Haemoptysis as a Presenting Manifestation of Hepatopulmonary Syndrome With Complete Resolution After Liver Transplantation
Venkatkiran Kanchustambham

TL;DR
A patient with liver disease showed haemoptysis as a rare symptom of hepatopulmonary syndrome, which resolved after a liver transplant.
Contribution
Haemoptysis is reported as a rare presenting feature of hepatopulmonary syndrome, with resolution after liver transplantation.
Findings
Contrast echocardiography confirmed intrapulmonary shunting in a patient with hepatopulmonary syndrome.
Haemoptysis and hypoxemia resolved completely after liver transplantation.
This case highlights an unusual clinical presentation of hepatopulmonary syndrome.
Abstract
Hepatopulmonary syndrome (HPS) is a pulmonary vascular complication of chronic liver disease characterised by intrapulmonary vascular dilatation and hypoxemia. Dyspnoea and orthodeoxia are classic features, while haemoptysis is rarely reported. We describe a patient with cirrhosis who presented with recurrent haemoptysis and progressive hypoxemia. Contrast‐enhanced transthoracic echocardiography demonstrated intrapulmonary right‐to‐left shunting, which resolved following orthotopic liver transplantation, with complete cessation of haemoptysis. Hepatopulmonary syndrome rarely presents with haemoptysis. This case demonstrates haemoptysis as a presenting manifestation of HPS, with intrapulmonary shunting documented on contrast echocardiography before liver transplantation and complete resolution after transplantation.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
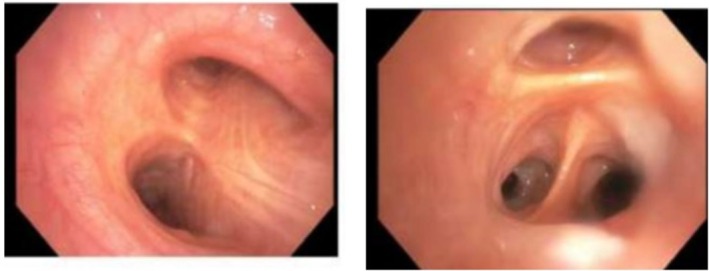 FIGURE 1
FIGURE 1| Parameter | Value |
|---|---|
| pH | 7.47 |
| PaCO2 (mmHg) | 25 |
| PaO2 (mmHg) | 34 |
| Oxygen saturation (%) | 86 |
| Alveolar–arterial gradient | Markedly elevated |
| Oxygen source | Room air |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Anomalies and Treatments · Liver Disease and Transplantation · Organ Transplantation Techniques and Outcomes
Introduction
1
Hepatopulmonary syndrome (HPS) is defined by the triad of chronic liver disease or portal hypertension, intrapulmonary vascular dilatation and impaired arterial oxygenation [1]. The prevalence among patients with cirrhosis ranges from 5% to 30% [1, 2]. Clinically, HPS typically presents with dyspnoea, platypnea–orthodeoxia, and progressive hypoxemia [1]. While uncommon, haemoptysis has been reported in isolated cases and remains an underrecognised manifestation [3, 4]. We report a case of haemoptysis as a presenting manifestation of HPS with complete resolution following liver transplantation.
Case Report
2
A patient with cirrhosis due to non‐alcoholic steatohepatitis presented with recurrent haemoptysis and progressive hypoxemia. Extensive evaluation including chest imaging, upper endoscopy, ENT examination and bronchoscopy failed to identify an alternative bleeding source. Flexible bronchoscopy demonstrated normal endobronchial anatomy without active bleeding or endobronchial lesions (Figure 1).
Bronchoscopy images demonstrating normal endobronchial anatomy without evidence of active bleeding or endobronchial lesion.
Arterial blood gas analysis confirmed severe hypoxemia with a widened alveolar–arterial gradient (Table 1). Transthoracic echocardiography with agitated saline contrast demonstrated delayed opacification of the left heart several cardiac cycles after right‐sided opacification, consistent with intrapulmonary right‐to‐left shunting (Video 1). The patient was diagnosed with hepatopulmonary syndrome and subsequently underwent orthotopic liver transplantation.
Pre‐transplant transthoracic echocardiogram with agitated saline demonstrating delayed opacification of the left heart, consistent with intrapulmonary right‐to‐left shunting. Video content can be viewed at https://onlinelibrary.wiley.com/doi/10.1002/rcr2.70508.
Additional anatomic localisation of the shunt (e.g., pulmonary angiography) was not pursued because intrapulmonary shunting in hepatopulmonary syndrome is typically diffuse, and further localisation would not have altered management. At the time of diagnosis, the patient already met criteria for liver transplantation based on advanced liver disease with severe hepatopulmonary syndrome–related hypoxemia, with haemoptysis considered a secondary manifestation rather than the primary indication for transplantation.
Following transplantation, oxygenation progressively normalised and haemoptysis did not recur. Repeat contrast‐enhanced echocardiography demonstrated complete resolution of intrapulmonary shunting with absence of delayed left‐heart opacification (Video 2).
Post‐transplant transthoracic echocardiogram with agitated saline demonstrating absence of delayed left‐heart opacification, consistent with resolution of intrapulmonary shunting. Video content can be viewed at https://onlinelibrary.wiley.com/doi/10.1002/rcr2.70508.
