Adverse drug reactions among children with tuberculosis in China: a multicentre study, 2017–2022
Yiqing Zhou, Yu Kan, Ping Liu, Hongmei Xu, Juan Ma, Haiyan Li, Xin Yu, Qingshan Cai, Man Tian, Qing Fang, Xianhui Zeng, Guangxu Yang, Tao Yang, Fei Wang, Bin Chen, Leonardo Martinez

TL;DR
This study examines how often children in China experience harmful side effects from tuberculosis medications and finds that severe disease and certain drug combinations increase the risk.
Contribution
The study identifies risk factors for adverse drug reactions in Chinese children with tuberculosis, focusing on treatment regimens and disease severity.
Findings
19% of 482 children experienced adverse drug reactions during anti-TB treatment.
Blood system damage and gastrointestinal reactions were the most common ADRs.
Children with severe TB or those on HRZ(E)+second-line drugs had higher odds of ADRs.
Abstract
Although tuberculosis (TB) treatment, if adequately taken and adhered to, is highly effective. To investigate the occurrence, frequency and related factors of adverse drug reactions (ADRs) during anti-TB treatment in children in China. We conducted a multicentre study and collected data from 11 representative paediatric specialists and general hospitals offering anti-TB treatment. The outcome of interest was the occurrence of any ADRs. Multivariable logistic regression was performed to explore factors associated with ADRs and to identify groups at high-risk for ADRs. In total, 482 patients were enrolled; of whom, 94 (19%) reported an ADR. The most common ADRs were blood system damage (24%) and gastrointestinal reactions (24%). Most ADRs occurred within the intensive treatment period and were of short duration. Children with severe TB or those treated with HRZ(E) + second-line drugs in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
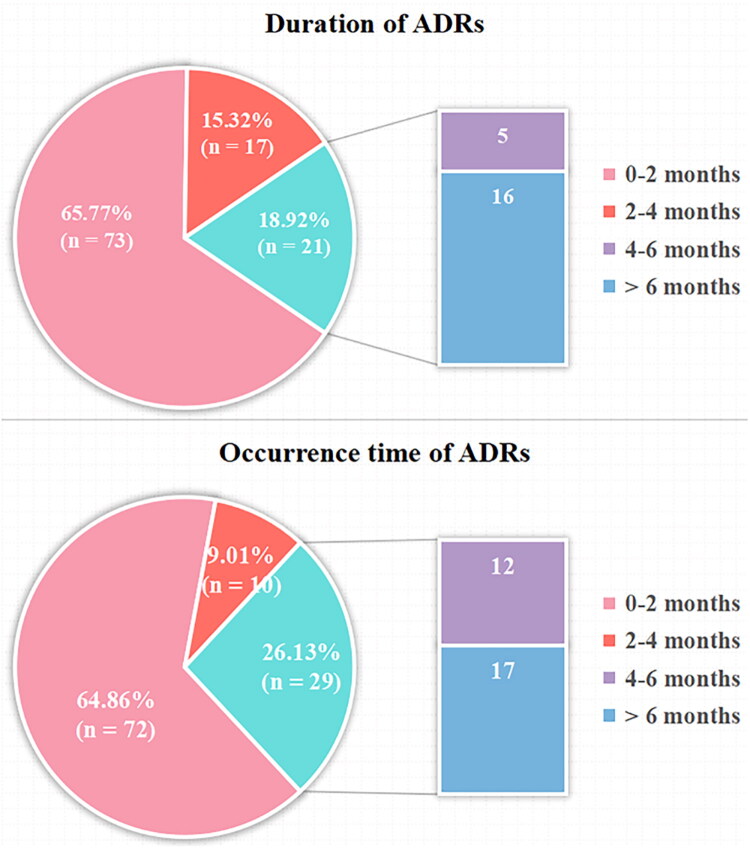 Figure 1
Figure 1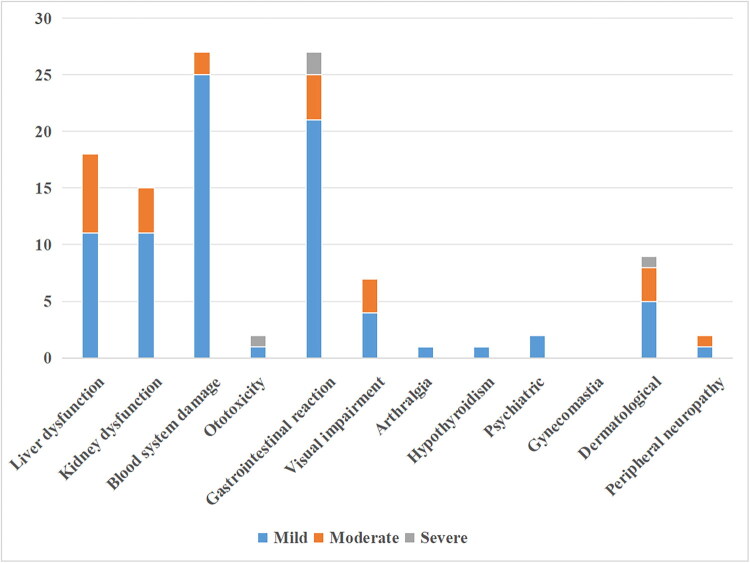 Figure 2
Figure 2| Variables | Total ( | No ADR ( | ADR ( |
|
|---|---|---|---|---|
| Sex | 0.919 | |||
| Male | 259 (53.73) | 210 (81.08) | 49 (18.92) | |
| Female | 223 (46.27) | 180 (80.72) | 43 (19.28) | |
| Age | 0.941 | |||
| 0–4 years old | 189 (39.21) | 152 (80.42) | 37 (19.58) | |
| 5–9 years old | 171 (35.48) | 138 (80.70) | 33 (19.30) | |
| 10–14 years old | 122 (25.31) | 100 (81.97) | 22 (18.03) | |
| Malnutrition | 0.983 | |||
| No | 409 (84.85) | 331 (80.93) | 78 (19.07) | |
| Yes | 73 (15.15) | 59 (80.82) | 14 (19.18) | |
| Site | 0.865 | |||
| PTB | 454 (94.19) | 367 (80.84) | 87 (19.16) | |
| EPTB | 28 (5.81) | 23 (82.14) | 5 (17.86) | |
| Disease severity |
| |||
| Non-severe | 175 (36.31) | 158 (90.29) | 17 (9.71) | |
| Severe | 307 (63.69) | 232 (75.57) | 75 (24.43) | |
| Isoniazid | 0.251 | |||
| Non-high dose | 459 (95.23) | 374 (81.48) | 85 (18.52) | |
| High dose | 23 (4.77) | 16 (69.57) | 7 (30.43) | |
