Association of left ventricular mass with discordant stress cardiac magnetic resonance and coronary angiography
Kanyaw Kader, Laust Dupont Rasmussen, Salma Raghad Karim, Jelmer Westra, Christin Isaksen, Jacob Hartmann Søby, Jonathan Nørtoft Dahl, Lau Brix, Steffen E Petersen, Theodore Murphy, Simon Winther, Evald Høj Christiansen, Morten Böttcher, Ashkan Eftekhari

TL;DR
This study shows that higher left ventricular mass can cause mismatch between stress CMR and coronary angiography results in patients with suspected heart disease.
Contribution
The study identifies left ventricular mass as a potential confounder in the agreement between stress CMR and ICA in coronary artery disease.
Findings
Higher left ventricular mass was associated with abnormal stress CMR results.
Discordant stress CMR and ICA results were linked to increased microvascular resistance and left ventricular mass.
Left ventricular mass did not differ significantly between patients with or without obstructive CAD.
Abstract
This study aimed to determine the impact of left ventricular mass (LVM) on discordant stress cardiac magnetic resonance (CMR) imaging and invasive coronary angiography (ICA) in patients with suspected coronary artery disease (CAD) at coronary computed tomography angiography (CCTA). In this substudy of the Dan-NICAD 2 trial (NCT03481712), 354 patients with suspected obstructive CAD on CCTA were examined with both rest and stress CMR and ICA for invasive physiological measurements. An abnormal stress CMR was defined as ≥2 contiguous segments with a stress perfusion defect, late gadolinium enhancement, or wall motion abnormality. CMR-derived LVM was sex-adjusted by conversion from grams to per cent. Haemodynamically obstructive CAD at ICA was defined as visual diameter stenosis >90% or FFR ≤0.80. LVM was higher in patients with an abnormal stress CMR compared to those with a normal CMR…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
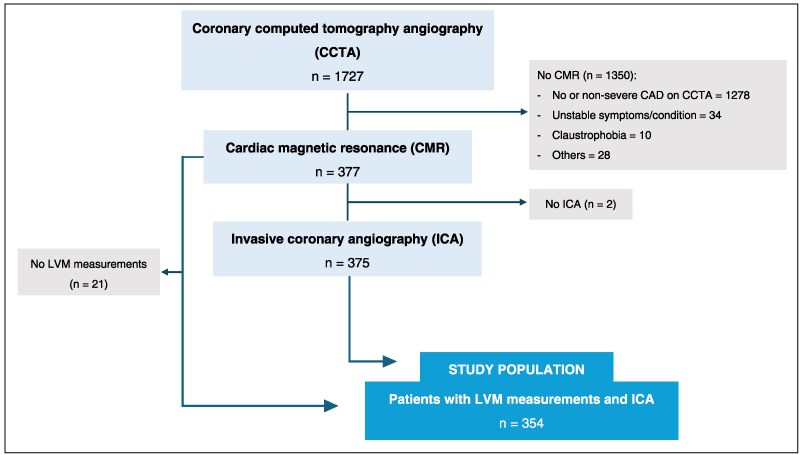 Figure 1
Figure 1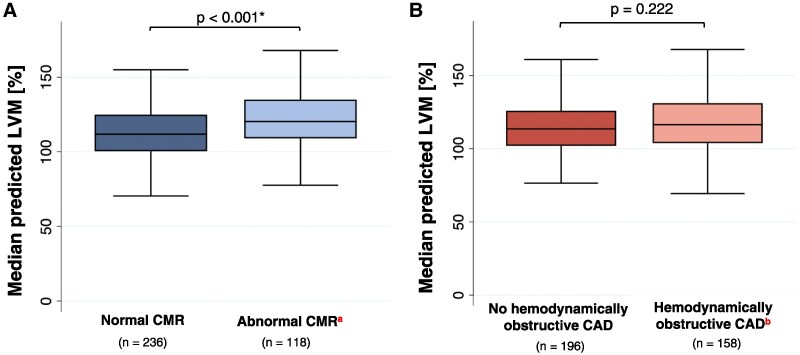 Figure 2
Figure 2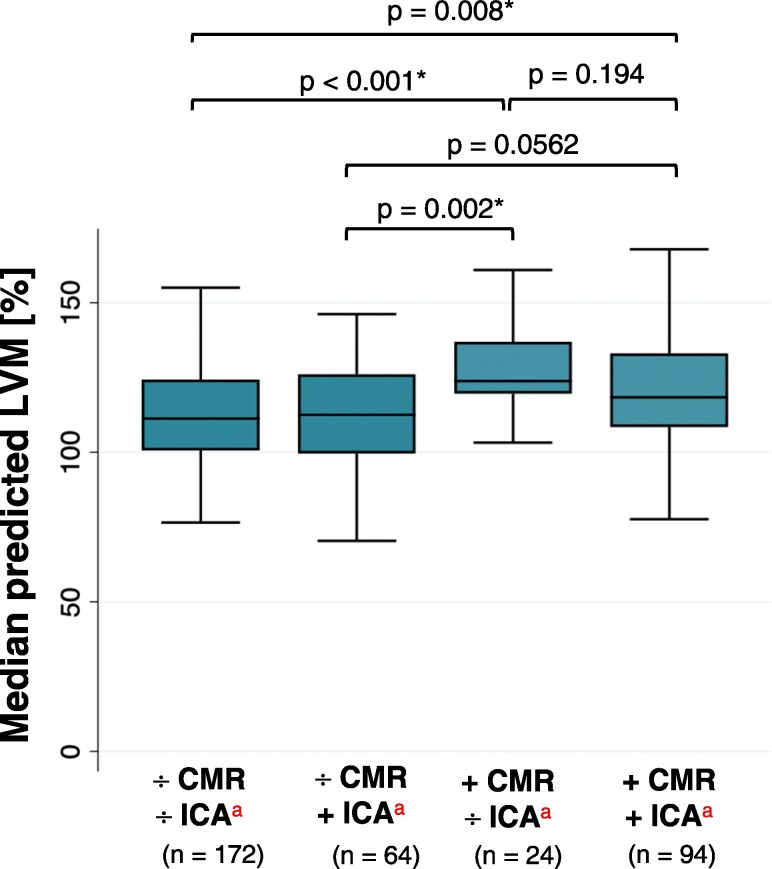 Figure 3
Figure 3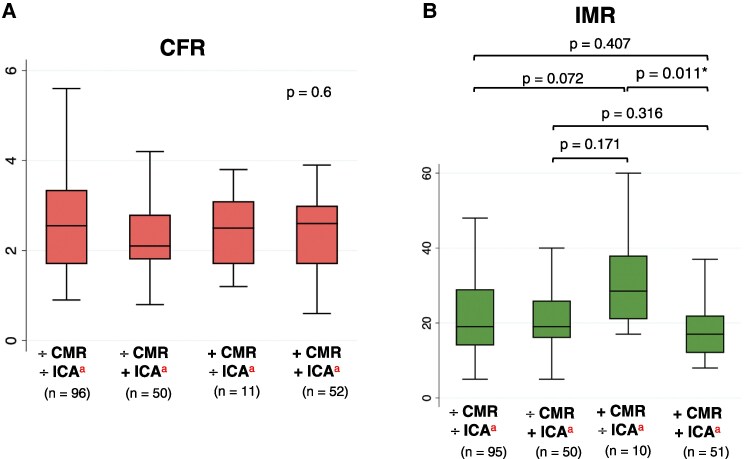 Figure 4
Figure 4| Study population ( | |
|---|---|
| Sex | |
| Male | 251 (71) |
| Age [years] | 64 (58–70) |
| Risk factors | |
| Hypertension | 180 (51) |
| Diabetes mellitus | 34 (9.6) |
| Active smoking | 118 (33) |
| Family history of CAD | 133 (38) |
