Feasibility, usability, and acceptability of the asynchronous trauma-focused CARE training program for healthcare providers: a cross-sectional study
Dana C. Ross, Nancy McCallum, Aysha Butt, Annie K. Truuvert, Eileen Wang, David Rojas, Sophie Soklaridis, Simone N. Vigod

TL;DR
A new online training program called CARE was found to be feasible and well-received by healthcare providers for learning trauma-focused skills.
Contribution
The CARE program introduces a scalable, asynchronous, multimedia training platform for trauma-focused psychoeducation.
Findings
Most participants completed the training modules and found the multimedia format helpful.
The program was described as clear, practical, and easy to navigate by participants.
Time constraints were the main barrier, but the content on emotion regulation was particularly valued.
Abstract
The long-term effects of adverse childhood experiences, including various forms of abuse, neglect, and trauma, are well-documented but often inadequately addressed in healthcare settings. Healthcare providers frequently lack the training necessary to provide trauma-focused, evidence-based interventions. To address this gap, we developed the ‘Community Access to Resourced & Resilient PsychoEducation’ (CARE) training program, a scalable, asynchronous, virtual learning platform designed to equip healthcare providers with the skills and knowledge to facilitate an 8-week trauma-focused psychoeducational group intervention for adults with a history of childhood interpersonal trauma. In this cross-sectional study, we evaluated the feasibility, usability, and acceptability of the CARE training program among 62 healthcare providers from six organizations across Ontario. Pre- and post-training…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
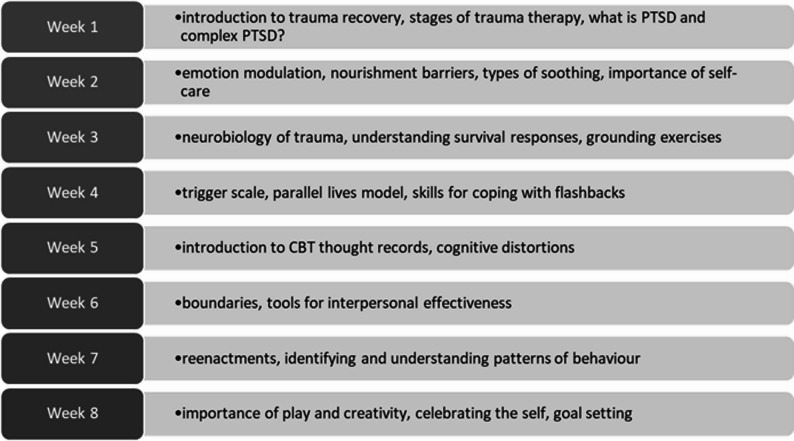 Figure 1
Figure 1- —The Slaight Family Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChild Abuse and Trauma · Posttraumatic Stress Disorder Research · Migration, Health and Trauma
Introduction
The lasting mental and physical effects of adverse childhood experiences (ACEs), including various forms of abuse, abandonment, and neglect, have been extensively studied and recognized [1, 2]. However, the impact of trauma is often overlooked and inadequately addressed in healthcare settings [3, 4]. Compounding this, healthcare providers (HCPs) frequently lack the training and confidence to provide evidence-based therapy interventions for trauma [5, 6]. Limited access to affordable and broadly accessible trauma training programs contributes to this gap, as many existing options are intensive, modality-focused, and primarily aimed at mental health clinicians, making them difficult for many HCPs to access [7]. A possible solution is a scalable, virtual training program for HCPs, focusing on facilitating a psychoeducational group therapy intervention for individuals with a history of ACEs. Such a program could significantly increase the capacity of the healthcare system to provide trauma care for patients [8, 9].
The benefits of virtual training programs include increased cost-effectiveness, enhanced accessibility, and rapid knowledge transfer [10, 11]. Research shows that online learning is at least as effective as in-person methods for augmenting HCPs knowledge, attitudes, and confidence [12–14]. The flexibility inherent in asynchronous (self-paced) training formats presents a promising avenue for vastly expanding educational opportunities for HCPs [15, 16]. However, research is needed to evaluate how to optimize the design and implementation of such training programs across diverse healthcare education contexts [17, 18].
