Advances in Minimally Invasive General Surgery: A Narrative Review of Techniques, Technologies, and Patient Outcomes
Ashok Kumar Verma, Banyeswar Pal, Somen Sanfui, Arnab Mondal, Rahima R Malek, Radhey Shyam Singh, G Harsha Vardhan Reddy

TL;DR
Minimally invasive general surgery offers better patient outcomes than open surgery but faces challenges in training, cost, and global access.
Contribution
This review synthesizes recent evidence on MIGS innovations and highlights the role of AI and ML in improving surgical precision and training.
Findings
MIGS reduces postoperative pain, hospital stay, and improves recovery and quality of life compared to open surgery.
AI and ML show promise in enhancing surgical precision but require validation and ethical oversight.
Global disparities in access and cost-effectiveness remain significant barriers to MIGS adoption.
Abstract
Minimally invasive general surgery (MIGS) encompasses a broad spectrum of contemporary operative techniques and technologies, including laparoscopy, robotic assistance, novel access approaches, advanced energy platforms, enhanced imaging, and emerging digital tools. This narrative review, conducted through a structured literature search of major medical databases, critically examines the evolution of these innovations and their impact on surgical practice, patient outcomes, and healthcare systems. Evidence from randomized controlled trials, meta-analyses, and large observational studies published over the past decade indicates that MIGS is generally associated with reduced postoperative morbidity, shorter hospital stay, reduced postoperative pain, faster functional recovery, improved cosmetic outcomes, and enhanced patient-reported quality of life compared with open surgery. However,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
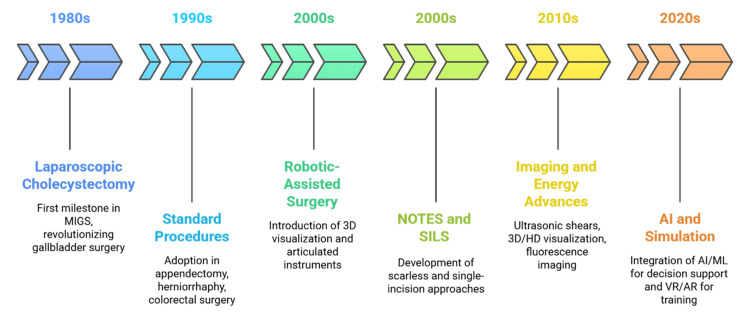 Figure 1
Figure 1| Dimension | Description | Clinical examples | Impact/outcomes | Reference |
| Principle | Small-port entry into the peritoneal cavity with video-mediated visualization | Cholecystectomy, appendectomy, colorectal resections | Minimally invasive access enabling broad general surgical application |
[ |
| Visualization advances | From fiber-optic to HD and 3D platforms, wide-angle and flexible-tip laparoscopes | Complex pelvic and hepatobiliary surgery | Improved depth perception and anatomical access, reduced operative difficulty |
[ |
| Energy devices | Bipolar cautery, ultrasonic shears, vessel-sealing systems | Colectomy, cholecystectomy, bariatric surgery | Reduced operative time, reliable hemostasis, and less intraoperative blood loss |
[ |
| Procedure-specific innovation | Self-fixating meshes and atraumatic fixation for hernia repair | Laparoscopic herniorrhaphy | Improved long-term outcomes, lower chronic pain, and decreased recurrence rates |
[ |
| Short-term outcomes | Demonstrated superiority over open surgery | Across all general surgical procedures | Reduced pain, infection, hospital stay, and faster mobilization |
[ |
| Long-term outcomes | Equivalent or superior to open surgery | Colorectal cancer, bariatric surgery | Comparable oncologic safety; durable weight loss and comorbidity reduction |
[ |
| System-level impact | Enabled Enhanced Recovery After Surgery (ERAS) pathways | Day-case cholecystectomy, colorectal resections | Shorter recovery, reduced healthcare costs, optimized system efficiency |
[ |
| Training limitations | Steep learning curve; requires structured simulation and mentoring | Complex colorectal, hepatopancreatobiliary surgery | Limits adoption in resource-poor settings |
[ |
| Cost limitations | Equipment is less costly than robotics, but still high for low-resource hospitals | General hospital settings | Restricts widespread uptake in developing healthcare systems |
[ |
| Overall status | Established as a global gold standard in minimally invasive practice | Benchmark for robotics and NOTES/SILS | Balances efficacy, safety, and cost-effectiveness, sustaining its central role |
[ |
| Technology | Description | Clinical examples | Reported clinical implications | Reference |
| 2D → HD → 3D | Evolution from early 2D laparoscopy to high-definition and 3D platforms | Broad MIGS procedures | Improved anatomical fidelity, depth perception, and safety |
[ |
| Near-infrared fluorescence (ICG) | Real-time visualization of biliary anatomy, vascular perfusion, and lymphatics | Colorectal (anastomotic perfusion), hepatobiliary surgery | Reduced anastomotic leaks and fewer bile duct injuries |
[ |
| Fluorescence angiography | ICG-based perfusion assessment | Colorectal resections | Correlated with reduced anastomotic leak rates |
[ |
| AR overlays | Superimposes preoperative imaging on the surgical field | Oncologic resections, vascular surgery | Enhanced localization of tumors and vascular structures |
[ |
| VR simulation | Immersive training and rehearsal using patient-specific models | Complex anatomical cases, surgical education | Improved preparation, reduced intraoperative uncertainty |
[ |
| Image-guided navigation | Integrates preoperative and intraoperative data into surgical maps | Liver and pancreatic surgery | Better margin clearance, reduced intraoperative blood loss |
[ |
| Limitations-fluorescence | Operator-dependent; need for standardized interpretation protocols | General MIGS | Variability in outcomes until standardization is achieved |
[ |
