Changes in transverse dimensions in growing patients treated with AMCOP® and electromyographic assessment with Teethan®
Laura Ferrante, Gianna Dipalma, Filippo Cardarelli, Angela Di Noia, Grazia Marinelli, Antonio Di Lorenzo, Francesco Inchingolo, Daniela Di Venere, Andrea Palermo, Angelo Michele Inchingolo, Alessio Danilo Inchingolo

TL;DR
This study evaluates how AMCOP® appliances affect maxillary expansion and neuromuscular balance in children with transverse maxillary deficiency.
Contribution
The study combines 3D digital model analysis and sEMG to assess both structural and neuromuscular outcomes of AMCOP® treatment in growing patients.
Findings
AMCOP® treatment led to transverse maxillary expansion in all patients.
sEMG showed improved neuromuscular coordination with normalized symmetry and torsion indices.
No adverse events were recorded during treatment.
Abstract
To retrospectively evaluate transverse maxillary changes and neuromuscular balance in growing patients treated with AMCOP® elastodontic appliances by combining three-dimensional digital model analysis and surface electromyography (sEMG). This monocentric retrospective case series included 12 children (8 females, 4 males; aged 4–7 years) treated for transverse maxillary deficiency with AMCOP® Integral or Class III (TC) devices for 10–18 months. Transverse widths were measured on digital models (Deltadent®) at baseline (T0) and post-treatment (T1) at the intercanine, inter–second deciduous molar (inter-5), and intermediate or first molar regions when erupted. Neuromuscular