| BMI | 27 (25–29) |
| Symptoms | |
| Typical angina | 102 (29) |
| Atypical angina | 127 (36) |
| Non-specific chest pain | 82 (23) |
| Others e.g. dyspnoea or arrhythmia | 43 (12) |
| Invasive haemodynamic parameters in coronary lesions with DS 30–90% | |
| FFR ( | 0.83 (0.75–0.89) |
| CFR ( | 2.3 (1.7–3.1) |
| IMR ( | 19 (14–28) |
| Univariate analysis | Multivariate analysis | |||
|---|---|---|---|---|
| OR (95% CI) |
| OR (95% CI) |
| |
| Age | 0.991 (0.964–0.1.020) | 0.557 | 0.994 (0.937–1.055) | 0.855 |
| Male | 3.127 (1.772–5.518) | <0.001 | 1.394 (0.424–4.580) | 0.585 |
| Hypertension | 1.290 (0.828–2.011) | 0.260 | 1.099 (0.428–2.821) | 0.844 |
| Diabetes | 1.268 (0.611–2.630) | 0.524 | 2.024 (0.580–7.063) | 0.269 |
| BMI | 1.066 (1.007–1.128) | 0.028 | 1.129 (0.990–1.1288) | 0.070 |
| Active smoking | 0.709 (0.427–1.175) | 0.182 | 0.302 (0.887–1.025) | 0.055 |
| Median predicted LVM | 1.123 (1.062–1.202) | <0.001 | 1.159 (1.013–1.326) | 0.032 |
| FFR ≤ 0.80 | 5.266 (2.286–12.131) | <0.001 | 4.542 (1.691–12.198) | 0.003 |
| CFR < 2.5 | 0.734 (0.347–1.551) | 0.418 | 0.606 (0.237–1.544) | 0.294 |
| IMR > 25 | 0.838 (0.359–1.955) | 0.683 | 1.223 (0.409–0.3.661) | 0.719 |
| Univariate analysis | Multivariate analysis | |||
|---|---|---|---|---|
| OR (95% CI) |
| OR (95% CI) |
| |
| Age | 0.988 (0.961–1.015) | 0.381 | 0.967 (0.921–1.015) | 0.176 |
| Male | 2.596 (1.552–4.343) | < 0.001 | 2.454 (1.023–5.886) | 0.044 |
| Hypertension | 1.171 (0.764–1.795) | 0.470 | 0.727 (0.344–1.536) | 0.404 |
| Diabetes | 2.111 (1.034–4.310) | 0.040 | 10.152 (2.581–39.930) | 0.001 |
| BMI | 0.999 (0.946–1.055) | 0.975 | 1.048 (0.949–1.158) | 0.355 |
| Active smoking | 1.192 (0.739–1.922) | 0.471 | 1.035 (0.455–2.356) | 0.934 |
| Median predicted LVM | 1.045 (0.987–1.106) | 0.134 | 1.065 (0.960–1.181) | 0.236 |
| CFR < 2.5 | 1.482 (0.789–2.783) | 0.221 | 2.279 (1.081–4.807) | 0.030 |
| IMR > 25 | 0.502 (0.241–1.048) | 0.067 | 0.456 (0.0.195–1.065) | 0.070 |
| − CMR | + CMR |
| |||
|---|---|---|---|---|---|
| − ICA | + ICA | − ICA | + ICA | ||
|
| |||||
|
| 172 | 64 | 24 | 94 | |
| Age [years] | 65 (59–70) | 65 (57–70) | 63 (59–69) | 63 (58–69) | 0.869 |
| Male | 103 (60) | 48 (75) | 19 (79) | 81 (86) | <0.001 |
| Age >65 years | 82 (48) | 31 (48) | 9 (38) | 42 (45) | 0.779 |
| Hypertension | 84 (49) | 31 (48) | 15 (63) | 50 (53) | 0.587 |