| Limitations-AR/VR | High cost, limited to specialized centers, lack of robust multicenter RCT evidence | Early adoption settings | Restricted availability; evidence base still largely exploratory |
[ |
| Future integration | Combining imaging with robotics, AI, and advanced energy devices | Next-generation platforms | Potential for real-time guidance, performance assessment, and surgical planning |
[ |
| Training approach | Description | Applications | Impact/outcomes | Reference |
| Conventional apprenticeship | Observation and hands-on training under supervision | Basic laparoscopic procedures | Insufficient for complex MIGS; limited by lack of tactile feedback |
[ |
| Virtual reality (VR) simulators | Immersive simulation replicating an operative environment | General laparoscopic training, bariatric/colorectal surgery | Improves precision, motion economy, and reduces intraoperative error |
[ |
| Augmented reality (AR) simulators | Superimposes anatomical landmarks and procedural steps | Live training and simulation of complex anatomy | Enhances spatial orientation, lowers cognitive burden |
[ |
| High-fidelity simulation | Rehearsal of procedures in a risk-free environment | Hemorrhage control, complex reconstructions | Builds confidence and preparedness for rare or high-risk situations |
[ |
| Objective performance metrics | Quantitative assessment of skills | VR-based training | Allows competency-based curricula, standardized evaluation |
[ |
| International collaboration | Networks and open-access training platforms | Shared training resources globally | Promotes equity, reduces disparities in access to training |
[ |
| Structured pathways | A combination of simulation, supervised surgery, and ongoing evaluation | Complex colorectal, hepatopancreatobiliary surgery | Facilitates progressive skill acquisition, reduces learning curve |
[ |
| Global variation | Disparities in resources, cost, and faculty expertise | High-income vs. low-income residency programs | Training inequities persist, limiting widespread adoption |
[ |
| Continuing professional development | Updating skills with new technologies | Robotics, AI, advanced imaging | Maintains the proficiency of experienced surgeons in rapidly evolving systems |
[ |
| Competency benchmarks | Evaluation based on performance, not case volume | Advanced laparoscopic and robotic surgery | Ensures safe practice and consistent global standards |
[ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSurgical Simulation and Training · Minimally Invasive Surgical Techniques · Augmented Reality Applications
Introduction and background
Minimally invasive general surgery (MIGS) has evolved from early laparoscopic applications to widespread use in complex colorectal, hepatobiliary, and bariatric procedures, supported by progressive advances in optics, energy devices, and robotic platforms [1]. Technological improvements, reflected in the progression from open to laparoscopic, robot-assisted, and yet more advanced modalities, also bear witness to ever more patient-centered care, safety, and economy [2]. This progress has been propelled by advances in visualization, instrumentation, and computer-assisted surgical technologies, enabling broader application of minimally invasive approaches across general surgery [3]. The widespread adoption of laparoscopic cholecystectomy marked a pivotal milestone in the expansion of MIGS, demonstrating the feasibility of performing complex procedures through minimal access techniques [4]. The advantages of less pain, reduced stay, and faster return to activity were soon proven and soon applied universally for procedures such as appendectomy, herniorrhaphy, and resection of the colon [2]. These early successes promoted the principle of minimizing tissue trauma, which is often associated with improved short-term recovery, while recognizing that procedural complexity, oncologic adequacy, and learning-curve effects may influence overall outcomes [5].
Despite its widespread adoption, conventional laparoscopy was limited by two-dimensional (2D) visualization, restricted instrument articulation, and a steep learning curve, particularly in complex hepatopancreatobiliary and esophageal procedures [6]. Robotic-assisted platforms emerged to address these constraints, offering three-dimensional (3D) visualization, articulated instruments, and enhanced ergonomics [7]. Robotic-assisted platforms were developed to address key limitations of conventional laparoscopy, including restricted instrument articulation and 2D visualization, and have been applied in technically demanding general surgical procedures such as colorectal and bariatric surgery [8]. However, cost, training requirements, and limited availability remain important barriers to widespread adoption [9]. Concurrent trends have also attempted to decrease invasiveness further. Approaches such as natural orifice transluminal endoscopic surgery (NOTES) and single-incision laparoscopic surgery (SILS) attempt to obviate or decrease visible scarring without hindering safety and efficacy [4]. Although their application remains limited in a nascent form due to technical limitations and issues of safety, these technologies are an expression of the ongoing pursuit of less invasive, more cosmetically acceptable therapy [10]. The sequential evolution of MIGS points to successive milestones from laparoscopy to digitization, as shown in Figure 1.