Evidence-based trauma-focused psychotherapies that are commonly used to treat trauma-related conditions often require extensive training to master, which poses challenges related to cost and time constraints for HCPs [19, 20]. In addition, although some HCPs can provide psychotherapy within their scope of practice, many do not have access to extensive trauma-specific training or the institutional resources needed to deliver intensive trauma-focused therapies. HCPs across diverse treatment settings may benefit from more broadly applicable treatment interventions that are both feasible for HCPs to deliver and efficacious for diverse populations impacted by trauma [21–24]. A stepped-care approach to mental health treatment, which has gained traction in the literature, offers a promising solution. Stepped care approaches typically match intervention intensity to client needs, offering lower-intensity options as an initial step before progressing to more specialized treatments. This approach requires less intensive training for HCPs and emphasizes lower-intensity interventions initially, focusing on psychoeducation and skills-building, which have demonstrated promising outcomes [25–27].
Importantly, psychoeducation as a treatment intervention for patients has demonstrated effectiveness in treating depression, anxiety, and complex mental health conditions like schizophrenia and bipolar disorder [28–30]. Psychoeducation aims to enhance patients’ knowledge and understanding of their struggles through education, insight-building, and skill development [31, 32]. It offers benefits such as improved treatment adherence, enhanced mood and self-regulation, reduced hospitalization rates, and symptom improvement [33, 34]. In addition, psychoeducational interventions are often offered in group settings, which can potentially be less resource-intensive and more cost-effective [34–37].
Based on the results of an earlier needs assessment study by our team, we developed the asynchronous, virtual ‘Community Access to Resourced & Resilient PsychoEducation’ (CARE) training program. The goal of the CARE training program is to equip HCPs with the skills and knowledge necessary to deliver an 8-week group-based psychoeducational treatment intervention for adult survivors of childhood trauma. The aim of current study, however, was not to evaluate the delivery of the group, but to assess the feasibility, usability, and acceptability of the CARE training program itself. By leveraging a virtual platform and asynchronous learning strategies, the CARE training program could overcome geographical distance and scheduling conflicts, increasing HCPs’ access to trauma training.
Methods
The intervention
The virtual, asynchronous CARE training program features eight modules based on content from an 8-week psychoeducational, trauma-focused Resourced and Resilient (R&R) group offered to adults enrolled in the Trauma Therapy Program (TTP) at Women’s College Hospital (WCH) in Toronto, Ontario, Canada. The TTP is in an academic ambulatory hospital department of the psychiatry program and offers primarily group psychotherapy to adults experiencing symptoms related to adverse childhood experiences. The R&R group was initially developed in 2004 by a multidisciplinary team of therapists and is a manualized group psychotherapy intervention that combines psychoeducation on the impact of childhood trauma, along with skills and strategies for healing. R&R is currently offered either in-person or synchronously via Zoom. It typically has 10–12 group participants and is co-facilitated by two staff members. The R&R group format was recently adapted in TTP to be a hybrid treatment intervention including self-paced online modules along with 1-hour weekly group sessions facilitated by trauma therapists [38]. This adapted version was evaluated in a pilot study showing a significant pre-post decrease in PTSD symptoms following completion of the intervention [39] and a randomized wait-list controlled trial has recently been completed [40]. The R&R group presents material focused on conceptualizing symptoms and struggles as understandable and often adaptive impacts of childhood trauma, while supporting the development of safer and more effective coping capacities. The content draws on evidence-based approaches shown to improve mood, anxiety, PSTD symptoms, self-regulation, and distress tolerance, including psychoeducational interventions [41–43], cognitive and dialectical behavioural therapy tools [44–46], mindfulness [47] and sensorimotor psychotherapy-informed strategies [48]. Additional detail is outlined in Fig. 1.
Fig. 1CARE Training Module content outline
Setting and participants
This cross-sectional study, using a pre-training questionnaire and a separate post-training questionnaire (supplementary file 1), was conducted at Women’s College Hospital between January 2020 and March 2021. HCPs were eligible for study participation, including social workers, physicians, nurses, registered psychotherapists, community support workers and mental health counsellors working at the six participating community healthcare organizations in Ontario, Canada. These six organizations had independently emailed the TTP program and expressed an interest in receiving trauma-related training. A research staff member then emailed organization contacts about the study. Interested individual HCPs from the participating sites responded via phone or email to learn more about the study and register for the asynchronous online CARE training program. Informed consent was obtained from participants. Once enrolled, a pop-up explaining the study, risks and benefits were presented to participants who were asked to select “I agree” to continue their participation in the study. Participant eligibility included having access to an internet-enabled device and the ability to speak and understand English. CARE training program registration was free, and participants were given approximately three months to complete the training modules. The team tracked participant progress and module completion.