| Rifampicin | 0.631 | |||
| Non-high dose | 472 (97.93) | 383 (81.14) | 89 (18.86) | |
| High dose | 10 (2.07) | 7 (70.00) | 3 (30.00) | |
| Pyrazinamide | 1.000 | |||
| Non-high dose | 464 (96.27) | 375 (80.82) | 89 (19.18) | |
| High dose | 18 (3.73) | 15 (83.33) | 3 (16.67) | |
| Treatment |
| |||
| HRZ (E) | 423 (87.76) | 358 (84.63) | 65 (15.37) | |
| HRZ (E) + second-line drug (s) | 59 (12.24) | 32 (54.24) | 27 (45.76) | |
| Combination medication |
| |||
| No | 395 (81.95) | 329 (83.29) | 66 (16.71) | |
| Yes | 87 (18.05) | 61 (70.11) | 26 (29.89) |
| Age groups | 0–4 years old ( | 5–9 years old ( | 10–14 years old ( | |||
|---|---|---|---|---|---|---|
| Crude odds ratio | Crude odds ratio | Crude odds ratio | ||||
| Sex | ||||||
| Male | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||
| Female | 0.99 (0.47–2.07) | 0.971 | 1.00 (0.47–2.13) | 0.995 | 1.18 (0.46–3.02) | 0.727 |
| Malnutrition | ||||||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||
| Yes | 1.98 (0.75–5.24) | 0.167 | 0.21 (0.03–1.62) | 0.134 | 1.13 (0.40–3.19) | 0.825 |
| Site | ||||||
| PTB | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||
| EPTB | 1.25 (0.33–4.80) | 0.742 | 1.21 (0.24–6.10) | 0.820 | 0.00 (0.00–Inf) | 0.992 |
| Disease severity | ||||||
| Non-severe | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||
| Severe | 4.07 (1.61–10.33) |
| 2.86 (1.16–7.03) |
| 2.02 (0.63–6.47) | 0.236 |
| Isoniazid | ||||||
| Non-high dose | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||
| High dose | 6.02 (1.29–28.19) |
| 0.40 (0.05–3.24) | 0.391 | 3.23 (0.51–20.62) | 0.214 |
| Rifampicin | ||||||
| Non-high dose | 1.00 (reference) | 1.00 (reference) | – | |||
| High dose | 6.62 (1.06–41.15) |
| 0.00 (0.00–Inf) | 0.989 | – | – |
| Pyrazinamide | ||||||
| Non-high dose | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||
| High dose | 0.82 (0.09–7.21) | 0.855 | 1.21 (0.24–6.10) | 0.820 | 0.00 (0.00–Inf) | 0.991 |
| Treatment | ||||||
| HRZ (E) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||
| HRZ (E) + second-line drugs | 4.38 (1.84–10.47) |
| 7.07 (2.52–19.79) |
| 2.97 (0.89–9.97) | 0.077 |
| Combination medication | ||||||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | |||
| Yes | 3.70 (1.74–7.87) |
| 0.98 (0.31–3.14) | 0.975 | 1.49 (0.43–5.09) | 0.527 |
| Types of ADR | Number of ADR | % patients with ADR | % total ADR | Time of occurrence | Duration of adverse event |
|---|---|---|---|---|---|
| ATDILI | 18 | 3.7 | 16.2 | 0.70 (0.23, 1.23) | 1.50 (0.90, 2.30) |
| Kidney dysfunction | 15 | 3.1 | 13.5 | 3.40 (0.20, 5.90) | 3.10 (1.20, 8.20) |
| Blood system damage | 27 | 5.6 | 24.3 | 2.95 (1.00, 5.20) | 1.70 (0.50, 5.80) |
| Ototoxicity | 2 | 0.4 | 1.8 | – | – |
| Gastrointestinal reaction | 27 | 5.6 | 24.3 | 2.00 (0.98, 3.28) | 1.00 (0.58, 2.75) |