Evidence-informed timeline of major technological milestones in minimally invasive general surgery (MIGS)A “milestone” denotes an innovation supported by reproducible clinical adoption and published evidence demonstrating expanded procedural capability and/or measurable perioperative benefit [1,3,4,7,9].NOTES: natural orifice transluminal endoscopic surgery; SILS: single-incision laparoscopic surgery; AI: artificial intelligence; 3D: three-dimensional; HD: high-definition; ML: machine learning; VR: virtual reality; AR: augmented realityFigure created by the authors
Technological improvements in imaging and energy systems are reported to contribute to an improved intraoperative environment in MIGS [1,10]. The use of 3D and high-definition images, near-infrared fluorescence and indocyanine green (ICG), and augmented reality (AR) systems is likely to significantly aid anatomical recognition and intraoperative decision-making in technically demanding resections [5]. Concurrently, advances in ultrasonic devices and vessel sealing systems are adding efficiency to some minimally invasive procedures by enhancing hemostasis [1]. With respect to clinical evidence, some comparative clinical trials reference reductions in postoperative pain, the number of postoperative complications, and improvements in functional postoperative recovery using minimally invasive procedures as compared to an open approach for various general surgery scenarios [2]. However, these advances and benefits are not equally accessible and remain subject to significant constraints by the cost and investment requirements that these systems often incur [8].
The newest frontier in minimally invasive surgery is shaped by data-driven digital technologies, particularly the integration of robotics with artificial intelligence (AI) to enable advanced data acquisition, system intelligence, and enhanced surgical decision support [11]. These technologies hold the potential to expedite surgical education and skill acquisition while preserving patient safety when combined with virtual reality (VR) and AR simulation [3]. Before widespread adoption, however, strong validation and economical implementation are still required [10]. The evolution of MIGS reflects the interaction between clinical need, patient-centered outcomes, and technological innovation [2]. With successive advances in laparoscopy, robotics, imaging, and AI, the scope and complexity of procedures that can be performed through minimally invasive approaches have progressively expanded [1,11]. Important uncertainties remain regarding long-term outcomes, equitable access, and cost-effectiveness, highlighting the need for further research [9,12].
Objectives of the review
This narrative review evaluates major technological domains in MIGS-laparoscopy, robotic-assisted surgery, NOTES/SILS, advanced imaging and energy devices, and emerging AI-enabled tools. Primary outcomes include perioperative safety and recovery (complications, pain, and length of stay), with secondary emphasis on training requirements, cost-effectiveness, and global access.
Methods
This is a qualitative narrative review article carried out according to a structured and transparent literature search. The electronic database search was done in the electronic databases of MEDLINE, Scopus, Web of Science, and the Cochrane Library, and articles published in peer-reviewed journals between January 1, 2015, and December 31, 2025. The search keywords and subject headings included “minimally invasive surgery,” “laparoscopic,” “robotic surgery,” “NOTES,” “single-incision,” “energy devices,” “fluorescence imaging,” “artificial intelligence,” “general surgery,” and “surgical outcomes.” Only human studies in the English language are considered.
The types of eligible studies were clinical trials, systematic reviews, meta-analyses, and large observational trials on MIGS procedures or enabling technologies (colorectal, hepatopancreatobiliary, bariatric surgery, and hernias). Conference abstracts without full texts or non-peer-reviewed literature were excluded. Titles and abstracts were checked to ensure relevance. Potentially eligible sources were examined in full text. Two authors worked independently to verify all sources and resolve any emerging differences. The need to address diversity in procedures and study designs required that results be presented thematically and narratively. Given the narrative design and heterogeneity in study designs and procedures, formal study-level risk-of-bias tools were not applied. Certainty-of-evidence grading frameworks such as GRADE (Grading of Recommendations Assessment, Development, and Evaluation) were not performed. Findings are therefore presented descriptively without quantitative synthesis or formal certainty grading.
Review
Evolution of MIGS
MIGS has gained traction among various domains of general surgery, primarily because of superior perioperative recovery compared to traditional open methods, which easily make it a preferred option for many surgeons [13]. The advancement of MIGS continues with developments in visual technology, instruments, and equipment [14]. The quest for alternatives that would decrease surgical trauma without sacrificing results led the way to minimally invasive surgery. The advent of laparoscopic cholecystectomy in the late 1980s was a turning point [15]. It offered persuasive evidence that intra-abdominal surgery could be done safely with minimal incisions and video guidance [16]. The early benefits reduced morbidity, quicker recovery, and enhanced patient satisfaction triggered instant propagation of the method globally. Laparoscopic methods rapidly became standard for appendectomy, hernia repair, and colorectal surgery, transforming both clinical practice and surgical education [17].
