Population-based incidence and antimicrobial susceptibility patterns of shigellosis among children and adults from rural and urban Kenya, 2010–2019
Richard Omore, Billy Ogwel, John B. Ochieng, Jane Juma, Victor Omballa, Alice Ouma, George Aol, Allan Audi, George O. Agogo, George Odongo, Clayton Onyango, Newton Wamola, Terry Komo, Daisy Chepkemoi, Elizabeth Hunsperger, Daniel R. Feikin, Joel M. Montgomery

TL;DR
This study analyzed shigellosis incidence and antibiotic resistance in Kenya's rural and urban areas over ten years, finding high rates in young children and older adults.
Contribution
The study provides population-based incidence data and antimicrobial susceptibility trends of Shigella in Kenya across urban and rural settings.
Findings
Shigella incidence was highest in children aged 12–23 months in both rural and urban areas.
Rural areas saw a significant decline in shigellosis incidence over the study period, unlike urban areas.
Most Shigella isolates remained susceptible to ciprofloxacin and ceftriaxone, with resistance being rare.
Abstract
Shigella is an important cause of diarrheal morbidity and mortality globally. Data on disease burden across age groups, in different epidemiologic settings, and over time are needed to guide preventive strategies. We examined shigellosis in two sites in Kenya over a 10-year period. We used data from the Population-Based Infectious Disease Surveillance (PBIDS) platform in a rural (Asembo, population ~35,000) and urban (Kibera, population ~23,000) setting. PBIDS participants presenting to surveillance clinics with diarrhea (≥3 loose stools in 24-hour period) had stool collected and cultured; Shigella isolates underwent antimicrobial susceptibility testing. We estimated incidence by dividing Shigella cases by person-years- observation, adjusting for the proportion of diarrhea cases with stool collected and for care-seeking outside surveillance clinics. From January 1, 2010 to December…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
