Maximal use of 0.05% topical isotretinoin in patients with congenital ichthyosis results in low systemic exposure
Holm Schneider, Christopher G. Bunick, Kathrin Hillmann, Thy N. Huynh, Steven Kempers, Nicolai Peschel, Ulrike Blume‐Peytavi, Joyce M. C. Teng, Alan M. Mendelsohn, John Stinson, Lara Wine Lee

TL;DR
A topical isotretinoin treatment for a rare skin condition shows minimal systemic absorption and is generally well tolerated.
Contribution
Demonstrates that maximal topical use of isotretinoin results in low systemic exposure in patients with congenital ichthyosis.
Findings
Systemic exposure levels were less than 1% of those from oral isotretinoin administration.
Most safety issues were mild and localized.
No systemic toxicity was observed despite maximal topical application.
Abstract
Congenital ichthyoses (CI) are rare, inherited skin disorders characterized by hyperkeratosis, scaling and fissuring that significantly impair patients' quality of life. Treatment options are limited, with systemic retinoids reserved for severe cases owing to their adverse effect profile. This open‐label, single‐arm, maximal‐use trial investigated the systemic exposure and safety of a topically administered isotretinoin ointment (TMB‐001 0.05%) in patients with moderate‐to‐severe CI. Thirty‐four patients aged ≥6 years applied TMB‐001 0.05% under maximal‐use conditions (twice daily to 75%–90% of the body surface area) for 14 days, with continued application for another 10 weeks. Exposure levels for TMB‐001 0.05% and its metabolites were < 1% of those observed after single oral administration of 80 mg isotretinoin to healthy adults. A majority of patients had local safety or tolerability…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
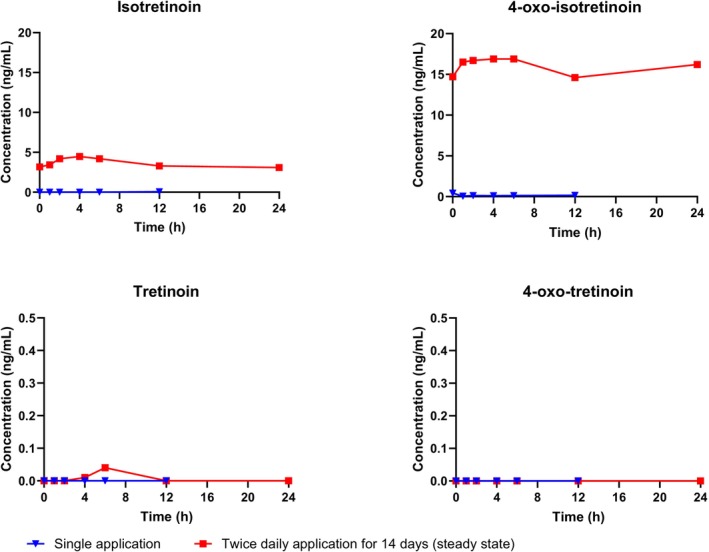 FIGURE 1
FIGURE 1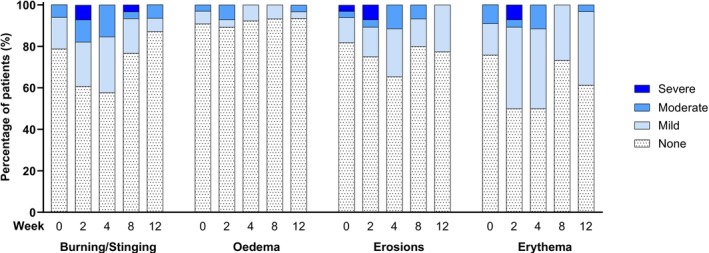 FIGURE 2
FIGURE 2| Compound | Age group | Mean AUC0–24 (h × ng/mL) | Mean Cmax (ng/mL) | Median Tmax (h) |
|---|---|---|---|---|
| Isotretinoin | Adults (≥17 years) | 78.44 | 4.13 | 1.50 |
| Adolescents (12–16 years) | 101.34 | 7.70 | 14.00 | |
| 4‐Oxo‐isotretinoin | Adults (≥17 years) | 352.95 | 16.70 | 5.00 |
| Adolescents (12–16 years) | 432.96 | 25.44 | 18.00 | |
| Tretinoin | Adults (≥17 years) | 0.17 | 0.04 | 0.00 |
| Adolescents (12–16 years) | 13.74 | 4.52 | 2.00 | |
| 4‐Oxo‐tretinoin | Adults (≥17 years) | 0.00 | 0.00 | 0.00 |
| Adolescents (12–16 years) | 10.15 | 3.60 | 1.00 |
- —Timber Pharmaceuticals
- —LEO Pharma A/S
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSkin and Cellular Biology Research · Genetic and rare skin diseases. · Cancer and Skin Lesions
INTRODUCTION
1
Congenital ichthyoses (CI) are a heterogeneous group of inherited skin disorders characterized by abnormal epidermal differentiation and skin barrier impairment. In autosomal recessive CI (ARCI; prevalence 1:100 000) and recessive X‐linked ichthyosis (RXLI; prevalence 1:3000 males), main features are widespread hyperkeratosis and scaling of the skin, typically accompanied by painful fissuring, pruritus and major impact on quality of life.1, 2 Management of CI is typically limited to the use of emollients, keratolytic agents and in severe cases systemic retinoids (vitamin A analogues).1, 3 Investigational use of systemic retinoids, such as oral isotretinoin, has shown efficacy in the treatment of CI but may be associated with significant adverse effects, including potential teratogenicity as well as skeletal, blood and hepatic toxicity.3, 4 Hence, any repeated administration of systemic retinoids requires careful monitoring.