This initial phase of MIGS was marked by incremental but necessary advancements. Progress in optics and camera design enhanced resolution and illumination, compensating for the depth-perception limitations of 2D visualization in surgery [18]. Miniaturization of instruments widened procedural possibilities, as training simulators and credentialing systems facilitated surgeon proficiency [19]. Initial doubt regarding oncological sufficiency increasingly dissipated as evidence mounted confirming similar oncologic outcomes in selected malignancies [20]. Therefore, the history of MIGS is an evolving process of interaction between technological advances, clinical acceptance, and cultural modification in the field of surgery [21].
Laparoscopic surgery: current standards and innovations
Laparoscopy remains the cornerstone of minimal invasive practice and remains the gold standard by which more recent modalities are measured [22]. The technique's principle of entering the peritoneal cavity via small portals but using video-mediated visualization as a source of information has pervasively found its use across general surgery domains, from elective cholecystectomy to emergency appendectomy to complex colorectal resections [23]. At its core has been a continued advancement in visualization. Evolution from early fiber-optic technology to high-definition and now 3D systems has critically increased anatomical accuracy and depth perception [14]. Emerging technologies such as wide-angle and flexible-tip laparoscopes continue to increase access to deep or restricted anatomical regions, reducing operative complexity [24].
Concurrent developments in energy instruments and equipment have also been crucial. Bipolar devices, ultrasonic shears, and integrated vessel-sealing systems provide effective hemostasis and tissue division, reducing operative time and intraoperative hemorrhage [25]. With hernia repair, self-fixating meshes and atraumatic fixation techniques have improved long-term results with decreased postoperative pain [26]. The clinical advantages of laparoscopy are repeatedly proven in comparative trials. Throughout numerous procedures, patients suffer less pain, have fewer infections, mobilize earlier, and are discharged earlier than with open surgery [27]. Long-term results, e.g., oncologic safety in colorectal cancer or sustained weight loss in bariatric surgery, also prove its effectiveness [20]. Notably, laparoscopy has made Enhanced Recovery After Surgery (ERAS) pathways possible, allowing day-case procedures in appropriately chosen cases and decreasing the strain on healthcare systems [23].
However, there are constraints. Expertise in complex laparoscopic operations requires extensive training, and the acute learning curve still limits availability in low-resource environments where mentoring and simulation are less readily accessible [19]. The cost of equipment, while below that of robotics, still presents difficulty for hospitals with limited budgets [28]. Amid these impediments, however, laparoscopy's established interplay of efficacy, safety, and relative value guarantees its ongoing status as the worldwide standard in MIGS. The essential principles, innovations, and limitations of laparoscopy are summarized in Table 1.
Robotic-assisted surgery
Robotic-assisted surgery is an increasing part of the spectrum of MIGS and has potential benefits for certain technically challenging operations; however, its clinical value is limited to specific operations and dependent on cost, availability, and the strength of evidence [29]. With the introduction of platforms such as the Da Vinci platform came 3D visualization, tremor removal, and wristed instruments superior to the traditional laparoscopy, without the constraint of rigidity [18]. These features may improve dexterity and precision, particularly in anatomically constrained operative fields where conventional laparoscopy is limited [22]. The benefits of robotics are optimally observed in advanced procedures. In colorectal surgery, robotic technology enables deep pelvic dissections with improved nerve preservation [30]. In bariatric and upper gastrointestinal (GI) surgery, they provide improved precision in anastomotic creation. Similarly, in hepatobiliary and pancreatic surgery, robotics extends the range of minimally invasive resections that were hitherto possible only through an open approach [20]. Surgeons also have improved ergonomics, reducing fatigue for lengthy procedures [31].
However, these advancements are accompanied by significant and complex challenges. The first is cost: acquisition and maintenance are significantly higher than with laparoscopy, and there are implications for cost-effectiveness, particularly in resource-limited settings [32]. There are inequalities in access, with robotic platforms concentrated in tertiary institutions of the developed world, therefore limiting global equity [29]. In addition, while more technical stress can be eliminated with the use of robotics, it is impossible to eliminate the learning curve; ordered training and institutional support for safe practice are still required [19]. Comparative evidence between robotic and laparoscopic outcomes remains inconclusive. While robotics has seen equivalence or minor superiority in some areas, such as low conversion rates in rectal cancer resections, good randomized controlled trials remain rare [31]. The current literature is biased toward single-institution reports and retrospective review, and robust randomized controlled trials are needed before making blanket statements of superiority [28].