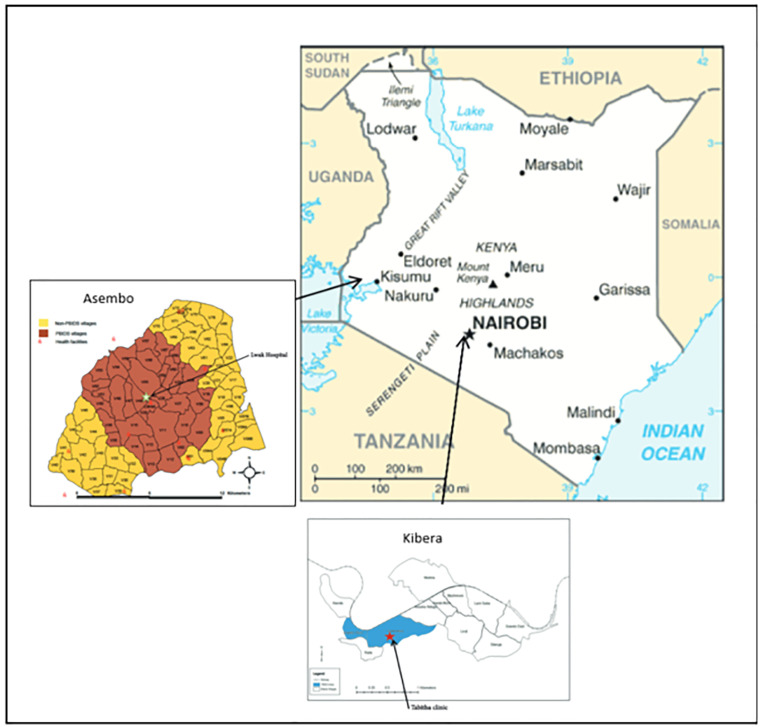 Fig 1
Fig 1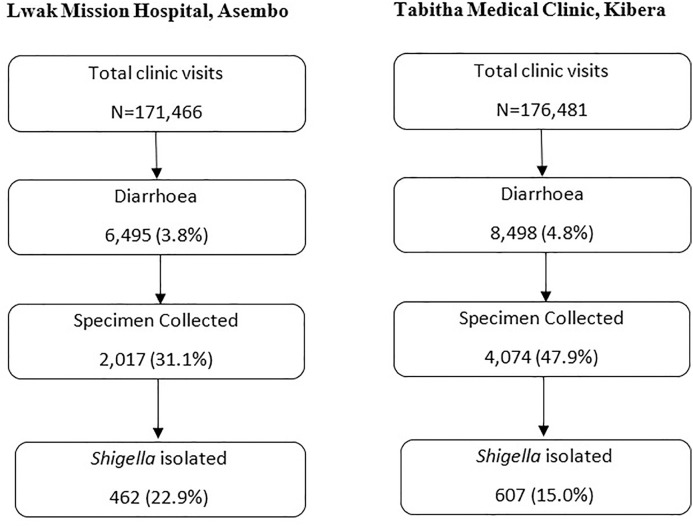 Fig 2
Fig 2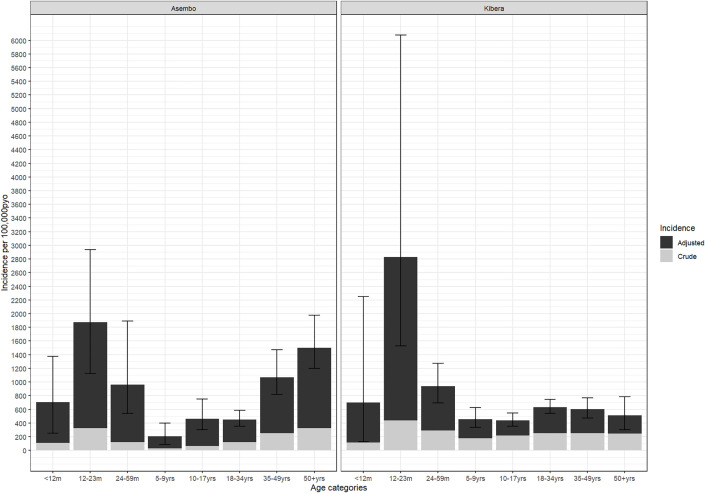 Fig 3
Fig 3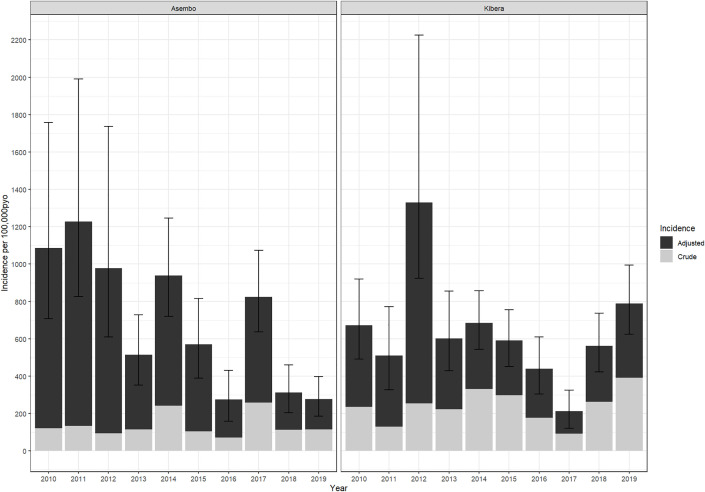 Fig 4
Fig 4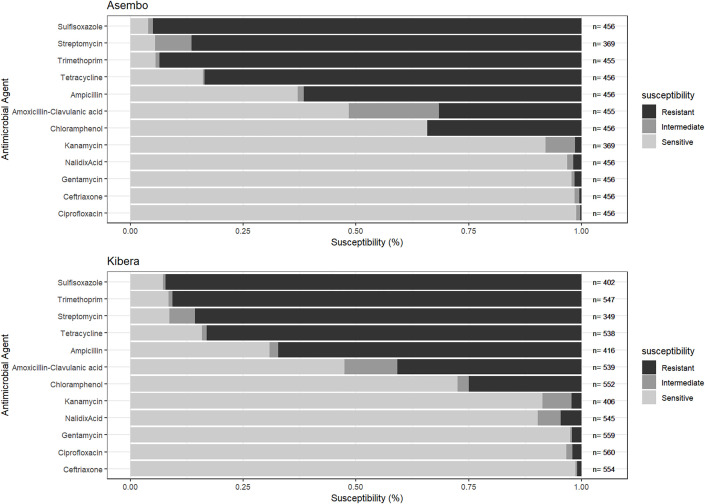 Fig 5
Fig 5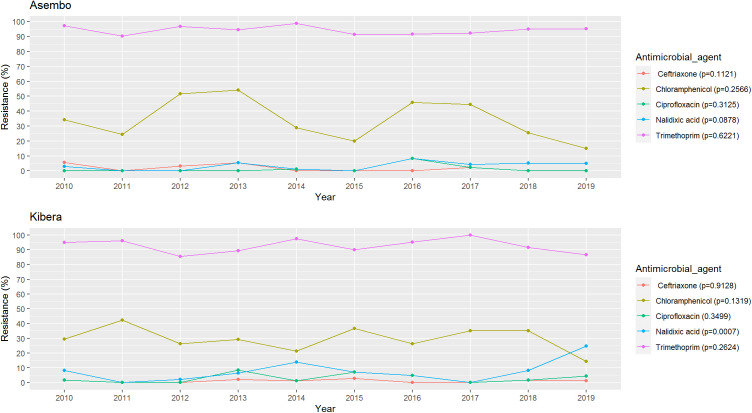 Fig 6
Fig 6- —CDC
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEscherichia coli research studies · Viral gastroenteritis research and epidemiology · Child Nutrition and Water Access
Background
Shigella is a common cause of diarrheal morbidity and mortality in lower-middle-income countries [1,2]. Shigella is highly infectious and spreads through the fecal-oral route with high burden in areas with poor sanitation [3,4]. While all four species of Shigella (Serogroup A: S. dysenteriae, Serogroup B: S. flexneri, Serogroup C: S. boydii, and Serogroup D: S. sonnei) can cause diarrhea and dysentery, species vary in disease severity and geographical distribution [5].
Efforts to prevent and control shigellosis have focused primarily on improvements in safe water, sanitation, and hygiene (WASH), promotion of exclusive breastfeeding for the first six months of life, and prompt treatment with an effective antimicrobial agent to decrease duration of illness and spread of infection [6]. However, the disease burden remains high in settings with limited access to sanitation and healthcare [1,2]. Furthermore, the emergence of resistance among Shigella isolates to commonly used antibiotic agents limits therapeutic options for bacteria in some settings [7]. No vaccines for shigellosis are currently licensed, but several candidates are in development and may offer a complementary strategy to reduce disease burden [1].