function was assessed using surface electromyography (Teethan®), evaluating symmetry indices (POC TA/MM), barycenter (BAR), torsion (TORS), asymmetry (ASIM), and impact index (IMP). All patients showed transverse…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
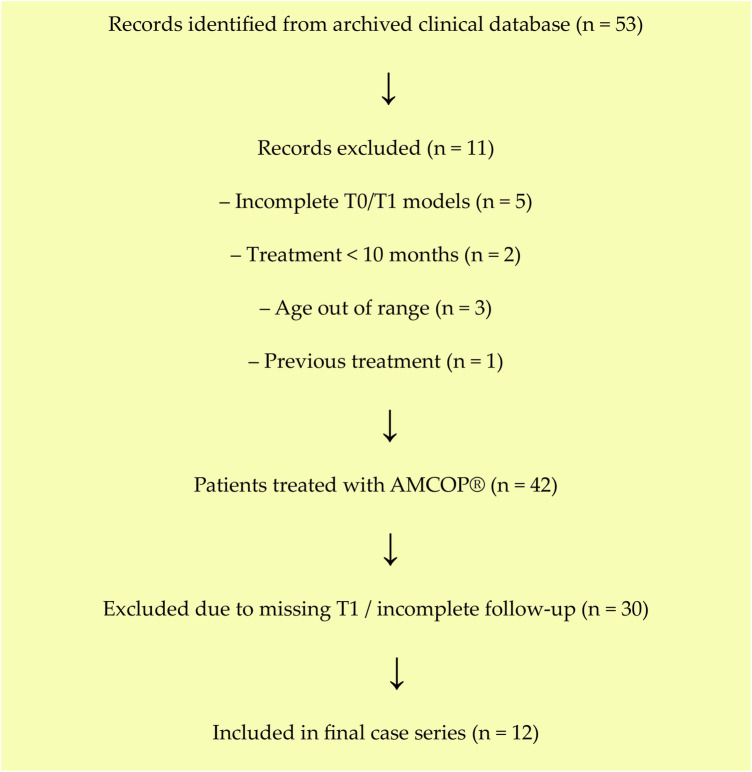 Figure 1
Figure 1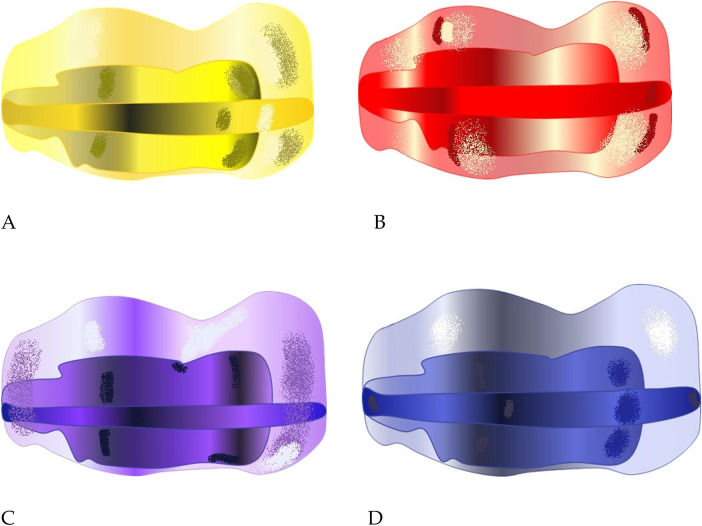 Figure 2
Figure 2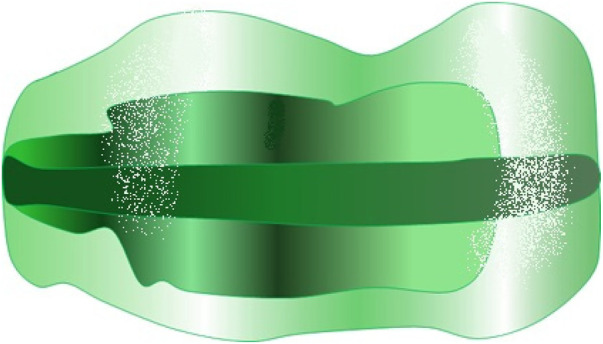 Figure 3
Figure 3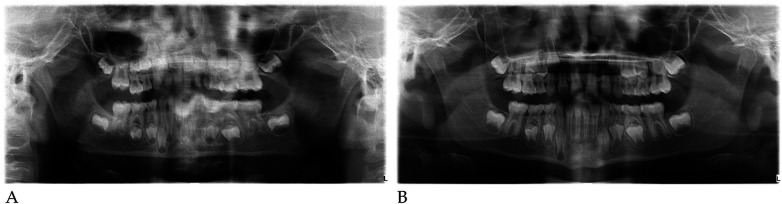 Figure 4
Figure 4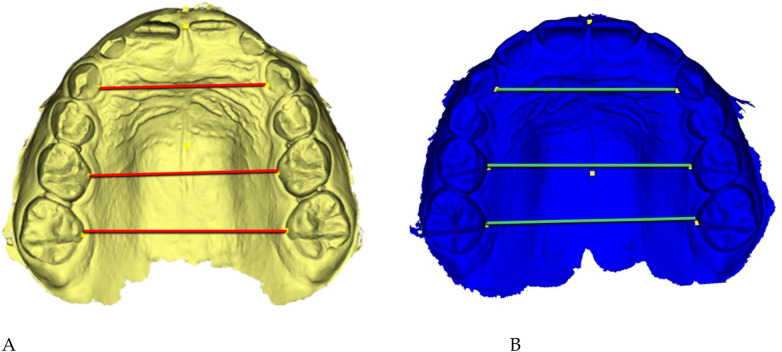 Figure 5