Competition and technological integration can determine the future direction of robotic surgery. Upcoming platforms with modular designs, smaller footprints, and haptic feedback incorporated are on the horizon and have the potential to reduce cost and enhance tactile control [33]. Robotics combined with digital technologies like AI, AR, and high-resolution imaging also promises that the long-term value of robotics is not only in dexterity but also in being a data-driven surgical system [34]. Robot-assisted surgery offers major advances, while also raising fundamental questions regarding value, access, and the strength of the supporting evidence. While it has already made its place in high-volume centers and complicated cases, it will be dependent on cost-cutting, innovation in training, and strong multicenter trial validation for its adoption into general surgery.
NOTES and SILS
The desire to make truly scarless surgery a reality has led to the development of NOTES and SILS [35]. These approaches were developed to reduce trauma to the abdominal wall while optimizing cosmetic results and hastening recovery [36]. While both procedures are still less commonly used than traditional laparoscopy, they are significant steps forward for the development of MIGS [35]. NOTES uses natural orifices like the stomach, vagina, or rectum as portals of entry, thus avoiding the requirement for external incisions [37]. Early reports demonstrated feasibility in procedures such as cholecystectomy, appendectomy, and diagnostic laparoscopy, with proposed benefits including reduced postoperative pain, faster mobilization, and improved cosmetic outcomes [38]. However, widespread adoption into routine practice was initially limited by training requirements, equipment availability, and variable institutional capacity [35]. Key barriers to widespread NOTES adoption include reliable viscerotomy closure, infection risk, limited triangulation and traction with flexible endoscopes, and the absence of standardized instrumentation and training pathways [37]. Current clinical use remains selective, most commonly in hybrid NOTES approaches that combine endoscopic access with laparoscopic assistance to improve safety and procedural control [39]. Available evidence suggests feasibility in carefully selected cases, but consistent advantages over conventional laparoscopy have not been demonstrated across most general surgical indications, and uptake remains limited by technical complexity, learning-curve demands, and concerns regarding reproducibility and complication management [40].
SILS, on the other hand, adapts laparoscopy by focusing all the instruments through a single umbilical port [40]. By hiding the scar inside the navel, SILS provides better cosmesis with well-known laparoscopic equipment [38]. It has been used effectively for appendectomy, cholecystectomy, nephrectomy, and bariatric surgery [40]. Patient satisfaction is frequently reported, with higher satisfaction in studies where cosmetic outcomes are a primary patient priority [36]. NOTES and SILS face significant ergonomic and technical challenges despite these benefits [35]. Longer operating times and more challenging dissections are caused by instrument crowding, loss of triangulation, and limited range of motion. Although specialized ports and articulating instruments provide partial solutions, there is still a significant learning curve [38]. Available comparative studies have not consistently demonstrated superiority of NOTES over conventional multiport laparoscopy in key perioperative endpoints, including complication rates, operative time, and recovery metrics [10]. As a result, NOTES remains a selective or adjunctive approach rather than a routine mainstream technique.
Nonetheless, NOTES and SILS are still driving innovation in closure technology, flexible endoscopy, and instrument design [37]. The patient-directed component is equally significant: even in cases where clinical outcomes are comparable, there is a strong demand for scarless solutions [39]. Future development of these methods is likely to involve hybrid integration of advanced imaging and robotic platforms to enhance precision while preserving cosmetic outcomes and procedural safety [35].
Progress in energy devices and instrumentation
Beyond innovations in access routes, developments in energy technologies and instrumentation have also had a significant impact on minimally invasive surgery. Effective dissection and hemostasis are critical determinants of surgical safety and effectiveness, and modern ultrasonic, bipolar, and vessel-sealing technology has transformed these capabilities [25]. Ultrasonic shears use high-frequency vibration to dissect and coagulate tissue, enabling precise dissection with minimal lateral thermal spread. Their use has been associated with reduced blood loss and shorter operative time in procedures such as cholecystectomy and colectomy [25]. Contemporary advanced bipolar vessel-sealing platforms incorporate real-time feedback mechanisms to regulate energy delivery and standardize sealing performance [25]. In clinical practice, these systems are primarily intended to support effective hemostasis and operative efficiency, with potential implications for intraoperative blood loss and procedure duration, although outcome benefits may vary by procedure and study design [24].
The integration with robotic systems has broadened their application and allowed surgeons to take advantage of enhanced dexterity along with effective energy transmission [28]. During hepatobiliary, bariatric, and colorectal procedures, this combination has enhanced surgical confidence in handling fine dissections as well as vascular structures [28]. In addition to energy devices, laparoscopic instrumentation itself has progressed significantly. Articulating and wristed instruments solve the ergonomic problem in SILS and deep pelvic surgery, whereas advanced stapling devices ensure uniform compression and lower leak rates in GI anastomoses [28]. Together, these have all served to shorten operative time, improve reproducibility, and enhance safety [22].
But there are still challenges. The cost of disposable devices raises concerns regarding cost-effectiveness, particularly in low-resource settings. Although some economic evaluations indicate decreased total costs as a result of fewer complications and lower hospital stays, these advantages are typically best realized in high-volume institutions [28]. Dependency on expensive disposables runs the risk of exacerbating surgical service disparities in low- and middle-income countries [22]. Therefore, further development of reusable or less expensive devices is required to spread the advantages of these technologies across the globe.
