The Implementation of Early Intervention Initiatives for Psychosis in Latin America and the Caribbean: A Case Study
Ruben Valle, Camila Velez, Srividya N. Iyer

TL;DR
This study explores the challenges and strategies for implementing early psychosis intervention programs in Latin America and the Caribbean, highlighting cultural adaptations and resource limitations.
Contribution
The paper provides new insights into implementing early psychosis interventions in low-resource settings by analyzing real-world initiatives and implementers' perspectives in Latin America and the Caribbean.
Findings
EIP initiatives in LAC face challenges like resource shortages and cultural adaptation difficulties.
Participants emphasized the importance of task-shifting and leveraging existing services for sustainability.
Most initiatives struggled with sustainment due to reliance on international funding and limited policy support.
Abstract
Psychosis is a serious mental illness, with onset in adolescence and young adulthood. Few early intervention for psychosis (EIP) programs exist in the Global South, where most of the world’s youth live. Addressing this gap requires understanding implementation contexts, pathways, and challenges. This study examines EIP initiatives in Latin America and the Caribbean (LAC) and explores implementers’ perspectives on scaling them. A single-case study design was employed. Guided by the Exploration, Preparation, Implementation, and Sustainment (EPIS) framework, we conducted semi-structured interviews with EIP implementers across LAC and gathered policy documents. Data was coded and analyzed using thematic analysis. Twenty-five participants from 10 countries described 26 initiatives, including clinical and research programs, guidelines, and a technical standard. Themes were mapped onto the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
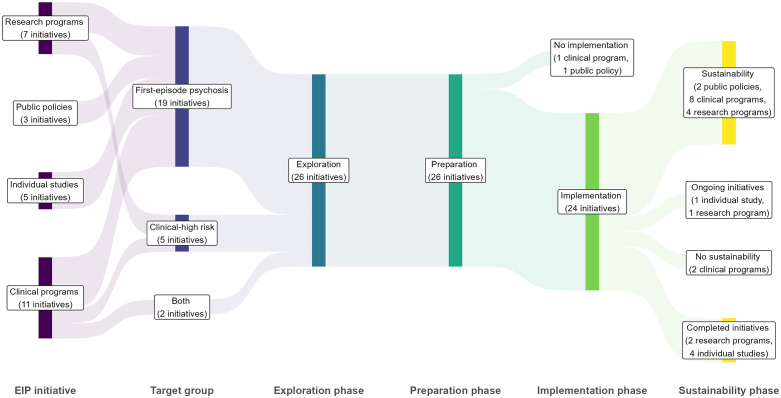 Fig 1
Fig 1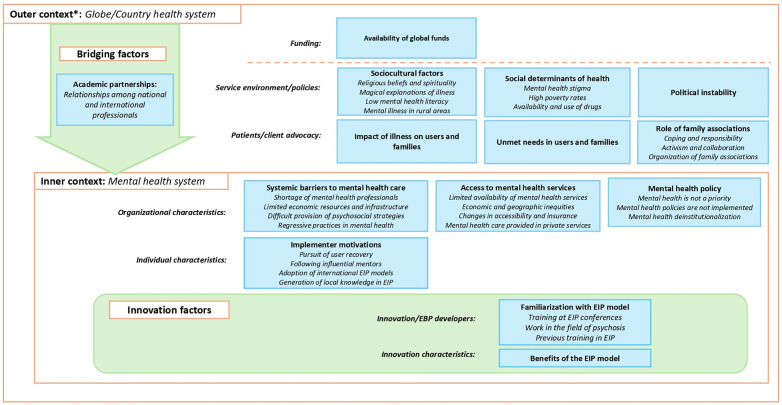 Fig 2
Fig 2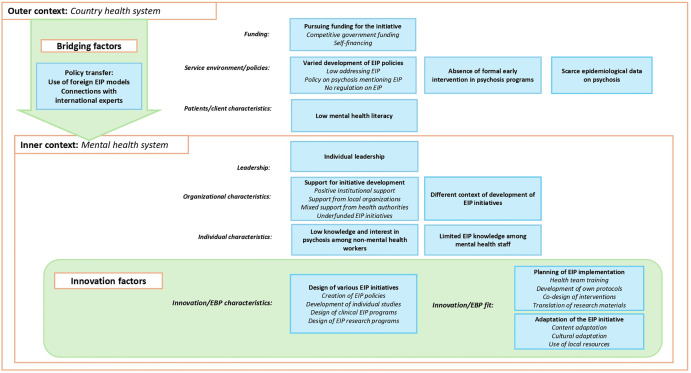 Fig 3
Fig 3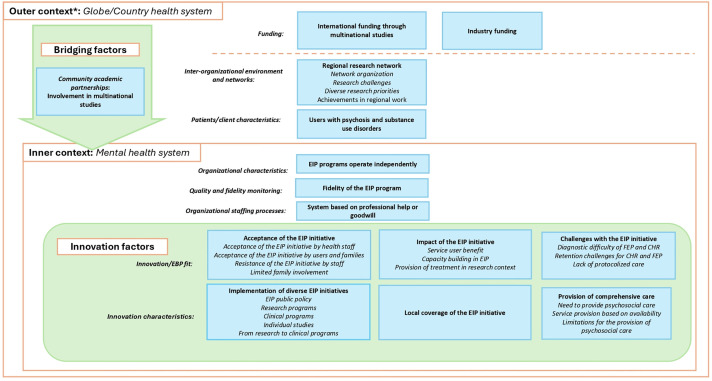 Fig 4
Fig 4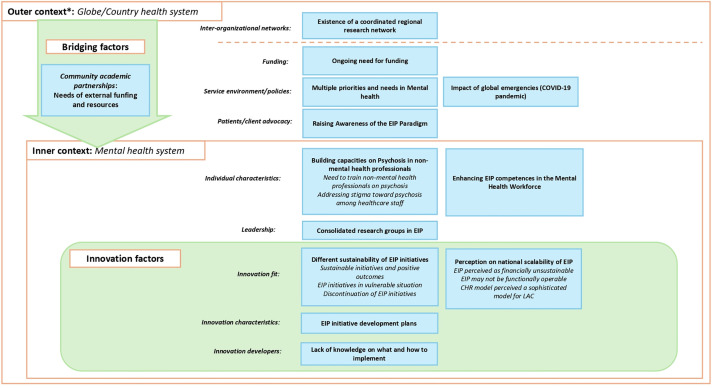 Fig 5
Fig 5- —CIHR
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth Policy Implementation Science · Mental Health and Patient Involvement · Schizophrenia research and treatment
Introduction
Early Intervention for Psychosis (EIP) is a multicomponent service model for early stages of psychotic disorders, specifically, clinical high-risk for psychosis (CHR) and first-episode psychosis (FEP) [1,2]. Grounded in a philosophy of hope and optimism [3], EIP promotes recovery by offering targeted interventions to patients and families (i.e., medication, case management, cognitive-behavioral therapy, family psychoeducation, etc.) [2]. Evidence from randomized clinical trials, systematic reviews, and meta-analyses shows that EIP leads to better clinical and functional outcomes in FEP compared to standard care [4–7]. Cost-effectiveness analyses demonstrate benefits in high- and low-resource countries [8,9]. For CHR, evidence is relatively weaker but suggests that EIP can reduce symptoms and potentially delay or prevent onset [10].