Data collection procedures
Data were collected using electronic questionnaires embedded within the Thinkific learning platform, which hosted the CARE training modules. Participants completed the pre-training questionnaire immediately after registering for the CARE program and before beginning module one. The pre-training questionnaire assessed prior training and experience with virtual courses. The post-training questionnaire was presented at the end of the final module, and evaluated feasibility, usability, and acceptability of the CARE modules.
Survey items were developed by the study team and reflected domains commonly evaluated in implementation science studies of digital healthcare interventions, including feasibility, usability, and acceptability studies [49–51], as well as content areas relevant to the CARE curriculum. Both Likert-scale items and open-ended questions were included. No personal identifiers were collected. Responses informed future refinements to the training content and overall platform design.
Data analysis
Consistent with prior implementation science literature, feasibility was defined as the practicality of delivering the CARE training program as intended, including participant engagement, module completion, and time required to complete the training [52]. Usability captured the ease of navigation, clarity, and functionality of the online training program [53]. Acceptability referred to participants’ perceptions of the training content, including its relevance, value, and overall satisfaction [54].
To assess feasibility, we calculated the proportion of participants who completed the pre-training questionnaires and the proportion of participants who completed (a) all training modules and (b) at least 50% of the modules. Feasibility was also assessed by calculating the length of time it took to complete the modules. Usability and acceptability outcomes were calculated using Likert-type scale responses and through qualitative feedback from open-ended questions. All analysis were descriptive and conducted using Microsoft Excel.
Results
Participant characteristics
Sixty-two participants were enrolled in the study, completed the pre-module questionnaires, and answered questions about their experience with e-learning and trauma-focused training prior to module completion (see Table 1). The timeline for training program registration varied between sites, beginning in March 2020, with the last registration in December 2020. Additional demographic data was not collected but will be collected in an upcoming study phase examining knowledge outcomes following CARE training program completion.
Table 1. Participant characteristicsCharacteristicNumber of Participants n = 62 (%)Time working in the healthcare field Less than 1 year13 (21.0%) 1–5 years14 (22.6) 6–10 years9 (14.5) 11–15 years9 (14.5) 16 or more years17 (27.4)Time working in current position 1–5 years44 (71.0) 6–10 years10 (16.1) 10–20 years8 (12.9)Done e-learning modules in the past Yes60 (96.8) No2 (3.2)Previous training on delivering trauma-focused health care Yes49 (79.0) No13 (21.0)
Feasibility
Regarding training program completion, 73% of participants completed at least 50% of the modules, and 65% completed the full training (i.e., at least 90% of the modules) (Table 2).
Table 2. Average time spent to complete all 8 modules n = 34(%)2–4 h6 (17.6%)5–7 h12 (35.3%)8–10 h10 (29.4%)More than 10 h6 (17.6%)
Out of the 62 participants, 81.3% of respondents took less than one hour to complete each module, and 18.8% took more than 60 min. 64.7% of participants required 5–10 h to complete all eight modules.
Post-module evaluation
Of the 40/62 (65%) participants who completed at least 90% of the modules, 34 (85%) completed the post-training modules questionnaire (Table 3). Of these, 97% agreed that the time invested in completing the modules was well-matched to the knowledge gained and would recommend the modules to their colleagues. All respondents thought the content quality was consistent and clear, and the modules were easy to navigate, met their expectations, and had no significant technical difficulties. In particular, 97% felt the multimedia format improved their learning experience. No participants reported accessibility issues.
Table 3. Post-Training survey: usability & acceptability ratingsStatementn = 34Strongly Disagree (%)Disagree (%)Neither Agree nor Disagree (%)Agree (%)Strongly Agree (%)Time spent completing modules was well-matched with the knowledge gained.001 (2.9)15 (44.1)18 (52.9)The multi-media format improved the experience of completing the modules.001 (2.9)9 (26.5)24 (70.6)Content quality was consistent throughout the modules.0008 (23.5)26 (76.5)Modules were easy to follow.0008 (23.5)26 (76.5)Content was clear to facilitate learning.0009 (26.5)25 (73.5)Modules met my learning expectations00014 (41.2)20 (58.8)I would recommend the e-learning modules to colleagues.001 (2.9)8 (23.5)25 (73.5)
While most respondents encountered no barriers to module completion, the most cited barrier (n = 4 or 11.4% of participants) was finding time to complete the modules. Participants answered open-ended questions about bias and provided feedback for future modifications. They felt that the modules were unbiased. However, two recognized that they lacked information on how to facilitate a session with an awareness of cultural differences and recommended this topic for future iterations. Three felt that including additional elements around cultural, systemic, and intergenerational trauma would create a more holistic and patient-focused program, which will be addressed in future program iterations.