| Visual impairment | 7 | 1.5 | 6.3 | 1.00 (1.00, 4.00) | 1.00 (1.00, 3.10) |
| Arthralgia | 1 | 0.2 | 0.9 | – | – |
| Hypothyroidism | 1 | 0.2 | 0.9 | – | – |
| Psychiatric | 2 | 0.4 | 1.8 | – | – |
| Gynecomastia | 0 | 0.0 | 0.0 | – | – |
| Dermatological | 9 | 1.9 | 8.1 | 1.00 (0.10, 1.00) | 0.20 (0.20, 1.00) |
| Peripheral neuropathy | 2 | 0.4 | 1.8 | – | – |
| Total | 111 | 23.0 | 100 | 1.30 (0.50, 4.68) | 1.35 (0.60, 3.93) |
| Variables | Crude odds ratio | Adjusted odds ratio | ||
|---|---|---|---|---|
| Sex | ||||
| Male | 1.00 (reference) | 1.00 (reference) | ||
| Female | 1.02 (0.65–1.61) | 0.919 | 1.05 (0.65–1.71) | 0.838 |
| Age | ||||
| 0–4 years old | 1.00 (reference) | 1.00 (reference) | ||
| 5–9 years old | 0.98 (0.58–1.66) | 0.947 | 1.12 (0.64–1.97) | 0.688 |
| 10–14 years old | 0.90 (0.50–1.62) | 0.735 | 0.97 (0.51–1.83) | 0.917 |
| Malnutrition | ||||
| No | 1.00 (reference) | 1.00 (reference) | ||
| Yes | 1.01 (0.53–1.90) | 0.983 | 0.77 (0.38–1.54) | 0.455 |
| Site | ||||
| PTB | 1.00 (reference) | 1.00 (reference) | ||
| EPTB | 0.92 (0.34–2.48) | 0.865 | 0.61 (0.21–1.84) | 0.383 |
| Disease severity | ||||
| Non-severe | 1.00 (reference) | 1.00 (reference) | ||
| Severe | 3.00 (1.71–5.28) |
| 2.44 (1.36–4.39) |
|
| Isoniazid | ||||
| Non-high dose | 1.00 (reference) | 1.00 (reference) | ||
| High dose | 1.93 (0.77–4.82) | 0.162 | 1.31 (0.45–3.88) | 0.621 |
| Rifampicin | ||||
| Non-high dose | 1.00 (reference) | 1.00 (reference) | ||
| High dose | 1.84 (0.47–7.27) | 0.382 | 1.35 (0.27–6.83) | 0.717 |
| Pyrazinamide | ||||
| Non-high dose | 1.00 (reference) | 1.00 (reference) | ||
| High dose | 0.84 (0.24–2.97) | 0.790 | 0.74 (0.19–2.90) | 0.669 |
| Treatment | ||||
| HRZ (E) | 1.00 (reference) | 1.00 (reference) | ||
| HRZ (E) + second-line drug (s) | 4.65 (2.61–8.27) |
| 3.70 (2.01–6.81) |
|
| Combination medication | ||||
| No | 1.00 (reference) | 1.00 (reference) | ||
| Yes | 2.12 (1.25–3.61) |
| 1.60 (0.89–2.89) | 0.118 |
- —‘Leading Goose’ R&D Program of Zhejiang
- —Zhejiang Provincial Traditional Chinese Medicine Science and Technology Project
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPharmacovigilance and Adverse Drug Reactions · Pharmaceutical studies and practices · Tuberculosis Research and Epidemiology
Introduction
Paediatric tuberculosis (TB) is amongst the top 10 health-related causes of death globally [1]. Despite highly effective preventive treatments, the age-specific risk of TB after Mycobacterium tuberculosis infection is highest in young children (<5 years of age); mortality is common after developing TB in this age group [2–6]. In 2023, there were an estimated 1.3 million new cases in children aged 0–14 years [7]. Among the 30 countries with high TB burden, China ranks third in the estimated number of TB cases (∼740,000), of which children aged 0–14 account for approximately 5% of total cases [7].