Advanced imaging and visualization methods
Visualization is central to minimally invasive surgery, and advances in optical technology have progressed alongside improvements in access and instrumentation [41]. From early 2D laparoscopy to today's high-definition and 3D technology, each leap forward in visualization has enhanced minimally invasive procedures' safety and scope [22]. Emerging technologies, including near-infrared fluorescence imaging, AR, and VR, are further expanding the technical capabilities and applications of minimally invasive surgery. Near-infrared fluorescence imaging using ICG has gained widespread application in hepatobiliary and colorectal surgery [20]. ICG aids in demarcating biliary anatomy, vascular perfusion, and lymphatic tracts intraoperatively, enhancing surgical precision and reducing complications. For example, fluorescence angiography during colorectal surgery has been reported to be associated with lower anastomotic leak rates, although findings vary across procedures and clinical settings [20]. In hepatobiliary surgery, ICG fluorescence can improve visualization of biliary anatomy and may be associated with a reduced risk of bile duct injury [42]. These applications suggest a potential safety benefit of enhanced imaging, while acknowledging that causal inference cannot be assumed.
AR and VR are newly emerging technologies in minimally invasive surgery [43]. Current uses of these technologies include simulation, anatomy visualization, and intraoperative assistance. However, extensive usage of these technologies is restricted by regulatory clearance, financial constraints, and results [44]. AR can allow surgeons to superimpose preoperative imaging reconstructions over the field, enabling more precise localization of tumors and vascular structures. This is especially useful for oncologic resections where margin status is key [21]. VR, on the other hand, has already been invaluable for training and rehearsal [45]. Patient-specific VR models enable surgeons to practice procedures, optimizing preparation for cases with complicated anatomy and decreasing intraoperative uncertainty. Image-guided navigation systems provide additional potential by combining preoperative imaging with intraoperative data, generating dynamic surgical maps [46]. Uses in liver and pancreatic surgery indicate margin clearance improvement and intraoperative blood loss reduction [20].
Even with these advances, there are limitations. Fluorescence imaging is operator-dependent, and standardized interpretation pathways are still being developed. AR and VR technologies are costly infrastructure investments and are not yet universally available outside of specialized centers [47]. Additionally, the strength of available evidence varies, with a substantial proportion derived from preliminary, single-center, or non-randomized studies rather than large multicenter randomized trials. Even with these challenges, enhanced imaging holds clear potential to transform both intraoperative decision-making and surgical education [21]. As integration with robotics, AI, and energy devices matures, visualization will increasingly function not merely as a tool for seeing but as a platform for real-time guidance, assessment, and planning [34]. Key advances in imaging and visualization for MIGS are summarized in Table 2.
AI and machine learning applications
AI and machine learning (ML) have become increasingly integrated into medical practice, including surgical care [35]. In MIGS, these technologies hold the potential to enhance surgeon performance, improve intraoperative decision-making, and develop new paradigms for individualized care [10]. While still at the beginning stages of their integration in the clinical field, applications of AI and ML are already transforming surgical training, operation planning, and outcome prediction [11].
The use of AI in minimally invasive surgery is growing, especially in surgical video analysis, where huge volumes of operative footage can be objectively evaluated to evaluate the steps of the procedure and the mastery of technical skills [11]. Initial investigations indicate that algorithmic measures of skills and errors can be related to expert rating and could be used to provide structured feedback and competence training, but the majority of findings are retrospective and reliant on curated datasets, and there is little external verification [11]. Real-time anatomy recognition, instrument, and complication-risk prediction are intraoperative decision-support applications that are still in the research and development phase and are not yet fully integrated into regular clinical processes [3]. Despite the computer vision models that are currently in development in order to assist tasks like biliary anatomy identification during laparoscopic cholecystectomy, clinical efficacy in minimizing bile duct injury has not been proven consistently in a prospective multicenter study [42]. In the same regard, predictive analytics of bleeding or anastomotic leak risks are also limited by data bias, poor generalization, regulatory restrictions, and the assimilation of the operating room setting [12].
Outside the operating room, surgical planning is being increasingly augmented by AI. ML algorithms can incorporate patient-specific information such as imaging, comorbidities, and genomic data to inform procedure choice and predict risk [34]. Such personalized care may facilitate patient counselling, maximize resource utilization, and enhance long-term results [2]. There are challenges to implementing AI in surgery, however. The quality and diversity of training datasets also affect algorithm performance, making it susceptible to bias and lacking in generalizability [12]. Strong computational hardware and seamless integration into clinical workflows are also necessary for real-time use [3]. Uncertainty surrounds ethical issues like data security and the medicolegal implications of algorithmic recommendations. Multidisciplinary collaboration between surgeons, data scientists, and policymakers will be essential for AI to reach its full potential in MIGS [11].
