Sustaining stewardship: longitudinal evaluation of an integrated antimicrobial programme in the ICU
Ashmitha Thomas, Sara Vogrin, Adele Batrouney, Misha Devchand, Sharmila Khumra, Shanti Narayanasamy, Satwik Motaganahalli, Jason A Trubiano, Stephen J Warrillow, Gemma K Reynolds

TL;DR
This study shows that an antimicrobial stewardship program in an ICU can be sustained over 7 years, reducing the use of broad-spectrum antibiotics while maintaining high acceptance of recommendations.
Contribution
The study provides a longitudinal evaluation of an integrated electronic medical record-driven antimicrobial stewardship program in an ICU.
Findings
High acceptance rates of AMS recommendations were observed, especially for antibiotic escalation.
Antimicrobial consumption for broad-spectrum antibiotics like meropenem and vancomycin significantly decreased post-implementation.
Compensatory prescribing was noted with increased use of amoxicillin/clavulanate.
Abstract
To evaluate the long-term sustainability and impact of an integrated electronic medical record–driven antimicrobial stewardship (AMS) ward round in an ICU at a tertiary referral hospital. The study assessed antimicrobial prescribing patterns, acceptance of stewardship recommendations, and antimicrobial consumption over 7 years. A prospective review commenced with implementation of the ICU-AMS ward round at Austin Health in 2017. When AMS recommendations were given, data were collected including patient demographics, antimicrobial prescribing, classification of recommendation, and acceptance. Antimicrobial use was assessed via DDDs per occupied bed day per month and analysed using interrupted time series analysis. Logistic regression examined patient and clinician factors associated with recommendation acceptance. Over 7 years, 9163 AMS recommendations were made for 4610 patients.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
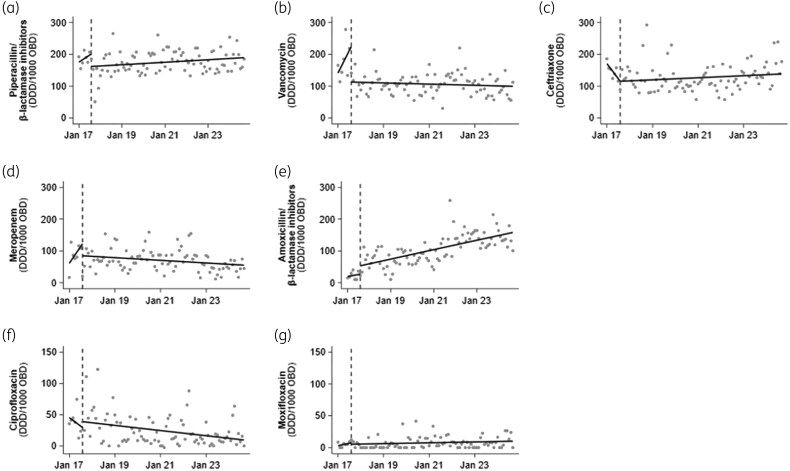 Figure 1
Figure 1| AMS moments | Recommendations, | Accepted, |
|---|---|---|
| Escalation | 873 (9.5) | 827 (94.7) |
| De-escalation | 1500 (16.4) | 1300 (86.7) |
| Discontinuation | 3958 (43.2) | 3257 (82.3) |
| Switch | 951 (10.4) | 793 (83.4) |
| Optimization | 1881 (20.5) | 1604 (85.3) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Use and Resistance · Urinary Tract Infections Management · Infection Control in Healthcare
Introduction
Antimicrobial stewardship (AMS) programmes in intensive care units (ICUs) reduce broad-spectrum antibiotic use, the incidence of MDR pathogens, antibiotic-associated adverse effects, and healthcare-associated costs.^1^ In-person delivery and feedback contribute to sustained improvements in antimicrobial consumption and cost;^2^ however, the long-term sustainability and impact of such programmes in the critically ill or ICU are infrequently examined.
Methods
This study was approved by our institution’s Human Research Ethics Committee (HREC/98045).
Based on the principles of ‘Handshake Stewardship’, an ICU-AMS ward round was instituted at Austin Health in 2017 and remains a core AMS component at this 500-bed tertiary hospital. The model is defined by three key elements: (i) no restriction or preauthorization requirement, (ii) comprehensive review of all prescribed antimicrobials, and (iii) in-person feedback delivered by a pharmacist–physician team.^3^ As previously described, the ward round is conducted on weekdays and is integrated into the workload of the Infectious Diseases (ID) and ICU medical teams, and AMS pharmacist.^4^ The round involves asynchronous review via the electronic medical record (EMR) followed by in-person discussion in the ICU. All patients receiving antimicrobials, or for whom antimicrobials are being considered, are discussed. Whereas pharmacist input is integral to case review and medication optimization, stewardship recommendations are communicated by the ID clinician during the round. Recommendations are classified according to the internally developed ‘5 Moments of Antimicrobial Prescribing’: escalation, de-escalation, discontinuation, oral switch and optimization. This metric was created by internal consensus to provide a framework to assess AMS compliance.^4^
An initial evaluation conducted in the first 6 months of implementation assessed recommendation acceptance, target antibiotic use and prescribing appropriateness, with follow-up at 2 years reporting sustained changes in antimicrobial use and further improvements in appropriateness.^4,5^ Building on these early evaluations, we conducted a prospective study of the 7 year sustainability and impact of the integrated AMS service from August 2017 to December 2024. We also examined patient- and clinician-level social factors that may influence the uptake of ‘handshake stewardship’.