| Diabetes | 7 (4) | 14 (22) | 3 (13) | 10 (11) | 0.001 |
| BMI | 26 (24–29) | 27 (25–29) | 28 (26–34) | 28 (25–29) | 0.097 |
| Active smoking | 60 (35) | 25 (39) | 5 (21) | 28 (30) | 0.785 |
| Family history of CAD | 69 (40) | 21 (33) | 8 (33) | 35 (38) | 0.717 |
| Median predicted LVM | 111 (101–124) | 113 (100–126) | 124 (120–137) | 118 (108–133) | <0.001 |
|
| |||||
|
| 98 | 44 | 10 | 31 | |
| FFR ( | 0.88 (0.84–0.92) | 0.73 (0.68–0.77) | 0.86 (0.85–0.93) | 0.73 (0.70–0.77) | <0.001 |
| CFR ( | 2.6 (1.7–3.4) | 2.1 (1.8–2.8) | 2.5 (1.7–3.1) | 2.6 (1.7–3.0) | 0.601 |
| IMR ( | 19 (14–29) | 19 (16–26) | 29 (21–38) | 17 (12–22) | 0.034 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Imaging and Diagnostics · Advanced MRI Techniques and Applications · Coronary Interventions and Diagnostics
Introduction
Coronary computed tomography angiography (CCTA) is recommended as the first-line non-invasive anatomical imaging in patients with low-intermediate pre-test likelihood of coronary artery disease (CAD) to rule out obstructive lesions.^1,2^ However, CCTA overestimates CAD severity, and one-in-two patients do not undergo revascularization after an invasive angiography with a preceding CCTA.^3^
Therefore, in patients with new-onset chest pain and clinically suspected obstructive CAD, guidelines recommend downstream non-invasive imaging before referral to invasive angiography to avoid unnecessary invasive coronary angiographies (ICA) and to verify inducible ischaemia following a CCTA-suspected stenosis.^1,2^ One method for this follow-up investigation is cardiac magnetic resonance (CMR) imaging, which has shown high diagnostic accuracy for obstructive CAD in cohorts with high-risk patients and high disease prevalence.^4^ However, guidelines recommend revascularization based on fractional flow reserve (FFR) ≤ 0.80.^5^ Furthermore, the ability of CMR to identify invasively assessed CAD is limited in patients with a preceding CCTA and a moderate pre-test likelihood of obstructive CAD.^6,7^
Previously, it has been proposed that increased left ventricular mass (LVM) is associated with myocardial ischaemia because of a decrease in coronary lumen volume to myocardial mass ratio, which, additionally, has been related to impaired invasive measures of FFR ≤0.80.^8^ However, the impact of LVM on discordant CMR and ICA findings regarding haemodynamically obstructive lesions has not been thoroughly addressed.