Information on Shigella disease burden across age groups, in different epidemiologic settings, and over time is needed to guide vaccine development and other preventive strategies. We used population-based surveillance data to characterize the epidemiology and antibiotic susceptibility patterns of shigellosis in a rural and an urban setting in Kenya over a 10-year period.
Materials and methods
Study setting and study population
The Kenya Medical Research Institute (KEMRI) in collaboration with the US Centers for Disease Control and Prevention (CDC) has jointly operated the Population-Based Infectious Disease Surveillance (PBIDS) platform since 2006 in Asembo and Kibera; the study methods have been detailed elsewhere [8,9]. Both settings have high burdens of infectious disease, characterized by inadequate WASH, and human colonization with multi-drug resistant bacteria is common [8,10,11]. Kibera is a large, densely populated urban informal settlement in Nairobi (population ~23,000) while Asembo is a sparsely populated rural area (population ~35,000) that is malaria-endemic [8] necessitating careful interpretation of fever within our syndromic diarrhea surveillance. The estimated HIV prevalence in Asembo and Kibera among adults was 16% and 6% in 2012 [12] and 15% and 4% in 2018–2019, respectively [13]. Persons residing in the surveillance areas for ≥ four consecutive months were eligible for participation in PBIDS surveillance including children born to active PBIDS participants [8,9]. S1 Fig shows the population distribution of the PBIDS residents at the community and sentinel clinics in both sites.
