical pharmacists was associated with a significantly higher preference (β = 0.37; 95% CI: 0.11–0.64). By comparison, the attributes related to participant enrollment (β = −0.24; 95% CI: −0.47 to 0.00) and theoretical basis (β = −0.21; 95% CI: −0.39 to −0.02) were perceived as relatively less important by respondents.
The mixed logit model demonstrated good fit (McFadden’s pseudo-R^2^ = 0.132) and internal validity (mean RLH = 0.526). Robustness checks using alternative model specifications confirmed that the relative importance rankings of the five key attributes remained consistent with the main analysis (Supplementary File 3).
Random parameters were incorporated into the mixed logit model to estimate standard deviations (SDs), allowing for the assessment of preference heterogeneity among respondents. The results indicated that only five attributes (i.e., instructor composition, training location, target population, duration of training sessions, and training frequency) exhibited statistically significant SD estimates. This suggests that substantial heterogeneity existed in respondents’ preferences regarding these aspects of training program. The estimated coefficients and the relative importance scores for each attribute, derived from the mixed logit model, are presented in Figure 2.
PCPs’ preferences for implementing training programs. β, the average preferences of the study population; Ref, reference level; RIS, relative importance scores.
Changes in selection rates for training implementation
Based on the mixed logit model estimates, Figure 3 illustrates the dynamic changes in choice probabilities across different training implementation scenarios. In the baseline scenario, which consisted of the least preferred attribute levels (instruction by general practitioners alone, lectures combined with case-based learning, onsite delivery, mandatory group participation, 90-min sessions, assessment via multiple-choice questions, and reliance on the clinical medication brochure), the predicted choice probabilities were 70.16% for monthly training and 29.84% for weekly training, reflecting primary care physicians’ inherent aversion to high-frequency training formats.
Changes in selection rates for training implementation. The baseline scenario is characterized by low-preference levels (general practitioners, lectures + case-based learning, onsite teaching, total involvement, 90 min, multiple-choice questions, and clinical medication brochure); S1 = Lectures; S2 = Online teaching; S3 = Case analysis; S4 = Clinical practice guidelines; S5 = Individual involvement; S6 = General practitioners + clinical pharmacists; S7 = ‘General practitioners + clinical pharmacists’ + Individual involvement; S8 = 45 min; S9 = Individual involvement + 45 min; S10 = ‘General practitioners + clinical pharmacists’ + 45 min; S11 = ‘General practitioners + clinical pharmacists’ + Individual involvement + 45 min; Best = ‘General practitioners + clinical pharmacists’ + lectures + online teaching + individual involvement + 45 min + case analysis + clinical practice guidelines.
By adjusting each attribute of the weekly training option individually toward the more preferred levels, we quantified the marginal contribution of each feature to increasing participation willingness. The results showed that, among all single-attribute optimizations, reducing session duration from 90 to 45 min yielded the greatest marginal benefit, increasing the choice probability of weekly training by 14.42 percentage points to 44.26%. This finding indicates that when resources are constrained and simultaneous optimization of multiple design elements is infeasible, prioritizing the compression of single-session duration is the most efficient strategy for enhancing physicians’ willingness to participate.
Notably, the effect of combined improvements substantially exceeded that of single-attribute adjustments. When both shorter session duration and individual voluntary enrollment were implemented together, the choice probability of weekly training approached that of the monthly option. Further optimization encompassing instructor composition, teaching format, assessment methods, and theoretical foundation elevated the predicted choice probability of weekly training to 66.75%, more than double the baseline rate. These results suggest that although time burden is a core barrier to participation, systematic multidimensional optimization can effectively mitigate physicians’ initial resistance to high-frequency training. Figure 3 presents the cumulative effects of various attribute combinations, offering actionable insights for phased and targeted enhancement of training program design.
Discussion
This study utilized a DCE to investigate PCPs’ preferences regarding training programs, with a particular focus on prescribing and deprescribing in the context of multimorbidity. Distinct from prior research, which often centers on general training needs or outcomes, this study emphasizes the structured design of implementation components by standardizing training content. This approach enables a more precise identification of the optimal configuration of training programs. Moreover, the study extends the application of DCE methodology to the field of medical education, an area where such approaches remain underutilized. The results underscore the multifaceted nature of PCPs’ preferences, which span key attributes such as instructor composition, participant enrollment, training duration and frequency, and the theoretical basis of the course.