Figure 5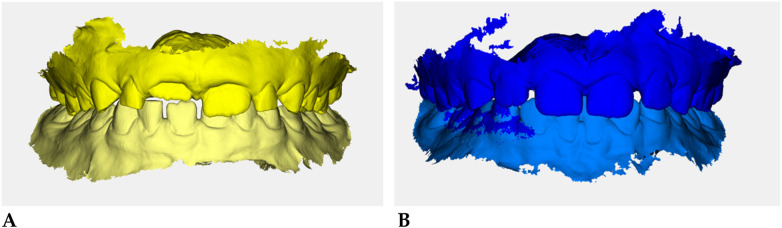 Figure 6
Figure 6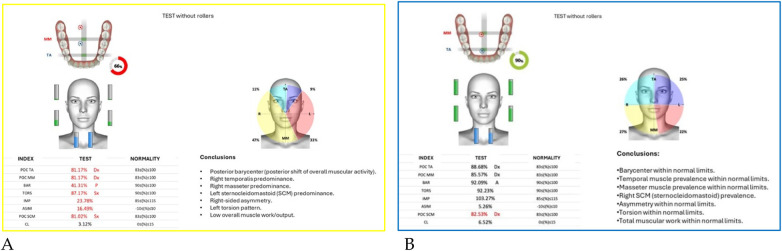 Figure 7
Figure 7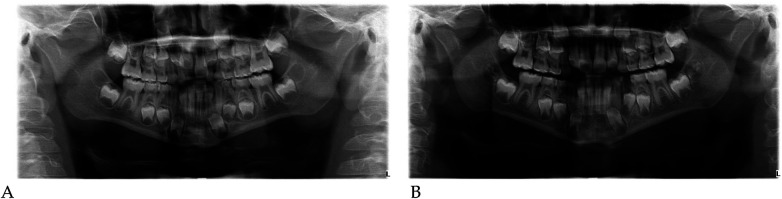 Figure 8
Figure 8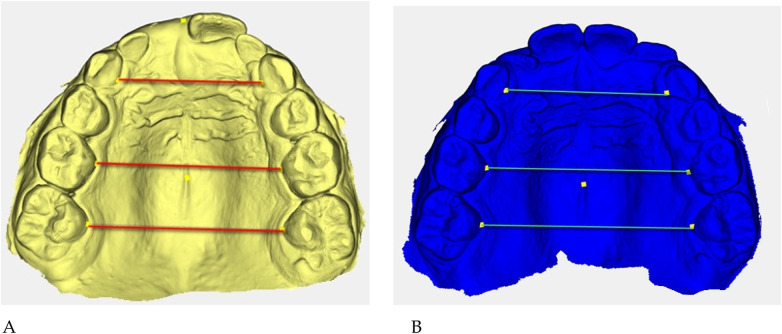 Figure 9
Figure 9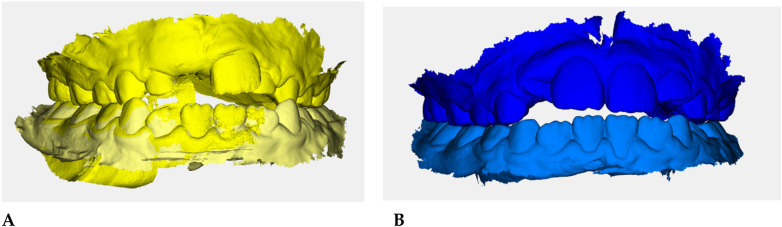 Figure 10
Figure 10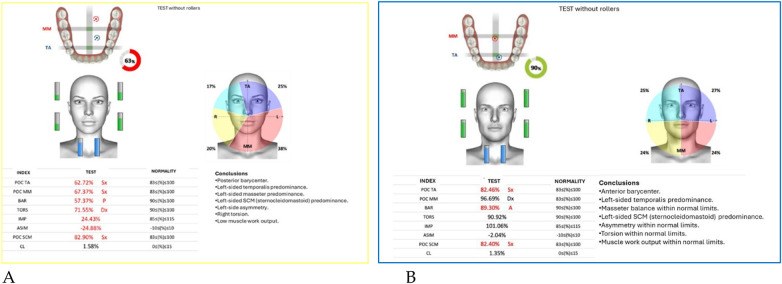 Figure 11
Figure 11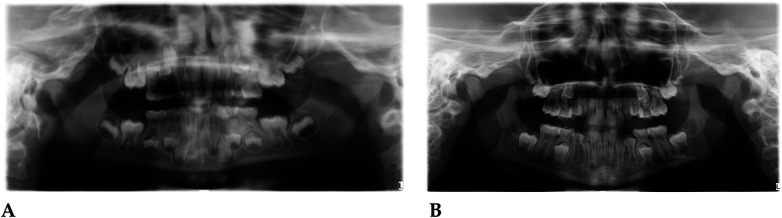 Figure 12
Figure 12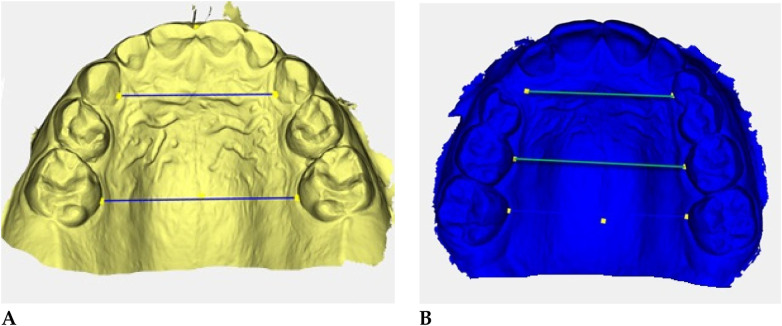 Figure 13