A proprietary, topical, polyethylene glycol‐based isotretinoin ointment (TMB‐001 0.05%) has been formulated as a potentially effective and safer alternative to oral isotretinoin for the treatment of CI.5 TMB‐001 0.05% was investigated in the recent Phase 3 ASCEND trial (NCT05295732). Here, we report the systemic exposure to TMB‐001 0.05% and its metabolites during maximal use in a subset of ASCEND trial participants, thereby adding to the limited data published on the pharmacokinetics (PK) of topical isotretinoin, particularly in children and adolescents. Furthermore, we compare these data with exposure data obtained after single oral administration of 80 mg isotretinoin to healthy adults.
METHODS
2
Data were obtained from an open‐label, single‐arm, maximal‐use part of the Phase 3 multi‐centre trial ASCEND (hereafter referred to as ASCEND‐MUsT), investigating the PK of topically applied TMB‐001 0.05% in patients aged ≥ 6 years with moderate‐to‐severe, genetically confirmed RXLI or ARCI. Eligibility criteria are described online (https://clinicaltrials.gov/study/NCT05295732). For PK assessment, TMB‐001 0.05% was dosed for 14 days under conditions of maximal use, defined as twice‐daily application to 75%–90% of the body surface area (BSA). For safety and exploratory efficacy assessments, the application was continued for another 10 weeks. The approximate maximum daily dose of isotretinoin, based on twice‐daily application to 90% of the BSA, was estimated to be 0.034 g/day in an average adult male and 0.013 g/day in an average 6‐year‐old.
Additionally, data were obtained from an open‐label, single‐arm, single‐dose Phase 1 monocentric trial (protocol no. C1D02307/TMB01‐101) investigating the PK of orally administered isotretinoin (Claravis™, 2 × 40 mg capsules) in healthy adult males. Claravis™ is an FDA‐designated reference standard for the reference‐listed drug (Accutane®, unavailable in the US since 2009).
Both clinical trials were approved by an IRB/IEC at each centre and conducted in accordance with the Declaration of Helsinki principles and Good Clinical Practice guideline. All participants gave their written informed consent. Parents or legal guardians provided written informed assent for participants < 18 years of age.
PK analysis was based on intensive sampling from patients aged ≥12 years in ASCEND‐MUsT and from participants in the oral‐dose trial and sparse sampling from patients aged 6–11 years in ASCEND‐MUsT (Tables S1–S2). Plasma concentrations of isotretinoin, its interconvertible geometric isomer tretinoin and their main metabolites, 4‐oxo‐isotretinoin and 4‐oxo‐tretinoin, were detected using high‐performance liquid chromatography–tandem mass spectrometry. PK parameters were derived from plasma concentration–time course data using non‐compartmental analysis and the linear‐up/log‐down method. Plasma concentrations and derived PK parameters were summarized by age group using descriptive statistics, excluding concentrations that were missing or below the limit of quantification.