EIP programs are widely implemented in many high-income countries (HICs) [11], typically as stand-alone services, but also through integrated services and hub-and-spoke models [12]. Pathways to implementation have been diverse, including government policies and research projects [13]. The success of EIP in HICs has relied on leadership, sustained funding, supportive policies, and partnerships [11]. Efforts complementary to EIP services development, like research [14], guidelines [15], and policies, have helped generate evidence, standardize care, and raise awareness about EIP’s benefits [16].
In Latin America and the Caribbean (LAC), where almost 60% of countries are low-and middle-income countries (LMICs) [17], EIP implementation has been fragmented. Brazil established the first documented EIP program in 1999 [18], contemporaneous with many HICs. Yet by 2011, a narrative review found that only Brazil and Mexico had programs [19]. A 2020 scoping review identified EIP programs in those two countries, plus two Chilean facilities and a one-off Argentinian study training primary care staff to refer FEP cases [20]. A 2025 narrative review reported no further expansion [21]. EIP programs in LAC remain concentrated in research centers within tertiary care in metropolitan areas, thus reaching fewer people [19–21].
Previous work on EIP in LAC has largely used desk reviews and focused on clinical programs [19–21], limiting our understanding into contextual factors, implementation processes, or challenges underlying uneven provision and uptake. Non-clinical initiatives have been overlooked despite their potential role in expanding EIP. For instance, many research projects in LMICs aim to evolve into services [22,23], and policies can facilitate care provision in psychosis [24]. Replicating EIP programs from HICs in LAC is not feasible due to socio-cultural and resource differences, highlighting the need to examine the full spectrum of EIP initiatives and multiple implementation pathways [25,26].
Addressing these gaps requires applying well-established implementation science frameworks to analyze implementation pathways, strategies, and contextual influences, as well as the roles and motivations of diverse stakeholders advancing EIP within their countries. Accordingly, this study’s objectives are to examine the implementation processes of EIP initiatives in LAC and explore implementers’ perspectives on disseminating EIP across the region. Understanding how EIP initiatives are implemented in LAC is critical to inform the adaptation, sustainability, and scale-up of these models in resource-constrained health systems, and to generate implementation-relevant evidence that can guide policy and service development both within the region and in other LMIC contexts. Examining EIP initiatives in LAC can also be valuable for expanding how EIP is conceptualized and enacted across diverse settings. Implementation in contexts shaped by social inequality, constrained specialist capacity, and fragmented care pathways can surface context-specific insights regarding the role of social determinants, alternative or non-specialist interventions, locally anchored explanatory models, and cultural and operational adaptations that align EIP with the broader health system and community realities and preferences.
Methods
Ethics statement
The project was approved by the Institutional Review Board of McGill University’s Faculty of Medicine (reference number: A05-E47-24B, approved 30 May 2024). The privacy rights of participants have been observed, and all participants provided written informed consent and allowed audio/video-recording of interviews.
Design
This qualitative study uses a single case design with embedded units [27]. The single case is EIP implementation in LAC. The embedded units of analysis are country-level EIP initiatives. This design was chosen to generate an in-depth analysis of both the implementation of EIP in LAC as a region, and each initiative’s trajectory. The study was guided by the well-established [28,29] Exploration, Preparation, Implementation, and Sustainment (EPIS) implementation framework [30–32]. This framework examines the outer context (factors external to the intervention), the inner context (internal factors within the intervention setting), bridging factors (mechanisms that connect the outer and inner contexts), and the innovation context (characteristics of the intervention) as well as different implementation phases, and is therefore well aligned with the study’s objectives. EPIS phases are: *Exploration (*assessing needs and deciding to adopt the intervention), Preparation (identifying barriers, facilitators, and adaptations), Implementation (launching the intervention and monitoring) and Sustainment (ensuring continued delivery). The study follows the Standards for Reporting Qualitative Research (S1 Table) [33].
Definitions
An EIP initiative refers to a plan or process addressing FEP or at CHR, including:
Clinical programs: organized healthcare services providing assessment, treatment, and follow-up.Research programs: structured, often multi-year initiatives, to generate knowledge around a theme.Clinical guidelines: evidence-based recommendations developed by experts for assessment, diagnosis and treatment.Technical standards: documents issued by an authoritative body specifying procedures, minimum requirements, and operational criteria for service delivery.Individual studies: standalone research projects addressing specific questions or evaluating care components.
