Functional Convergence Spasm and Dysconjugate Eye Movements: A Vignette
Iryna Klopotovska, Koemi‐Jade Garrick, Diego Kaski

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
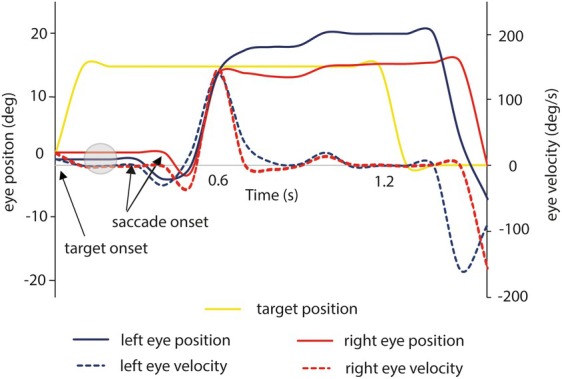 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOphthalmology and Eye Disorders · Vestibular and auditory disorders · Botulinum Toxin and Related Neurological Disorders
A 46‐year‐old woman presented with a 3‐month history of intermittent diplopia, blurred vision, and unsteadiness, following a sudden episode of disorientation and collapse while supervising an examination. After this collapse, she developed increased sound sensitivity and worsening motion sickness. She had no prior medical history or regular medications. Her family history included multiple sclerosis and brain tumor. Examination was limited due to visual discomfort. Eye movements were full, with no spontaneous or gaze‐evoked nystagmus, but were often dysconjugate, showing brief paroxysms of convergent effort—especially during saccades and pursuit—accompanied by pupillary constriction (see Video 1). Vestibulo‐ocular reflex (VOR) was intact. Dix‐Hallpike and roll test elicited no nystagmus, though convergence effort occurred intermittently. Gait was broad‐based and cautious, with prolonged single‐leg stance time. She took multiple steps on the pull test and had a positive shoulder tap sign. Based on the above, a diagnosis of functional gait disorder and functional convergence spasm with dysconjugate eye movements was made. Magnetic resonance imaging (MRI) was normal. The patient was educated on the diagnosis and referred to physiotherapy and ocular motor rehabilitation.
Conjugate horizontal saccades rely on a brainstem circuit involving burst neurons in the paramedian pontine reticular formation (PPRF), normally inhibited by omnipause neurons in the nucleus raphe interpositus. When omnipause neurons stop firing, burst neurons activate the abducens nucleus, stimulating the ipsilateral lateral rectus and contralateral medial rectus via internuclear neurons through the medial longitudinal fasciculus (MLF), enabling conjugate movement.1 Despite near‐perfect coordination, slight physiological dysconjugacies can occur. Early differences (within 5 ms) may reflect internuclear transmission delay, whereas later‐phase disparities often relate to biomechanical factors like greater peak velocity in the abducting eye.1
Functional convergence spasm (CS) is a functional eye movement disorder characterized by involuntary convergence, accommodation, and miosis without a near stimulus. It is the most frequently reported functional ocular motor abnormality.2 Pupillary constriction, as shown in our patient, is a key feature suggesting accommodative effort rather than a deficit.3 CS may be triggered during sustained gaze, as demonstrated in Video 1. Other neurological causes of convergence spasm are rare and include lesions in the diencephalic–mesencephalic junction (eg, thalamic esotropia), Wernicke‐Korsakoff syndrome, and posterior fossa pathology.4
In our patient, videonystagmography (VNG) revealed dysconjugate movements unrelated to visual stimuli, often mistaken for abducens palsy or internuclear ophthalmoplegia (INO). Our patient demonstrated variability in excessive abduction (convergence spasm) affecting either eye, consistent with the variability reported in functional movement disorders (Fig. 1). Management focuses on patient education, reassurance, and structured rehabilitation (that may include eye movement retraining), with cognitive behavioral therapy or psychological support when necessary. The use of mydriatics has been suggested for convergence spasm, but there is very limited evidence to support their use,5 and anecdotally, we have not had success with these.
Author Roles
(1) Research project: A. Conception, B. Organization, C. Execution; (2) Statistical analysis: A. Design, B. Execution, C. Review and critique; (3) Manuscript: A. Writing of the first draft, B. Review and critique.
I.K.: 1B, 1C, 3A
K.J.G.: 1B, 1C
D.K.: 1A, 1B, 1C, 1B, 3B
Disclosures
Ethical Compliance Statement: The authors confirm that approval of an institutional review board was not required for this work. The patient provided written consent for eye recordings using videonystamography. We confirm that we have read the journal's position on issues involved in ethical publication and affirm that this work is consistent with those guidelines.
Funding Sources and Conflicts of Interest: No specific funding was received for this work. The authors declare that there are no conflicts of interest relevant to this work.
Financial Disclosures for the Previous 12 Months: I.K. is supported by a Clinical Fellowship grant from the European Academy of Neurology. D.K. is supported by the National Institute for Health Research University College London Hospitals Biomedical Research Centre.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Serra A , Liao K , Matta M , Leigh RJ . Diagnosing disconjugate eye movements: phase‐plane analysis of horizontal saccades. Neurology 2008;71(15):1167–1175. 10.1212/01.wnl.0000327525.72168.57 PMID: 18838664; PMCID: PMC 2586990.18838664 PMC 2586990 · doi ↗ · pubmed ↗
- 2Fekete R , Baizabal‐Carvallo JF , Ha AD , Davidson A , Jankovic J . Convergence spasm in conversion disorders: prevalence in psychogenic and other movement disorders compared with controls. J Neurol Neurosurg Psychiatry 2012;83(2):202–204. 10.1136/jnnp-2011-300,733 Epub 2011 Sep 23. PMID: 21949106.21949106 · doi ↗ · pubmed ↗
- 3Kaski D , Pradhan V , Bronstein AM . Clinical features of functional (psychogenic) eye movement disorders. J Neurol Neurosurg Psychiatry 2016;87(12):1389–1392. 10.1136/jnnp-2016-313,608 Epub 2016 Sep 28. PMID: 27683918.27683918 · doi ↗ · pubmed ↗
- 4Kaski D , Bronstein AM , Edwards MJ , Stone J . Cranial functional (psychogenic) movement disorders. Lancet Neurol 2015;14(12):1196–1205. 10.1016/S 1474-4422(15)00226-4 PMID: 26581970.26581970 · doi ↗ · pubmed ↗
- 5Teodoro T , Cunha JM , Abreu LF , Yogarajah M , Edwards MJ . Abnormal eye and cranial movements triggered by examination in people with functional neurological disorder. Neuro‐Ophthalmol 2018;43(4):240–243. 10.1080/01658107.2018.1536998.PMC 673612731528188 · doi ↗ · pubmed ↗