Completely thrombosed middle cerebral artery aneurysm mimicking cavernous malformation: illustrative case report with operative video and review of the literature
Beatrice Zucca, Marissa Koscielski, Aaron Kakazu, Sanjit Shah, Mary Gaskill-Shipley, Matthew Smith, Charles Prestigiacomo, Jonathan Forbes

TL;DR
A rare case of a completely thrombosed middle cerebral artery aneurysm was mistaken for a cavernous malformation and successfully treated surgically.
Contribution
This case report adds to the limited literature on the clinical presentation and surgical management of completely thrombosed middle cerebral artery aneurysms.
Findings
Five cases of completely thrombosed middle cerebral artery aneurysms were identified in the literature review.
Surgical management with ultrasonic evacuation and clip reconstruction was effective in treating the reported case.
Abstract
Complete aneurysmal thrombosis is a rare occurrence in which a combination of thrombus and plaque contributes to the complete obliteration of the lumen of an aneurysm, rendering it occult on angiographic imaging. To date, there is a paucity of information in the literature describing the clinical/radiographic presentation and operative management of complete thrombosed aneurysms of the middle cerebral artery. A focused literature review was performed to identify previously reported cases of complete MCA aneurysm thrombosis. Five cases meeting these criteria were identified, of which four underwent open microsurgical management and one was treated endovascularly. We report a clinical case of a 35-year-old female who presented with severe exacerbation of baseline headaches. Radiographic features were suggestive of a ruptured cavernous malformation. In the operating room, a large and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
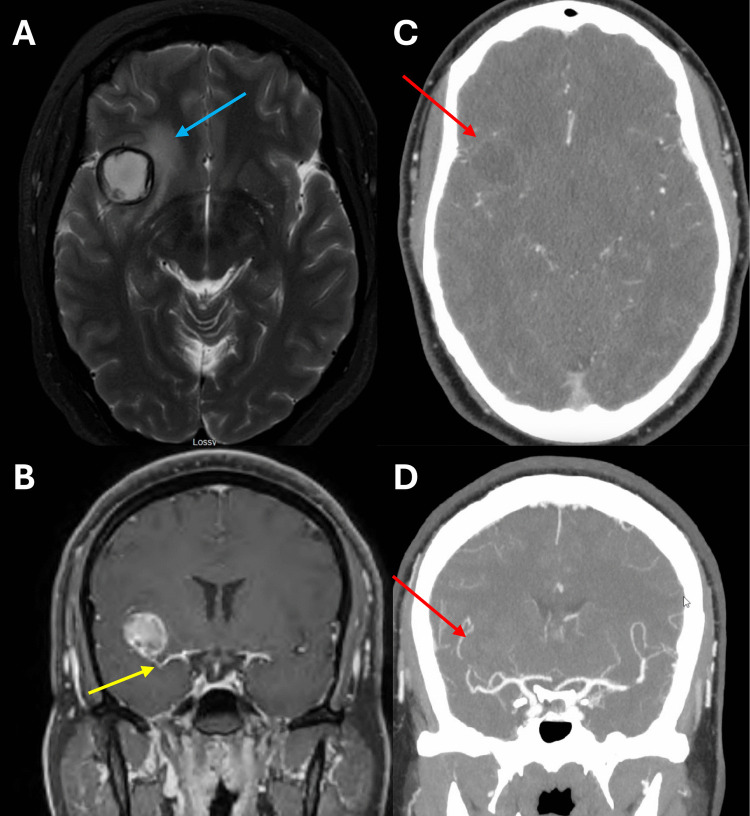 Figure 1
Figure 1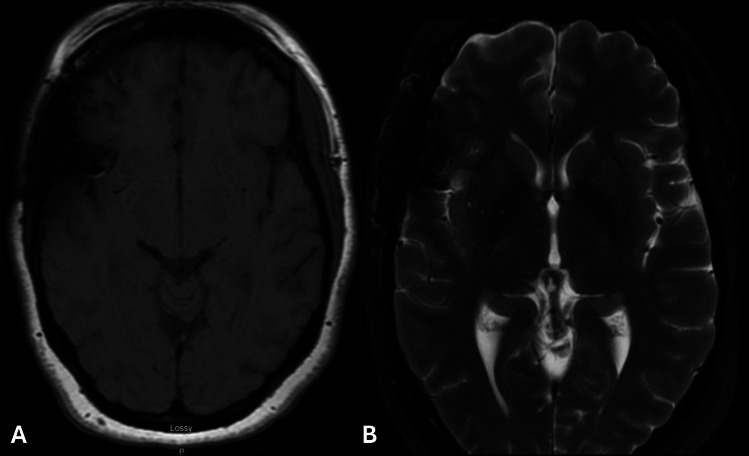 Figure 2
Figure 2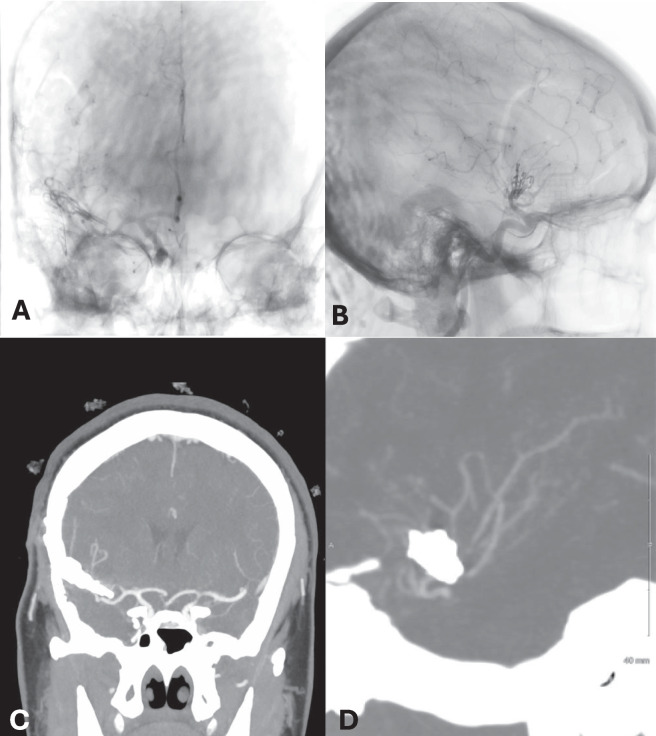 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntracranial Aneurysms: Treatment and Complications · Vascular Malformations Diagnosis and Treatment · Cerebral Venous Sinus Thrombosis
Introduction
Middle cerebral artery (MCA) aneurysms represent approximately 20–25% of all intracranial unruptured aneurysms (IUA) [3, 4]. Complete middle cerebral aneurysmal thrombosis is a rare occurrence whereby a combination of thrombus and plaque contributes to the complete obliteration of the lumen of an aneurysm, rendering it occult on angiographic imaging. While partial spontaneous thrombosis of cerebral aneurysms can occur in a small number of ruptured aneurysms and 10–30% of intracranial giant aneurysms (IGA), complete thrombosis of an MCA aneurysm is an exceptionally rare occurrence [2, 9]. As cerebral angiography by definition is unremarkable, completely thrombosed aneurysms are commonly mistaken for cavernous malformations (CCMs) or intra‑axial neoplasms on initial imaging.^.^ To date, only five reports of complete MCA aneurysm thrombosis have been documented in the literature. We present the case of a complete thrombosis of a superior M2 aneurysm that required ultrasonic removal of plaque and clip reconstruction for definitive treatment.
Case report
A 35-year-old woman presented to an outside emergency department with severe exacerbation of baseline headaches that started approximately 6 weeks before seeking medical consultation. Initial non-contrast CT was negative for subarachnoid hemorrhage but demonstrated a hypodense lesion adjacent to the right Sylvian fissure. CT angiography of the head was negative for evidence of aneurysm or vascular irregularity. The patient was ultimately discharged home with plans to obtain elective MRI imaging.