Figure 13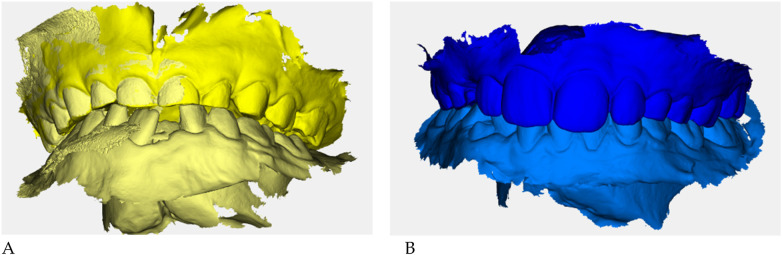 Figure 14
Figure 14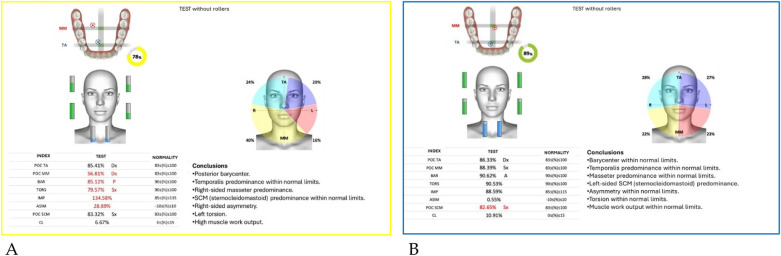 Figure 15
Figure 15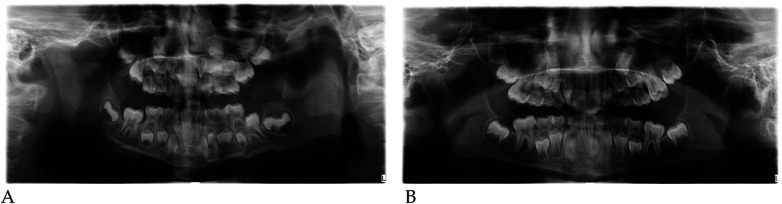 Figure 16
Figure 16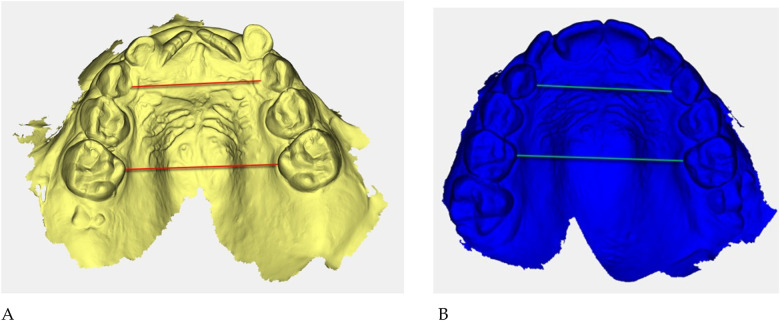 Figure 17
Figure 17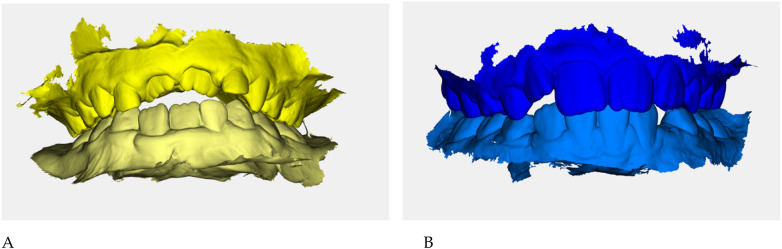 Figure 18
Figure 18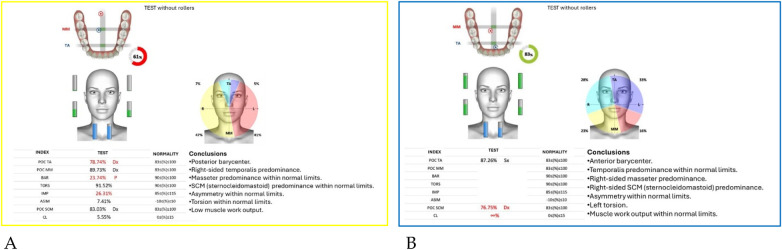 Figure 19
Figure 19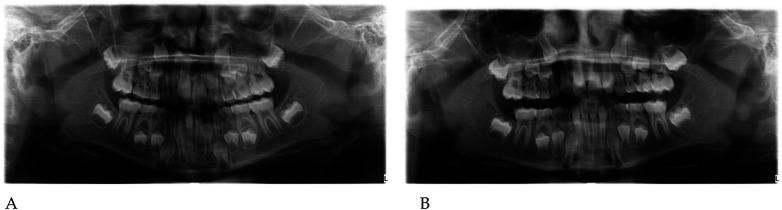 Figure 20
Figure 20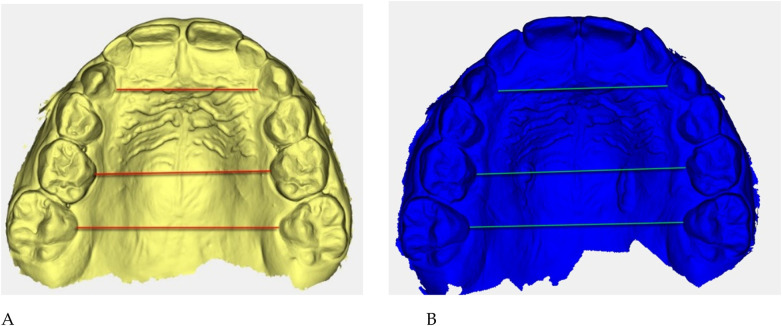 Figure 21
Figure 21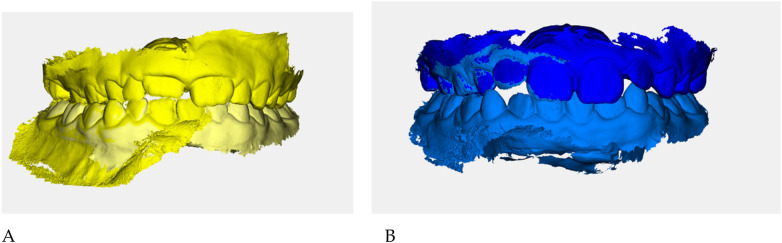 Figure 22