Data collection methods
Enrolled PBIDS households were visited regularly for collection of demographic data and recent illness including diarrhea (≥3 looser than normal stools in a 24-hour period) [8]. If diarrhea was reported, additional data were collected on whether the stool was bloody, whether healthcare was sought and if so, at which health facility. The frequency of household visits at the start of this study period (January 1, 2010) was weekly. In May 2011, the frequency changed to biweekly, and in April 2015, to biannual. The household data collection tools remained unchanged, and the biannual rounds were conducted continuously over the course of the year.
PBIDS participants received free medical care for acute infectious illnesses at a centrally located health facility in each site. In Asembo, participants resided within ~5 kilometers of the surveillance health facility— St. Elizabeth Lwak Mission Hospital, which has a large outpatient clinic and small inpatient ward (~60 beds). In Kibera, PBIDS participants resided within ~1 kilometer of Tabitha Medical Clinic, which provided outpatient services only. At each of the surveillance facilities (Fig 1), trained clinical staff assessed patients and entered patient data into an electronic patient care system. Patients presenting with diarrhea (≥3 loose stools or clinician diagnosis of diarrhea) were eligible for stool sample collection. Characteristics of stool were captured based on patient or caretaker report.
A series of maps showing Kenya’s location in East Africa, and the locations of KEMRI and CDC jointly operated PBIDS study areas served by St. Elizabeth Lwak Mission Hospital in Siaya County and Tabitha Medical clinic in Kibera, Nairobi, Kenya.
Laboratory methods
Whole stool specimens were collected in stool cups and immediately placed in Cary-Blair transport media, maintained at 4^o^ C, and transported within 24 hours to KEMRI microbiology laboratories located near each site [8]. Stool specimens were cultured by standard techniques for bacterial pathogens; Shigella was identified biochemically [11]. Susceptibility of Shigella isolates to a panel of antimicrobial agents was determined by Kirby Bauer disk diffusion method and interpreted according to 29th edition Clinical and Laboratory Standards Institute (CLSI) guidelines [14]. Isolates that were resistant or had intermediate resistance to antibiotics tested were classified as non-susceptible. Laboratory results were communicated back to the surveillance facilities to guide clinicians in patient management.
Statistical analysis
We described the demographic and clinical characteristics of shigellosis cases using frequencies and percents. Crude shigellosis incidence was calculated as the number of culture-confirmed Shigella cases divided by person-years of observation (PYO) based on cumulative residency within the PBIDS area from January 1, 2010, to December 31, 2019, accounting for migrations. We employed a two-step adjustment in calculating adjusted incidence, to account for both under-sampling and out-of-network care seeking by weighting the number of observed culture-confirmed cases by two proportions: [1] the proportion of PBIDS participants eligible for stool collection (presenting to the clinic with the diarrhea case definition) who had stool collected, and [2] the proportion of diarrheal episodes reported, at household visits, to have sought medical care at a health facility and for which this care was sought at the study facility.
Chi-square or Fisher’s exact tests were used to compare characteristics of participants who had stool collected versus those who did not to understand potential limitations of the adjustment for sample collection. Adjustment factors were stratified by site, age group, study year, and whether diarrhea was bloody or not.
Adjusted case counts were divided by the respective PYOs to estimate adjusted incidence. The uncertainty around the adjusted incidence was calculated using 95% Confidence Intervals (CI) estimated via Monte Carlo simulations (0.025 and 0.975 quantiles of 10,000 simulations), sampling from Poisson distribution for crude incidence, and binomial distribution for adjustment factors as detailed elsewhere by Greenland [15], and as applied previously to data from this surveillance platform [16]. Trends in adjusted shigellosis incidence were assessed using the Mann-Kendall test. For all statistical tests, a two-sided p-value of <0.05 was considered statistically significant. Analyses were performed using SAS statistical software version 9.4 (SAS Institute Inc., Cary, NC).