For children diagnosed with TB, anti-TB treatment typically involves the use of isoniazid, rifampin, pyrazinamide and ethambutol during an intensive phase, followed by isoniazid and rifampin during a consolidation phase. Characteristics of anti-TB treatment include the use of a wide variety of drugs and long duration of medication; due to this, adverse drug reactions (ADRs) can occur. Common ADRs include TB-specific drug induced liver injury, renal function damage and gastrointestinal reactions, etc. These ADRs, at the slight level, bring about physical and psychological sufferings to patients. In serious circumstances, they may directly influence the patients’ compliance with and effectiveness of the treatment, resulting in treatment interruption. Furthermore, it is possible to increase the risks of recurrence and drug resistance, exerting a tremendous influence on the economic burden of the patients’ families [8–10]. For instance, gastrointestinal reactions can cause patients to experience nausea, vomiting, abdominal pain, bloating, loss of appetite and other conditions, which affect the patients’ nutritional intake and are not conducive to the recovery from the disease. Mild drug induced liver injury is manifested as a transient increase in transaminase levels, while severe cases can lead to liver failure and even threaten the patient’s life. Some patients are forced to discontinue anti-TB treatment as a result, which affects the overall treatment outcome [11]. In addition, because children are in a special stage of growth and development, their drug absorption, metabolism and elimination characteristics are different from adults, and ADR is also different from adults [12,13]. Therefore, more attention should be paid to the frequency and severity of ADR in children with TB, and timely intervention should be carried out for patients.
Although several studies have reported adverse drug events in adults treated with TB, few studies have thoroughly investigated adverse drug events in children on treatment. We aimed to explore the frequency and timing of these events in children diagnosed with TB in a multicentre study conducted throughout China.
Methods
Study design, setting and population
This was a multicentre study including paediatric TB cases from 11 representative paediatric TB hospitals throughout China (Northeast, East, South, Southwest and Northwest regions), including Shanghai, Jiangsu, Zhejiang, Hainan, Chongqing, Qinghai and Jilin. Children with TB (<15 years of age) treated at 11 hospitals between 2017 and 2022 and weighing up to 40 kg were included in the study. We additionally excluded neonates aged 1 month and under and weighing <4 kg at the time of admission. Children with TB were treated with at least three drugs, isoniazid, rifampin and pyrazinamide, at doses determined according to pre-treatment weight. This was followed by treatment with at least two drugs, H and R, during the continuation period.
Data collection
We reviewed health records and collected data from several data systems including the Hospital Information System (HIS), the Laboratory Information System (LIS), Picture Archiving and Communication Systems (PACS), among others. Variables that were collected included sex, age, malnutrition, site, severity of TB, treatment dose (including those from isoniazid, rifampin and pyrazinamide), treatment therapy in the intensive phase, and combination medication. Data on ADRs including the type of ADR, occurrence time, duration and severity. ADRs were retrospectively collected from the hospital management system (HIS, LIS) across participating centres, with systematic extraction of data tailored to different ADR types: (1) clinical symptoms (e.g. nausea, vomiting, gastrointestinal discomfort, skin allergies, arthralgia and numbness) were extracted from physicians’ progress notes and medical records; (2) laboratory-confirmed ADRs (e.g. liver/renal function impairment, haematological abnormalities) were documented via review of full-course laboratory test results (e.g. liver enzymes, renal function panels and blood counts); and (3) specialized ADRs were verified through relevant diagnostic records (e.g. hearing tests, psychiatric assessment scales).