The primary outcome was antimicrobial consumption measured through the National Antimicrobial Utilisation Surveillance Program (NAUSP)—a volume-based method for monitoring and benchmarking use of antimicrobials between Australian hospitals, expressed as DDDs per 1000 occupied bed days (OBDs), calculated monthly.^6^ Institutional standard dosing regimens for target antimicrobials are summarized in Table S1 (available as Supplementary data at JAC Online). Changes in antimicrobial consumption over time were analysed using interrupted time series analysis using ordinary least squares regression with Newey–West standard errors.
Secondary outcomes included AMS recommendation type, classified by the ‘5 Moments’ framework,^4^ and acceptance by the ICU team within 24 h. Patient demographics and admitting unit were recorded. Immunocompromised patients were identified by admitting unit (liver and renal transplant, haematology, oncology, rheumatology). The relationship between acceptance of recommendation, and patient/clinician characteristics was analysed using univariable logistic regression, overall and separately for each type of recommendation. Standard errors were adjusted for clustering within the participant. Results are expressed as ORs with 95% CIs. All analyses were performed using Stata 18 (StataCorp LLC).
Results
The ICU-AMS service provided recommendations for 4610 patients during the study period. Median age was 62 years (IQR 50–73), with 60.2% male predominance (Table S2). Most patients were admitted under medical units (63.4%), and 835 (18.1%) were immunocompromised. Over a 7 year period (2017–2024) there were 1078 rounds, with an average duration of 30 min (IQR 25–40). The most reviewed antibiotics were piperacillin/tazobactam, ceftriaxone and vancomycin (1906, 1162 and 766 instances, respectively).
Antimicrobial consumption of target agents is shown in Figure 1. Additional consumption data are found in Table S3 and Figures S1 and S2. Prior to programme implementation in 2017, piperacillin/tazobactam use was rising (3.6 DDD/1000 OBD/month; 95% CI, 1.3–5.9; P = 0.003); post-intervention it decreased (−38.9 DDD/1000 OBD/month; 95% CI, −60 to 17.4; P = 0.001) without significant change in trend thereafter (0.32 DDD/1000 OBD/month; 95% CI, −0.01 to 0.7; P = 0.059). Meropenem use also decreased at implementation (−37.7 DDD/1000 OBD/month; 95% CI, −66.1 to 9.4; P = 0.01), with continued decline over subsequent years (−0.3 DDD/1000 OBD/month; 95% CI, −0.6 to 0.1; P = 0.021). Vancomycin use decreased immediately after programme commencement (−111.7 DDD/1000 OBD/month; 95% CI, −193.2 to −30.2; P = 0.008), with no significant change since (−0.2 DDD/1000 OBD/month; 95% CI, −0.4 to 0.1; P = 0.277). Ciprofloxacin showed a sustained reduction (−0.35 DDD/1000 OBD/month; 95% CI, −0.6 to −0.1; P = 0.004) with both oral and IV formulations showing decline (Figure S1); moxifloxacin use remained low and unchanged (0.06 DDD/1000 OBD/month; 95% CI, −0.0 to 0.1; P = 0.124). No significant change was seen in ceftriaxone use. Amoxicillin/clavulanate in both oral and IV formulations increased post-intervention (26.5 DDD/1000 OBD/month; 95% CI, 6.9–46.0; P = 0.009), with continued rise long-term (1.2 DDD/1000 OBD/month; 95% CI, 0.9-1.6; P < 0.001), although the upward trend had plateaued (Figure S2).
DDD antibiotic use for commonly targeted antibiotics in the ICU 6 months before and 7 years after ICU-AMS intervention. Dotted vertical lines represent start of intervention (August 2017). Solid lines represent pre- and post-intervention trends in antimicrobial use estimated using interrupted time series analysis. The dots on the graph are raw data points. (a) piperacillin/tazobactam, (b) vancomycin, (c) ceftriaxone, (d) meropenem, (e) amoxicillin/clavulanate, (f) ciprofloxacin, (g) moxifloxacin.