Ethical procedures
The protocols for this study were reviewed and approved by KEMRI Scientific and Ethics Review Unit (KEMRI SSC Protocol # 1899 and 2761) and CDC (protocol # 4566 and #6775) (See 45 C.F.R. part 46; 21 C.F.R. part 56). Written informed consent was provided by heads of households for household-level participation in PBIDS; individual household members could decline participation. Individual written informed consent was obtained from all patients (or their parents/guardians if aged <18 years) before specimen collection at the surveillance facilities.
Results
Clinic visits and sample collection
From January 1, 2010, through December 31, 2019, there were 171,466 and 176,481 clinic visits in Asembo and Kibera, respectively. of whom 6,495 (4%) and 8,498 (5%) met the case definition for diarrhea, respectively (Fig 2). Overall, stool specimen was collected from 2,017 (31%) of diarrhea cases in Asembo and 4,074 (48%) in Kibera. In both sites, diarrhea cases who provided a stool specimen were older and more frequently presented with bloody stool than those who did not provide stool; in Asembo, additional factors associated with stool specimen collection were presenting with sunken eyes, and hospitalization with male sex less likely to produce stool specimen (S1 Table).
Flow diagram of diarrhoea cases and Shigella testing among Patients seeking care from PBIDS 2010-2018.
Characteristics of shigellosis cases
We isolated Shigella from 23% of stool specimens collected in Asembo, and from 15% in Kibera (Fig 2). Among shigellosis cases in Asembo and Kibera, the median age was 33 and 20 years, respectively; 34% and 44%, respectively, were male (Table 1). Among Shigella cases with known HIV status in Asembo (64%) and Kibera (9%), the HIV infection rate was 25% (74/296) and 9% (5/53), respectively. Bloody stool was reported in 47% of cases in Asembo and 36% in Kibera. In both sites, the most common Shigella species was S. flexneri, accounting for 61% of isolates in Asembo and 67% in Kibera (Table 1). The relative frequency of species varied annually over the 10-year study period in both Asembo and Kibera but with no clear trend over time (S2 Table). Specifically, in both Asembo and Kibera, S. flexneri consistently dominated over the years (42%−90%), with S. sonnei showing a recent upward trend. After a 2013 peak, S. dysenteriae declined in Asembo, while remaining low in Kibera. and S. boydii was more variable in Kibera compared to a low and sporadic presence in Asembo.
Table 1: Characteristics of medically attended Shigella cases in Lwak Mission Hospital, Asembo and Tabitha Medical Clinic, Kibera, Kenya, 2010-2019.
Incidence rates of shigellosis
The overall crude incidences for shigellosis in Asembo and Kibera surveillance areas were 137 (95%CI 66–499) and 239 (95%CI 121–866) per 100,000 PYO, respectively; adjusted incidences were 684 (95%CI 151–2,332) and 647 (95% CI 288-3,887) per 100,000 PYO, respectively (S3 and S4 Tables). In Asembo, the adjusted incidence was highest in the 12–23 months age group (1,873; 95%CI 1126–2937), followed by ≥50 years (1,502; 95%CI 1,202-1,979), and 35–49 years (1,068; 95%CI 818-1,471) (Fig 3 and S3 Table). In Kibera, the adjusted incidence was also highest in the 12–23 months age group (2,828; 95% CI 1,527-6,074) followed by 24–59 months (936; 95%CI 692-1,271), and <12 months (698; 95%CI 127–12,250). By year, the highest adjusted incidence in Asembo was in 2011 (1,227; 95%CI 826-1,991) and the lowest in 2016 (275; 95%CI 158–432) (Fig 4 and S4 Table). In Kibera, the adjusted incidence was highest in 2012 (1,330; 95%CI 923-2,225) and lowest in 2017 (213; 95%CI 122–324). We did not identify any clear outbreak or surveillance change explaining these peaks. In Asembo the adjusted incidence declined significantly during the study period (p = 0.0095), but there was no trend over time in Kibera (p = 0.5312).
*Crude and Adjusted Age-Stratified Shigella Incidence in PBIDS: 2010-2018.Incidence rates were adjusted first for the proportion who were sampled among diarrhea cases, and second for proportion of cases with diarrhea at home who sought care in any clinic other than the surveillance clinic.