Patient outcomes and quality of life
The main motivating force for minimally invasive surgery has always been improved patient outcomes [4]. Evidence always indicates that MIGS has clear advantages over open surgery in terms of less morbidity, faster recovery, and improved quality of life (QoL) [2]. These benefits cross both short-term perioperative outcomes and long-term functional and psychosocial outcomes [4]. During the acute postoperative phase, MIGS is preceded by less pain, reduced surgical site infection incidence, and shorter length of hospital stay [14]. Faster mobilization and earlier oral feed are components in the pathway of enhanced recovery protocols, which decrease healthcare utilization and cost [24]. These are particularly precious to working-age patients, where sooner return to normal activity means socioeconomic advantage.
Long-term outcomes are also convincing. For oncologic surgery, evidence exists that laparoscopic and robotic surgery are oncologically equal to open surgery according to margin status, lymph node yield, and survival [6]. The functional outcomes are also better. As an example, minimally invasive rectal surgery has been linked with better preservation of urinary and sexual functions due to improved visualization and precision during deep dissections in the pelvis [30]. Similarly, in bariatric surgery, minimally invasive approaches achieve long-term weight loss and comorbidity remission with reduced perioperative morbidity compared with traditional open methods.
QoL is a complex concept that encompasses not only physical recovery but also psychological functioning and satisfaction with the patient [4]. MIGS is beneficial as it reduces scarring, decreases chronic pain, and facilitates quicker return to social and vocational activities [2]. Patient-reported outcome measures always reflect greater ratings for satisfaction with minimally invasive approaches, particularly in younger populations who are more fixated upon cosmesis and independence. However, results are not always optimal. Availability of sophisticated minimally invasive technology is unequal, with variation between high- and low-income areas [9]. In addition, MIGS benefits depend on surgical skill: inappropriate training or incompetent case selection can reverse benefits and boost complications [24]. Therefore, although the evidence unequivocally supports MIGS in enhancing patient outcomes, guaranteeing universal delivery of these benefits involves equal access, rigorous training, and uniform quality assurance [9].
Training, simulation, and skill acquisition
The accelerating growth of MIGS has created new challenges for surgical education [11]. In contrast to open surgery, where direct visualization and tactile feedback control techniques are used, minimally invasive surgery demands proficiency in indirect visualization, instrument use within limited spaces, and dependency on sophisticated technologies [3]. In consequence, conventional apprenticeship models are inadequate to guarantee safe and effective training [19]. VR and AR simulators have proven to be valuable tools for skill acquisition [45]. The simulators model the operating environment with high fidelity, and trainees are able to rehearse procedures in a risk-free environment [18]. Simulator-based training has been demonstrated to enhance technical competence and decrease rates of error during actual procedures [45]. Furthermore, VR allows objective measurement of performance metrics like precision, economy of motion, and time to complete the procedure, facilitating competency-based curricula [45].
Simulation also enables training in low-frequency or high-consequence situations [14]. For instance, intraoperative hemorrhage control or complex reconstructions can be performed repeatedly, incrementally building confidence and preparedness for actual use [48]. AR systems provide additional benefit by superimposing anatomical landmarks and step-by-step procedural instructions during both simulation and live procedure, improving spatial awareness and minimizing cognitive burden [43]. Global differences in training and accreditation underscore the necessity for uniform curricula [19]. Whereas high-income nations more fully incorporate simulation into residency training, lower-resource regions are disadvantaged by cost, infrastructure, and expertise of faculty [49]. International networks and open-access training websites can bridge such differences and lead to greater global equality in the acquisition of skills [5].
Conquering the learning curve in MIGS mandates formal pathways blending simulation, supervised operative training, and continuing evaluation [22]. Competence must be measured not solely on case volume but on proven proficiency against uniform benchmarks [50]. With advancing technology, ongoing professional development is as crucial, preserving established surgeons' proficiency in using robotics, AI, and imaging [34]. Training strategies and simulation methods in MIGS are outlined in Table 3.
Cost-effectiveness and healthcare system implications
The economic considerations of minimally invasive surgery underlie its sustainability and global spread [51]. Although MIGS has robustly established clinical advantages, the costs incurred, especially for sophisticated platforms like robotics, are threats to healthcare systems, particularly in low-resource environments [52]. Comparative studies invariably show that traditional laparoscopic surgery is less expensive compared to open surgery, mainly because it involves reduced hospitalization time, fewer complications, and quicker return to productivity [53]. These savings commonly pay for the higher initial cost of laparoscopic technology. By contrast, the economics of robotic surgery are disputed [54]. Although robotics has been demonstrated to improve results and lower conversion rates in specific complex procedures, its acquisition and maintenance costs are significantly higher than those of laparoscopy. Analyses of cost-effectiveness have produced conflicting findings, with benefits being more noticeable in institutions with high volume and optimized use [55].
