Asymmetric Parietal Cortical Atrophy in a Patient with RAB39B ‐Associated Parkinsonism
Luca Gallo, Emna Ben Mansour, Silvia Nicolosi, Anna Pichiecchio, Simone Gana, Samia Ben Sassi, Silvano Cristina, Micol Avenali, Enza Maria Valente

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
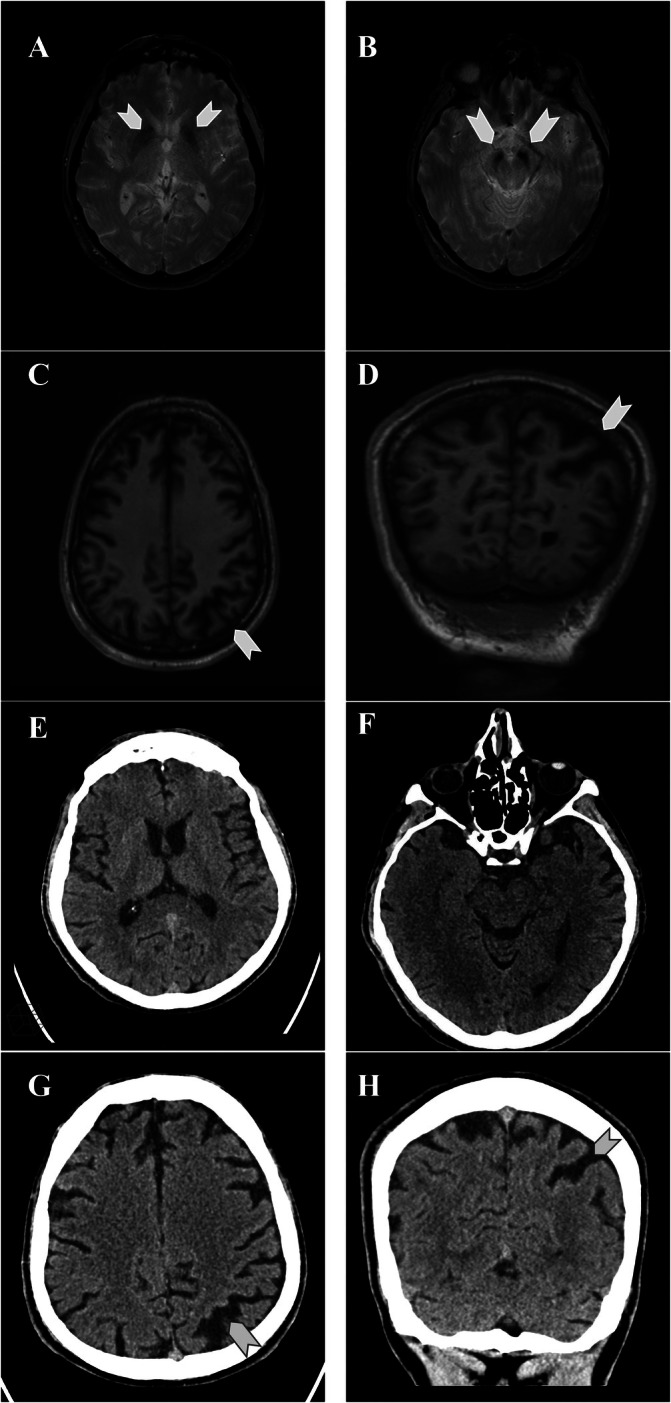 FIG 1
FIG 1| Reference | Patients | Brain MRI | Brain CT scan |
|---|---|---|---|
| Giannandrea et al | II‐3 (M, 52y), III‐3 (M, 13y) | Both: normal | ‐ |
| Vanmarsenille et al11 |
II.1 (M,6.5) AV1, (M, 22y), KM1 (M, 6.5y) | All: normal | ‐ |
| Wilson et al12 | II:1 (M, adult age) | Mild hypointensity of SN (T2) | ‐ |
| II:2 (M, adult age) | Normal | ‐ | |
| El‐Hattab et al13 | Family 4 (M, 12y), Family 6 (F, 11y), Family 7 (F, 0.25y) | All: normal | ‐ |
| Lesage et al14 | M, 39y | Normal (repeated twice) | ‐ |
| Güldner et al15 | M, 42y | Hypointensity of SN and BG (T2*) | ‐ |
| Shi et al16 | II‐2 (M, 58y), III‐1 (M, 20y) | Both: hypointensity of bilateral GP (SWI) | Calcifications of BG |
| Ciammola et al17 | Family 1, II‐3 (M, 67y) | Hypointensity of SN and GP, milder hypointensity of red nuclei, putamen, and pulvinar (GRE, SWI) | Moderate calcifications of GP |
| Family 1, II‐1 (M, adult age) | ‐ | Moderate calcifications of GP | |
| Family 2, IV‐2 (M, 49y) | Hypointensity of SN and GP, milder hypointensity of red nuclei, putamen, and pulvinar (GRE, SWI) | No calcifications | |
| Ballout et al18 | Case 3 (F, 2y) | Normal | ‐ |
| Santoro et al19 | M, 4y | Hyperintensity of hippocampi and temporomesial regions (FLAIR); hyperintensity of BG (T2); hyperintensity of periventricular regions due to respiratory distress at birth (T2) | ‐ |
| Mackels et al20 | M, 37y | Inferior vermian hypoplasia, corpus callosum dysgenesis (T1, FLAIR); hypointensity of GP and SN (T2*W‐GRE) | Calcifications of caudate nuclei, subtle calcifications of the GP |
| Jacobson et al21 | F, 41y | Normal | ‐ |
| Dayan et al22 | III‐7 (M, 46y) | Normal | No calcifications |
| III‐10 (M, 47y) | Normal | Small calcifications of BG | |
| Geoffre et al | M, 49y | Hypointensity of GP, SN and dentate nuclei; mild frontal atrophy (FLAIR, SWI) | ‐ |
| F, 52y | Normal | ‐ | |