Study settings
LAC has 664 million inhabitants in 42 countries [34]; 24.5% are aged 15–29 years [34], an age group at heightened risk for psychosis [35]. By 2015, Brazil, Chile, Panama, and Peru had community-based mental health models [36,37]; in most other LAC countries, care remains centralized in city-based psychiatric hospitals [38]. Schizophrenia affects 277.8 per 100,000 people in LAC [39], yet estimated service coverage is only 26.7% [40]. Treatment consists primarily of antipsychotic medication, with limited availability of psychosocial interventions [41].
Participants
Eligible participants were clinicians, researchers, or policymakers involved in implementing EIP initiatives in LAC. Purposive sampling [42] was used to identify initial implementers via systematic reviews [19–21], conference abstracts [43], and networking. Based on the results, we identified 22 initiatives and compiled a dataset of the 22 primary implementers of each of these initiatives. The dataset comprised initiative type, implementers’/authors’ names, institutions, and emails. We invited all 22 participants via email to explain the study, obtain consent, and schedule the individual interview. We used snowball sampling to identify additional participants.
Sample size
The sample size was determined based on data saturation [44] and ensuring the inclusion of at least one implementer per identified initiative. The final sample included 25 participants — 20 of the 22 initially identified implementers (response rate = 90%), two replacements (e.g., co-authors) for two primary implementers who did not respond, and three identified through snowball sampling (representing three new initiatives that had not initially been identified in our dataset). The 25 participants represented 26 EIP initiatives, with one participant reporting that he had helped implement two initiatives during the interview.
Data saturation was reached by interview 22, as no new codes or themes emerged in the final two interviews during iterative coding and team-based analysis. However, the three subsequent interviews had been conducted to cover the three new initiatives that had emerged from snowball sampling to ensure that all identified initiatives had been covered by our interviews. Table 1 presents sample characteristics. Seventeen participants reported clinical practice as their primary activity and 12 reported research. 20 had backgrounds in psychiatry and five in psychology.
Table 1: Sociodemographic characteristics of participants (n = 25).
Data collection
Semi-structured interviews (~one hour) were conducted via Zoom from August 2024-February 2025 in Spanish or English and video-recorded. We used a demographic questionnaire and an EPIS-based open-ended interview guide, that was adapted to each EIP initiative and topics raised during interviews (S1 Text). The questionnaire and guide were piloted in three interviews with EIP coordinators in Canada and India. At the end of the interview, participants were asked to share relevant policy documents.
Reflexivity
RV, the first author and interviewer, is a male psychiatrist from Peru with a master’s in epidemiology and a doctoral focus on EIP. His professional background and cultural proximity may have facilitated rapport and trust with interviewees. CV, an immigrant woman from Colombia, is a psychotherapist and doctoral student with familiarity with the LAC region but no prior EIP experience, offering an outsider perspective with respect to EIP and approaching the data with fresh eyes. SNI, an immigrant psychologist and experienced EIP researcher in Canada and LMICs, contributed broad expertise during analysis. Throughout the analysis, the team engaged in reflexive discussions to examine how their identities, disciplinary backgrounds and professional experiences influenced their coding decisions and interpretations. Differences in interpretations were discussed collectively, with interpretations refined through questioning assumptions and alternative explanations during theme refinement and development. The team also maintained reflective notes during analysis to document assumptions, reactions and perceived power dynamics.
Data analysis
Recordings were transcribed in their original language. Following an iterative process during and after data collection, we used thematic analysis to identify, analyze, and report patterns within the data [45]. This involved familiarization with the data, generation of initial codes, identification and review of themes and subthemes, refinement, definition, and synthesis. RV and CV independently coded transcripts in ATLAS.ti (v25), met regularly and reached consensus through discussion, involving senior author SNI at critical junctures. Themes were subsequently mapped onto the EPIS framework, which are presented in Results with illustrative quotes.
Rigor and trustworthiness [46] were ensured through prolonged engagement with the data, investigator triangulation via independent coding, data triangulation between interviews and four health policy documents shared by participants, grounding findings in participants’ quotations, and member checking by sharing preliminary themes with participants (in group presentations and individual communications).
Results
EIP initiatives
Participants implemented 26 EIP initiatives across 10 countries, with one participant reporting on two initiatives (Table 2). These included 11 clinical programs, seven research programs, two clinical guidelines, one technical standard, and five individual studies. Most (19) initiatives focused on FEP, five on CHR, and two on both. All progressed through the exploration and preparation phases of EPIS. At the time of the interviews, one standard awaited government approval, and one planned clinical program awaited funding for implementation. Among those implemented, only some advanced to sustainment. Two clinical programs were discontinued, four studies ended without follow-up projects, two research programs concluded without additional funding, and one study and one research program were ongoing but faced uncertain futures (Fig 1).
Table 2: Early intervention in psychosis initiatives (n = 26) by country.
Implementation trajectories of 26 EIP initiatives in Latin America and the Caribbean.Public policies include clinical guidelines and standards. The EPIS framework conceptualizes implementation as a dynamic process unfolding across four interrelated stages. During the Exploration stage, implementers identified emerging or existing clinical or public health needs and considered whether and how an intervention may address those needs. The Preparation stage focused on planning for adoption by identifying barriers and facilitators, assessing adaptation needs, and developing implementation plans. The Implementation stage involved the delivery of the intervention within systems, supported by ongoing monitoring and adjustment of implementation strategies. The Sustainment stage reflected the continuation of intervention delivery over time, supported by ongoing contextual conditions and adaptations.
Exploration phase
Participants reflected on their motivations for implementing EIP and their local settings (Fig 2). Most initiatives were locally driven, motivated by participants’ awareness of the impacts of untreated psychotic illnesses and unmet needs for comprehensive care on individuals and their families (suffering, employment/social losses, etc.). Many became involved in EIP through attending international meetings, prior work in non-EIP psychosis services, and/or postgraduate or international training.