Highlights of learning experience
The topics in Table 4 were covered in the online modules and were seen as particularly valuable content by respondents.
Table 4. Topics in the modules that HCP participants highlighted as most importantModule Topic highlighted by participantsDefinitionTraumatic re-enactments in adulthood (n = 10)Ways trauma-based interpersonal patterns play out in current relationships or situations.Emotional regulation strategies for patients (n = 10)Models and skills on how to regulate emotional and physiological distressClinical pearls for HCPs facilitating future R&R groups (n = 6)Tips for HCPs when working with content in a group format.Dissociation – an explanation for HCPs on dissociative symptoms (n = 1)Disconnecting from internal or external experiences as a protection against pain and distress.Nourishment barriers as a form of self-protection (n = 2)Difficulty taking in positive or healthy experiences or treating self with care and kindness.Tension-reduction behaviours for patients (n = 1)Various behaviours that are potentially harmful but are used to regulate trauma-related distress.
Discussion
This study examined the feasibility, usability, and acceptability of the virtual, asynchronous CARE training program for healthcare providers. The CARE program consists of modules that educate HCPs about the psychoeducational content of the R&R group intervention for adults with a history of adverse childhood experiences, as well as how to deliver this content in a group setting. Despite high levels of prior e-learning experience, prior training in trauma-focused care, and over half having six or more years of experience in healthcare, participants reported that the modules continued to meet their learning needs, with all agreeing that the content met their expectations. These findings align with broader literature suggesting that even experienced HCPs value structured educational programs and may benefit from ongoing learning opportunities across their practice settings [55, 56]. Notably, most participants had relatively short tenures in their current positions (five years or less), suggesting that an easily accessible, asynchronous training program may be particularly well-suited to a healthcare environment characterized by high staff turnover. Training programs that utilize asynchronous or blended approaches can accommodate the dynamic nature of healthcare settings, provide ongoing training opportunities, and may support knowledge transfer even amidst personnel changes.
Feasibility of the CARE training program was supported by high levels of module completion and a time commitment that was generally manageable within routine clinical workflows. Nearly three-quarters of participants completed at least half of the modules, and almost two-thirds completed the full training, suggesting that the program could be delivered as intended in real-world healthcare settings. Most participants completed individual modules in under one hour, and the majority completed all eight modules within five to ten hours, indicating that the overall training burden was reasonable. Not unexpectedly, our study identified that the most reported barrier to attendance was a need for more time to complete the training modules, highlighting the importance of institutional support and paid time for employees to engage in training. This finding confirms the significant importance of protected time for online training programs seeking optimal implementation and sustainability [57, 58].
In terms of acceptability of the format and delivery of the CARE training program, participants reported positive experiences with the asynchronous, multimedia design. Integrating technology in education can effectively engage learners by incorporating multimedia content, such as video and audio recordings [59]. In the post-module evaluation, respondents appreciated the multimedia format of the asynchronous online modules, feeling that the time invested in module completion was well-balanced and appropriate to the knowledge gained. This positive reception of our asynchronous program may be influenced by the widespread adoption of virtual care during the COVID-19 pandemic, which likely enhanced participants’ familiarity and comfort with utilizing technology for learning. All participants reported prior engagement with online modules, indicating HCP’s growing acceptance of and integration of technology in healthcare education initiatives [13, 60]. These findings align with literature supporting the acceptability and usability of virtual platforms for delivering training on evidence-based treatments to HCPs with variable experience [61, 62].
With respect to acceptability of the training content, HCPs appreciated the psychoeducational nature of the CARE training program, emphasizing the valuable insights gained from experienced trauma therapists featured in the modules and the integration of emotion regulation skills and tension-reduction behaviours within the program. These results align with existing literature supporting the acceptability and usefulness of psychoeducational interventions in mental health, including those used by HCPs in diverse settings [63, 64]. Stepped care refers to matching intervention intensity to patient needs; the CARE training prepares HCPs to deliver a lower-intensity psychoeducational intervention that aligns with the early steps of stepped care.
Training that targets diverse HCPs, rather than a single profession, can provide an opportunity to bridge gaps and communication divides between different professional perspectives by providing shared knowledge and a common language learned [65]. In this study, usability of the CARE training program was supported by participants’ reports that the modules were easy to follow and navigate, content was clear to facilitate learning, and no significant technical or accessibility barriers were encountered. Participants described the program as practical to use and perceived it as unbiased. Suggestions for additional content on facilitating sessions that consider cultural differences, systemic issues, and intergenerational trauma will be addressed in the program’s next iteration, followed by consultation with key stakeholders. Our findings are supported by research demonstrating the effectiveness of web-based training programs in engaging multidisciplinary audiences, even without tailoring the content for specific provider roles [66, 67].