Definition
We divided drugs into high-dose and non-high-dose groups according to daily dose per kilogram and daily maximum dose. The high-dose group was defined as at least one of the daily doses per kilogram (kg) or daily maximum dose exceeding the upper limit. The non-high-dose group was defined as daily dose per kg and daily maximum dose not exceeding the upper limit. In particular, the dosing details of H, R and Z were as follows: H had a daily dose of 10 (7–15) mg/kg, with a maximum daily dose of 300 mg for individuals weighing <50 kg and a conventional administration frequency of once daily; R was administered at 15 (10–20) mg/kg daily, with a maximum dose of 600 mg for those weighing <50 kg, with a once-daily regimen; Z had a daily dose of 35 (30–40) mg/kg, with no specified daily maximum dose for individuals weighing <50 kg, and a standard administration frequency of once daily. Severe TB was defined as TB except for the following: peripheral lymph node; intrathoracic lymph node TB, no airway obstruction; uncomplicated TB pleural effusion or oligotrophic nonvacua’s disease, confined to the lung lobes, without miliary changes [14]. And the age group classification in this study was also based on the WHO Consolidated Guidelines on Tuberculosis (Module 5: Management of Tuberculosis in Children and Adolescents, 2022): (1) young child: aged 0–4 years; (2) older child: aged 5–9 years; (3) young adolescent: aged 10–14 years [14].
The occurrence of ADRs of all anti-TB drugs in this study was recorded in accordance with the relevant contents of China’s Adverse Drug Reaction Report and Monitoring and Management Measures [15]. The types of ADRs observed included liver dysfunction, kidney dysfunction, blood system damage, ototoxicity, gastrointestinal reaction, visual impairment, arthralgia, hypothyroidism, psychiatric, gynecomastia, dermatological and peripheral neuropathy.
The criteria for judging the severity of ADRs during the application of anti-TB drugs were according to the Anti-tuberculosis Drug Adverse Reaction Treatment Manual, which was divided into mild, moderate and severe criteria according to the relevant criteria [16]. Mild: After the occurrence of ADRs, the symptoms were mild without serious damage to the body. The discomfort symptoms of the patients did not show any progress in the process of continuous medication, and there was no need to receive targeted treatment. Moderate: After the occurrence of ADRs, the patient had obvious damage to the body, and the important organs or systems of the patient were damaged by the drug, resulting in the change of the patient’s treatment plan; Severe: the patient had obvious body injury during the medication, and the patient’s life safety was threatened, resulting in the discontinuation of the patient’s treatment plan.
Statistical analysis
Sociodemographic and clinical characteristics of the study population were summarized by frequency and proportion. The outcome of interest was the occurrence of any ADRs, while sex, age, malnutrition, site, severity of TB, dosage (including H, R and Z) and treatment therapy in the intensive phase, and combination medication were identified as potential risk factors. Odds ratios (ORs) were calculated to measure the association between risk factors and ADRs. Univariate and multivariate logistic regression were used for statistical analysis. All statistical tests were double-tailed and 95% confidence intervals were used to assess statistical significance. Statistical analysis was performed using R 4.4.1 statistical software (R Foundation for Statistical Computing, Vienna, Austria).
Ethics approval and consent to participate
This study has been approved by the Ethics Committee of Zhejiang Provincial Center for Disease Control and Prevention (approval number: 2023-018-01). Since this study only collected medical record information and did not involve relevant personal information of patients, it will not cause risks or adverse effects on the rights and health of subjects, and an application for informed consent exemption has been submitted (Ethics Committee of Zhejiang Center for Disease Control and Prevention).
Results
Of the 482 patients we included, 94 cases experienced ADR. The majority were male (n = 259, 54%) and the proportion of children aged 0–4 years old was 39% (n = 189). A small number of patients had extrapulmonary TB (n = 28, 6%). Sixty-four percent (n = 307) were severe. The duration of intensive treatment was 3.20 (IQR: 2.00–6.00) months and the duration of continuation treatment was 8.00 (IQR: 5.48, 10.50) months. A small number of patients were treated with high doses of isoniazid (5%, n = 23), rifampicin (2%, n = 10) and pyrazinamide (4%, n = 18). During intensive therapy, isoniazid exceeded the daily dose per kg or daily maximum dose in 23 cases, and the median dose was 16.67 (15.75–17.73) mg/kg in 16 cases exceeding 15 mg/kg. There were seven patients with a daily maximum dose of more than 300 mg, and the dosage was between 350 and 450 mg. Rifampicin exceeded the upper limit of daily dose per kg in 10 cases, and the median dose was 21.96 (21.43–27.06) mg/kg. Eighteen patients exceeded the upper limit of the daily dose per kg, and the median dose was 47.48 (42.86–50.00) mg/kg. Some (12%, n = 59) patients were treated with second-line drugs. The second-line drugs mainly used in the present study were linezolid and levofloxacin. A small number of children also received combination medication such as antibiotics, mainly including meropenem, azithromycin and cephalosporins (18%, n = 87). There were statistically significant differences between the two groups in the severity of TB, treatment options and combination medication (χ^2^ = 15.63, p < 0.001 for severity of TB; χ^2^ = 30.98, p < 0.001 for treatment options; χ^2^ = 8.01, p = 0.005 for combination medication) (Table 1). When stratified by age, children aged 0–4 and 5–9 years with severe TB had a significantly higher incidence of ADRs than those with non-severe TB (p = 0.002 and p = 0.019, respectively). Use of HRZ(E) + second-line drugs was also associated with a higher incidence of ADR in both age groups (both p < 0.001). Among 0–4-year-olds, high-dose H and use of combination medications were significantly associated with ADRs (p = 0.039 and p < 0.001, respectively; Table S1).
