Concurrent variations of the left renal and gonadal vessels: a case report
Surekha Devadasa Shetty, Mohandas Rao Kappettu Gadahad, Ashwini Aithal Padur, Naveen Kumar, Satheesha Badagabettu Nayak

TL;DR
This case report describes unusual blood vessel variations near the left kidney, which could impact kidney surgeries and transplants.
Contribution
The report documents a rare case of multiple vascular variations in the left kidney region.
Findings
An additional left renal artery originated from the abdominal aorta below the inferior mesenteric artery.
An additional renal vein drained into the left common iliac vein.
Two testicular veins were present on the left side.
Abstract
A thorough knowledge of vascular variations in the vicinity of the kidney is essential due to the increased number of kidney transplants, more so on the left side because the donor’s left kidney is preferred for transplantation. We found multiple vascular variations in the vicinity of the left kidney, which were noted during routine dissection classes. The left renal artery arose from the abdominal aorta and supplied the left kidney in a usual manner. There was an additional left renal artery, which took its origin from the abdominal aorta, below the origin of the inferior mesenteric artery. This artery was accompanied by an additional renal vein, which drained into the left common iliac vein. On the left side, there were two testicular veins. Knowledge of these abnormal vessels can be useful during radiological and surgical procedures in cases of nephrectomies, renal tumors,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
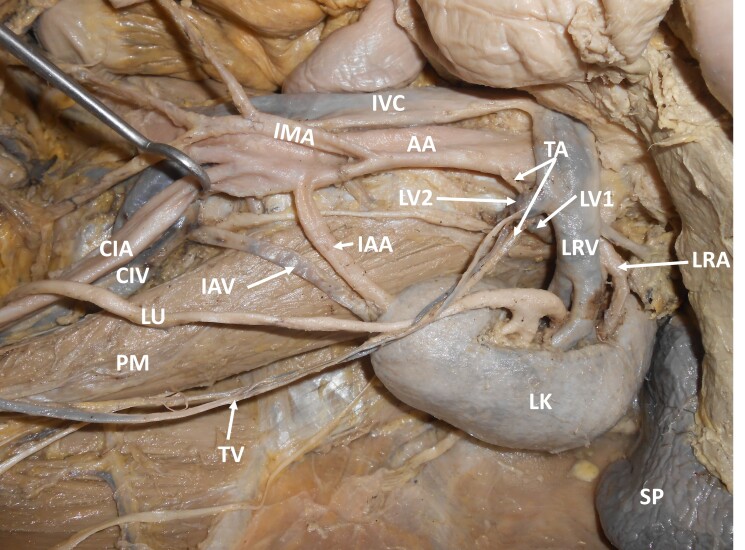 Figure 1
Figure 1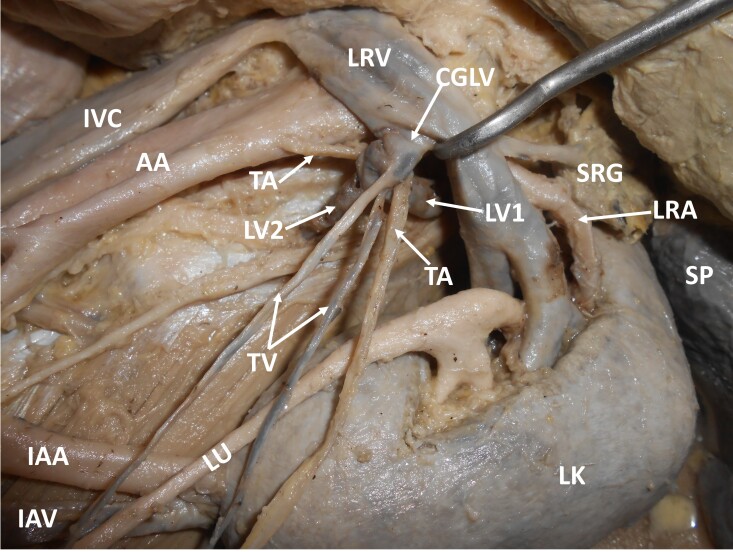 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal and Vascular Pathologies · Vascular anomalies and interventions · Infectious Aortic and Vascular Conditions
INTRODUCTION
The renal arteries are a pair of lateral branches of the abdominal aorta arising just below the level of the origin of the superior mesenteric artery.^1^ Variations in number and branching of renal arteries are common.^2,3^ Renal artery variations have been classified as aberrant, supplementary, and accessory, among other terms.^1^ Accessory renal arteries are frequently seen, especially on the left side.^4^ They usually enter above or below the renal hilum.^5^ Supernumerary renal arteries are of two types: polar or accessory hilar type. Polar type arteries enter the kidney through the pole without passing through the hilum, whereas accessory hilar type arteries enter the kidney after passing through the hilum.^6^ Various developmental positions of the kidney are one of the main reasons for renal arteries abnormalities.^7^
The renal veins lie anterior to the renal artery and open into the inferior vena cava at the level of the 1st and 2nd lumbar vertebrae. The right renal vein is a short vessel and does not receive any tributaries except from the right kidney. The left renal vein crosses anterior to the aorta to open into the left lateral aspect of inferior vena cava and is three times longer than the right. It usually receives two tributaries, the left suprarenal vein and the left gonadal vein.^5^
The testicular artery is a branch of the abdominal aorta, given off at the level of the 2nd lumbar vertebra below the renal artery. The testicular artery may show variations at its origin or may be absent. One or both of these arteries may arise from the renal artery, suprarenal artery, or lumbar artery. The testicular veins accompany the arteries.^8^ Congenital variations of the testicular vein include variations in its course, areas of drainage, and termination.^9^
Here, we present a case of concurrent variations of the left renal and gonadal vessels. This variation could predispose a person to varicocele and infertility. Urologists and radiologists may find this case useful in their practice.