This study aimed to determine the impact of LVM on discordant stress CMR and ICA findings in patients with suspected CAD.
Methods
Study design and population
This was a substudy of the Danish study of Non-Invasive testing in Coronary Artery Disease (Dan-NICAD) 2 trial (NCT03481712). A thorough study protocol, including inclusion and exclusion criteria, has previously been published.^9^ In brief, this cross-sectional, multicentre study included 1734 patients with low to intermediate pre-test likelihood of obstructive CAD but without history of CAD. All patients underwent CCTA, and if CCTA suspected obstructive stenoses (diameter stenosis ≥50%), patients were further referred to myocardial perfusion imaging including 3.0T CMR, and subsequent ICA including measures of FFR (Figure 1). The ICA operator was blinded to the results of the myocardial perfusion imaging (MPI) modalities.
Flowchart of study design. CAD, coronary artery disease; LVM, left ventricular mass.
This study assessed the impact of LVM on discordant stress CMR and ICA findings of haemodynamical impairment using logistic regression analyses. Patients were stratified by CMR and ICA abnormality by pre-specified thresholds. Analyses included distributive LVM means across arbitrary groups of CMR findings and other invasive physiological measures, i.e. the coronary flow reserve (CFR) and the index of microvascular reserve (IMR). The primary analyses of the association of LVM with discordant CMR and ICA findings were conducted on a per-patient level.
Imaging
Coronary computed tomography angiography
CCTA images were obtained using a 320 multi-slice volume computed tomography (CT) scanner (Aquilion One, Toshiba Medical Systems, Japan, and Siemens Flash, Siemens Healthcare, Germany) with prospective electrocardiogram triggering. All images were analysed onsite by experienced cardiologists in a dedicated workstation (Vitrea Advanced Workstation, Vital Images, MN, USA, or Syngo.Via, Siemens Healthcare, Erlangen, Germany). Suspected obstructive CAD was defined as segments with ≥50% diameter stenosis using the 18-segment model of the coronary tree.
CMR imaging
CMR scans were performed using a 3.0T MRI system (Siemens Skyra, Software release E11A, Siemens Healthcare GmbH, Germany) using the Body 18 and Spine 32 receive coils. Stress perfusion was performed upon intravenous adenosine infusion 140 µg/kg/min, followed by a rest perfusion examination after washout of the stress agent. Myocardial blood flow was assessed using injection of a gadolinium contrast agent (Gadovist®, Bayer Schering Pharma AG, Germany) during stress and rest, after which a late gadolinium enhancement (LGE) protocol was performed to assess cardiac viability. Abnormalities in ventricular wall motion were visually assessed from 1 to 5 (1 = normal, 2 = mild hypokinesia, 3 = severe hypokinesia, 4 = akinesia, and 5 = dyskinesia).
Analyses of CMR scans were conducted in an independent core laboratory (William Harvey Research Institute, Queen Mary University of London, London, UK), blinded to patient characteristics and results of previous examinations. An abnormal CMR was pre-defined as ≥ 2 contiguous segments with either a significant perfusion defect (either subendocardial or transmural signal changes), LGE, and/or wall motion abnormalities. For both LGE and wall motion assessment, the threshold for abnormality was solely based on ischaemic changes, ruling out inclusion of patients with non-ischaemic patterns.^7^
Left ventricular myocardial mass was assessed using a short-axis balanced steady-state free precession cine sequence. The endocardial and epicardial borders of the left ventricle in both end-diastolic and end-systolic phases were automatically segmented using CVI42 (Release 5.16, Circle Cardiovascular Imaging Inc., Calgary, Canada) software and could be manually corrected. The volumes were automatically calculated for end-diastolic volume and end-systolic volume phases. The myocardial mass was calculated using the formula:
where mmyo is myocardial mass, Vepi and Vendo are epicardial and endocardial volumes, respectively, and ρtissue is the tissue density in g/cm^3^.
LVM was then sex-adjusted to allow comparison across sex by converting LVM from grams to per cent as suggested in The Multi-Ethnic Study of Atherosclerosis (MESA) trial^10^ (see Supplementary data online, Equation S1). In the trial, left ventricular hypertrophy (LVH) was defined as LVM greater than the 95th percentile (equivalent to >136%).
Invasive coronary angiography
Prior to ICA, 250 μg of intracoronary nitroglycerine and 5000 IU heparin were administered. All lesions with a diameter stenosis of 30–90% by visual assessment and a reference diameter of >2 mm were considered for physiological assessment in the main Dan-NICAD 2 study. The pressure-wire (PressureWire × Guidewire, Abbott, Chicago, IL) and CoroFlow (Coroventis Research AB, Uppsala, Sweden) systems were used according to manufacturer instructions.