| Present case | M, 57y | Hypointensity of GP and SN (T2*); diffuse cortical atrophy (T1) | Cortical atrophy, no calcifications |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParkinson's Disease Mechanisms and Treatments · Neurological disorders and treatments · Alzheimer's disease research and treatments
The RAB39B (Ras Analogue in Brain 39b) gene on the X chromosome encodes for a small GTPase protein involved in intracellular trafficking and mainly expressed in the central nervous system.1
Loss‐of‐function variants of RAB39B cause early‐onset parkinsonism with intellectual disability, predominantly in males.2 To date, 78 patients have been described, harboring 26 distinct variants3 (supplementary references). The imaging phenotype associated to this genetic condition has not been characterized in detail. We report a novel RAB39B pathogenic variant in a patient with late‐onset parkinsonism, paramagnetic deposits in the basal ganglia and left‐predominant parietal cortical atrophy.
Case Report
The patient is a 57‐year‐old Caucasian male, born from unrelated parents, with three maternal uncles presenting intellectual disability, of whom one also with parkinsonism. Comorbidities include diabetes mellitus type 2 and systemic hypertension.
He had mild social skill impairment since childhood but completed secondary school. Parkinsonian symptoms appeared at age 50 years, with subtle resting tremor in the right upper limb and camptocormia. DAT‐SCAN showed bilateral reduced uptake in the right putamen/caudate nucleus. After 2 years, levodopa therapy was started (LEDD 300 mg), with good motor control.
We first evaluated the patient at age 52 years. Physical and neurological examination revealed mild craniofacial dysmorphisms (long and narrow face, large ears and broad forehead), resting, postural and kinetic tremor only on the right side, slight bradykinesia and ipsilateral reduced arm swing (Video 1). Neurocognitive evaluation revealed mild intellectual disability (IQ 53). Brain MRI at age 52 years showed bilateral paramagnetic deposits in the substantia nigra and basal ganglia, along with diffuse cortical atrophy predominantly involving the parietal lobes, with marked left‐sided asymmetry.