*Crude and Adjusted Annual Shigella Incidence in PBIDS: 2010-2018.Incidence rates were adjusted first for the proportion who were sampled among diarrhea cases, and second for proportion of cases with diarrhea at home who sought care in any clinic other than the surveillance clinic.
Antimicrobial prescription and susceptibility patterns
Among shigellosis cases in Asembo, 74% (343/462) were treated with antibiotics on initial presentation to the clinic, including 75% (163/218) of those with and 74% (180/244) without bloody diarrhea (Table 1). Among those prescribed an antibiotic, the most common agents were nalidixic acid (62%), metronidazole—likely prescribed empirically for undifferentiated diarrhea—(46%), and ciprofloxacin (22%). In Kibera, 46% (279/607) of cases were treated with antibiotics, including 43% (92/216) and 48% (187/391) of those with and without bloody diarrhea, respectively. The most frequently used antibiotics in Kibera were ciprofloxacin (67%), metronidazole (48%), and erythromycin (15%).
Only 2% of patients received antibiotics recommended for Shigella to which their isolates were non-susceptible, suggesting generally appropriate empiric treatment. In both sites, Shigella isolates were most frequently non-susceptible to sulfisoxazole, trimethoprim, streptomycin, tetracycline, and ampicillin (Fig 5). In Kibera, 3% of isolates were non-susceptible to ciprofloxacin and 1% ceftriaxone; in Asembo, 1% were non-susceptible to ciprofloxacin and 2% to ceftriaxone. The frequency of ciprofloxacin and ceftriaxone non-susceptibility were highest in 2016 (2/24 [8%]) and 2010 (2/35 [6%]), respectively, in Asembo and 2013 (4/47 [9%]) and 2015 (2/71 [3%]), respectively, in Kibera. Although rare, one isolate in Kibera in 2013 was resistant to both ciprofloxacin and ceftriaxone—the two primary recommended treatments for shigellosis. No isolates from Asembo were non-susceptible to both agents during the study period. In Asembo, non-susceptibility did not significantly change over the study period (Fig 6). In contrast to other antibiotics, nalidixic acid, non-susceptibility in Kibera increased significantly from 8% to 25% (p = 0.0007).
Antimicrobial drug resistance in Shigella among patients seeking care at PBIDS Sentinel Clinics, 2010-2018.
Antimicrobial drug resistance trends in Shigella among patients seeking care at PBIDS Sentinel Clinics, 2010-2018.
Discussion
Our study findings demonstrated: 1) a high incidence of shigellosis in both rural and urban areas of Kenya, with children aged 12–23 months bearing the greatest burden in both areas, and older adults also heavily affected in the rural area; 2) declining incidence over time in the rural setting, but not in the urban setting; 3) Shigella isolates were largely susceptible to first line antibiotics for treating shigellosis; and 4) S. flexneri accounted for approximately two-thirds of all Shigella isolates in both sites.
The high shigellosis burden observed among children aged 12–23 months is consistent with data from other resource-limited settings [11,17–19]. Several factors may contribute to a higher risk of shigellosis in the second year of life. Malnutrition, which is prevalent among children in this age group in resource limited settings [20], heightens the risk of diarrhea, both in terms of incidence and severity [21]. Shigella, specifically, is strongly associated with moderate-to-severe diarrhea in malnourished children [22]. Additionally, children aged 12–23 months have increasing interaction with possibly contaminated environmental reservoirs, especially in settings with inadequate WASH [20]. Moreover, less consumption of breastmilk in the second year of life means reduced protection from maternal antibodies and possibly lactoferrin, which may have antimicrobial activity against Shigella [23]. The high burden of disease among children aged 12–23 months suggests that a Shigella vaccine administered late in infancy [24,25] could be an important prevention tool, in conjunction with efforts to improve WASH.