Hyperaemia was induced using intravenous adenosine (140 µg/kg/min). Functional measurements of FFR were obtained during maximum hyperaemia when distal pressure (Pd)/aortic pressure (Pa) were stable. Routine checks were made to ensure that drift did not occur after the recordings, and an absolute drift value of ≤±0.02 was accepted. CFR and IMR were measured with three bolus injections of 3 mL saline to obtain hyperaemic thermodilution curves for mean transit time calculation during rest and maximum hyperaemia. CFR was calculated as the average hyperaemic mean transit time/resting mean transit time. IMR was calculated as hyperaemic transit time × Pd_(hyperaemia)_.
Three-dimensional quantitative coronary angiography (QCA) was performed with two angiograms with 15 frames/s without panning, no foreshortening, and at least 25° apart.
All physiological core laboratory analyses were performed blinded to the baseline characteristics and non-invasive imaging examinations. Invasive physiology traces were evaluated in an offline core laboratory (Institute of Clinical Medicine, Aarhus University, Denmark).
Haemodynamically obstructive CAD was pre-defined as a high-grade stenosis (diameter stenosis >90%) by visual assessment or FFR ≤0.80 in a vessel with a diameter stenosis of 30–90% or QCA based diameter stenosis (≥50% diameter) if FFR was indicated but not performed. For the analyses of the association between LVM, CFR, and IMR, cut-off values of CFR <2.5 and IMR >25 were defined as abnormal.^11^
Statistical analysis
Categorical variables were expressed as numbers and percentages and were compared using χ^2^ test or Fisher’s exact test if the assumptions of a χ^2^ test were violated. Continuous variables were expressed with means and standard deviations, or median and interquartile range (IQR) if data did not follow normal distribution by Shapiro–Wilk test. Medians were compared using Mann–Whitney U test.
Univariate logistic regressions assessed the association between LVM and the probability of an abnormal CMR or heamodynamically obstructive CAD at ICA. This was followed by multivariate analyses to determine the impact of pre-defined risk factors of CAD on the regression model, namely age, sex, smoking, body mass index (BMI), hypertension, diabetes, FFR, CFR, and IMR. Results were presented with odds ratios (OR) and a 95% confidence interval (CI). For LVM, OR were presented per 5% increase in LVM. In both uni- and multivariate analyses, FFR, CFR, and IMR were converted to categorical variables based on pre-defined thresholds. This was done to only include physiological measurements in coronary lesions with a visual diameter stenosis 30–90%.
Patients were classified into four binary concordant or discordant groups according to CMR abnormality and the presence of haemodynamically obstructive CAD at ICA, respectively. In concordant outcomes, the result of CMR and ICA were both either normal or abnormal, whereas discordant outcomes warranted incongruent findings at CMR and ICA. A Kruskal–Wallis H test was performed to assess overall difference within the binary groups, and if significant, a post hoc Dunn’s test with Bonferroni correction was done.
For all analyses, a two-sided P-value <0.05 was considered statistically significant. Statistical analyses were conducted in Stata/MP 17.0 (StataCorp, College Station, TX, USA).
Results
Study characteristics
In total, 375 patients underwent both stress CMR imaging and ICA, of whom LVM measurements were assessed in 354 (94%) patients. Most patients were male (71%), and median age was 64 (58–70) years (Table 1). Hypertension was the predominant cardiovascular risk factor and was present in 180 (51%) patients.
The impact of LVM and invasive measures on CMR
Of the 354 patients, 118 (33%) had an abnormal CMR. With some overlap, 94/118 (80%) had stress perfusion defects, 19/118 (16%) had LGE, and 32/118 (27%) had stress-induced wall motion abnormalities. Median predicted LVM was higher in patients with an abnormal CMR compared to patients with a normal CMR [median predicted LVM = 120% (IQR: 109–135) vs. median predicted LVM = 112% (IQR: 100–125), respectively, P < 0.001] (Figure 2A). A total of 49/354 (14%) patients had LVH according to the above definition of >136%, of which 26 (53%) had an abnormal myocardial perfusion on CMR.
*Median predicted LVM stratified by CMR and ICA. Boxplots displaying median (IQR) predicted LVM [%] stratified by A) stress CMR result and B) haemodynamically obstructive CAD. Difference in median LVM calculated by Mann–Whitney U test. Significant P-values marked with . a Panel A: Defined as a significant perfusion defect in ≥2 contiguous segments and/or LGE in ≥2 contiguous segments and/or wall motion abnormalities in ≥2 contiguous segments. b Panel B: Defined as a visual diameter stenosis >90% or FFR ≤0.80 in lesions with 30–90% diameter stenosis during ICA. LVM = left ventricular mass; CMR, cardiac magnetic resonance; CAD, coronary artery disease.