Safety and tolerability of TMB‐001 0.05% after topical application for 12 weeks in ASCEND‐MUsT were assessed based on reported adverse events (AEs) and local skin reactions (LSRs; burning/stinging, oedema, erosions, erythem, and suspected allergic contact dermatitis). Efficacy was evaluated using the Investigator's Global Assessment (IGA; Table S3).
The key ligand in this article is hyperlinked to the corresponding entry online (http://www.guidetopharmacology.org) and is permanently archived in the Concise Guide to PHARMACOLOGY 2023/24.6
RESULTS AND DISCUSSION
3
ASCEND‐MUsT enrolled 34 patients (52.9% males; 76.5% ARCI, 23.5% RXLI; age range: 4–64 years; mean age: 24.7 [±17.8] years; mean body mass index [BMI]: 24.47 [±8.70] kg/m^2^; Table S4). All were dosed with TMB‐001 0.05% and 31 patients completed the trial. 27 patients could be included in the PK analysis set (excluding patients with major protocol deviations related to drug administration): 13 adults (aged ≥17 years), 6 adolescents (aged 12–16 years) and 8 children aged 4–11 years. The oral‐dose trial enrolled 15 healthy males (age range: 25–54 years; mean age: 42.3 [±9.5] years; mean BMI: 26.35 [±2.31] kg/m^2^); all received isotretinoin orally.
In ASCEND‐MUsT, a total of 208 plasma samples were analysed (147 samples from adults, 34 from adolescents and 27 from children). Exposure levels for isotretinoin and its geometric isomer and metabolites after topical application of TMB‐001 0.05% were low (Figure 1 and Table 1). The highest steady‐state exposure was seen for 4‐oxo‐isotretinoin, consistent with this being the major metabolite of isotretinoin; the major metabolic pathway of isotretinoin appears to be its oxidation to 4‐oxo‐isotretinoin, catalysed primarily by cytochrome P450 (CYP) isoform 3A4, with further glucuronidation of 4‐oxo‐isotretinoin.7 In children aged 6–11 years, the highest mean plasma concentration during steady state was 2.82 ng/mL for isotretinoin and 9.53 ng/mL for 4‐oxo‐isotretinoin, that is, lower than the mean maximum plasma concentration (C_max_) in patients aged ≥12 years. Most PK parameters were not calculable in children, owing to their sparse blood sampling schedule.
Mean plasma concentration profiles for isotretinoin and its metabolites in adult patients with moderate‐to‐severe congenital ichthyosis after topical application of TMB‐001 0.05% under maximal‐use conditions. Plasma concentrations are plotted vs. nominal time and are baseline‐adjusted, that is, obtained by subtracting patient‐specific baseline values for each metabolite at pre‐dose from the concentration at each timepoint. Number of patients in analysis set: 13 adults; number of patients with calculable data: 10 adults.
In the oral‐dose trial, a total of 313 plasma samples were analysed. The mean C_max_ for isotretinoin was 1160 ng/mL and the mean area under the plasma concentration–time curve from 0–24 h post‐dose (AUC_0–24_) was 10 800 h × ng/mL. Hence, systemic exposure after multiple topical applications of TMB‐001 0.05% proved to be much lower than the exposure after a single oral dose of 80‐mg isotretinoin: mean C_max_ was 280‐fold lower in adults and 150‐fold lower in adolescents; mean AUC_0–24_ was 138‐fold lower in adults and 107‐fold lower in adolescents.
Eighty‐six AEs, all non‐serious, were reported for 24 (70.6%) of the patients dosed with TMB‐001 0.05% for up to 12 weeks in ASCEND‐MUsT. Seventy‐six AEs were mild or moderate and 10 were severe (8 administration site reactions, 2 pruritus events); 4 patients permanently discontinued treatment because of AEs, all considered probably treatment‐related by the investigator: 1 adult with severe pruritus, 1 adolescent with 3 events of mild or moderate administration site reactions, 1 adolescent with moderate application site pain and moderate skin irritation and 1 child with severe application site erythema and severe application site dermatitis along with mild chills and mild hidrosis. In addition, 5 patients had their treatment interrupted from 2 to 12 days because of AEs considered probably or possibly treatment‐related by the investigator: 1 adult with severe pruritus, 3 adults with administration site reactions of mild, moderate or unknown severity, and 1 adolescent with mild administration site reactions. There were no AEs consistent with systemic isotretinoin exposure. The most frequently reported AE type was administration site reactions (53 in 18 [52.9%] patients). LSRs occurred in the majority of patients, mainly as erythema (70.6% of patients), burning/stinging (55.9% of patients) and erosions (44.1% of patients); few patients had oedema (17.7%), and none had suspected allergic contact dermatitis. LSRs were reported most frequently at Week 2 and Week 4 and were usually mild (Figure 2).