Among children aged 0–4 years, those with severe TB were more likely to develop ADRs (OR = 4.07, 95% CI: 1.61–10.33, p = 0.003). High-dose isoniazid (OR = 6.02, 95% CI: 1.29–28.19, p = 0.023), high-dose rifampicin (OR = 6.62, 95% CI: 1.06–41.15, p = 0.043), combination medication (OR = 3.70, 95% CI: 1.74–7.87, p < 0.001) and the HRZ (E) + second-line drug(s) regimen (OR = 4.38, 95% CI: 1.84–10.47, p < 0.001) were all significantly associated with the risk of adverse reactions in this age group. In the 5–9 years old group, the ‘Severe’ severity of TB (OR = 2.86, 95% CI: 1.16–7.03, p = 0.022) was significantly associated with adverse reactions; and the HRZ (E) + second-line drug(s) regimen (OR = 7.07, 95% CI: 2.52–19.79, p < 0.001) was an important factor for the increased risk of adverse reactions in this group. In the 10–14-year-old group, after univariate logistic regression analysis of each variable, the p values corresponding to the crude ORs were all >0.05. Moreover, since the rifampicin dose was not high for all children aged 10–14, rifampicin was not included in the univariate analysis (Table 2).
The most common ADRs were blood system damage and gastrointestinal reaction (Table 3), accounting for 24% of all ADRs, respectively, which could be observed in 6% of patients. Followed by anti-TB drug-induced liver injury (ATDILI) (4%), kidney dysfunction (3%) and dermatological (2%). ATDILI often appeared at 0.70 (IQR: 0.23–1.23) months of anti-TB treatment and lasted for 1.50 (IQR: 0.90–2.30) months; kidney dysfunction often appeared at 3.40 (IQR: 0.20–5.90) months and lasted for 3.10 (IQR: 1.20–8.20) months; blood system damage appeared at 2.95 (IQR: 1.00–5.20) months and lasted for 1.70 (IQR: 0.50–5.80) months; gastrointestinal reaction lasted for 1.00 (IQR: 0.58–2.75) months at 2.00 (IQR: 0.98–3.28) months; visual impact appeared at 1.00 (IQR: 1.00–4.00) months and lasted for 1.00 (IQR: 1.00–3.10) months; dermatological appeared at 1.00 (IQR: 0.10–1.00) months and lasted for 0.20 (IQR: 0.20–1.00).
Among patients included in the analysis, 79 (16%) and 10 (2%) participants experienced one or two ADRs, respectively. One patient (<1%) experienced three, four and five ADRs each, respectively.
The median time and IQR of various ADRs were during the intensive period (Table 3, Figure 1); most (66%) of the ADRs were short-term (≤2 months) (Figure 1). Some (14%) of the ADRs were long-term (>6 months) and the details were as follows: there was one case of ATDILI (9 months), four cases of kidney dysfunction (8.2, 8.7, 11.1 and 12.3 months), five cases of blood system damage (11.0, 11.3, 12.3, 13.8 and 14.1 months), one case of gastrointestinal reaction (11.4 months), one case of visual impairment (9.1 months), one case of arthralgia (6.5 months), one case of hypothyroidism (13.0 months), one case of psychiatric adverse reaction (6.5 months) and one case of dermatological adverse reaction (10.0 months). The treatment plan and dosage in the continuous period may have little impact on the occurrence of ADRs, so only the impact of the treatment plan and dosage in the intensive period was analysed. Univariate logistic regression showed that disease severity, treatment and combination medication were the influencing factors of ADRs. After multivariable logistic regression, the results showed that the odds of ADRs in patients with severe TB were 2.39 times higher than those in non-severe patients (OR = 2.44, 95% CI: 1.36–4.39, p = 0.003); patients treated with HRZ(E) + second-line drug(s) in the intensive phase were at higher odds of developing ADRs compared to those treated with HRZ(E) alone (OR = 3.70, 95% CI: 2.01–6.81, p < 0.001) (Table 4).
