GPi‐DBS for SERAC1 ‐Related Dystonia‐Parkinsonism
Vidal Yahya, Alessandro Di Maio, Mauro Treddenti, Ludovica Tundo, Giulia Scacciatella, Costanza Masetti, Marta Pengo, Chiara Casellato, Desiree Lattanzi, Marcello Egidi, Sara Marceglia, Tommaso Bocci, Alberto Priori, Gaia Oggioni

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
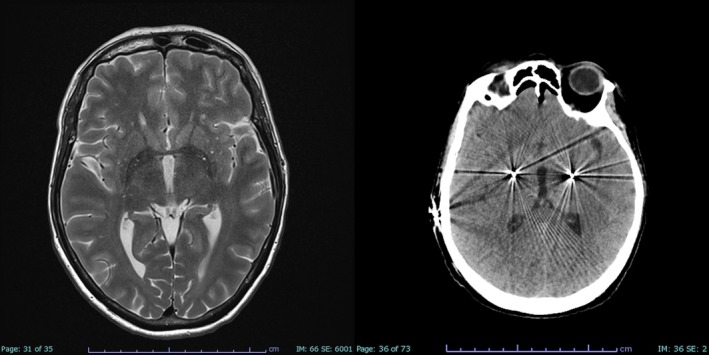 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurological disorders and treatments · Genetic Neurodegenerative Diseases · Parkinson's Disease Mechanisms and Treatments
Globus pallidus internus deep brain stimulation (GPi‐DBS) is an effective treatment for dystonia. Yet, the outcome of GPi‐DBS is variable in monogenic dystonia: optimal responses are commonly reported for DYT‐TOR1A and ‐SGCE, a significant benefit is also recognized for DYT‐GNAL, ‐KMT2B, ‐PANK2, ‐TAF1, and ‐THAP1, while the effect of GPi‐DBS remains uncertain for rarer forms.1, 2, 3
In this context, dystonia associated with monogenic mitochondriopathies constitutes a challenging field characterized by significant genetic heterogeneity and complex clinical pictures.4 GPi‐DBS implantation is approached very carefully in this cohort for several reasons: basal ganglia, including GPi, are particularly susceptible to mitochondrial dysfunction5; systemic disturbances classically associated with mitochondrial diseases may interfere with neuroimaging and surgery (eg, cochlear implants for sensorineural deafness); intellectual disability or young age often contraindicate awake surgery; common anesthetics like propofol suppress mitochondrial activity, potentially causing harm.6
A rare form of dystonia lacking solid evidence on GPi‐DBS is caused by biallelic SERAC1 variants. SERAC1‐related disease is a mitochondriopathy encompassing a wide phenotypic spectrum, ranging from severe infantile‐onset Leigh‐like syndromes (ie, 3‐methylglutaconic aciduria with deafness, encephalopathy, and Leigh‐like syndrome—MEGDEL) to the recently described adult‐onset dystonia‐parkinsonism.7, 8, 9 Typically, SERAC1‐related dystonia involves cranio‐cervical districts, manifesting with dysarthria, dysphagia, repetitive tongue protrusion, and excessive drooling.7
Here we report a patient with SERAC1‐related dystonia treated with GPi‐DBS. The proband, whose genetic and clinical features are detailed in reference,9 is a 56‐year‐old female carrying the homozygous c.1231C>T p.(Arg411Cys) variant. She presented dystonia‐parkinsonism with onset at 38 years, representing one of the mildest SERAC1‐related phenotypes reported to date.9 After the diagnosis, the patient underwent several therapeutic attempts: levodopa (up to 1000 mg/day), amantadine, trihexyphenidyl, and tetrabenazine were administered with poor response; onabotulinum toxin A (right splenius capitis 75 U, right levator scapulae 30 U, left platysma 20 U, upper orbicularis oris 2.5 U, intrinsic muscles of the tongue 10 U), clozapine (suspended due to neutropenia), and olanzapine offered a relevant but partial clinical benefit (Video 1).
Thus, at the age of 55 years, the patient underwent DBS surgery. The surgical procedure was performed under general anesthesia using the Leksell Vantage stereotactic system and the Medtronic StealthStation S8, guided by 1.5 T brain MRI and CT imaging (Fig. 1). The anterior commissure‐posterior commissure (AC‐PC) measured 23.2 mm. The optic tract was traced and its lateral coordinate—identified on a coronal plane 2 mm anterior to the midcommissural point—was selected as the lateral coordinate for the trajectory targeting the GPi. Based on microelectrode recordings of GPi activity from 3 to 1 mm above the target across all trajectories and absence of pyramidal effects after macrostimulation up to 3 mA, two Medtronic® B3300542 directional leads were implanted bilaterally. The lead tips were positioned 1 mm above the target along the central track and connected to the Medtronic Percept PC neurostimulator. Based on the planned coordinates and final electrode placement, the stimulation site was estimated to lie 2–3 mm anterior and 22 mm lateral at the AC‐PC plane (Video 2). Two months later, stimulation was progressively initiated reaching the following setting at 6 months follow‐up: right GPi 10‐C+ 3.2 mA, 90 μs, 110 Hz; left GPi 2‐C+ 3.2 mA, 90 μs, 110 Hz.
The patient exhibited a remarkable improvement with GPi‐DBS: speech, though still dysarthric, became eventually comprehensible; jaw tremor and tongue protrusion improved significantly; cervical posture appeared stable, yet with resolution of the chronic pain; bradykinesia as well as rest and action tremor almost disappeared in right upper limb and became milder in left upper limb; repetitive actions execution became more fluent (Video 3). No dysphagia could be detected at instrumental evaluation. No neuropsychological abnormalities were detected besides a mild attentional deficit.