Discussion
3
Hepatopulmonary syndrome (HPS) is defined by chronic liver disease or portal hypertension, intrapulmonary vascular dilatation, and impaired arterial oxygenation. Typical manifestations include dyspnoea, platypnea–orthodeoxia, and hypoxemia, while haemoptysis remains exceptionally rare [1].
A focused review identifies approximately six reported cases associating haemoptysis with HPS or related pulmonary vascular phenotypes. Schraufnagel et al. described haemoptysis with respiratory failure in severe HPS [3]. Gupta et al. reported haemoptysis resolving after liver transplantation [4]. More recently, Condon and Kanchustambham reported haemoptysis as a presenting manifestation of HPS with post‐transplant resolution [5]. Pasha et al. described haemoptysis in Abernethy malformation with secondary HPS, suggesting accelerated pulmonary vascular remodelling [6]. Lawton and Holmes‐Liew reported HPS in the setting of common variable immunodeficiency [7]. Sarac et al. described pulmonary arteriovenous fistula with haemoptysis, illustrating vascular mimics that may overlap with HPS physiology [8]. Shah et al. reported combined hepatopulmonary and portopulmonary vascular disease after paediatric liver transplantation [9]. Collectively, these remain isolated reports, with no cohort studies identifying haemoptysis as a recognised manifestation of HPS.
The pathophysiology of HPS involves pulmonary endothelial dysfunction with increased nitric oxide production and dysregulated angiogenic signalling, including vascular endothelial growth factor (VEGF), resulting in diffuse capillary dilatation, intrapulmonary arteriovenous communications and right‐to‐left shunting [1, 2]. Progressive vascular remodelling may create fragile microvascular networks susceptible to rupture under increased pulmonary blood flow and shear stress, providing a plausible mechanism for haemoptysis.
Previously reported cases often describe haemoptysis occurring late in the disease or in association with complex vascular or congenital abnormalities [3, 6, 8]. In contrast, the present case demonstrates haemoptysis as a presenting manifestation of HPS, with objective confirmation of intrapulmonary shunting and complete resolution of both hypoxemia and haemoptysis following liver transplantation, strengthening causal inference.
In this case, intrapulmonary shunting was confirmed by contrast‐enhanced transthoracic echocardiography. An additional anatomic localisation was not pursued because HPS‐related shunting is typically diffuse and would not have altered management once transplant candidacy was established.
Clinically, HPS should be considered in patients with chronic liver disease or portal hypertension who present with unexplained hypoxemia, orthodeoxia or otherwise unexplained haemoptysis after exclusion of common pulmonary, airway and gastrointestinal causes, as liver transplantation remains the only definitive therapy [10].
In conclusion, this case highlights haemoptysis as a rare but clinically significant presentation of hepatopulmonary syndrome. In patients with chronic liver disease, unexplained haemoptysis and hypoxemia should prompt evaluation for intrapulmonary shunting. Early recognition is essential, as liver transplantation can result in complete resolution of pulmonary manifestations.
Author Contributions
Venkatkiran Kanchustambham was responsible for clinical management, imaging review and manuscript preparation.
Funding
The author has nothing to report.
Consent
The author declares that written informed consent was obtained for the publication of this manuscript, images and echocardiographic videos using the consent form provided by Respirology Case Reports.
Conflicts of Interest
The author declares no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1R. Rodríguez‐Roisin and M. J. Krowka , “Hepatopulmonary Syndrome — A Liver‐Induced Lung Vascular Disorder,” New England Journal of Medicine 358, no. 22 (2008): 2378–2387.18509123 10.1056/NEJ Mra 0707185 · doi ↗ · pubmed ↗
- 2M. B. Fallon , S. M. Kawut , E. Taioli , et al., “Pulmonary Vascular Complications of Liver Disease,” American Journal of Respiratory and Critical Care Medicine 189, no. 5 (2014): 509–519.10.1164/rccm.201209-1583 CIPMC 357065723155142 · doi ↗ · pubmed ↗
- 3D. E. Schraufnagel , R. Malik , K. Parekh , et al., “Hemoptysis, Hepatopulmonary Syndrome, and Respiratory Failure,” Chest 112, no. 1 (1997): 282–284.10.1378/chest.111.6.17249187200 · doi ↗ · pubmed ↗
- 4S. Gupta , H. Castel , R. V. Rao , and M. Picard , “Hemoptysis in Hepatopulmonary Syndrome,” Respiratory Medicine 104, no. 2 (2010): 314–316.
- 5S. Condon and V. K. Kanchustambham , “Hemoptysis as a Rare Presentation of Hepatopulmonary Syndrome,” Chest 166, no. 4 Suppl (2024): A 5313.
- 6S. U. Pasha , “An Unusual Case of Hemoptysis Secondary to Abernethy Malformation Type II and Hepatopulmonary Syndrome,” IP Indian Journal of Immunology and Respiratory Medicine 6, no. 4 (2021): 237–240.
- 7E. Lawton and C. L. Holmes‐Liew , “A Rare Case of Common Variable Immunodeficiency and Hepatopulmonary Syndrome,” Respirology Case Reports 10 (2022): e 0898.35028155 10.1002/rcr 2.898PMC 8737112 · doi ↗ · pubmed ↗
- 8S. Sarac , “Pulmonary Arteriovenous Fistula and Bronchiectasis in a Female Patient With Hemoptysis,” Respiratory Medicine Case Reports 21 (2017): 154–157.28560147