*Themes and subthemes identified regarding the Exploration phase of 26 EIP initiatives.The outer context comprises two dimensions, separated by the dashed orange line: global context and the national health systemin which EIP initiatives were implemented. In the exploration phase, at the global level, the availability of international funding for the development of EIP studies was highlighted, while at the local level, sociocultural factors and the unmet needs of people with psychosis and their families were emphasized. Within the inner context, the figure primarily highlights barriers to accessing mental health services, alongside the presence of champions seeking to improve psychosis care through clinical services, research, or policy development. Pre-existing relationships between local mental health professionals and international counterparts were reflected as Bridging factors. Familiarity with and knowledge of the EIP model, as well as its perceived benefits, emerged as key determinants at this stage.
“The World Psychiatric Association offered training opportunities. I applied for a call to receive training at [organization in HIC], where they kindly showed me everything they were doing and allowed me to participate in their activities. This greatly inspired me to propose an early intervention program.” [Interview 5]
Clinicians were inspired by EIP’s recovery orientation and by mentors. Researchers were drawn to generating local evidence for EIP in LAC, while policymakers aimed to implement best practices for people with psychosis. In a few cases, international researchers and funders initiated projects in collaboration with local leads, with funders requiring locally based leadership.
“Our program emerged because a group at [foreign university], led by [researcher], a professor of psychiatric epidemiology with experience working in LAC, reached out to us and said it might be interesting to implement an adapted version of [EIP program] in [country], taking advantage of the [Health policy] to develop a program specifically for first-episode psychosis. So, we applied for a [foreign agency] grant.” [Interview 2]
Implementation contexts were widely seen as challenging. Mental health was not a governmental priority; recent regulations, though well-intentioned, often fell short due to limited resources and organizational capacity; and deinstitutionalization policies were rarely paired with services development. Only one country, where a clinical guideline for first-episode schizophrenia is supported by a universal access to health care law and strong primary care, was seen as supportive of case identification. Most described persistent structural barriers, including shortages of personnel, infrastructure, funding, and capacity for psychosocial care and outdated practices such as pro-institutionalization policies in some areas. Despite reforms and expanded insurance coverage, access remained limited, unequal, and often dependent on private services.
“... what happens in [country], especially in cities without academic services or emergency psychiatric units, is that people with FEP experience a longer duration of untreated psychosis, because they don’t have easy access to these facilities.” [Interview 8]
Participants also identified sociocultural factors which shaped local understandings of mental illness and help-seeking and care pathways, such as low mental health literacy, stigma, cultural beliefs like Aluxes (supernatural beings in Maya cosmology), and strong religious traditions such as Catholicism, Kardecist spiritism and African religions. Individuals or families often consulted shamans, priests, or healers before formal services.
“So many religions in [country] involve spiritual contact with dead people, so it’s not always easy to tell whether a patient’s symptoms are due to psychosis or are part of their cultural background. This can interfere people from seeking psychiatric help, as they may first consult a priest or a medium associated with these religions.” [Interview 17]
Many participants identified adverse social determinants disproportionately affecting youths in LAC, including poverty, violence, and the availability of drugs. Political instability in some countries further disrupted health policy coordination. Within these challenging contexts, families played central, complex roles, sometimes seeking institutionalization due to pessimism about recovery, but more often acting as recovery allies and advocates working with government and health institutions to support individuals with mental health conditions. In rural areas, family support, being in nature and working in the field (e.g., herding sheep) were identified as recovery-promoting.
“I tell you an anecdote about a young man who was in his final years of secondary school when he started to suffer from psychosis. The doctor’s message to the mother was: ‘Madam, take him out of school, don’t waste your money and your time’. She turned out to be a very brave mother and continued to seek treatment. Not only did she encourage him to continue in school, but she also encouraged the young man to enroll in university...This young man applied to law school, beating out a lot of people of his generation.” [Interview 5]
Preparation phase
In the preparation phase, local actors developed EIP initiatives in clinical services, universities, and/or public agencies, these settings shaping their focus and structure (Fig 3). Participants affiliated with health institutions created EIP programs that integrated clinical and research components; public agencies concentrated on developing policies; and university researchers led studies or contributed to guidelines. Except for public agencies developing policies, most relied on individual initiative and strong leadership, using strategies like engaging decision-makers and building institutional relationships.
Themes and subthemes identified regarding the Preparation phase of 26 EIP initiatives.In the preparation phase, the outer context described the setting in which the intervention was to be implemented, characterized by the absence of psychosis-specific programs, limited epidemiological data to inform intervention design, and low mental health literacy in the population. The inner context captured the mental health system, highlighting varying levels of knowledge and interest in psychosis among health professionals, as well as differing degrees of institutional support for intervention planning. The main bridging factor was the availability and use of foreign EIP manuals, which were used as models to prepare local initiatives. During this phase, planning and adaptation activities were undertaken to support the development of different types of initiatives.
“They told me that there were psychiatrists who might be interested in this subject and then they passed me the details of the director of the schizophrenia clinic, and I made an appointment with him and his team...They helped me a lot to open doors... So, you meet one person, he gets involved in the project, and then you get to know someone else.” [Interview 1]
Another key step was adapting EIP initiatives, as most were based on models from HICs, e.g., Australia or U.S.A., reflecting participants’ training, work experience, or institutional ties. A common strategy was to preserve core evidence-based components, use local resources, and align with public health priorities. For instance, one participant emphasized strengthening family interventions, as youths in their context often live with their parents well into adulthood, reflecting the value of familismo (family unity, obligation, and interconnection) common in LAC. Cultural adaptation was often considered but applied unevenly due to its complexity. Common adaptations were translating tools, involving traditional healers, and incorporating cultural activities.