Occurrence time and duration of each ADR among paediatric tuberculosis patients in China, 2017–2022.
Patients were more likely to have ATDILI and lead to protocol change than other ADRs (Figure 2), followed by kidney dysfunction, gastrointestinal reaction and visual impairment. Among the ADRs that led to treatment discontinuation, gastrointestinal reaction was the most common, followed by ototoxicity, and dermatological.
Severity assessment of each ADR among paediatric tuberculosis patients in China, 2017–2022.
Discussion
In a large hospital-based study of children with TB from 11 representative paediatric TB hospitals throughout China, the incidence of ADRs was common reaching almost one in five children. Although the incidence of ADRs in our study was lower than the reported range of ADRs among adults with TB [17–24], it is relatively similar to the incidence reported in some other paediatric TB studies [25–27]. In general, the incidence of ADR was high, and there were large differences between different studies, which might be related to a variety of factors. First of all, different studies had differences in criteria and features of included cases. Second, treatment regimens, types of monitoring, and patient management strategies varied. Since the TB diagnosis and treatment hospitals included in this study were basically provincial or municipal regional diagnosis and treatment centres, more difficult and critical TB cases would be treated than at grass-roots hospitals. In our study, the proportion of severe children with TB was higher, at 63.69%. This high proportion of severe cases may partially contribute to the relatively high incidence of ADRs observed in our study, given that severe cases often require more intensive or prolonged treatment regimens.
ADRs among paediatric TB patients during anti-TB treatment were predominantly haematological damage, gastrointestinal reactions, ATDILI and renal dysfunction. Specifically, ATDILI accounted for only 16% of all ADRs, which was significantly lower than the occurrence frequency reported in adult TB cases [28–30]. In terms of temporal distribution, 56% of paediatric liver injuries occurred within the first 2 weeks of treatment, earlier than the peak incidence at 1–2 months observed in adults [31]. Most ADRs in children with TB emerged during the intensive phase of treatment, consistent with findings in adult studies [29]. Regarding severity, only 17% of paediatric TB patients required drug discontinuation due to ADRs, primarily attributed to gastrointestinal reactions and ototoxicity. Notably, this rate remains substantially lower even when compared to the discontinuation rates observed in adults with multidrug-resistant TB – despite the fact that the latter population typically faces more complex treatment regimens and higher baseline risks of adverse reactions [32,33]. These findings suggested that children with TB had decent tolerance to anti-TB drugs. This provided a confident basis for clinicians to complete the treatment course through supportive therapies (such as hepatoprotective agents and antiemetics) rather than radical drug regimen changes in the presence of mild to moderate ADRs.
Gastrointestinal reactions caused by anti-TB drugs are relatively common in clinical practice, often occurring in the early stages of anti-TB treatment and manifesting as nausea, vomiting, chest burning sensation, etc. In this study, blood system damage accounted for about 1/4 of all ADRs. For ADRs in the blood system that occur during anti-TB treatment, the current recommendation is to take corresponding measures based on the severity of the damage. If symptoms are mild, anti-TB drugs can be continued while closely monitoring changes in blood counts. If the reaction is more severe, the drugs need to be discontinued until the blood routine test returns to normal, and then consideration can be given to restarting the drug treatment at a lower dose [34,35]. ATDILI accounted for about 1/6 of all recorded ADRs. Previous studies have shown that the occurrence of ATDILI is related to many factors, including host factors, drug factors and other factors [36–39]. However, the mechanism of ATDILI is still unclear, which is mainly related to abnormal drug metabolism, mitochondrial damage, immune function damage and genetic factors [40]. Therefore, in the process of anti-TB treatment, changes of liver biochemical indicators should be closely monitored. If the patient has ATDILI, timely intervention should be carried out to prevent serious progression and poor prognosis. Visual impairment is usually associated with ethambutol and linezolid, and the severity of the impairment is related to its dose and duration [41–43]. Relevant studies on TB in children have shown that the incidence of visual impairment related to ethambutol during anti-TB treatment was <1% [41,42]. Our results found that 1.5% of children had visual impairment. Clinically, ethambutol should be used with caution for infants and non-responders who cannot complain and cooperate with visual acuity examination.