In both uni- and multivariate analyses, higher median predicted LVM was associated with an increased likelihood of an abnormal CMR; OR = 1.123, 95% CI: 1.062–1.202 (P < 0.001) and OR = 1.159, 95% CI: 1.013–1.326 (P = 0.032), respectively (Table 2). An FFR ≤0.80 in coronary lesions with a diameter stenosis of 30–90% was also associated with an abnormal CMR in both univariate (OR = 5.266, 95% CI: 2.286–12.131, P < 0.001) and multivariate analysis (OR = 4.542, 95% CI: 1.691–12.198, P = 0.003).
The impact of LVM and invasive measures on haemodynamically obstructive CAD
Haemodynamically obstructive CAD at ICA was found in 158/354 (45%) patients; 81/159 (51%) were based on a high-grade stenosis, 61/158 (39%) on FFR ≤0.80, and 16/158 (10%) on QCA ≥50% diameter stenosis.
Median predicted LVM was similar in patients with and without haemodynamically obstructive CAD [116% (IQR: 104–131) vs. 114% (IQR: 102–126), respectively, P = 0.222] (Figure 2B). In multivariate analyses, patients of male sex (OR = 2.454, 95% CI: 1.023–5.886, P = 0.044), with diabetes (OR = 10–152, 95% CI: 2.581–39.930, P = 0.001), and CFR <2.5 in coronary lesions with 30–90% diameter stenosis (OR = 2.279, 95% CI: 1.081–4.807, P = 0.030) were associated with haemodynamically obstructive CAD (Table 3).
LVM and invasive haemodynamic parameters based on CMR and ICA
Patient and haemodynamic characteristics across four binary groups based on CMR abnormality and the presence of haemodynamically obstructive CAD are displayed in Table 4. In total, 172/354 (49%) patients had concordant normal CMR and no haemodynamically obstructive CAD, 94/354 (27%) patients had concordant abnormal CMR and haemodynamically obstructive CAD, 64/354 (18%) patients had discordant normal CMR and haemodynamically obstructive CAD, and 24/354 (6.8%) patients had discordant abnormal CMR and no haemodynamically obstructive CAD (Table 4a).
Patients with discordant abnormal CMR and no haemodynamically obstructive CAD [median predicted LVM = 124% (IQR: 120–137)], and patients with concordant abnormal CMR and haemodynamically obstructive CAD [median predicted LVM = 118% (IQR: 108–133)] had the highest predicted LVM (Table 4A), with no difference between the two groups (P = 0.194) (Figure 3). The greatest difference in LVM was found between the former group and patients with concordant normal CMR and no haemodynamically obstructive CAD (median LVM difference = 13%, P = 0.001). Patients with an abnormal CMR and haemodynamically obstructive CAD had higher LVM than patients with normal CMR and no haemodynamically obstructive CAD (median LVM difference = 7.0%, P = 0.008) (Figure 3).
*Sex-adjusted median predicted LVM stratified by CMR and ICA. Median (IQR) predicted LVM [%] within binary groups stratified by CMR abnormality and presence of haemodynamically obstructive CAD. Difference between groups was calculated by Dunn’s test. Significant P-values marked with . aThe plus symbol (+) represents an abnormal outcome of CMR and/or ICA. The minus symbol (−) represents a normal outcome of CMR and/or ICA. LVM, left ventricular mass; CMR, cardiac magnetic resonance; ICA, invasive coronary angiography.
Across groups, CFR was only below the pre-defined abnormality threshold in patients with discordant normal CMR and haemodynamically obstructive CAD [median CFR = 2.1 (IQR: 1.8–2.8)], and no difference in median CFR levels was found between the groups (Kruskal–Wallis H test = 0.601) (Table 4B) (Figure 4A). IMR was highest in patients with discordant abnormal CMR and no haemodynamically obstructive CAD [median IMR = 29 (IQR: 21–38)] and was higher compared to patients with concordant abnormal CMR and haemodynamically obstructive CAD (median IMR difference = 12, P = 0.011) (Figure 4B).
*Box plots of CFR and IMR stratified by CMR and ICA. Boxplots displaying median (IQR) A) CFR and B) IMR in coronary lesions with DS 30–90% within binary groups stratified by CMR abnormality and by presence of haemodynamically obstructive CAD. Difference between groups was calculated using Dunn’s test. Significant P-values marked with . P-values for intergroup for CFR are not calculated because the Kruskal–Wallis H test was non-significant (P = 0.6). aThe plus symbol (+) represents an abnormal outcome of CMR and/or ICA. The minus symbol (−) represents a normal outcome of CMR and/or ICA. CFR, coronary flow reserve; IMR, index of microvascular resistance; CMR, cardiac magnetic resonance; ICA, invasive coronary angiography.