Figure 22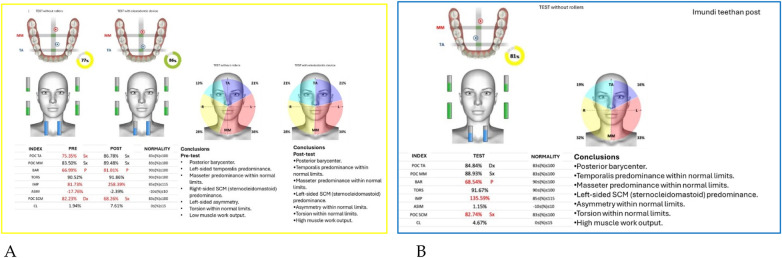 Figure 23
Figure 23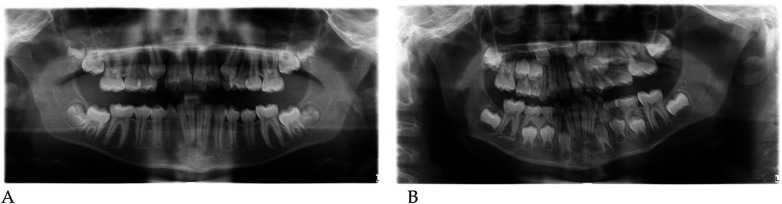 Figure 24
Figure 24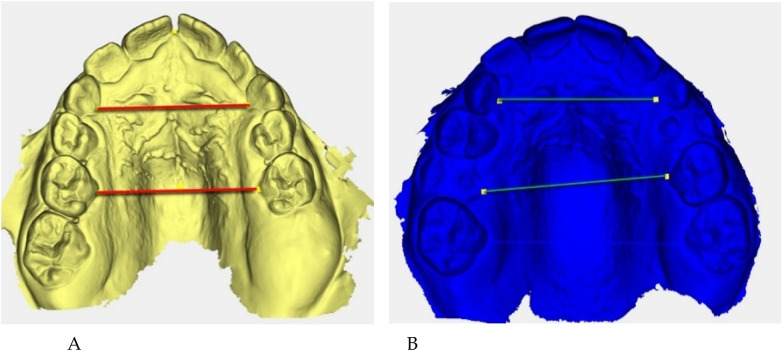 Figure 25
Figure 25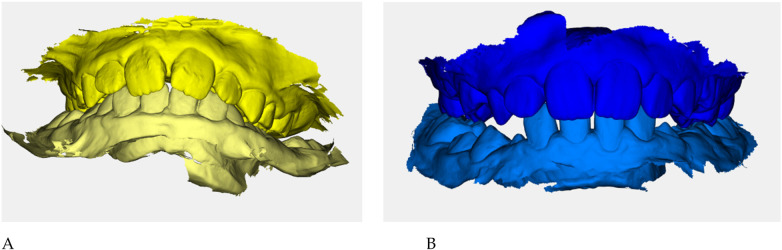 Figure 26
Figure 26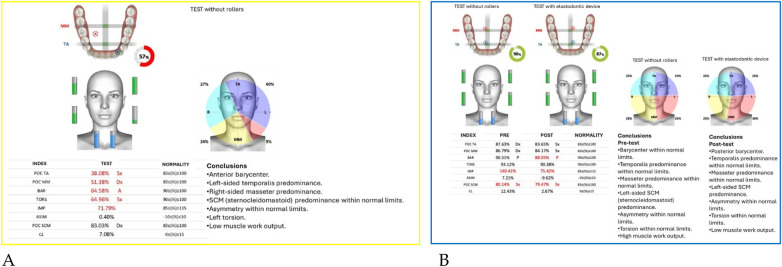 Figure 27
Figure 27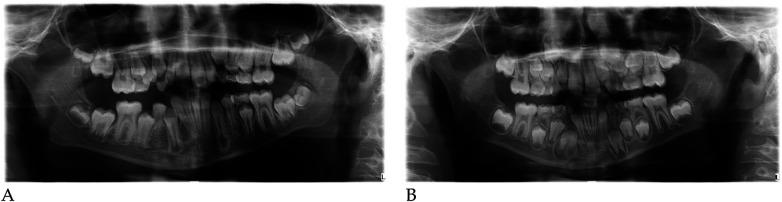 Figure 28
Figure 28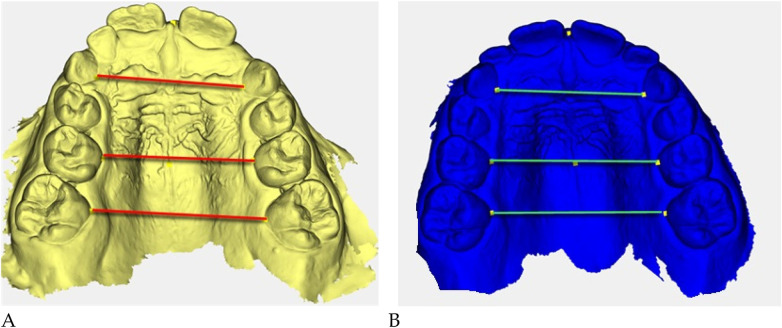 Figure 29
Figure 29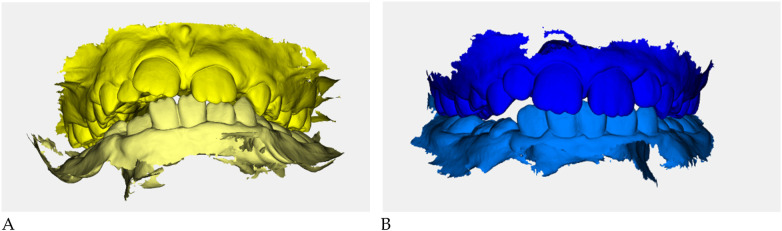 Figure 30
Figure 30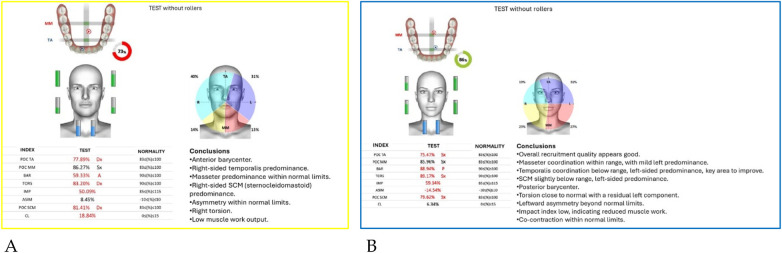 Figure 31