We also observed a high burden of disease among elderly populations in the rural setting, but not among their urban counterparts. This finding may reflect higher HIV prevalence in the rural population [8,26,27], which has been linked to increased risk and severity of shigellosis [28,29].HIV infection among shigellosis cases in Asembo, based on available HIV status data, was relatively higher than estimates of HIV in the general population from a national survey (25% vs 15%), suggesting possible association between HIV status and shigellosis. Ongoing efforts to prevent HIV infection and improve access and adherence to antiretroviral therapy in Kenya may therefore also serve to lessen the burden of shigellosis, particularly among older adults, and may help explain, in part, the decline in shigellosis incidence observed in the rural area only.
Antibiotics play an important role in the control of Shigella by reducing the duration of illness and risk of disease spread [30]. WHO recommends empiric treatment of dysentry with antibiotics, including ciprofloxacin and ceftriaxone as first line and second line drugs, respectively [31]. In our current study, non-susceptibility to ciprofloxacin and ceftriaxone was detected in both sites, albeit infrequently (<3% of isolates). The observed significant increase over time in resistance to nalidixic acid in Kibera is alarming because nalidixic acid resistance is often a precursor to ciprofloxacin resistance [32]. We observed poor adherence to WHO guidelines, including frequent antibiotic use for Shigella cases that presented with non-bloody stool, highlighting the unreliability of dysentery as a sole indicator of Shigella, and use of antimicrobials not currently recommended for treatment of shigellosis (i.e., metronidazole, erythromycin). Furthermore, ~ 2% of patients were treated with drugs to which their Shigella isolates were not susceptible to. However, in the Vaccine Impact on Diarrhea in Africa (VIDA) study, as much as 25% of moderate-to-severe diarrhea cases in Kenya were prescribed an antibiotic when there was no indication [33]. These findings draw attention to the need for educating clinicians on guidelines for diarrhea management and of the need for continued monitoring of Shigella resistance patterns to help inform treatment recommendations.
Increasing evidence— including from this study, where 53% and 64% of Shigella cases in Asembo and Kibera, respectively, presented without bloody stool—suggests that dysentery alone, as stipulated in the existing WHO guidelines, may not be a reliable indicator of Shigella infection [34,35]. From these observational studies, watery shigellosis are potentially being missed and inappropriately treated, highlighting the need to reassess WHO guidelines and promote point-of-care Shigella diagnostics for accurate and cost-effective treatment [36].
Shigella vaccines under development offer promise in reducing disease burden and antibiotic resistance by preventing infection and limiting empiric antibiotic use. In both rural and urban Kenya, S. flexneri—responsible for about two-thirds of cases—was the most common species, aligning with global findings from low- and middle-income countries [37]. A vaccine targeting Shigella flexneri 2a, 3a, 6, and Shigella sonnei O-antigens could directly cover 64% of global Shigella isolates, based on serotyping data from the Global Enterics Multicenter Study, potentially reaching 88% coverage with cross-protection against other S. flexneri serotypes [38]. Our data highlight the need for a vaccine that offers protection through the second year of life aligning with WHO’s Preferred Product Characteristics for Shigella vaccines targeting infants and young children in LMICs [25]. Our data also suggest that in certain settings, vaccination of older adults against Shigella could be important for optimal disease control as they may be potential reservoirs of infection for children, especially in rural settings where children sometimes remain under the care of the elderly. Shigella-powered studies like Enterics for Global Health (EFGH) surveillance are crucial for generating up-to-date Shigella-specific incidence data and defining primary endpoints, thereby accelerating vaccine trials and licensure [39].
This study has limitations. Adjusted incidence estimates assume that untested diarrhea cases—both at non-surveillance facilities and among those without stool collection at the surveillance clinic—had similar Shigella detection rates as those tested, which may be incorrect. The low stool collection rate and differences between those who provided stool and those who did not may introduce selection bias. Changes in the frequency of household data collection over time could affect the accuracy of healthcare-seeking adjustments. Additionally, culture-based detection likely underestimates Shigella burden due to its lower sensitivity compared to molecular methods [18,20]. Furthermore, some subgroup estimates, particularly in Kibera, have wide confidence intervals and should be interpreted cautiously. No antibiotic susceptibility testing was conducted for azithromycin, which is also currently recommended for shigellosis. Furthermore, data on HIV status was missing for a substantial proportion of cases.