When implementing training programs, PCP demonstrated a clear preference for sessions facilitated by a multidisciplinary team comprising general practitioners and clinical pharmacists, conducted individually rather than in groups, held on a monthly basis, limited to 45 min in duration, and grounded in clinical practice guidelines. Among the various training attributes evaluated, session frequency and duration emerged as the most influential factors shaping PCPs’ preferences. Notably, PCPs expressed a preference for less frequent and shorter training sessions which contrasts with initial expectations. The observed preference for less frequent and shorter training sessions aligns with the demanding clinical workloads faced by PCPs (38). Subgroup analyses stratified by the sample medians provided empirical support for this interpretation. Physicians with higher workload exhibited substantially stronger aversion to weekly training and 90-min sessions (see Supplementary Tables 5, 6). These findings indicate that time pressure intensifies the need for time-efficient formats (30, 39). Although more experienced physicians also showed stronger preference for monthly over weekly training, the difference between workload groups was more pronounced, and no consistent pattern emerged for session duration by experience. This suggests that current workload may be a more salient determinant of training format preferences than cumulative professional experience. However, this reluctance may be mitigated through targeted adjustments in training design. For instance, optimizing the composition of the instructional team, streamlining enrolment procedures, enhancing the relevance and practicality of training materials, and maintaining concise session durations could enhance the acceptability and feasibility of more frequent training sessions among PCPs.
The mode of involvement in training programs plays a critical role in influencing PCPs’ willingness to participate. As physicians are increasingly expected to attend multiple training initiatives, the cumulative time commitment can lead to training fatigue and reduced enthusiasm for participation (40). Moreover, the growing accessibility of medical knowledge through digital platforms has fostered a stronger preference for self-directed learning among PCPs (31), as it offers greater flexibility and autonomy in managing their professional development. This may account for the observed preference for individual participation over mandatory group-based or all-staff training formats, which are perceived as less adaptable to individual schedules and learning needs.
With regard to the composition of instructional staff, PCPs expressed a preference for training sessions delivered jointly by general practitioners and clinical pharmacists, a finding consistent with our initial expectations. Given the specialized nature of prescribing and deprescribing, the inclusion of pharmacists as co-instructors is perceived as particularly valuable, offering targeted expertise and clinical depth. This interdisciplinary approach not only enhances the comprehensiveness and quality of the training but also ensures that participants receive guidance grounded in real-world pharmacological practice (41). Moreover, exposure to role models from relevant professional backgrounds, particularly those who are both knowledgeable and engaging, has been shown to significantly enrich the educational experience. Such exposure supports the acquisition of advanced prescribing competencies and increases participant engagement and interest in the training content (42). Evidence also indicates that collaborative practice between pharmacists and physicians improves prescribing accuracy and promotes safer prescribing behaviors within the healthcare system (43, 44).
While the average preference for training location among respondents did not reach statistical significance, notable heterogeneity was observed, suggesting that only a subset of PCPs expressed strong preferences regarding training venue. Previous studies have reported comparable levels of participant engagement and knowledge retention between on-site and online training modalities (29, 45). Although online training offers clear advantages in terms of convenience and scheduling flexibility, on-site formats continue to provide unique benefits, particularly in promoting interpersonal interaction, collaboration among trainees, and real-time engagement with instructors (32, 46). Furthermore, disparities in digital literacy and comfort with technology, especially among older PCPs, can limit the accessibility and effectiveness of online training. As a result, despite growing acceptance of online learning, it is unlikely to serve as a full substitute for in-person training in the near term (14). Nonetheless, online formats can play a valuable supplementary role when their strengths are strategically leveraged—for instance, by providing recorded lectures, digital course materials, or follow-up modules that enhance and reinforce on-site learning experiences (45, 46).
Given the demanding clinical workloads and familial obligations commonly faced by PCPs, training programs must prioritize feasibility and voluntary participation. Our findings suggest that optional, self-directed enrollment may be more acceptable than compulsory formats, promoting greater engagement and sustained commitment. Moreover, the inclusion of a multidisciplinary teaching faculty, particularly the active involvement of clinical pharmacists, can enhance the depth and credibility of training content. This interdisciplinary approach is critical to ensuring both pedagogical rigor and practical relevance in clinical practice. To maximize engagement and accessibility, curriculum design should emphasize flexible scheduling. A hybrid model combining online and offline modalities appears particularly effective. Live sessions facilitate real-time interaction, while digital platforms provide access to recorded lectures and learning materials. This format accommodates PCPs’ time constraints, supports self-paced learning, expands geographical reach, reduces logistical barriers, and ultimately enhances participation and knowledge uptake.