First neurological assessment. In this video, we can see the patient at his first neurological evaluation, at age 52 years. Mild resting tremor in the right hand can be observed, which is more pronounced during walking. There is also mild bradykinesia in the right side.
NGS‐based genetic analysis of a virtual panel of 68 genes related to parkinsonism identified a novel hemizygous truncating variant in RAB39B (NM_171998.4): c.202C>T; p.(Gln68*).
Motor symptoms slowly worsened, with tremor becoming bilateral, and the patient progressively developed autonomic symptoms, mood disorders, dysphagia, pain, and sleep disturbances. At age 57 years, motor fluctuations occurred, with disabling tremor‐akinetic off periods, occasionally associated with freezing of gait (Video 2). LEDD was increased with limited motor benefit. The cognitive profile remained stable (Supplementary Table S1). A second brain MRI showed unmodified paramagnetic deposits and cortical atrophy. A concurrent CT scan excluded cerebral calcifications (Figure 1).
Neurological evaluation after 5 years, at age 57 years. The disease showed marked progression, with severely disabling tremor and worsening bradykinesia impairing agility tests. the patient still walks unassisted, with a positive pull test and preserved recovery. The patient is still able to walk without support. Pull test is positive with recovery.
Brain MRI and CT of the patient at 57 years. Axial‐gradient‐recalled‐echo‐T2‐weighted images demonstrate bilateral hypointensities in the substantia nigra (A) and globi pallidi (B), likely related to paramagnetic deposits. 3D‐T1‐weighted axial reconstruction (C) shows diffuse cortical atrophy mostly prevalent in the parietal regions. Parietal atrophy is also evident in the coronal section (D). SWI (susceptibility Weighted Imaging) sequence could not be obtained due to motion artifacts. Axial CT brain scan shows absence of calcifications in the basal ganglia (E) and substantia nigra (F). Cortical atrophy is visible on axial (G) and coronal reconstruction images (H).*
Discussion
Here we report a novel RAB39B truncating variant in a male presenting with mild intellectual disability, late‐onset parkinsonism and brain imaging abnormalities. The typical RAB39B‐associated phenotype features infantile‐onset non‐progressive intellectual disability associated with parkinsonism;2 epilepsy, autism spectrum traits and craniofacial dysmorphism can also occur.4, 5, 6 Parkinsonian signs usually manifest early (mostly in the third decade), yet the spectrum of ages at onset is broad and few cases have been reported with adult onset.3
The neuroimaging phenotype of RAB39B‐related parkinsonism has been described only in 26 patients, with heterogeneous outcome (Table 1). In 14 patients, brain MRI was reported as normal. However, this finding should be interpreted with caution, as several individuals underwent imaging in the first or second decade of life, when alterations may not have developed yet. Furthermore, all but one negative case did not undergo a CT scan, thus the presence of subtle calcifications cannot be ruled out with certainty. Six patients had basal ganglia calcifications which were demonstrated by CT scan, and confirmed in many cases by the detection of hypointense signal at MRI sequences sensitive to paramagnetic and diamagnetic compounds, such as SWI (Susceptibility Weighted Imaging) and T2 GRE (Gradient‐Recalled Echo). Similar hypointensities of the basal ganglia and, often, of the substantia nigra were reported in a further six patients, using a range of MRI sequences with variable sensitivity in detecting paramagnetic and diamagnetic compounds. Interestingly, in two of these patients, including the one reported here, CT scan excluded the presence of brain calcifications, suggesting that the observed hypointensities could result from deposition of paramagnetic compounds such as iron. The underlying pathology still remains uncertain in the other four cases.
Only two patients showed mild cortical atrophy, which was limited to the frontal region in one male patient,7 while it was diffuse with predominance in the left parietal lobe in our case. Follow‐up imaging after 5 years demonstrated that the asymmetric cortical atrophy remained stable, suggesting a developmental origin rather than a neurodegenerative process. This hypothesis is supported by the role of RAB39B in neuronal development, as the gene is highly expressed in the cortex, thalamus, basal ganglia and substantia nigra2, 8, 9 and its protein product is implicated in neurite and synapse formation.4, 10
While iron accumulation and cortical atrophy can occur in other neurodegenerative disorders—such as Neurodegeneration with Brain Iron Accumulation and tauopathies—the clinical presentation and progression in RAB39B‐related parkinsonism are clearly distinct, allowing for differential diagnosis.