Outpatient MRI demonstrated a 2.3 cm rounded hemorrhagic lesion involving the right frontal opercular region and associated with minimal peripheral enhancement in post-contrast imaging. The hemorrhagic lesion involved the distal MCA bifurcation (Fig. 1). Pre-contrast T1 and T2-MRI weighted imaging defined a discrete hypointense rim and considerable peri-lesional edema. Following discussion in a multi-disciplinary setting, radiographic features were thought to be most consistent with a ruptured cavernous malformation. The possible etiology of complete thrombosis of MCA aneurysm was discussed, although it was deemed significantly less probable. Pre-operative diagnostic cerebral angiography (DSA) was not performed. Ultimately, a right frontotemporal craniotomy for definitive treatment was advocated. Intraoperatively, a large, completely thrombosed aneurysm of the superior M2 was encountered (operative video available in the Supplementary Material). The blood pressure was augmented in preparation for temporary clipping. Proximal and distal vascular control of the superior M2 was obtained with temporary clips. The aneurysm wall was opened sharply and treated with ultrasonic evacuation of thrombus and plaque followed by clip reconstruction. As motor-evoked potentials (MEPs) and somatosensory evoked potentials (SSEPs) remained stable until the end of the procedure, the temporary clips were only removed a single time to allow for reperfusion (with total temporary occlusion time of 17 minutes). After a very brief decline near the end of the phase of clip reconstruction, MEPs and SSEPs returned completely to normal after removal of temporary clips. Two long straight clips were used to disconnect the lumen of the aneurysm from the superior M2; these were buttressed by two fenestrated clips for circumferential vessel wall reconstruction. Subsequently, the dome of the aneurysm was sharply disconnected from the reconstructed aneurysm neck to de-vascularize the living aneurysm wall. Indocyanine Green (ICG) and doppler ultrasound confirmed appropriate preservation of the parent and daughter branches. At the completion of the procedure, all neuromonitoring signals were noted to be intact.Fig. 1. Pre-operative brain imaging demonstrates perilesional edema (blue arrow) on axial T2- weighted MRI of the brain (A), and post-contrast T1-weighted MRI (B) reveals involvement of the distal MCA bifurcation (yellow arrow). Axial (C) and coronal (D) CTA show no evidence of vascular irregularity (red arrows)
The patient had an uncomplicated postoperative course and was discharged home. At the three-month follow-up, she was neurologically intact and reported considerable improvement in baseline headaches. Post-clip MRI demonstrated resection of the T1 hyperintense focus with complete resolution of perianeurysmal T2 hyperintensity. (Fig. 2). Routine post-operative DSA performed in the elective setting following treatment demonstrated complete preservation of the parent and daughter vasculature (Fig. 3A-B). Post-operative CT angiogram obtained 2 years following treatment again demonstrated preservation of the parent and daughter vasculature with no evidence of aneurysm recurrence (Fig. 3C-D). This case highlights the diagnostic challenges and intraoperative findings posed by completely thrombosed aneurysms, which are angiographically occult and often misidentified before surgery. Full patient consent for photography and/or recording was obtained in the preoperative period.Fig. 2. Post-operative brain imaging obtained two months after surgery demonstrates complete resection of the hyperintense lesion on axial T1-weighted MRI (A), while axial T2- weighted MRI (B) shows resolution of the perilesional edemaFig. 