For middle- and low-income countries, cost barriers are stronger [54]. Inadequate infrastructure, excess cost of equipment, and lack of trained staff act as barriers to adoption, leading to unequal access to highly developed care. Investment in cost-efficient laparoscopic programs, therefore, might achieve more population-level gains than early adoption of robotics in those environments [56]. However, with competition among manufacturers on the rise and modular robotic platforms being developed, costs will come down, and access will increase with the passage of time [57].
Health systems also need to reconcile innovation with equity [58]. Unwavering enthusiasm for expensive technology may exacerbate disparities, pull resources from needed services, and restrict access to marginalized groups. Policymakers must navigate how to nurture innovation while promoting equitable distribution of benefits [58]. Value-based models that balance clinical results and societal costs offer a helpful template for steering adoption [55]. Lastly, MIGS's financial viability depends on striking a balance between the demands of the health system and technological innovation [52]. This entails making strategic investments in infrastructure, training, and access, in addition to cutting costs through innovation and competition [57]. Only by responding to both clinical and financial aspects is minimally invasive surgery able to realize its potential for improving surgical care worldwide.
Limitations and future recommendations
Although there is a substantial body of evidence supporting MIGS, there are also important limitations. Numerous studies have heterogeneity in design, outcome reporting, and follow-up interval, making meta-analyses difficult and consensus challenging. Limitations such as small sample size, publication bias, and varying definitions of success reduce the strength of the available evidence. For more recent technologies like robotics, fluorescence imaging, and AI, longer-term outcome data are limited, making consideration of durability, cost-effectiveness, and true clinical benefit challenging. Economic constraints also remain a continuing obstacle: high-end platforms remain concentrated in affluent areas and demonstrate global disparities in access.
Future growth will be based on an even more harmonized and evidence-driven strategy. Appropriately powered multicenter randomized controlled trials with standardized endpoints will be needed to determine comparative efficacy in various populations. Innovations will need to be designed with affordability and scalability in mind to avoid expanding inequities. Digital technologies such as AI and AR need to be not only thoroughly tested but also translated into clinical practice workflows from a perspective of regulatory and ethical compliance. Equally vital is the harmonization of surgical education and accreditation worldwide, so that technological advancement is transferred into consistent, fair outcomes for patients.
Conclusions
MIGS has transformed from early laparoscopic pioneering to an advanced, high-technology discipline involving robotics, high-tech imaging, precision energy devices, and digital technologies. This narrative review provides a novel contribution through the integration of several aspects of technical innovation, patient outcomes, training, and economic considerations into a critical overview with a description of the present state and future direction of the discipline. The advantages of minimally invasive methods with regard to reduced morbidity, quicker recovery, and improved QoL have been well established; however, methodological heterogeneity, lack of long-term data, very high costs, and uneven access worldwide remain significant barriers to global acceptance. Notably, the promise of MIGS in the future will be dictated not only by technological innovation but also by its application to sustainable, equitable, and ethically responsible healthcare systems. Success will rely on solid multicenter trials, standardized training systems, and the pairing of innovation with affordability to avoid exacerbating disparities. By setting forth MIGS as a clinical and societal endeavor, this review highlights that its long-term success will be determined by providing safe, effective, and equitable surgery across the globe.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A new era of minimally invasive surgery: progress and development of major technical innovations in general surgery over the last decade Surg J (N Y) Siddaiah-Subramanya M Tiang KW Nyandowe M 063201710.1055/s-0037-1608651 PMC 568004629134202 · doi ↗ · pubmed ↗
- 2Minimally invasive gastrointestinal surgery: from past to the future Ann Med Surg (Lond) Rudiman R 1029227120213470358510.1016/j.amsu.2021.102922 PMC 8521242 · doi ↗ · pubmed ↗
- 3Medical technologies and challenges of robot-assisted minimally invasive intervention and diagnostics Annu Rev Control Robot Auton Syst Simaan N Yasin RM Wang L 46549012018
- 4Past, present, and future of minimally invasive abdominal surgery JSLS Antoniou SA Antoniou GA Antoniou AI Granderath FA 19201510.4293/JSLS.2015.00052 PMC 458990426508823 · doi ↗ · pubmed ↗
- 5Advancements in minimally invasive surgical techniques: a comprehensive review Salud Cienc Tecnol Ayme AP Suárez JM Ortega MM 74542024
- 6The Miami international evidence-based guidelines on minimally invasive pancreas resection Ann Surg Asbun HJ Moekotte AL Vissers FL 11427120203156750910.1097/SLA.0000000000003590 · doi ↗ · pubmed ↗
- 7Review of emerging surgical robotic technology Surg Endosc Peters BS Armijo PR Krause C Choudhury SA Oleynikov D 163616553220182944224010.1007/s 00464-018-6079-2 · doi ↗ · pubmed ↗
- 8Trends in the adoption of robotic surgery for common surgical procedures JAMA Netw Open Sheetz KH Claflin J Dimick JB 03202010.1001/jamanetworkopen.2019.18911 PMC 699125231922557 · doi ↗ · pubmed ↗