Early Surgical Intervention in Nonbacterial Thrombotic Endocarditis to Prevent Systemic Embolization
Paul Weber, Dhruva Govil, Christopher Bradley, Stephen Lynch

TL;DR
A 65-year-old woman with a nonbacterial heart mass underwent early surgery to prevent dangerous blood clots, highlighting the importance of multidisciplinary care in rare heart conditions.
Contribution
The case emphasizes early surgical intervention for nonbacterial thrombotic endocarditis to prevent embolization.
Findings
A large, mobile aortic valve mass was identified as nonbacterial thrombotic endocarditis (NBTE).
Surgical excision and anticoagulation reduced embolic risk and confirmed the diagnosis.
NBTE can mimic infective endocarditis but requires different management strategies.
Abstract
Aortic valve masses are rare and diagnostically challenging entities that may confer a significant risk of systemic embolization, particularly when large or highly mobile. We report the case of a 65-year-old woman who presented to an outside hospital with acute chest pain. Electrocardiogram demonstrated no ischemic changes, and serial cardiac troponins were negative. Transthoracic echocardiography revealed a large, mobile mass within the left ventricular outflow tract. Subsequent transesophageal echocardiography identified a 1.8-cm echogenic mass on the ventricular aspect of the aortic valve, prolapsing into the ascending aorta. An extensive infectious disease evaluation, including six sets of blood cultures, showed no evidence of infective endocarditis. Hematologic evaluation revealed a mildly elevated lupus anticoagulant, and perioperative anticoagulation with heparin was recommended,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
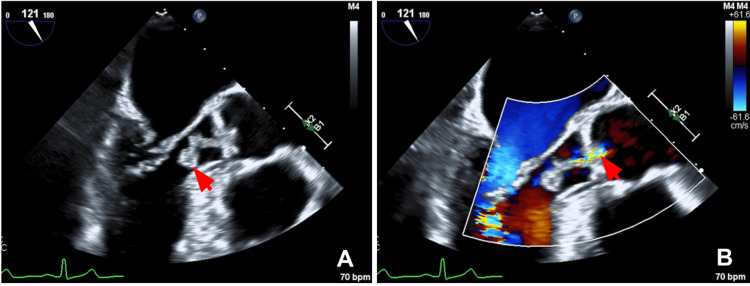 Figure 1
Figure 1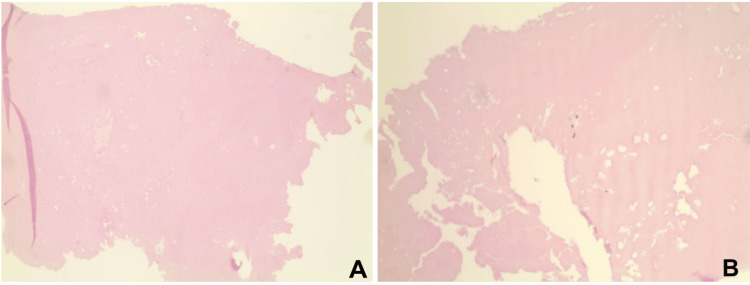 Figure 2
Figure 2| Lab | Value | Reference Range |
| NT-proBNP | 551 pg/mL | 50 - 177 pg/mL |
| Erythrocyte sedimentation rate | 8 mm/hr | ≤ 15 mm/hr |
| C-reactive protein | <3 mg/L | 0 - 10 mg/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Actinomycetales infections and treatment · Aortic Thrombus and Embolism
Introduction
Intracardiac masses are uncommon but carry important diagnostic and prognostic implications when identified. Cardiac valve lesions are particularly challenging, as they span a wide differential diagnosis. Among these, aortic valve masses are especially rare, with large or highly mobile masses having a large risk of systemic embolization requiring prompt and careful evaluation. Nonbacterial thrombotic endocarditis (NBTE) is a rare and frequently underrecognized cause of valvular masses. It is characterized by sterile fibrin or platelet vegetations that form in the absence of active infection and are most often associated with hypercoagulable states, autoimmune conditions, or malignancy. The pathogenesis of NBTE involves endothelial injury, deposition of platelet-fibrin thrombi on previously normal valve surfaces, and amplification with a systemic prothrombotic state. Clinically and echocardiographically, NBTE can closely resemble infective endocarditis, often leading to diagnostic uncertainty and delays in definitive management. Distinguishing between infectious and noninfectious etiologies is critical, as treatment strategies and prognostic outcomes differ substantially.
We present a case of a large, mobile aortic valve mass initially concerning for native valve infective endocarditis (NVE) that was ultimately diagnosed as NBTE following multidisciplinary evaluation, surgical intervention, and histopathologic confirmation. This case highlights the importance of maintaining a broad differential diagnosis for valvular masses and underscores the role of coordinated, multimodal assessment in guiding timely and appropriate management.