3Post-operative DSA demonstrates complete preservation of flow of the reconstructed superior M2 division without luminal compromise or irregularity (A-B). 2-year post-operative coronal (C) and sagittal (D) CTA demonstrated preservation of the parent and daughter vasculature with no evidence of aneurysm recurrence
Discussion
Physiologically, aneurysm thrombosis is caused by low shear rates and the suppression of pulsatile flow, resulting in a procoagulant milieu. Complete aneurysmal thrombosis is a rare occurrence whereby a combination of thrombus and plaque contributes to the complete obliteration of the lumen of an aneurysm, rendering the lesion occult on angiographic imaging. The rarity of complete aneurysmal thrombosis, as well as the essential role angiographic imaging routinely plays in the diagnosis of aneurysmal pathology, makes accurate diagnosis of completely thrombosed aneurysms extremely challenging. Notably, in the existing reports detailing complete thrombosis of an MCA aneurysm, the majority of the lesions were misclassified as either cavernous malformations or intra-axial neoplasms prior to surgical intervention.
Given the inability to rely on angiographic imaging in the diagnosis of complete aneurysmal thrombosis, other radiographic features must be evaluated by the neurosurgeon. As a general recommendation, any time a lesion of unusual radiographic characteristics is found in a fissure or cistern typically occupied by large or medium sized vessels, the diagnosis of aneurysmal thrombosis should remain on the differential—even if angiographic imaging is negative. CT imaging of completely thrombosed aneurysms can reveal specific features such as peripheral ring enhancement, curvilinear mural calcifications, or heterogeneous high-density attenuation within the aneurysmal lumen. MRI features can sometimes include “onion skin” appearance due to layered signal intensities, heterogeneous signal within the lumen consistent with hemorrhage of different ages, marginal contrast enhancement involving the aneurysmal wall, and perianeurysmal edema on T2-weighted sequences [1, 7]. High-resolution vessel wall MR imaging, an emerging radiographic technique able to detect instability or inflammation within the vessel wall with higher sensitivity than traditional forms of MR imaging alone, was unfortunately not obtained in this case. However, the presence of marginal wall enhancement noted on traditional MR imaging was in hindsight perhaps indicative of an active biological process involving the arterial/aneurysm wall. While there is limited available data on the utility of high-resolution vessel wall MR imaging in the setting of completely thrombosed aneurysms, this technology offers hypothetical promise [7, 11]. As CT, MRI, and angiographic findings in thrombosed aneurysms are rarely pathognomonic, the surgeon must maintain a high index of suspicion for an accurate pre-operative diagnosis. Importantly, completely thrombosed aneurysms retain the potential to recanalize and evolve into partially thrombosed aneurysms, a configuration known to carry a significant risk of rupture. Prior studies have documented this phenomenon with systematic reviews reporting recanalization rates of up to 33% in non‑giant aneurysms, thereby underscoring the fact that thrombosis alone does not eliminate future instability [1].