Local skin reactions in patients with moderate‐to‐severe congenital ichthyosis after topical application of TMB‐001 0.05% under maximal‐use conditions. Number of patients in analysis set: 34; number of patients with available data: 33.
At Week 12, 55.9% of the patients in ASCEND‐MUsT had a ≥2‐point improvement from baseline on the 5‐point IGA scale (combined scaling and fissuring). The single‐arm design of ASCEND‐MUsT, however, precludes any conclusion on the efficacy of topical isotretinoin for treatment of CI.
In summary, topical application of the isotretinoin ointment formulation TMB‐001 0.05% for 14 days under maximal‐use conditions in patients with CI provided C_max_ and AUC_0–24_ values < 1% of those resulting from a single oral dose of 80 mg isotretinoin. The sample sizes of the trial populations and age groups contributing with data to the analysis were small. Nevertheless, these results from the final analysis of ASCEND‐MUsT add to the sparse data published to date on the PK of topical isotretinoin application. Although a majority of patients had local safety or tolerability issues, most of these were mild. Overall, treatment with TMB‐001 0.05% in this trial was well tolerated, with a safety profile similar to that observed in previous studies.5, 8 The results reported herein may inform the potential use or further investigation of isotretinoin formulations for topical treatment of various skin conditions.
AUTHOR CONTRIBUTIONS
Conceptualization: A.M.M., C.G.B., J.M.C.T.; Data curation: A.M.M., C.G.B., H.S., J.M.C.T., J.S.; Formal analysis: A.M.M., C.G.B., H.S., J.M.C.T., J.S., K.H., L.W.L., N.P., S.K., T.N.H., U.B.P.; Investigation: A.M.M., C.G.B., H.S., J.M.C.T., K.H., L.W.L., N.P., S.K., T.N.H., U.B.P.; Methodology: A.M.M., C.G.B., H.S., J.M.C.T.; Writing—review and editing: A.M.M., C.G.B., H.S., J.M.C.T., J.S., K.H., L.W.L., N.P., S.K., T.N.H., U.B.P.
CONFLICT OF INTEREST STATEMENT
H. S. has served as consultant for Krystal Biotech, Novartis, Roche and SRE GmbH; and as investigator and consultant for Edimer Pharmaceuticals, Pervormance International GmbH, Pierre Fabre and Wyeth Pharma GmbH. C. G. B. has served as investigator for AbbVie, Almirall, Apogee, Daiichi Sankyo, LEO Pharma, Ortho Dermatologics, Sun Pharma, Takeda, Timber and Palvella; and as consultant for AbbVie, Almirall, Amgen, Apogee, Arcutis, Botanix, Connect Biopharma, Dermavent, Eli Lilly, EPI Health/Novan, Incyte, LEO Pharma, Novartis, Ortho Dermatologics, Pfizer, Regeneron Pharmaceuticals, Sanofi, Sun Pharma, Takeda, Teladoc, Triveni and UCB. K. H. has served as investigator for AbbVie, Eli Lilly, Sanofi, Amryt Pharma, Bayer, Cassiopea, Concert Pharma (Sun Pharma), Novartis, Legacy Healthcare and LEO Pharma. U. B. P. has served as advisor, consultant, and speaker for AbbVie, Boots Healthcare, CeraVe, Eli Lilly, Galderma Laboratorium GmbH, Pfizer, Pierre Fabre, Regeneron Pharmaceuticals, Sanofi and Vichy; and as investigator for Amryt Pharma, Bayer, Cassiopea, Concert Pharma (Sun Pharma), Novartis, Legacy Healthcare and LEO Pharma. J. M. C. T. has served as consultant for Abeona Therapeutics, AFT Pharmaceuticals, Amryt Pharma, BridgeBio, Krystal Biotech, Menlo Therapeutics and Nobelpharma; and as investigator and consultant for Castle Creek Biosciences, LEO Pharma, Novartis, Palvella Therapeutics, Pfizer, Regeneron Pharmaceuticals and Timber Pharmaceuticals. A. M. M. was an employee of Timber Pharmaceuticals, a LEO Pharma company, at the time of this trial. J. S. is an employee of LEO Pharma. L. W. L. is an advisory board member for Castle Creek Biosciences, Chiesi, Eli Lilly, Pfizer, Verrica, Regeneron Pharmaceuticals Inc. and Twi Biotechnology; a consultant for AbbVie, Apogee, Chiesi, Kimberly‐Clark, Krystal Biotech, Eli Lilly and Novartis; an investigator with AbbVie, Amgen, Amryt Pharma, Arcutis Biotherapeutics, Apogee, Boehringer Ingelheim, Castle Creek Biosciences, Celgene, Eli Lilly, Galderma, Incyte, LEO Pharma, Mayne Pharma, Novartis, Pfizer, Regeneron Pharmaceuticals Inc., Sanofi, Target Pharma, Trevi Therapeutics, Twi Biotechnology and UCB; and a speaker for Sanofi, Chiesi and Krystal Biotech and participates on data safety monitoring boards for BMS. The remaining authors state no conflict of interest.