CASE REPORT
During dissection classes for medical undergraduates, we witnessed multiple vascular variations in relation to the left kidney. The variations were unilateral and were observed in a South Indian adult male cadaver. The left kidney was supplied by the left renal artery, arising as usual from the abdominal aorta, and was drained by the left renal vein into the inferior vena cava. Apart from this, the left kidney was also supplied by an aberrant renal artery arising from the abdominal aorta, one inch below the origin of the inferior mesenteric artery. This artery entered the kidney through its inferior pole. This artery was accompanied by an aberrant renal vein, which drained into the left common iliac vein. There were two testicular veins on the left side. About 1cm below the left renal vein, these two veins united with the first and second lumbar veins to form a ‘common gonado-lumbar vein’. The common gonado-lumbar vein drained into the left renal vein. Further, the left testicular artery arose from the abdominal aorta, ascended upwards and hooked around the junction of the first lumbar vein with the common gonado-lumbar vein. The further course of the testicular artery was normal. These variations are shown in Figures 1 and 2. Ethics committee clearance was obtained for the study. This study complies with the Helsinki Declaration and with local ethical guidelines. We have obtained all appropriate consent forms and ethics committee clearance for the use of cadavers in this study. No patient data were used in the study.
Dissection of the upper abdomen, showing the multiple vascular variations. IVC – inferior vena cava; AA – abdominal aorta; IMA – inferior mesenteric artery; LRV – left renal vein; LRA – left renal artery; SP – spleen; LK – left kidney; LU – left ureter; IAA – inferior accessory artery; IAV – inferior accessory vein; LV1 – first lumbar vein; LV2 – second lumbar vein; TA – testicular artery; TV –testicular veins; PM – psoas major; CIV – left common iliac vein; CIA – left common iliac artery.
Closer view of the multiple vascular variations. IVC – inferior vena cava; AA – abdominal aorta; LRV – left renal vein; LRA – left renal artery; SP – spleen; LK – left kidney; LU – left ureter; IAA – inferior accessory artery; IAV – inferior accessory vein; CGLV – common gonado-lumbar vein; LV1 – first lumbar vein; LV2 – second lumbar vein; TA – testicular artery; TV –testicular veins; SRG – suprarenal gland.