Discussion
This multicentre study aimed to assess the impact of LVM on discordant findings between CMR imaging and invasive coronary angiography (ICA) in patients with suspected stenosis on CCTA. Regardless of the presence of haemodynamically obstructive CAD, sex-adjusted LVM was higher in patients with abnormal CMR results. Patients with abnormal CMR findings but no haemodynamically obstructive disease on ICA had both elevated LVM and increased IMR. These findings suggest that CMR results may be falsely positive due to LVH, or that ICA with fractional flow reserve (FFR) may yield false negatives due to high IMR. Therefore, assessment of LVM may be an important factor to consider when evaluating patients with new-onset chest pain and clinically suspected obstructive CAD using both CMR and FFR.
The clinical application of CMR
The performance of CMR to assess CAD has been extensively investigated. Several studies report high sensitivities and specificities in cohorts with high-risk patients and high disease prevalence using haemodynamically obstructive CAD as a reference standard.^12–16^ However, in patients with moderate stenoses yielding positive FFR values, rather low sensitivities have been demonstrated.^6,7,17^ This is in alignment with our findings, where concordant abnormal CMR and ICA findings are present in 94/354 (27%) patients. Compared to previous studies, besides inclusion of patients with known CAD,^13–15^ yielding higher disease burdens^12,18,19^ and dissimilar definitions of CMR abnormality,^16^ reasons for the rather high rate of discordant CMR and ICA results could be partly attributable to LVM, which was higher in patients with discordant abnormal stress CMR and no haemodynamically obstructive CAD (Table 4a).
Determinants of increased LVM and its diagnostic yield
A longitudinal evaluation of LVM in the Framingham cohort revealed that an abnormal left ventricular (LV) geometry and LVH are associated with an increased risk of cardiovascular events.^20^ The most significant risk factors influencing LVM are systemic blood pressure, male sex, age, and BMI. Patients in the two groups with the highest LVM i.e. patients with an abnormal CMR with and without haemodynamically obstructive CAD, were overweight, male patients with a high prevalence of hypertension (Table 4a). This was also consistent with the LVM index (LVMI) being increased but below the hypertrophic threshold when compared to patients with a normal CMR. A linear regression between LVM and BMI indicated that increasing BMI reduced LVM (see Supplementary data online, Figure S1). However, in a large cohort study, obesity (BMI ≥30 kg/m^2^) was associated with increased LVM.^21^ The inconsistent results can be explained by patients in this study being overweight (median BMI = 27 kg/m^2^), and not obese. Within the two groups, LVM was highest in patients with discordant abnormal CMR and no haemodynamically obstructive CAD. This could further suggest that increased LVM detected on CMR may contribute as an independent indicator of myocardial ischaemia regardless of epicardial dysfunction at ICA, which warrants further investigation (Table 4a).
The impact of LVM on microvascular function
In this study, patients with the highest LVM, namely those with discordant abnormal CMR and no haemodynamically obstructive CAD, presented with elevated IMR and normal FFR. This is consistent with coronary blood flow increasing proportionally with LVM, but the relative flow to mass ratio decreases.^22^ Given the inverse relationship between flow and resistance according to Ohm’s law of resistance, increased LVM leads to increased microvascular resistance relative to LVM, and accordingly, the pressure gradient across an epicardial stenosis decreases, resulting in a higher FFR.^23^ Myocardial remodelling following LVM enlargement is known to predispose to isolated coronary microvascular disease, a known cause of myocardial infarction with non-obstructive coronary arteries (MINOCA).^24^ While the clinical presentation of MINOCA can be indistinguishable from obstructive myocardial infarction, invasive angiographic findings include non-obstructive CAD and increased IMR. Thus, microvascular dysfunction, with or without epicardial stenosis, could cause a scenario of combined normal FFR, elevated IMR, and low coronary blood flow. This may explain patients presenting with discordant normal FFR and abnormal CMR in this study.
Conversely, the opposite scenario entails impaired FFR and normal CMR, indicating high coronary blood flow and low microvascular resistance. As expected, patients with concordant normal CMR and ICA findings had preserved FFR and low IMR, suggesting no significant CAD. Patients with impaired FFR also presented with lower IMR. A common feature was lower LVM compared with those having discordant abnormal CMR but normal ICA. This corresponds to the coherent relationship between epicardial and microvascular physiology, where a decrease in epicardial pressure reduces the microvascular perfusion.