Compared with adult TB, TB in children has atypical clinical manifestations, rapid disease progression and dissemination into severe TB [44,45]. Severe patients may have concurrent autoimmune diseases, and the weakened immune function leads to disorders in drug absorption and metabolism. These patients typically need a combination of multiple anti-TB drugs, or even higher doses or longer courses of treatment. This complex treatment regimen increases the risk of drug–drug interactions, thereby elevating the relative risk of ADRs. In addition, some severe patients may be complicated with autoimmune diseases, and the immune system function will decline, which will affect the metabolism and absorption of drugs and increase the risk of ADRs. Although HRZ is the recommended regimen for the intensive phase of TB in children, in clinical practice, doctors may adjust the medication regimen according to the actual situation of patients. For those patients with complex or severe conditions, second-line drugs may be used in combination at the beginning of treatment. Our results showed that these patients were more prone to ADR. This may be because some second-line drugs lack the recommended dose for children, which makes it difficult for clinicians to adjust the dose according to their weight [46,47]. Therefore, for children with TB, clinicians should be cautious in the use of first-line drugs combined with second-line drugs, and if used, the occurrence of ADR in children needs to be closely monitored and early intervention and treatment should be carried out.
Early and correct treatment of ADRs is the key to ensuring patient compliance and successful treatment. Therefore, medical personnel should pay attention to ADRs, explain the possible ADRs and their clinical manifestations to patients and their guardians in detail before anti-TB treatment, and guide patients to conduct self-monitoring to detect and deal with abnormalities in time. At the same time, it is necessary to strengthen the training of medical personnel on the types of ADRs and the risk factors of ADRs, so that they can master the principles and procedures of ADRs.
Conclusions
ADRs are frequently observed during anti-TB treatment in children in China, with haematological system abnormalities and gastrointestinal disturbances being the most common manifestations. The majority of ADRs occur during the intensive phase of treatment and are transient in nature, although a subset may persist over a longer duration. Patients with severe forms of TB or those receiving intensified regimens combining HRZ(E) with second-line agents are at increased risk of developing ADRs. To improve treatment safety and patient adherence, it is recommended to implement targeted monitoring for ADRs – particularly among high-risk paediatric patients during the intensive treatment phase. Furthermore, there is an urgent need to develop optimized, child-appropriate therapeutic strategies that effectively minimize adverse events without compromising antimicrobial efficacy.
Supplementary Material
Table_S1_Characteristics_of_the_adverse_drug_react clean.docx
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dodd PJ, Yuen CM, Sismanidis C, et al. The global burden of tuberculosis mortality in children: a mathematical modelling study. Lancet Glob Health. 2017;5(9):e 898–e 906. doi:10.1016/S 2214-109X(17)30289-9.28807188 PMC 5556253 · doi ↗ · pubmed ↗
- 2Pelzer PT, Stuck L, Martinez L, et al. Effectiveness of the primary Bacillus Calmette–Guérin vaccine against the risk of Mycobacterium tuberculosis infection and tuberculosis disease: a meta-analysis of individual participant data. Lancet Microbe. 2025;6(2):100961. doi:10.1016/j.lanmic.2024.100961.39709975 PMC 12778190 · doi ↗ · pubmed ↗
- 3Martinez L, Seddon JA, Horsburgh CR, et al. Effectiveness of preventive treatment among different age groups and Mycobacterium tuberculosis infection status: a systematic review and individual-participant data meta-analysis of contact tracing studies. Lancet Respir Med. 2024;12(8):633–641. doi:10.1016/S 2213-2600(24)00083-3.38734022 PMC 12061052 · doi ↗ · pubmed ↗
- 4Du Preez K, Jenkins HE, Martinez L, et al. Global burden of tuberculous meningitis in children aged 0–14 years in 2019: a mathematical modelling study. Lancet Glob Health. 2025;13(1):e 59–e 68. doi:10.1016/S 2214-109X(24)00383-8.39706662 PMC 11729397 · doi ↗ · pubmed ↗
- 5da Costa FBP, Nicol MP, Botha M, et al. Mycobacterium tuberculosis infection and tuberculosis disease in the first decade of life: a South African birth cohort study. Lancet Child Adolesc Health. 2024;8(12):891–899. doi:10.1016/S 2352-4642(24)00256-6.39515364 PMC 11579303 · doi ↗ · pubmed ↗
- 6Martinez L, Le Roux DM, Barnett W, et al. Tuberculin skin test conversion and primary progressive tuberculosis disease in the first 5 years of life: a birth cohort study from Cape Town, South Africa. Lancet Child Adolesc Health. 2018;2(1):46–55. doi:10.1016/S 2352-4642(17)30149-9.29457055 PMC 5810304 · doi ↗ · pubmed ↗
- 7WHO. Global tuberculosis report 2024. Geneva: World Health Organization; 2024. Available from: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2024
- 8Koh Y, Yap CW, Li SC. A quantitative approach of using genetic algorithm in designing a probability scoring system of an adverse drug reaction assessment system. Int J Med Inform. 2008;77(6):421–430. doi:10.1016/j.ijmedinf.2007.08.010.17921048 · doi ↗ · pubmed ↗