Clinical response to GPi‐DBS has been quantitatively evaluated with the Movement Disorders Society Unified Dystonia Rating Scale (40 → 19), the Movement Disorders Society Global Dystonia Severity Scale (35 → 13), the Burke‐Fahn‐Marsden Movement Scale (41 → 21) – Supplementary File S1. Health‐related Quality of Life Instrument with 20 items (HINT‐20) total transformed score improved from 60/100 to 85/100.
The resolution of dysphagia allowed the resumption of an adequate oral intake leading to weight gain from 56 to 75 kg (BMI 20.1 → 26.9 kg/m2) in 6 months, therefore feeding through percutaneous endoscopic gastrostomy was suspended. As mild cervical dystonia persisted, onabotulinumtoxin A was injected again in the right splenius capitis (75 U) and in the left trapezius (25 U). The global motor and psychological improvement allowed a gradual tapering of pharmacological therapy with olanzapine.
To our knowledge, among the ~70 reported cases of SERAC1‐related disease, only a 16‐year‐old girl with generalized dystonia, athetoid movements, and ataxia underwent GPi‐DBS with significant and enduring motor improvement.10
In conclusion, we report a patient with SERAC1‐related dystonia‐parkinsonism who had a remarkable and persistent benefit from bilateral GPi‐DBS. Our case, along with the one reported by Sharma et al, 202110 suggests that GPi‐DBS can be a valuable therapeutic option for this rare disease, especially for patients with later onset and mild phenotype, emphasizing the importance of SERAC1 screening in patients with dystonia.
Author Roles
(1) Research project: A. Conception, B. Organization, C. Execution; (2) Statistical Analysis: A. Design, B. Execution, C. Review and Critique; (3) Manuscript Preparation: A. Writing of the first draft, B. Review and Critique
V.Y.: 1A, 1C, 3A.
A.D.M.: 1A, 1C, 3A.
M.T.: 1C, 3B.
L.T.: 1C, 3B.
G.S.: 1C, 3B.
C.M.: 1C, 3B.
M.P.: 1C, 3B.
C.C.: 1C, 3B.
D.L.: 1C, 3B.
M.E.: 1B, 1C, 3A.
S.M.: 1C, 3B.
T.B.: 1C, 3B.
A.P.: 1A, 1B, 3B.
G.O.: 1A, 1C, 3A.
Disclosures
Ethical Compliance Statement: The authors confirm that the approval of an institutional review board was not required for this work. Written informed consent was obtained by the patient. We confirm that we have read the Journal's position on issues involved in ethical publication and affirm that this work is consistent with those guidelines.
Funding Sources and Conflicts of Interest: No specific funding was received for this work. The authors declare that there are no conflicts of interest relevant to this work.
Financial Disclosures for the previous 12 months: AP was consultant for Newronika, Milan, Italy SpA in the last 12 months. The other authors declare that there are no additional disclosures to report.
Supporting information
File S1. Tables displaying detailed motor scales before and after DBS surgery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Artusi CA , Dwivedi A , Romagnolo A , et al. Differential response to pallidal deep brain stimulation among monogenic dystonias: systematic review and meta‐analysis. J Neurol Neurosurg Psychiatry 2020;91:426–433.32079672 10.1136/jnnp-2019-322169 · doi ↗ · pubmed ↗
- 2Tisch S , Kumar KR . Pallidal deep brain stimulation for monogenic dystonia: the effect of gene on outcome. Front Neurol 2021;11:630391. 10.3389/fneur.2020.630391.33488508 PMC 7820073 · doi ↗ · pubmed ↗
- 3Duga V , Giossi R , Romito LM , et al. Long‐term Globus pallidus internus deep brain stimulation in pediatric non‐degenerative dystonia: a cohort study and a meta‐analysis. Mov Disord 2024;39:1131–1144.38646731 10.1002/mds.29815 · doi ↗ · pubmed ↗
- 4Indelicato E , Boesch S , Mencacci NE , Ghezzi D , Prokisch H , Winkelmann J , Zech M . Dystonia in ATP synthase defects: reconnecting mitochondria and dopamine. Mov Disord 2024;39:29–35.37964479 10.1002/mds.29657 · doi ↗ · pubmed ↗
- 5Ghaoui R , Sue CM . Movement disorders in mitochondrial disease. J Neurol 2018;265:1230–1240.29307008 10.1007/s 00415-017-8722-6 · doi ↗ · pubmed ↗
- 6Niezgoda J , Morgan PG . Anesthetic considerations in patients with mitochondrial defects. Paediatr Anaesth 2013;23:785–793. 10.1111/pan.12158.23534340 PMC 3711963 · doi ↗ · pubmed ↗
- 7Maas RR , Iwanicka‐Pronicka K , Kalkan Ucar S , et al. Progressive deafness–dystonia due to SERAC 1 mutations: a study of 67 cases. Ann Neurol 2017;82:1004–1015.29205472 10.1002/ana.25110 PMC 5847115 · doi ↗ · pubmed ↗
- 8Ashton C , Davis M , Laing N , Ravenscroft G , Lamont P . Novel SERAC 1 variant presenting with adult‐onset extrapyramidal dystonia‐parkinsonism phenotype. Neurol Genet 2023;9:e 200067.37090937 10.1212/NXG.0000000000200067 PMC 10117696 · doi ↗ · pubmed ↗