Case presentation
A 65-year-old woman presented to an outside hospital with acute substernal chest tightness accompanied by mild dyspnea at rest. Her medical history included hypertension, dyslipidemia, hypothyroidism, a prior transient ischemic attack four years earlier, and an unprovoked submassive pulmonary embolism two years prior, for which she was compliant with lifelong rivaroxaban therapy. She had been in her usual state of health until symptom onset the night prior to presentation, prompting emergency department evaluation the following morning.
On arrival, she was hypertensive with a blood pressure of 194/87 mmHg but otherwise hemodynamically stable, afebrile, and saturating well on room air. Electrocardiogram demonstrated a normal sinus rhythm without ischemic changes, and serial cardiac troponins were negative.
Transthoracic echocardiography (TTE) demonstrated a left ventricular ejection fraction of 55-60% and revealed a large, mobile mass within the left ventricular outflow tract. Transesophageal echocardiography (TEE) further characterized a 1.8-cm echogenic mass attached to the ventricular aspect of the aortic valve, prolapsing into the ascending aorta, and associated with mild aortic regurgitation (Figure 1). Laboratory evaluation revealed elevated NT-proBNP, low inflammatory markers (Table 1), and all other labs within normal limits. Given imaging findings, blood cultures were obtained.
Preoperative transesophageal echocardiography of the aortic valve(A) Long-axis view demonstrating a 1.8-cm mobile mass attached to the aortic valve (red arrow). (B) Color flow Doppler imaging during diastole showing a central jet of mild aortic regurgitation (red arrow).
Given concern for NVE, empiric broad-spectrum antibiotics and a therapeutic intravenous heparin infusion were initiated while oral anticoagulation was temporarily held. Infectious disease, cardiology, and cardiothoracic surgery consultations were obtained. The patient remained afebrile without clinical evidence of infection, and six sets of blood cultures remained negative. She did not meet the Duke criteria for infective endocarditis. Despite this, intravenous ceftriaxone was continued for presumed culture-negative endocarditis until definitive surgical pathology and intraoperative cultures excluded infection. Hematology was also consulted due to her prior unprovoked pulmonary embolism. Hypercoagulable testing revealed a mildly elevated lupus anticoagulant (50 seconds) with negative anticardiolipin, beta-2 glycoprotein, and antinuclear antibodies. There was also no concern for rivaroxaban failure, and therapeutic anticoagulation with heparin was continued perioperatively, with plans to resume rivaroxaban postoperatively.
Given the mass’s size, marked mobility, embolic risk, and lack of evidence for infection, a multidisciplinary consensus favored surgical intervention. Preoperative coronary angiography demonstrated mild, non-obstructive coronary artery disease. Cardiothoracic surgery proceeded with excision of the aortic valve mass and repair of the native valve. Intraoperative inspection via sternotomy and ascending aortotomy revealed a large mass involving all three aortic valve leaflets, which was carefully excised and submitted for culture and histopathologic analysis. Intraoperative TEE demonstrated preserved left ventricular systolic function with trace residual aortic regurgitation.
Pathologic examination of the excised mass (1.7 × 0.8 × 0.5 cm) demonstrated homogeneous eosinophilic organized fibrin without cellular elements (Figure 2). Intraoperative tissue cultures finalized after seven days showed no microbial growth, consistent with nonbacterial thrombotic endocarditis. A limited TTE on postoperative day two showed normal aortic valve structure and function with preserved ejection fraction. The postoperative course was uncomplicated, and rivaroxaban was resumed per hematology recommendations. The patient was discharged home on postoperative day three with close outpatient follow-up.
Histopathology of the aortic valve mass(A, B) Hematoxylin and eosin-stained sections demonstrate a bland, acellular eosinophilic mass composed predominantly of fibrin, without significant inflammatory infiltrate or identifiable microorganisms.
Discussion
Cardiac valve masses, particularly those involving the aortic valve, are rare and often unexpected findings that present a significant diagnostic challenge, with an estimated incidence of less than 1 in 1,000,000 individuals. While some lesions are benign and clinically silent, others carry substantial risk, especially when large or highly mobile. The differential diagnosis is broad and includes primary cardiac tumors, thrombi, vegetations, and metastatic disease, making prompt recognition and accurate diagnosis essential. NBTE, also referred to as marantic endocarditis, is a rare, noninfectious valvular condition characterized by sterile fibrin-platelet vegetations, most commonly occurring in the setting of systemic hypercoagulability, autoimmune disease, or advanced malignancy. NBTE most frequently affects the aortic and mitral valves and is associated with a high risk of systemic embolization, approximately 40% (range 14.1%-90.9%), particularly involving the cerebral and coronary circulations [1-3].