The overwhelming majority of documented cases of aneurysm thrombosis in the literature involve partial or subtotal thrombosis. To date, only five cases of complete MCA spontaneous thrombosed aneurysms have been reported in the literature. Four of these cases were discussed in a review of the literature by Scerrati et al. that identified 94 cases of MCA aneurysms associated with some element of thrombosis [1, 5, 6, 8]. As an example of the rarity of completely thrombosed MCA aneurysms, 96% of the cases in the Scerrati report represented partially-thrombosed aneurysms [10].
Clinical and radiographic summaries of the five existing cases of completely thrombosed MCA aneurysms can be found in Table 1. Despite attainment of multiple imaging studies, three of the five cases were initially misdiagnosed, with one case classified as an intra-axial neoplasm and another case misdiagnosed as a cavernous angiomas. The results of open neurosurgical intervention for completely thrombosed aneurysms, performed in four of the five cases, demonstrate the complexity and morbidity associated with treatment of these lesions. In two of the four cases treated with open surgery, the identified aneurysm could not be clipped successfully and was treated with wrapping. In the remaining two cases treated with open microsurgery, one patient was treated with resection of the aneurysm and sacrifice of two daughter vessels. The other patient underwent partial debulking of the aneurysm with failure to definitively treat with clip reconstruction. In four of four cases of complete aneurysm thrombosis requiring open microsurgical intervention, aneurysm management was suboptimal with either incomplete treatment or daughter vessel sacrifice. In three of these four cases, suboptimal outcomes were at least partially attributed to the failure to recognize the aneurysm preoperatively. Review of these cases emphasizes the significance of accurate preoperative identification, as the primary therapeutic objective is complete aneurysm obliteration while preserving the flow of the parent and branching vessels. Table 1. Completely thrombosed MCA aneurysmsAuthor, YearSex/AgeSymptomsImagingAneurysm LocationInitial MisdiagnosisTreatmentPre-Operative DiagnosisOperative OutcomeLenthall, 2001F/36Migraine, right-sided sensory weaknessDSA, MRIM2 segmentNUnable to clip partially thrombosed aneurysm; aneurysm wrappedPartially thrombosed MCA aneurysmPost-operative MRI demonstrated spontaneous progression to complete aneurysm thrombosis, patient subsequently observed Cohen, 2003M/25Sudden headache and left arm weaknessCTA and DSAMCA bifurcationYSurgical intervention + endovascular embolizationIntracranial hemorrhage; Blister-like dilatation at MCA bifurcation of uncertain etiologyUnable to clip initially. Clipping aborted, wrapped with gauze. Aneurysm eventually recanalized requiring embolization Kim, 2014M/58Headache and dizzinessCTA and DSAProximal MCANEndovascular embolization after recanalization noted on DSA 2 months laterMCA aneurysmInitial coil embolization aborted after aneurysm found to have completely thrombosed; subsequentcoil embolization performed after aneurysm found to recanalize Nguyen, 2015F/43Generalized tonic–clonic seizureMRI, CTA and DSAMCA (not specified)YSurgical interventionIntra-axial neoplasmResection of aneurysm with sacrifice of two distal vesselsSoler-Rico, 2023M/40Transient left hemiparesis and hypoesthesiaCTA and MRIDistal MCAYSurgical interventionCavernous angiomaAneurysmal sac incision and partial debulking; unable to clip reconstruct; patient subsequently observedPresent caseF/35Exacerbation of baseline headacheCTA and MRIDistal M2 bifurcationYSurgical interventionCavernous angiomaAneurysm clipping with ultrasonic evacuation of thrombus
Consideration should be given to treatment of completely thrombosed MCA aneurysms, as they remain at risk for potential recanalization, instability, and delayed rupture. Given the small number of existing reports of completely thrombosed aneurysms, optimal treatment strategies are uncertain. Because these lesions are associated with complete angiographic obliteration of the lumen, endovascular intervention is not possible in the absence of delayed recanalization. Complete flow arrest with evacuation of plaque and thrombus and vessel wall reconstruction is thought to be an adequate management strategy that was successful in the index patient presented. Trapping of the aneurysm with bypass is an alternative strategy that may be associated with a lower risk of recurrence as compared to clip reconstruction alone. However, trapping and bypass requires extensive preparation and planning which is sometimes not possible due to many completely thrombosed aneurysms not being correctly diagnosed prior to operative exploration.
Conclusions
Complete thrombosed aneurysms are challenging lesions that are commonly misdiagnosed prior to operative exploration. Surgeons must be conscious of the limitations of pre-operative imaging in identifying completely thrombosed aneurysms and be prepared to treat these lesions effectively when encountered.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 Narrative video illustrating the surgical procedure (MP4 446137 KB)