A total of 9163 recommendations were made over 7 years, with overall acceptance of 84.9% (Table 1 and Figures S3 and S4). Discontinuation was the most common recommendation (43.2%) but had the lowest overall acceptance rate (82.3%). Factors associated with acceptance of recommendations within 24 h are presented in Table S4. Recommendations for immunocompromised patients were more likely to be accepted overall (OR 1.31; 95% CI, 1.09–1.57; P = 0.003), and for antibiotic discontinuation (OR 1.33; 95% CI, 1.04–1.70; P = 0.024). Recommendations made for non-surgical patients were also more likely to be accepted (OR 1.31; 95% CI, 1.14–1.5; P < 0.001). Targeted sub-analysis demonstrated de-escalation and discontinuation recommendations (Table S5) were more likely to be accepted for meropenem compared with other antibiotics (87.7% versus 82.6%, P = 0.009).
Psychosocial factors including round duration, ID physician gender, and seniority were also analysed (Table S4). In univariable analysis, overall recommendations by ID clinicians who identified as men were more likely to be accepted (OR 1.23; 95% CI, 1.07–1.4; P = 0.003). This association was further examined for effect of seniority, using a gender-by-seniority interaction, which was not significant, suggesting that effect of gender was consistent across seniority strata. ID clinician seniority was associated with increased acceptance of de-escalation recommendations (OR 1.03; 95% CI, 1.01–1.05; P = 0.01). Longer rounds (per 10 min increment) were associated with higher rates of acceptance (OR 1.10; 95% CI, 1.02–1.19; P = 0.018), particularly for antibiotic discontinuation (P = 0.007) and oral switch (P = 0.016).
Discussion
This long-term evaluation found that a structured, integrated AMS programme was sustainable and effective, with high recommendation acceptance and reduced broad-spectrum antimicrobial use. Escalation had the highest acceptance, whereas discontinuation had the lowest, consistent with prior data in our cohorts and others,^5–7^ likely reflecting the high acuity and diagnostic uncertainty common in ICU settings, where clinicians may be more reluctant to withdraw antimicrobials due to risk of deterioration. However, the overall good compliance with discontinuation recommendations (82%), coupled with an association between increased acceptance and longer clinical discussion, reinforces the value of direct clinician engagement compared with other stewardship strategies.^8^ Notably, de-escalation or discontinuation recommendations involving meropenem were accepted more frequently than for other agents, which may reflect clearer microbiology-driven triggers for narrowing therapy once a carbapenem has been started, or greater clinician prioritization of carbapenem-sparing stewardship. Although this study did not directly assess the effect of an AMS programme on patient outcomes, it is reassuring to note that survival for patients with infective diagnoses and sepsis remained consistent over the study period and compares favourably with peer ICUs according to independent external benchmarking (Figures S5–S7).
The shift in antimicrobial use highlights the programme’s impact. We demonstrated successful influence on prescribing practices, leading to sustained reduction in use of meropenem, piperacillin/tazobactam, vancomycin and ciprofloxacin, despite representing a tertiary ICU servicing solid-organ transplant and haematology-oncology patients. The observed increase in amoxicillin/clavulanate use may indicate compensatory prescribing trends. Although this may reflect improved de-escalation or promotion of oral switch, further evaluation is needed to confirm alignment with AMS goals.
Generalizability of this model to ICUs with a higher antimicrobial resistance burden, or in less-resourced settings may vary. Although the core ‘handshake stewardship’ principles are transferable, the magnitude and pattern of change in consumption may differ where baseline broad-spectrum use is higher and de-escalation options are constrained by local resistance epidemiology.^9^ In such settings, stewardship impact may depend more heavily on rapid diagnostics, local antibiograms and availability of effective carbapenem-sparing regimens. Implementation in many low- and middle-income country (LMIC) contexts may also be further limited because ‘lift-and-shift’ stewardship models are reliant on local health system capacity for adaptation.^10^
Acceptance of AMS recommendations appears to be shaped by patient-specific, clinical and social factors. Higher acceptance in immunocompromised patients may be evidence of increased receptiveness to specialist input in complex cases. This finding in our cohort aligns with growing evidence supporting AMS effectiveness in this population. Other studies have also demonstrated that AMS interventions in high-risk patients, such as those with haematological malignancies or undergoing chemotherapy, can safely reduce antimicrobial exposure without adverse outcomes, and may even be associated with improved survival.^11,12^ The reduced acceptance of AMS recommendations among non-medical patients in our study reflects well-documented challenges in surgical populations.^13,14^ AMS efforts have traditionally focused on perioperative prophylaxis, with less emphasis on postoperative therapeutic prescribing.^15^ Adherence to antibiotic guidelines is often inconsistent, influenced by individual clinician preferences, institutional protocols, and concerns about postoperative infections,^13^ where diagnostic uncertainty can foster reluctance to de-escalate antimicrobials.