A strength of our study is the inclusion of HCPs from six different healthcare organizations, broadening our findings’ generalizability. However, the community organizations involved in the study were not randomly selected; they approached us for training, which may have introduced selection bias. In addition, provider-type data was not collected in this feasibility phase, limiting our ability to examine differences across disciplines or roles. Provider-type data will be collected in the next phase, enabling examination of role-specific engagement patterns. We also did not collect data from non-completers, which introduces the possibility of completion bias. Additionally, completion rates for post-module questions (n = 40) were lower than pre-module questions (n = 62), potentially impacting the reliability and validity of our data. Systematic reviews have noted that more research is required to gain a better understanding of how to optimize the design, development, and implementation of online interventions [68–70]. We did not explore the attitudes and acceptability of the program in organizational leaders/management beyond their sanctioning of employees’ participation in the study; this will be important to factor into a future implementation phase of this study. However, we anticipate offering organizations access to the training at no cost in the next phase of this study, which may add to its appeal to future partners.
Conclusion
Our study strengthens the existing literature’s emphasis on the need for accessible, affordable, and scalable trauma-focused training on psychoeducational interventions [7, 71]. HCPs across six healthcare organizations responded positively to our virtual CARE training program’s asynchronous, multimedia, psychoeducational content. Our results suggest that the CARE training program offers a feasible and engaging approach to trauma-focused psychoeducational training. Future phases of this study will include post-training confidence and knowledge outcomes and will examine effectiveness and implementation.
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sucich J, Breitbart V, Williams S, Sanichar N, Candelaria-Arce E, Frankle WG, et al. Prevalence of childhood trauma in a community-based mental health clinic. Community Ment Health J. 2023;59(6):1136–49.10.1007/s 10597-023-01094-136752932 · doi ↗ · pubmed ↗
- 2Hartzler B, Hinde J, Lang S, Correia N, Yermash J, Yap K, et al. Virtual training is more cost-effective than in-person training for preparing staff to implement contingency management. J Technol Behav Sci. 2023:8:255–64.10.1007/s 41347-022-00283-1PMC 955363036246531 · doi ↗ · pubmed ↗
- 3Davis LL, Schein J, Cloutier M, Gagnon-Sanschagrin P, Maitland J, Urganus A, et al. The economic burden of posttraumatic stress disorder in the United States from a societal perspective. J Clin Psychiatry. 2022;83(3):21m 14116.10.4088/JCP.21m 1411635485933 · doi ↗ · pubmed ↗
- 4Sweet CMC, Li EJ, Sagui-Henson S, Chamberlain CEW, Altman M. Impact of online group psychoeducation and support sessions on receptivity towards digital mental health care during the COVID-19 pandemic: a pilot study. J Technol Behav Sci. 2022;8:216–24.10.1007/s 41347-022-00281-3PMC 951018736189429 · doi ↗ · pubmed ↗
- 5Ross DC, Mc Callum N, Truuvert AK, Butt A, Behdinan T, Rojas D, et al. The development and evaluation of a virtual, asynchronous, trauma-focused treatment program for adult survivors of childhood interpersonal trauma. J Ment Health. 2024:33(5):566–75.10.1080/09638237.2024.233279738572918 · doi ↗ · pubmed ↗
- 6Behdinan T, Truuvert AK, Adekunte A, Mc Callum N, Vigod SN, Butt A , et al. The Trauma PORTAL-A blended e-Health intervention for survivors of childhood interpersonal trauma: an open-label pilot study. Telemed Rep. 2024;5(1):195–204.10.1089/tmr.2024.0020 PMC 1128600039081455 · doi ↗ · pubmed ↗
- 7Ross DC. The Trauma Portal Project: a Virtual, Asynchronous Treatment for Interpersonal Trauma 2022 [CT 05670405]. Available from: https://clinicaltrials.gov/study/NCT 05670405.
- 8Kodweis KR, Hall EA, Renfro CP, Thomas-Gosain N, Lennon-Dearing R, Walker JK, et al. Successful development and implementation of a large virtual interprofessional education activity applying the social determinants of health. Pharm (Basel). 2022;10(6):157.10.3390/pharmacy 10060157 PMC 978087736548313 · doi ↗ · pubmed ↗