A detailed assessment of brain imaging in a larger number of patients is needed to better define the spectrum and underlying pathology of brain defects in RAB39B‐associated parkinsonism.
Author Roles
(1) Research project: A. Conception, B. Organization, C. Execution; (2) Statistical Analysis: A. Design, B. Execution, C. Review and Critique; (3) Manuscript: A. Writing of the first draft, B. Review and Critique.
L.G., E.B.: 1A, 1B, 1C, 3A.
S.N.: 1C, 3B.
A.P., S.G., S.B., S.C.: 1A, 3B.
M.A.: 1A, 1B, 1C, 3B.
E.M.V.: 1A, 1B, 3B.
Disclosures
Ethical Compliance Statement: Patient informed consent was obtained for this work. The approval of an institutional review board was not required. We confirm that we have read the Journal's position on issues involved in ethical publication and affirm that this work is consistent with those guidelines.
Funding Sources and Conflict of Interest: The authors report no sources of funding or conflicts of interest with regards to the present topic.
Financial Disclosures for the previous 12 months: MA has received consulting fees or speaking honoraria from Bial, and research grants from Italian Ministry of Health. EMV has received research grants from the Italian Ministry of Health, Telethon Foundation and CARIPLO Foundation. The remaining authors declare that no sources of funding and no conflicts of interest.
Supporting information
Data S1. Supporting Information.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cheng H , Ma Y , Ni X , et al. Isolation and characterization of a human novel RAB (RAB 39B) gene. Cytogenet Genome Res 2002;97:72–75. 10.1159/000064047.12438742 · doi ↗ · pubmed ↗
- 2Gao Y , Martínez‐Cerdeño V , Hogan KJ , Mc Lean CA , Lockhart PJ . Clinical and neuropathological features associated with loss of RAB 39B. Mov Disord 2020;35:687–693. 10.1002/mds.27951.31951675 · doi ↗ · pubmed ↗
- 3Tang BL . RAB 39B's role in membrane traffic, autophagy, and associated neuropathology. J Cell Physiol 2021;236:1579–1592. 10.1002/jcp.29962.32761840 · doi ↗ · pubmed ↗
- 4Koss DJ , Campesan S , Giorgini F , Outeiro TF . Dysfunction of RAB 39B‐mediated vesicular trafficking in Lewy body diseases. Mov Disord 2021;36:1744–1758. 10.1002/mds.28605.33939203 · doi ↗ · pubmed ↗
- 5Mignogna ML , Ficarella R , Gelmini S , et al. Clinical characterization of a novel RAB 39B nonstop mutation in a family with ASD and severe ID causing RAB 39B downregulation and study of a Rab 39b knockdown mouse model. Hum Mol Genet 2022;31:1389–1406. 10.1093/hmg/ddab 320.34761259 PMC 9071400 · doi ↗ · pubmed ↗
- 6Giannandrea M , Bianchi V , Mignogna ML , et al. Mutations in the small GT Pase gene RAB 39B are responsible for X‐linked mental retardation associated with autism, epilepsy, and macrocephaly. Am J Hum Genet 2010;86(2):185–195. 10.1016/j.ajhg.2010.01.011.20159109 PMC 2820185 · doi ↗ · pubmed ↗
- 7Geoffre N , Jaulent P , Laurencin C , et al. Two case reports of RAB 39B deletion displaying highly variable parkinsonism. Parkinsonism Relat Disord 2025;135:107824. 10.1016/j.parkreldis.2025.107824.40245817 · doi ↗ · pubmed ↗
- 8Gao Y , Wilson GR , Stephenson SEM , et al. Distribution of Parkinson's disease associated RAB 39B in mouse brain tissue. Mol Brain 2020;13:52. 10.1186/s 13041-020-00584-7.32228644 PMC 7106796 · doi ↗ · pubmed ↗