The observed association between ID clinician gender and recommendation acceptance suggests that interpersonal dynamics and team structures may play a role; however, confounding related to clinician experience, case-mix and temporal changes remains possible. Recent survey and interviews of stewardship providers found that those who identified as women were almost three times more likely to report experience of bias, compared with counterparts who identified as men.^16^ These findings highlight the need for qualitative research and interventions co-designed with the relevant stakeholders, to help clarify these social determinants and support consistent uptake of stewardship advice across varied clinical settings; sustainable AMS programmes must attend not only to prescribing behaviours and outcomes, but also to the interpersonal and organizational context in which they operate.
This study has some limitations. The ICU-AMS service exists within a strong secular culture of AMS within our institution, with pre-approval prescribing restrictions,^4,5^ other sub-specialty handshake models,^17^ and a comprehensive antibiotic allergy service.^18^ Nonetheless, our programme shows enduring changes in a high-acuity unit, with increased patient complexity, which has unique pressures toward frequent and broader-spectrum prescribing.^19^ Reasons for non-acceptance were not systematically captured across the study period as such barriers to uptake are not explored. Patient-level outcomes such as length of stay, mortality or re-admission were not assessed. Antibiotic consumption, although standardized, may be influenced by institutional dosing practices (e.g. augmented renal clearance, renal replacement therapy, and extended-infusion protocols). Finally, generalizability may vary, particularly in lower-resource settings, and in high antimicrobial resistance settings where prescribing patterns and de-escalation options are shaped by local antibiograms and formulary constraints.
This study underscores the long-term viability of an integrated AMS service in a critical care setting. Sustained reduction in broad-spectrum antibiotic use, high recommendation acceptance rates, and ongoing engagement over several years highlight the value of this ICU-AMS programme. These findings, based on a uniquely long-term study in this setting, support the role of AMS in reducing unnecessary antimicrobial exposure, in turn decreasing the selection pressure for MDR organisms, and ultimately improving patient outcomes.^20^ Future efforts should focus on maintaining and enhancing these gains, and explore the qualitative drivers of AMS acceptance, to develop a more nuanced and tailored ‘handshake’.
Supplementary Material
dkag086_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Timsit J-F, Bassetti M, Cremer O et al Rationalizing antimicrobial therapy in the ICU: a narrative review. Intensive Care Med 2019; 45: 172–89. 10.1007/s 00134-019-05520-530659311 · doi ↗ · pubmed ↗
- 2Morris AM, Bai A, Burry L et al Long-term effects of phased implementation of antimicrobial stewardship in academic IC Us: 2007-2015. Crit Care Med 2019; 47: 159–66. 10.1097/CCM.000000000000351430407951 · doi ↗ · pubmed ↗
- 3Hurst AL, Child J, Pearce K et al Handshake stewardship: a highly effective rounding-based antimicrobial optimization service. Pediatr Infect Dis J 2016; 35: 1104–10. 10.1097/INF.000000000000124527254036 · doi ↗ · pubmed ↗
- 4Devchand M, Stewardson AJ, Urbancic KF et al Outcomes of an electronic medical record (EMR)–driven intensive care unit (ICU)-antimicrobial stewardship (AMS) ward round: assessing the “five moments of antimicrobial prescribing”. Infect Control Hosp Epidemiol 2019; 40: 1170–5. 10.1017/ice.2019.21831407651 · doi ↗ · pubmed ↗
- 5Devchand M, Nolen A, Stewardson AJ et al Long-term outcomes of an electronic medical record (EMR)–integrated antimicrobial stewardship (AMS) intensive care unit (ICU) ward round. Infect Control Hosp Epidemiol 2022; 43: 670–2. 10.1017/ice.2021.7133731236 · doi ↗ · pubmed ↗
- 6NAUSP . National Antimicrobial Utilisation Surveillance Program (NAUSP). Government of South Australia; 2025. https://www.sahealth.sa.gov.au/wps/wcm/connect/public+content/sa+health+internet/clinical+resources/clinical+programs+and+practice+guidelines/infection+and+injury+management/antimicrobial+stewardship/national+antimicrobial+utilisation+surveillance+program+nausp/national+antimicrobial+utilisation+surveillance+program+nausp
- 7Chiotos K, Tamma PD, Gerber JS. Antibiotic stewardship in the intensive care unit: challenges and opportunities. Infect Control Hosp Epidemiol 2019; 40: 693–8. 10.1017/ice.2019.7431046851 · doi ↗ · pubmed ↗
- 8Hurst AL, Child J, Parker SK. Intervention and acceptance rates support handshake-stewardship strategy. J Pediatric Infect Dis Soc 2019; 8: 162–5. 10.1093/jpids/piy 05429912364 · doi ↗ · pubmed ↗