Several key considerations are essential for the successful implementation of such training programs. First, modular and flexible learning formats should be prioritized. Structuring the curriculum into smaller, focused “mini-training” modules enables physicians to incorporate learning into their routine clinical practice, thereby mitigating time and regional limitations. These micro-courses, delivered via a blended learning platform, offer a pragmatic solution for continuous professional development. Second, the establishment of a multidisciplinary and diverse teaching team is critical. Involving experts from various fields (such as clinical pharmacology, geriatrics, and pharmacy) enriches the learning experience by providing multiple clinical perspectives, thereby enhancing both the academic rigor and real-world applicability of the content. Third, the adoption of demand-driven strategies and incentive mechanisms can significantly increase program uptake. Providing formal certification or continuing education credits serves as a motivational tool. Furthermore, ongoing feedback from participants and regular assessments of clinical demand can inform curriculum refinement and ensure sustained relevance. Lastly, robust assessment strategies are necessary to evaluate the effectiveness of the training. Periodic evaluations, such as quizzes, case-based discussions, simulated prescriptions, or prescription audits, can help assess learner competence, reinforce knowledge retention, and inform continuous curriculum improvement.
This study has several limitations. First, the geographic focus on eastern China may constrain the generalizability of the findings, and replication in other regions is needed to validate the results. Second, the DCE design did not include an opt-out option and implicitly assumed respondents’ willingness to participate in training, limiting the ability to assess actual training intent or identify barriers to engagement. Third, due to space limitations in the survey instrument, certain potentially relevant attributes and levels were excluded, which may have resulted in the omission of key factors influencing PCP preferences. Fourth, this study captures stated preferences rather than revealed preferences, and a gap may exist between hypothetical choices and actual behavior. Therefore, our findings provide theoretical guidance for training design but require future validation against real-world participation and prescribing outcomes. Future research should consider a more comprehensive range of implementation attributes and adopt longitudinal designs to assess the long-term impact of training on prescribing and deprescribing behaviors and patient outcomes.
Conclusion
This study elucidates PCPs’ preferences for training programs focused on prescribing and deprescribing in the context of multimorbidity. The results indicate that PCPs prefer training programs characterized by low frequency, short duration, individual involvement, instruction by a multidisciplinary team, and content grounded in clinical practice guidelines. These insights offer a theoretical foundation for the future design of training interventions, with the potential to enhance their feasibility, acceptability, and participation among PCPs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tian F Chen Z Wu J. Prevalence of polypharmacy and potentially inappropriate medications use in elderly Chinese patients: a systematic review and meta-analysis. Front Pharmacol. (2022) 13:862561. doi: 10.3389/fphar.2022.86256135795561 PMC 9251439 · doi ↗ · pubmed ↗
- 2Bodenheimer T Wagner EH Grumbach K. Improving primary care for patients with chronic illness. JAMA. (2002) 288:1775–9. doi: 10.1001/jama.288.14.177512365965 · doi ↗ · pubmed ↗
- 3Zhou X Han L Farmer A Yao M Xia Y Yan M . Challenges and barriers to physician decision-making for prescribing and deprescribing among patients with multimorbidity in eastern China’s primary care settings: a qualitative study. BMJ Open. (2025) 15:e 095063. doi: 10.1136/bmjopen-2024-095063 PMC 1180890039922587 · doi ↗ · pubmed ↗
- 4Marengoni A Angleman S Melis R Mangialasche F Karp A Garmen A . Aging with multimorbidity: a systematic review of the literature. Ageing Res Rev. (2011) 10:430–9. doi: 10.1016/j.arr.2011.03.00321402176 · doi ↗ · pubmed ↗
- 5Nie XY Dong XX Lu H Li DL Zhao CH Huang Y . Multimorbidity patterns and the risk of falls among older adults: a community-based study in China. BMC Geriatr. (2024) 24:660. doi: 10.1186/s 12877-024-05245-139112944 PMC 11304791 · doi ↗ · pubmed ↗
- 6Skou ST Mair FS Fortin M Guthrie B Nunes BP Miranda JJ . Multimorbidity. Nat Rev Dis Primers. (2022) 8:48. doi: 10.1038/s 41572-022-00376-435835758 PMC 7613517 · doi ↗ · pubmed ↗
- 7National Health Commission of the People’s Republic of China. Statistical bulletin on the development of health care in China (2023). Available online at: https://www.nhc.gov.cn/guihuaxxs/c 100133/202408/0c 53d 04ede 9e 4079 afff 912d 71b 5131 c.shtml (Accessed May 10, 2025).
- 8Pazan F Wehling M. Polypharmacy in older adults: a narrative review of definitions, epidemiology and consequences. Eur Geriatr Med. (2021) 12:443–52. doi: 10.1007/s 41999-021-00479-333694123 PMC 8149355 · doi ↗ · pubmed ↗