DISCUSSION
Other than the main renal artery, any artery arising from the abdominal aorta and entering the kidney should be named an accessory renal artery and any renal artery that arises from a source other than the aorta and enters the kidney should be called an aberrant renal artery.^10^ When aberrant renal arteries enter the upper or lower poles of the kidney, they are named polar arteries.^11^ Accessory renal arteries are end arteries and if an accessory renal artery is ligated, the part of the kidney it supplies becomes ischemic.^4^ Abnormal renal arteries penetrate the substance of the kidney rather than entering its hilum to supply it. The currently observed variant renal artery, entering the left kidney through the inferior pole should be called by all three names, as accessory renal artery, aberrant renal artery, and inferior polar artery. Inferior polar arteries have been implicated as an etiological factor in a form of hydronephrosis correctable by surgery.^12^
Many authors have reported the presence of aberrant renal arteries. They happened to enter the kidney as either upper or lower polar arteries. Short polar arteries can enhance the degree of difficulty during surgical procedures.^13,14^
The left renal vein normally drains into the inferior vena cava, after passing anterior to the abdominal aorta. There are also reports of lumbar veins draining into the left renal vein. Recently, a case of renal vein variation was reported in which left suprarenal, ovarian, and lumbar veins drained into a single left renal vein which then drained into the left common iliac vein.^15^ In another case, there were two left renal veins, one of which retroaortically drained into the inferior vena cava, while the other drained into the left common iliac vein.^16^ A retroaortic course of the left renal vein is relatively rare.^17^ Very rarely, the left renal vein receives the left gonadal vein indirectly through the kidney. A case has also been reported in which the left testicular vein penetrated the lower pole of the kidney before opening into the renal vein.^18^ In some cases, the inferior pole of the kidney drains into the contralateral common iliac vein through a separate vein.^19^
Testicular veins can be absent, double, triple, or multiple.^20,21^ Variations in the terminations of testicular veins have also been reported. The right testicular vein might drain into the right renal vein, an accessory renal vein, or the lower part of the inferior vena cava.^22^ The left testicular artery may arch around the left renal artery or renal vein before it descends.^23^
Possible embryologic basis of the variation
The definitive left renal vein develops from the left mesonephric vein, left subcardinal vein, and intersubcardinal anastomosis. The part of the subcardinal vein above the renal vein forms the left suprarenal vein and the part below forms the gonadal vein. The subcardinal vein communicates with nearby venous channels like the supracardinal veins and azygos line of veins and eventually disappears.^7^ Formation of the gonado-lumbar vein in the current case could be due to the failure of the communications to disappear. The left testicular artery’s looping course around the gonado-lumbar vein could also be due to the union of lumbar veins with the testicular veins. It is very simple to understand the presence of the aberrant inferior polar artery and vein. The kidney begins its development in the pelvic cavity and later ascends. While in the pelvis, it derives its blood supply from the iliac vessels. Later, as it ascends, it receives blood supply from the aorta and drains into the inferior vena cava. During the process of ascent, the pelvic and lower lumbar vessels supplying it degenerate and disappear. In the current case, the presence of aberrant vessels is due to their failure to disappear.
Clinical importance of the case
The current pattern of multiple variations could lead to the development of left sided varicocele. As such, varicoceles are more common on the left side. In the current case, the abnormal hooking of the left testicular artery around the gonado-lumbar vein could alter the hemodynamics of the left testis leading to infertility. Knowledge of the above-mentioned variations could be useful during renal transplant surgeries, therapeutic embolization of testicular veins, and abdominal radiological procedures.
CONCLUSION
Knowledge of renal and gonadal vascular variations is essential for diagnostic, endovascular, and operative procedures involving the abdomen. This report highlights the presence of an aberrant left renal artery and a variant type of termination of the left testicular vein. The unique feature of this case report is the formation of a gonado-lumbar vein by the union of two left testicular veins and the first and second lumbar veins. There are no previous reports of such a termination of the left testicular vein.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Standring S Gray’s Anatomy: the anatomical basis of clinical practice.41th Philadelphia Churchill Livingstone 2016
- 2Asala S Chaudhary SC Masumbuko-Kahamba N Bidmos M Anatomical variations in the human testicular blood vessels Ann Anat 2001183654554910.1016/S 0940-9602(01)80064-911766526 · doi ↗ · pubmed ↗
- 3Nayak SB Shetty SD Ravindra S et al Eight prehilar branches of the right renal artery Anat Cell Biol 201447321421610.5115/acb.2014.47.3.21425276483 PMC 4178199 · doi ↗ · pubmed ↗
- 4Satyapal KS Haffejee AA Singh B Ramsaroop L Robbs JV Kalideen JM Additional renal arteries; Incidence and morphometry Surg Radiol Anat 2001231333810.1007/s 00276-001-0033-y 11370140 · doi ↗ · pubmed ↗
- 5William PL Bannister LH Berry MM et al Cardiovascular system. Gray H Gray’s Anatomy 38th Ed.Churchill Livingstone Edinburg 19951547
- 6Ozkan U Oguzkurt L Tercan F Kizilkilic O Koc Z Koca N Renal artery origins and variations: angiographic evaluation of 855 consecutive patients Diagn Interv Radiol 200612418318617160802 · pubmed ↗
- 7Moore KL Per Sand TVN The developing human.10th Philadelphia Saunders 2015293
- 8Bergman RA Cassell MD Sahinoglu K Heidger PM Jr Human doubled renal and testicular arteries Ann Anat 1992174431331510.1016/S 0940-9602(11)80292-X 1416060 · doi ↗ · pubmed ↗