“I don’t think people have a good definition of cultural adaptation. There are models, I know several, FRAME is one of them. ADAPT is another one that always includes that cultural element. But the cultural, I think is difficult, how to operate it….[Interview 2]
Participants described institutional support as generally positive, though seldom accompanied by additional resources. Several initiatives received backing from professional associations and universities. Some required collaboration with health authorities, usually the Ministry of Health, which was mostly a positive process, with some exceptions. Funding sources varied: clinical and government programs often used regular resources, while research-oriented initiatives relied on competitive grants. This was seen as challenging, requiring repeated applications to sustain activities.
“The initial program was based on research funds, with competitive research funds here in [country]. Until this year, science was done based on these competitive funds. From one of those research funds, this program was put together...because the clinic lent us the facilities, but the human resource to be able to evaluate and follow up these patients was what the funds mainly financed”. [Interview 9]
External factors also shaped the planning and design of EIP initiatives. In one country, EIP was backed by a clinical guideline for first-episode schizophrenia, and in a few others, clinical guidelines for psychosis included EIP, but most lacked formal policies. Participants noted the absence of dedicated services for early psychosis, making these initiatives pioneering efforts. Designing and integrating these programs was difficult due to scarce epidemiological data, low mental health literacy, and limited capacity or interest among non-mental health professionals. Several noted that EIP was a new concept even for most mental health staff.
“When the training was done, it was seen that this [EIP] was something relatively new, even for psychiatrists... I understand, at least when I graduated and was an undergraduate, I finished in 2018, I remember that there was no talk of a first psychotic episode as such until that date.” [Interview 3]
Preparatory actions included staff training, translating international research materials, and developing care protocols from HICs’ manuals. Policy initiatives often co-designed documents with user and family associations. Two initiatives had not been implemented at the time of interviews due to funding challenges, highlighting barriers to implementation.
“Yes, we presented it [EIP clinical program] to the hospital, presented it to the Ministry of Health, then to the [country] Society of Psychiatry. We even applied for a Canadian fund, but we didn’t manage to get funding. We applied to two international calls for proposals and were unable to move forward due to lack of financial resources.” [Interview 5]
Implementation phase
Participants described how EIP initiatives functioned in their settings, were received by users and providers, and the challenges faced (Fig 4). In the country with the clinical guideline for first-episode schizophrenia and strong primary care, the policy provided a strong foundation for further initiatives. Individual studies addressed specific goals but did not expand into broader research agendas. Clinical programs focused on care delivery, though they also engaged in research. Research programs initially prioritized scientific inquiry, but those in clinical settings often began offering care to address unmet needs. As a result, most programs combined care and research to varying extents.
*Themes and subthemes identified regarding the Implementation phase of 26 EIP initiatives.The outer context comprises two dimensions, separated by the dashed orange line: global context and national health system. In the implementation phase, EIP initiatives were operating within their respective settings. The outer context showed the organization of clinical and research initiatives into regional networks and indicated that, once operational, these initiatives benefited from external or industry funding for the development of research studies. The inner context illustrated how initiatives operated within mental health systems characterized by limited integration and reliance on staff undergoing training. The main bridging factor was the connection with other EIP initiatives for the development of multinational studies. In this phase, the intervention was well received by users, families, and health care providers, while its local coverage remained limited.
“We first initiated as a research program, so at the beginning we only had the assessments and the medical and then after the research assessments…[we began] to provide care, but we were all psychiatrists. So, I would say that things were evolving as patients were being enrolled in the research and we needed to provide some care for them.” [Interview 8]
Participants described perceiving that their clinical and research EIP initiatives were wellreceived by users and families, who trusted implementers’ clinical competence or institutional reputation. However, participants also perceived that initial enthusiasm sometimes declined, due to limited family involvement, unrealistic expectations for rapid recovery or rising comorbidity with substance use, which demanded more complex clinical management. While EIP models were generally accepted by mental health providers in these contexts, some resistance to innovation and the perception that there is no difference between FEP and chronic stages were reported. Despite challenges, initiatives were generally seen as important clinically and for building capacity. Research programs also enabled early detection and treatment of cases that might otherwise go missed.
“In our research, sometimes we did anti-psychotics for them. Sometimes we did antidepressants, sometimes we referred them to the psychologist for psychotherapy. Sometimes this was done for individual psychotherapy group therapy, and sometimes we just maintained surveillance on symptoms. So this was not structured, but was more on a as needed basis on an individual basis.” [Interview 6]
Across all initiatives, psychosocial interventions were deemed important but difficult to sustain due to resource and trained staffing shortages. Only one research program on psychosis epidemiology prioritized case identification over treatment but noted some psychosocial interventions offered within local services. Psychosocial interventions specialized for psychosis, including cognitive-behavioral therapy, were rarely available. Reflecting on constraints, one participant noted that they could deliver only half of what might be clinically recommended for psychosis.
“I think it [referring to fidelity scale for EIP] was developed by Donald Addington, and we realized half of what would be needed to be a first episode of psychosis proper program. But this is due to the lack of support...I think that we are not much better than we were at the beginning.” [Interview 8]
Participants described clinical and research initiatives as often disconnected from the broader health system. Private sector programs served small groups; public programs also had low coverage due to their stand-alone structure. In contrast, in the country with a clinical guideline for first-episode schizophrenia, the policy facilitated structured care through case notification, follow-up, and treatment. Programs in academic settings relied on researchers and trainees volunteering for core tasks like assessments and therapy, due to limited budgets.
“Depending on the resources that we had available, if we have someone, a psychologist, that would be a volunteer, then we could provide psychotherapy for [patients]. But so that’s why it’s hard for us to follow a specific model as we don’t have people really hired specifically for this.” [Interview 8]
The implementation phase revealed operational challenges. For CHR, these were under-resourced health systems, coordination challenges (e.g., limited referral pathways), and contextual factors like substance use complicating diagnosis. For FEP, defining onset was difficult when individuals arrived after long periods of untreated psychosis or unreliable antipsychotic use records. Some participants, therefore, preferred broader terms like “untreated psychosis” or “early-onset psychosis.” Retention of service users was also a challenge, with many disengaging after initial symptom improvement. Programs often provided non-protocolized care based on resources and individual needs.