The diagnosis of NBTE is particularly challenging, as it can closely mimic infective endocarditis both clinically and echocardiographically. Large, mobile vegetations and constitutional symptoms, particularly when accompanied by major or minor Duke clinical criteria, frequently raise concern for infectious etiology. However, features that favor NBTE include persistently negative blood cultures, normal or minimally elevated inflammatory markers, sterile tissue cultures, and pathologic findings of acellular fibrinous material [4]. In the present case, repeatedly negative blood cultures, low inflammatory markers, and sterile operative specimens shifted diagnostic suspicion away from infection and toward NBTE. Additionally, the presence of a mildly elevated lupus anticoagulant supported a transient hypercoagulable state, consistent with previously reported associations between NBTE and antiphospholipid antibody-related mechanisms [2].
Management of aortic valve masses should be individualized and guided by lesion characteristics and clinical risk, including size (≥10 mm), mobility, and embolic potential [5,6]. In NBTE, treatment primarily focuses on addressing the underlying prothrombotic condition and preventing thromboembolic complications through systemic anticoagulation. Surgical intervention is generally reserved for patients with large or highly mobile vegetations, hemodynamic compromise, recurrent embolic events, or diagnostic uncertainty [1,7]. In this case, surgical excision was appropriate given the lesion’s size and mobility, the high risk for catastrophic embolization, and the need for definitive diagnosis.
This case highlights the importance of maintaining a high index of suspicion for NBTE in patients presenting with valvular masses and persistently negative blood cultures, particularly in the absence of systemic infection or elevated inflammatory markers. Early distinction between infective and noninfective etiologies is critical, as management strategies and prognostic implications differ substantially. Multidisciplinary collaboration among cardiology, hematology, infectious disease, and cardiothoracic surgery teams was essential in establishing the diagnosis and achieving a favorable clinical outcome.
Conclusions
Intracardiac masses remain rare but potentially high-risk findings. When located on the aortic valve, these lesions present a broad differential diagnosis that includes infective endocarditis, primary cardiac tumors, thrombi, and less common entities such as nonbacterial thrombotic endocarditis. As demonstrated in this case, distinguishing between infectious and noninfectious causes can be challenging, particularly when imaging reveals a large, mobile mass that raises immediate concern for embolic complications.
This case underscores the importance of integrating clinical presentation, microbiologic data, inflammatory markers, advanced imaging, and histopathologic analysis to establish an accurate diagnosis. Persistently negative blood cultures and low inflammatory markers should prompt consideration of alternative etiologies beyond infection. Importantly, this case supports consideration of early surgical intervention in selected high-risk patients with large, highly mobile vegetations, even before embolic events occur, when diagnostic uncertainty persists, and embolic risk is substantial. Early multidisciplinary collaboration was essential in guiding appropriate management and preventing potential catastrophic embolic events.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Non-bacterial thrombotic endocarditis: a clinical and pathophysiological reappraisal Eur Heart J Ahmed O King NE Qureshi MA 2362494620253956532410.1093/eurheartj/ehae 788 · doi ↗ · pubmed ↗
- 2Nonbacterial thrombotic endocarditis: presentation, pathophysiology, diagnosis and management Rev Cardiovasc Med Al Chalaby S Makhija RR Sharma AN Majid M Aman E Venugopal S Amsterdam EA 1372320223907622810.31083/j.rcm 2304137 PMC 11273749 · doi ↗ · pubmed ↗
- 3Nonbacterial thrombotic endocarditis: clinicopathologic study of a necropsy series Rev Esp Cardiol (Engl Ed) Llenas-García RJ Guerra-Vales JM Montes-Moreno S López-Ríos F Castelbón-Fernández FJ Chimeno-García J 49350060200717535760 · pubmed ↗
- 4The 2023 Duke-International Society for Cardiovascular Infectious Diseases criteria for infective endocarditis: updating the modified Duke criteria Clin Infect Dis Fowler VG Durack DT Selton-Suty C 5185267720233713844510.1093/cid/ciad 271PMC 10681650 · doi ↗ · pubmed ↗
- 5Nonbacterial thrombotic endocarditis: a review Am Heart J Lopez JA Ross RS Fishbein MC Siegel RJ 7737841131987354829610.1016/0002-8703(87)90719-8 · doi ↗ · pubmed ↗
- 6Updates in culture-negative endocarditis Pathogens Mc Hugh J Saleh OA 10271220233762398710.3390/pathogens 12081027 PMC 10459830 · doi ↗ · pubmed ↗
- 72020 ACC/AHA guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines Circulation Otto CM Nishimura RA Bonow RO 071143202110.1161/CIR.000000000000093233332149 · doi ↗ · pubmed ↗