In both scenarios, CMR would appear either less sensitive or specific for obstructive CAD if FFR is used as gold standard. This could be due to dissimilar definitions of obstructive CAD by CMR and FFR, and their diagnostic yield. Moreover, CMR primarily provides measures of anatomy, volume, and perfusion on a myocardial level to detect ischaemia, while FFR is used to assess the functional severity of coronary lesions and, consequently, to guide revascularization.^1^ Thus, patients may have myocardial perfusion defects without obstructive CAD. For this reason, suspected obstructive CAD detected on CMR may contribute as a second-line non-invasive tool to not only refer selective patients to ICA with FFR measurements but also to consider MINOCA.
Limitations
This study has some limitations. First, primarily low-intermediate-risk patients were included, which may have affected the prevalence and detection rate of CAD by CMR compared to an all-comer population. Therefore, the external validity of the findings is limited by the inclusion of only new onset stable chest pain patients with suspected obstructive disease on CCTA.
Visual assessment of diameter stenosis on ICA may influence the internal consistency, resulting in operator-specific outcomes. Invasive physiological measurements during ICA were assessed in coronary lesions with a visual diameter stenosis of 30–90%. If diameter stenoses were under- or overestimated by visual assessment (<30% or >90%), more vessels would be non-suitable for physiological measures. The guideline from the European Society of Cardiology recommends invasive functional testing during ICA in vessels with a diameter stenosis of 40–90%. This means that FFR in this study was potentially assessed in vessels with non-significant lesions, resulting in a low sensitivity of ICA with visual assessment and FFR as reference.
LVM was not estimated according to vessel-specific territories, and patients were not stratified by the number of diseased vessels. This constitutes a discrepancy in the use of a global vs. a vessel-specific LVM, with assessment of LVM based on ischaemic vessel territories being more specific.
Conclusion
In patients with stable chest pain and suspected obstructive CAD on CCTA, increased LVM can potentially confound concordance between stress CMR and ICA. This is due to increased microvascular resistance, which decreases the pressure gradient across an epicardial stenosis, resulting in an apparent high FFR and thus classified as a normal ICA.
Supplementary Material
jeaf350_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vrints C, Andreotti F, Koskinas KC, Rossello X, Adamo M, Ainslie J et al 2024 ESC guidelines for the management of chronic coronary syndromes: developed by the task force for the management of chronic coronary syndromes of the European Society of Cardiology (ESC) endorsed by the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2024;45:3415–537.39210710
- 2Gulati M, Levy PD, Mukherjee D, Amsterdam E, Bhatt DL, Birtcher KK et al 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021;144:e 368–454.10.1161/CIR.000000000000102934709879 · doi ↗ · pubmed ↗
- 3Nissen L, Winther S, Schmidt M, Rønnow Sand NP, Urbonaviciene G, Zelechowski MW et al Implementation of coronary computed tomography angiography as nationally recommended first-line test in patients with suspected chronic coronary syndrome: impact on the use of invasive coronary angiography and revascularization. Eur Heart J Cardiovasc Imaging 2020;21:1353–62.32888290 10.1093/ehjci/jeaa 197 · doi ↗ · pubmed ↗
- 4Knuuti J, Ballo H, Juarez-Orozco LE, Saraste A, Kolh P, Rutjes AWS et al The performance of non-invasive tests to rule-in and rule-out significant coronary artery stenosis in patients with stable angina: a meta-analysis focused on post-test disease probability. Eur Heart J 2018;39:3322–30.29850808 10.1093/eurheartj/ehy 267 · doi ↗ · pubmed ↗
- 5Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U et al 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J 2019;40:87–165.30165437 10.1093/eurheartj/ehy 394 · doi ↗ · pubmed ↗
- 6Nissen L, Winther S, Westra J, Ejlersen JA, Isaksen C, Rossi A et al Diagnosing coronary artery disease after a positive coronary computed tomography angiography: the Dan-NICAD open label, parallel, head to head, randomized controlled diagnostic accuracy trial of cardiovascular magnetic resonance and myocardial perfusion scintigraphy. Eur Heart J Cardiovasc Imaging 2018;19:369–77.29447342 10.1093/ehjci/jex 342 · doi ↗ · pubmed ↗
- 7Rasmussen LD, Winther S, Eftekhari A, Karim SR, Westra J, Isaksen C et al Second-line myocardial perfusion imaging to detect obstructive stenosis: head-to-head comparison of CMR and PET. JACC Cardiovasc Imaging 2023;16:642–55.36881421 10.1016/j.jcmg.2022.11.015 · doi ↗ · pubmed ↗
- 8van Diemen PA, Schumacher SP, Bom MJ, Driessen RS, Everaars H, Stuijfzand WJ et al The association of coronary lumen volume to left ventricle mass ratio with myocardial blood flow and fractional flow reserve. J Cardiovasc Comput Tomogr 2019;13:179–87.31302027 10.1016/j.jcct.2019.06.016 · doi ↗ · pubmed ↗