“We registered this participant as a patient here at the [institution], and we started treating the participants and there was no standard, it was more like on an individual basis.” [Interview 8]
As clinical and research programs developed, some joined multicenter EIP studies, mainly contributing to participant recruitment, but gaining networks, research capacity, and funds. Some initiatives received industry support. One regional initiative was highlighted for unifying EIP efforts across LAC, setting regional research priorities and generating publications. Still, challenges included remaining focused solely on EIP, competing research priorities, and limited funding mechanisms.
“Research in Latin America exists, there are funds. There are places that obviously have a greater offering; people from Brazil with FAPESP have good support; in Chile, ANID works; for example, COLCIENCIAS in Colombia also works. The Mexicans also works since they have the CONACYT. The problem is that generally all these funds are for intra-country financing. So, there’s no way to harmonize projects together, and that’s where we fall.” [Interview 22]
Sustainability phase
EIP initiatives followed various sustainability trajectories revealing implementation challenges in LAC (Fig 5). The COVID-19 pandemic influenced both their development and long-term viability. A clinical program was discontinued due to administrative disruptions and service reorganization; another due to difficulties in identifying and retaining service users, both exacerbated by the pandemic.
*Themes and subthemes identified regarding the Sustainability phase of 26 EIP initiatives.The outer context comprises two dimensions, separated by the dashed orange line: global context and national health system. In the sustainability phase, the outer context reflected ongoing pressure on initiatives to secure additional funding in order to remain operational, often in competition with other mental health priorities. In the inner context, the need to build psychosis-related capacity among health workers was highlighted, particularly the strengthening of EIP-specific skills within the mental health workforce. As bridging factors, the figure emphasizes the continued need for, and dependence on, external funding and resources among initiatives that were initially supported through these mechanisms. Across settings, EIP initiatives followed divergent paths: some scaled up, whereas others were discontinued due to external factors, such as the COVID-19 pandemic or insufficient funding.
[CHR program] around 2022, we closed it because we didn’t have so many volunteers. We didn’t have so many patients. And we decided then to focus on the first-episode program.” [Interview 8]
At the time of the interviews, sustained initiatives included two clinical guidelines, eight clinical programs, and four research programs. The guideline in the strong primary care-based country was seen as essential for enabling and sustaining EIP-related initiatives, whereas a similar guideline was deemed unfeasible in another country due to limited resources and staffing. This contrast underscores that policy, without proper resource allocation, has limited impact. Some initiatives remained fragile with unstable funding and staff shortages. Others had benefited from institutional support and recognition (e.g., one initiative had been in place for 25 years), and had expanded regionally or used research to inform national policies. Both vulnerable and consolidated initiatives continuously sought resources.
“Funding is already gone, and we are looking for more funding. And the idea would be to, let’s say, scale the screening process and make it a good cost benefit about screening process. This is one of the main goals, so that it turns sustainable.”[Interview 6]
Large EIP research projects in LAC depended on international funding. One persisted but faced uncertain system integration once funding ended; another’s continuation depended on new international funding; as local resources were insufficient for large-scale research. The one regional research initiative had depended on international funding, as national grants were typically limited to country-specific projects. It continued through strong regional collaboration despite the loss of funding.
“Although we currently do not have funding, we maintain a collaboration. That is, we always have collaborations in Latin America with contacts and knowing that we can also apply for things together. So, we are applying with different countries; now more have joined us... we are going to do something with Uruguayans and Argentineans, without money, less resources, but we are able to keep the network alive.” [Interview 22]
Participants emphasized the need for sustained health sector action to support EIP initiatives, including reducing stigma; enhancing EIP training in academic programs; and improving mental health workers’ knowledge of psychosis and competencies to integrate care into non-specialized settings. As EIP remains novel, participants recommended raising visibility through media, conferences, and policy-/decision-maker engagement.
“Academia needs to be closer to those who are the public mental health organize the system. So I think academia needs to go outside the walls and try to influence mental health policies. Not only the training, because if we have the training, but we don’t have the service and we don’t have a protocol, but it’s adopted the whole country, we’ll do the same.” [Interview 8]
Participants valued EIP but held concerns about its nationwide expansion, particularly of HIC-like stand-alone clinical services, given their perceived high costs and implementation challenges in contexts with widely unmet mental health needs and limited services. They also justified this given the lack of guidance on implementing EIP in complex LAC contexts.
“The difficult part is sometimes being able to implement it, right? I mean, I think that, in theory, we know that we have to treat it early and provide the best possible treatment. What is complicated, and perhaps not so clear to me, is how we are going to implement it across the country. But I would think that the will, at least theoretically, exists.” [Interview 13]
Alternative approaches to scaling EIP
As nationwide implementation of existing EIP programs was considered unfeasible in LAC, participants proposed context-responsive dissemination models. Some suggested reserving CHR models for research, given limited resources and the need to prioritize FEP care.
“Perhaps the best position of the CHR model for LMIC is to focus on research fundamentally, but it’s not possible in terms of wide implementation. It’s not so cost effective to implement this kind of model across a country because there are other conditions that require also attention.”[Interview 17]
Strengthening existing primary care or youth mental health services was proposed as a platform for identifying, managing, or referring CHR cases, as these are already integrated into national systems and better positioned for early detection.
“I think it would be important to involve other institutions that work on mental health issues, which are not third level...that treat patients already with a diagnosis...for example, like a service that was implemented a few years ago, which is a hospital of emotions and treats young people, adolescents, and young adults. So they offer psychological services and I think that working with them would be a very good option.” [Interview 1]
Several participants recommended implementing FEP clinical programs in tertiary care settings, specialized institutions, or hospitals in major cities where services already exist, while also promoting early intervention in regional areas with limited services and trained staff.