In conclusion, our findings demonstrate a high burden of Shigella among children aged 12–23 months in Kenya, as well as a relatively high burden among older adults and a declining burden over time in a rural context. Shigella isolates remain largely susceptible to first and second-line recommended antibiotics. However, continued monitoring is necessary to detect and contain possible emergence of resistant strains. Our findings suggest that Shigella vaccines under development, if successful, could help reduce both the incidence and antimicrobial resistance burden of Shigella in Kenya, and that longitudinal population-based surveillance data can inform the development of candidate vaccines, strategies for vaccine roll-out, and evaluation. Nonetheless, population-based surveillance should integrate data on household WASH infrastructure and practices to better identify risk factors and strengthen intervention strategies for long-term, definitive control of Shigella and other enteric infections.
Disclosure
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Kenya Medical Research Institute, US Centers for Disease Control and Prevention, nor any other partner institutions.
Supporting information
S1 FigPopulation Distribution of PBIDS surveillance sites and sentinel clinics, Kenya 2010–2019.(TIF)
S1 TableCharacteristics of diarrhoea cases that had stool sample collected compared to those who had no stool sample collected from PBIDS, 2010–2019.(DOCX)
S2 TableDistribution of Shigella species over time: 2010–2019.(DOCX)
S3 TableAge-stratified Shigella incidence in Asembo and Kibera surveillance areas, 2010–2019.(DOCX)
S4 TableShigella incidence rates in Asembo and Kibera, 2010–2019.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Khalil IA, Troeger C, Blacker BF, Rao PC, Brown A, Atherly DE, et al. Morbidity and mortality due to shigella and enterotoxigenic Escherichia coli diarrhoea: the global burden of disease study 1990–2016. The Lancet Infectious Diseases. 2018;18(11):1229–40.30266330 10.1016/S 1473-3099(18)30475-4PMC 6202441 · doi ↗ · pubmed ↗
- 2Lamberti LM, Bourgeois AL, Fischer Walker CL, Black RE, Sack D. Estimating diarrheal illness and deaths attributable to Shigellae and enterotoxigenic Escherichia coli among older children, adolescents, and adults in South Asia and Africa. P Lo S Negl Trop Dis. 2014;8(2):e 2705. doi: 10.1371/journal.pntd.0002705 24551265 PMC 3923718 · doi ↗ · pubmed ↗
- 3Paciello I, Silipo A, Lembo-Fazio L, CurcurùL, Zumsteg A, Noël G, et al. Intracellular Shigella remodels its LPS to dampen the innate immune recognition and evade inflammasome activation. Proc Natl Acad Sci U S A. 2013;110(46):E 4345-54. doi: 10.1073/pnas.1303641110 24167293 PMC 3832022 · doi ↗ · pubmed ↗
- 4Du Pont HL, Levine MM, Hornick RB, Formal SB. Inoculum size in shigellosis and implications for expected mode of transmission. J Infect Dis. 1989;159(6):1126–8. doi: 10.1093/infdis/159.6.1126 2656880 · doi ↗ · pubmed ↗
- 5Shigellosis. The Lancet. https://www.thelancet.com/article/S 0140-6736(17)33296-8/fulltext. Accessed 2023 November 16.
- 6Khan MU. Interruption of shigellosis by hand washing. Trans R Soc Trop Med Hyg. 1982;76(2):164–8. doi: 10.1016/0035-9203(82)90266-8 7101400 · doi ↗ · pubmed ↗
- 7Ranjbar R, Farahani A. Shigella: antibiotic-resistance mechanisms and new horizons for treatment. Infect Drug Resist. 2019;12:3137–67.31632102 10.2147/IDR.S 219755 PMC 6789722 · doi ↗ · pubmed ↗
- 8Feikin DR, Olack B, Bigogo GM, Audi A, Cosmas L, Aura B, et al. The burden of common infectious disease syndromes at the clinic and household level from population-based surveillance in rural and urban Kenya. P Lo S One. 2011;6(1):e 16085. doi: 10.1371/journal.pone.0016085 21267459 PMC 3022725 · doi ↗ · pubmed ↗