PRINCIPAL INVESTIGATOR STATEMENT
The authors confirm that the PI for this paper is Holm Schneider, MD, and that he had direct clinical responsibility for patients.
TRIAL REGISTRATION
ClinicalTrials.gov: NCT05295732.
Supporting information
Table S1. Blood sampling schedule in patients with moderate‐to‐severe congenital ichthyosis (ASCEND trial). Table S2. Blood sampling schedule in healthy males (TMB01–101 trial). Table S3. Investigator's Global Assessment 5‐point scale. Table S4. Patient demographics (ASCEND trial).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vahlquist A , Torma H . Ichthyosis: a road model for skin research. Acta Derm Venereol. 2020;100(7):adv 00097. doi:10.2340/00015555-3433 32147743 PMC 9128938 · doi ↗ · pubmed ↗
- 2Gutierrez‐Cerrajero C , Sprecher E , Paller AS , et al. Ichthyosis. Nat Rev Dis Primers. 2023;9(1):2. doi:10.1038/s 41572-022-00412-3 36658199 · doi ↗ · pubmed ↗
- 3Mazereeuw‐Hautier J , Paller AS , Dreyfus I , et al. Management of congenital ichthyoses: guidelines of care: part one: 2024 update. Br J Dermatol. 2025;193(1):16‐27. doi:10.1093/bjd/ljaf 076 40156154 · doi ↗ · pubmed ↗
- 4Digiovanna JJ , Mauro T , Milstone LM , Schmuth M , Toro JR . Systemic retinoids in the management of ichthyoses and related skin types. Dermatol Ther. 2013;26(1):26‐38. doi:10.1111/j.1529-8019.2012.01527.x 23384018 PMC 3884695 · doi ↗ · pubmed ↗
- 5Teng JMC , Bunick CG , Guenthner S , et al. The CONTROL study: a randomized, double‐blind vehicle‐controlled phase 2b study of novel topical isotretinoin formulation demonstrates improvement in recessive X‐linked and autosomal recessive lamellar congenital ichthyosis. J Am Acad Dermatol. 2022;87(6):1455‐1458. doi:10.1016/j.jaad.2022.07.028 35872261 · doi ↗ · pubmed ↗
- 6Alexander SPH , Kelly E , Mathie AA , et al. The concise guide to PHARMACOLOGY 2023/24: introduction and other protein targets. Br J Pharmacol. 2023;180(S 2):S 1‐S 22.38123153 10.1111/bph.16176 · doi ↗ · pubmed ↗
- 7Sonawane P , Cho HE , Tagde A , et al. Metabolic characteristics of 13‐cis‐retinoic acid (isotretinoin) and anti‐tumour activity of the 13‐cis‐retinoic acid metabolite 4‐oxo‐13‐cis‐retinoic acid in neuroblastoma. Br J Pharmacol. 2014;171(23):5330‐5344. doi:10.1111/bph.12846 25039756 PMC 4294043 · doi ↗ · pubmed ↗
- 8Paller AS , Browning J , Parish LC , Bunick CG , Rome Z , Bhatia N . Safety, tolerability, and efficacy of a novel topical isotretinoin formulation for the treatment of X‐linked or lamellar congenital ichthyosis: results from a phase 2a proof‐of‐concept study. J Am Acad Dermatol. 2022;87(5):1189‐1191. doi:10.1016/j.jaad.2022.02.060 35271936 · doi ↗ · pubmed ↗