“I think they can be done in all the major Latin American capitals, yes. I think they should and can be done. But also balancing it with the fact that in the regional cities there is a clear lack of psychiatrists, lack of development of services and awareness. So, it is not really feasible to be able to make an early intervention service that is more extensive, but probably rather to raise awareness of the issue and try to make an early recognition, a relatively benign intervention in more general services.” [Interview 22]
Others proposed developing EIP protocols or care standards to guide service delivery across system levels, and staff training for implementation and sustainability.
“I would say that the two needs is to organize first episode protocol in the health system, [country name], using the existing network, and also to organize better the psychiatric emergency services in the country.” [Interview 8]
Some recommended innovative delivery strategies, like taskshifting and simplified care packages, reflecting concerns about the feasibility of resource-intensive HIC models in low-resource settings.
“We would have to think of a compact version of that without losing the principles. If we cannot include interventions to prevent suicide or cognitive remediation. We can include other types of cheaper, more flexible interventions, which can be taskshifting, which can be provided here and which people have experience [with].” [Interview 2]
Discussion
Our findings highlight the contextual realities, structural barriers, and adaptive strategies shaping EIP initiatives across different implementation phases and levels of the social ecology in LAC. The EIP paradigm in LAC has been translated into diverse initiatives, largely driven by individual motivation, modelled after foreign programs, and constrained by local resources. While participants valued EIP, they cautioned against stand-alone EIP programs in LAC due to limited resources, instead proposing contextually grounded, resource-sensitive alternatives to ensure feasibility and effective scaling across LAC.
Toward a broader approach to EIP in LMICs
It is well established that replicating models developed in HICs is often unfeasible in LMICs [25,47]. Some have proposed implementing only the “key ingredients” of these interventions [25]. However, this assumes clearly defined core components that work across contexts, an assumption that is insufficiently defined. This one-dimensional framing also overlooks the potential of alternative strategies in LAC and may partly explain the stagnation of EIP implementation in many LMICs. Our findings underscore the value of diverse initiatives, whether standardizing practices, prioritizing specific populations, or addressing varied needs, thus calling for a more flexible conceptualization of EIP to advance it.
Beyond implementing programs, LMICs must foster complementary structures to enhance psychosis care. Unlike in HICs, guidelines, technical standards, and research [16,48,49] are largely absent in most LMICs [47]. Consequently, there is often no robust legal, educational, or evidence-based foundation to support the implementation of EIP programs in these settings. These structures are essential to support broader engagement in and sustainability of EIP, by leveraging local strengths such as strong primary care systems, community networks, and advocacy groups.
Context shaping EIP initiatives
Our results suggest that EIP programs in LAC have been shaped by the same structural conditions and resource limitations that define mental health care more generally in LMICs: low policy and funding priority, scarce or fragile funding, and reliance on individual initiatives or external support. This is unlike HICs, like the U.K. Australia, Denmark, Singapore, and Canada [11,50–53], where strong political and financial commitment enabled widespread implementation and sustainability of EIP. These differences highlight the extent to which structural and funding contexts influence the organization and delivery of EIP services.
The provision of psychosocial interventions in LMICs is recognized as highly challenging due to limited resources [54,55]. EIP services in most LAC countries faced similar barriers. Although policies often stated that psychosocial care should be available nationwide, participants acknowledged that broader implementation was unfeasible due to a shortage of trained human resources or because services were concentrated in tertiary care. Although no formal fidelity evaluations were reported, care was generally described as non-protocolized and only partially aligned with international recommendations as well as local aspirations and needs. The challenges to meet alignment with international recommendations, as well as the non-protocolized nature of care, reflect structural constraints. Even in HICs, EIP programs struggle with aligning with standards. Furthermore, there is a need for context-sensitive guidelines and fidelity scales [56]. The lack of alignment with local aspirations and needs reflects both the barriers implementers faced in implementing EIP services as desired, as well as the limited systematic exploration and integration of local service users’ and families’ needs and preferences in designing EIP services.
International influences
Most EIP initiatives were conceptualized on foreign models, aided by guidelines, implementation manuals, and connections with implementers from HICs. This externally driven approach may have introduced a desire to emulate foreign practices and a missed opportunity to fundamentally incorporate contextual knowledge and culturally relevant practices. Systematic cultural and content adaptation was not formally pursued in any initiative. Only public policies showed some degree of co-design with service users. Instead, adaptations emerged pragmatically, based on implementers’ experience and resources, a process also reported in other LMICs [57].
Interestingly, in the cases with formal North–South collaboration and external funding, there was an emphasis on capacity building and cultural sensitivity. In one case, the international funder required that institutional leadership be established in the South. In another, the funding call requested the inclusion of culturally sensitive practices and local stakeholders. While such actions by funders should continue [58], they come with a risk of tokenistic practices [59]. Dependence on foreign funding may also discourage local investment; and external funds can be abruptly withdrawn due to shifting political or institutional priorities. Future efforts must therefore centre LMIC agency and leadership in EIP [14].
Perspectives on scaling EIP
This study has important implications for EIP implementation in LAC. In fragmented, under-resourced, urban-centered mental health systems, participants viewed scaling traditional EIP clinical program models as largely unfeasible and difficult to replicate from HICs. They called instead for flexible, context-specific strategies that integrate EIP into national agendas and align with existing capacities, while addressing structural inequities, strengthening the workforce, and promoting mental health literacy to reduce stigma and improve understanding of psychosis.
Participants’ proposals for dissemination of EIP were experienced-informed and appear feasible within low-resource environments, and could be structured to inform resource allocation, policy, and workforce training. Strategies, such as task sharing and task shifting, have already been successful in scaling mental health interventions in LMICs [60,61]. Regardless of the initiatives implemented, psychosis care must be included in universal health coverage frameworks to ensure that the population has access to services and financial protection against associated costs. The experience of LMICs like China and Brazil suggests that this measure can improve outcomes and reduce care gaps [62]. Future EIP implementation must be centered more strongly on the voices of people with lived experience and families, which is currently missing despite such involvement being a rights-based imperative that can enhance uptake, innovation, and advocacy [63].
Limitations and strengths
This study focused on implementers’ perspectives. For example, the acceptability of the intervention among service users and their families was assessed from implementers’ perspectives, which represents a limitation. Had we included service users, we may have gathered insights about the acceptability of and experiences with EIP from the perspective of diverse service users and families, and how these may have been shaped by explanatory models, trust, systemic, and logistical barriers (e.g., costs), stigma, etc. Future work should integrate the perspectives of services users and families. Second, the implementers were predominantly men, which may have shaped findings around gendered influences on needs and pathways, and implementation pathways. Female implementers may have arguably been more attuned to identifying gendered barriers to implementation in institutional contexts where positions of authority remain male-dominated and in historically patriarchal social contexts. They might have been more attuned to how gendered experiences and roles influence needs, service engagement and stigma (e.g., better services for post-partum psychosis in early intervention, etc.). Third, some initiatives may have been overlooked, particularly of countries with low research capacity, although a wide definition for EIP initiatives and multiple identification strategies were used. Finally, by examining only EIP actors, other approaches to addressing psychosis and mental illness in LAC may have been missed, some of which may be more locally grounded and more scalable on their own or as elements of EIP, for example, informal, community or peer-led organizations caring for persons with mental illnesses. Despite these limitations, the richness and consistency of data across countries strengthen the credibility of our findings. This is the first qualitative study to comprehensively examine EIP implementation across multiple countries in LAC, covering 26 initiatives across 10 countries, providing a comprehensive regional perspective. It also captured the evolving nature of EIP in the region. For example, a technical standard moved from draft to rollout during the study. Triangulation and member checking enhanced the trustworthiness of the findings.
Implementation science remains limited in EIP and more generally in LMICs. Guided by the EPIS framework, our study thus makes important methodological and substantive contributions. Still, it did not fully capture factors such as supernatural explanations of psychosis, poverty, and other social determinants. We suggest viewing implementation science frameworks as adaptable tools, echoing previous calls to add domains like resource constraints and system characteristics in LMIC implementation studies [57].
This study shows how the EIP paradigm has been translated into diverse, locally adapted initiatives across LAC, despite constraints, limited funding, and uneven political support. Some achieved progress and others struggled with sustainability. Findings underscore the need to move beyond replicating HIC models toward a broader range of initiatives aligned with local priorities and capacities. Implementers’ proposals—integrating EIP into youth mental health and primary care, promoting taskshifting, simplified care packages and early psychosis literacy—offer feasible strategies for scaling early psychosis care in resource-limited settings.
Supporting information
S1 TableStandards for Reporting Qualitative Research.(DOCX)
S1 TextInterview guide.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Gorry P. Early psychosis prevention and intervention centre. Australas Psychiatry. 1993;1(1):32–4. doi: 10.3109/10398569309081303 21275861 · doi ↗ · pubmed ↗
- 2Mc Gorry PD, Killackey E, Yung A. Early intervention in psychosis: concepts, evidence and future directions. World Psychiatry. 2008;7(3):148–56. doi: 10.1002/j.2051-5545.2008.tb 00182.x 18836582 PMC 2559918 · doi ↗ · pubmed ↗
- 3Mc Gorry PD. Early intervention in psychosis: obvious, effective, overdue. J Nerv Ment Dis. 2015;203(5):310–8. doi: 10.1097/NMD.0000000000000284 25919380 PMC 4414340 · doi ↗ · pubmed ↗
- 4Petersen L, Jeppesen P, Thorup A, Abel M-B, Øhlenschlaeger J, Christensen TØ, et al. A randomised multicentre trial of integrated versus standard treatment for patients with a first episode of psychotic illness. BMJ. 2005;331(7517):602. doi: 10.1136/bmj.38565.415000.E 01 16141449 PMC 1215551 · doi ↗ · pubmed ↗
- 5Craig TKJ, Garety P, Power P, Rahaman N, Colbert S, Fornells-Ambrojo M, et al. The Lambeth Early Onset (LEO) Team: randomised controlled trial of the effectiveness of specialised care for early psychosis. BMJ. 2004;329(7474):1067. doi: 10.1136/bmj.38246.594873.7C 15485934 PMC 526115 · doi ↗ · pubmed ↗
- 6Correll CU, Galling B, Pawar A, Krivko A, Bonetto C, Ruggeri M, et al. Comparison of Early Intervention Services vs Treatment as Usual for Early-Phase Psychosis: A Systematic Review, Meta-analysis, and Meta-regression. JAMA Psychiatry. 2018;75(6):555–65. doi: 10.1001/jamapsychiatry.2018.0623 29800949 PMC 6137532 · doi ↗ · pubmed ↗
- 7Puntis S, Minichino A, De Crescenzo F, Cipriani A, Lennox B, Harrison R. Specialised early intervention teams for recent-onset psychosis. Cochrane Database Syst Rev. 2020;11(11):CD 013288. doi: 10.1002/14651858.CD 013288.pub 2 33135811 PMC 8092671 · doi ↗ · pubmed ↗
- 8Rosenheck R, Leslie D, Sint K, Lin H, Robinson DG, Schooler NR, et al. Cost-Effectiveness of Comprehensive, Integrated Care for First Episode Psychosis in the NIMH RAISE Early Treatment Program. Schizophr Bull. 2016;42(4):896–906. doi: 10.1093/schbul/sbv 224 26834024 PMC 4903057 · doi ↗ · pubmed ↗