Figure 31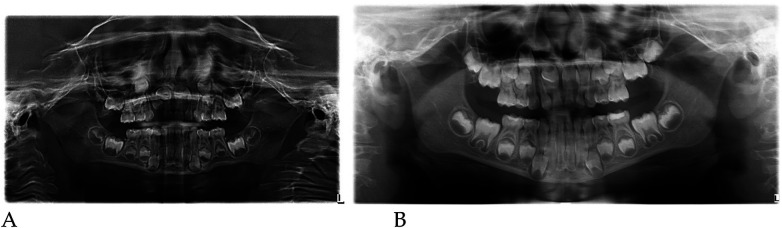 Figure 32
Figure 32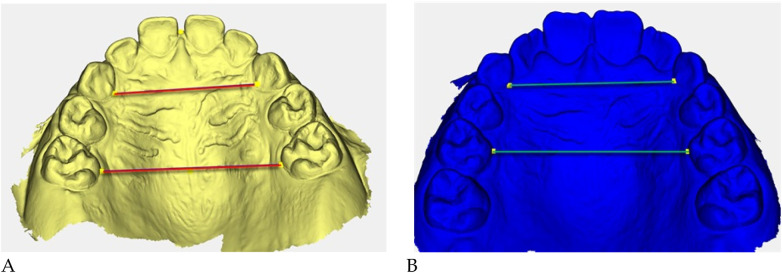 Figure 33
Figure 33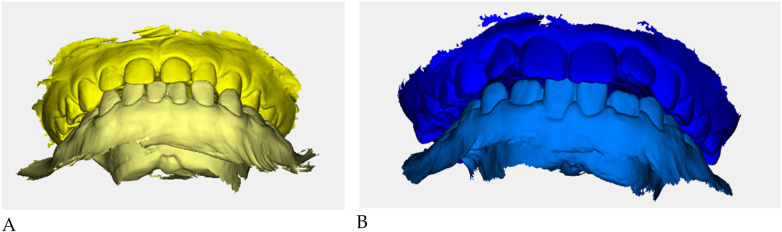 Figure 34
Figure 34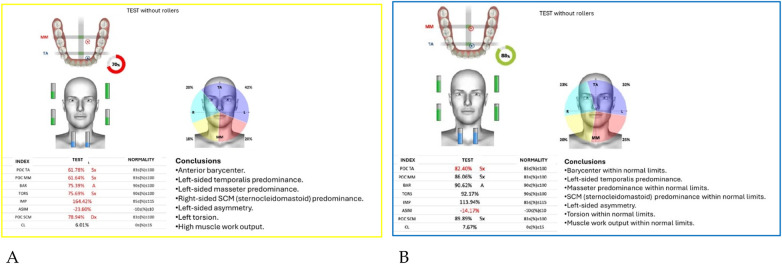 Figure 35
Figure 35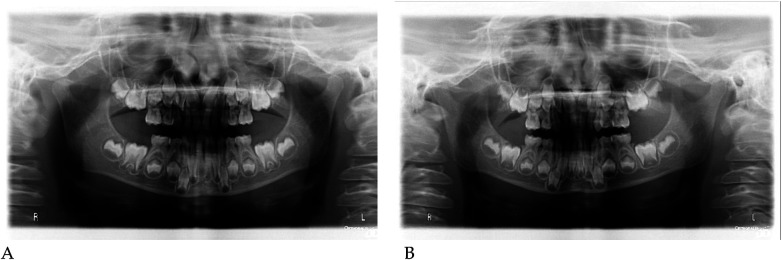 Figure 36
Figure 36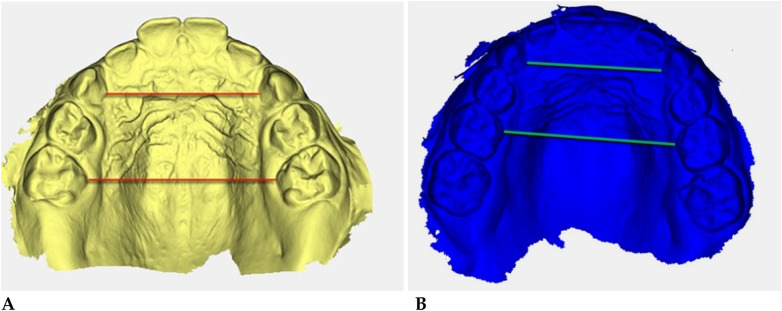 Figure 37
Figure 37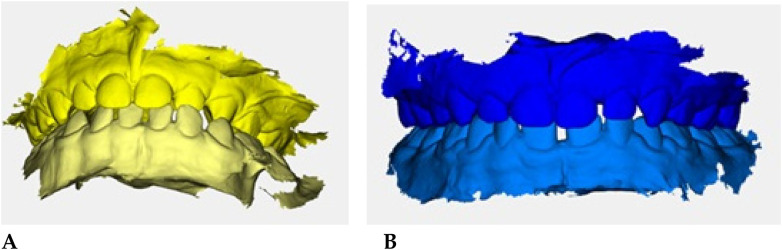 Figure 38
Figure 38 Figure 39
Figure 39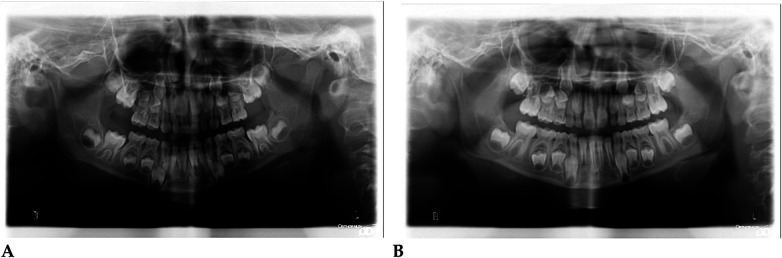 Figure 40
Figure 40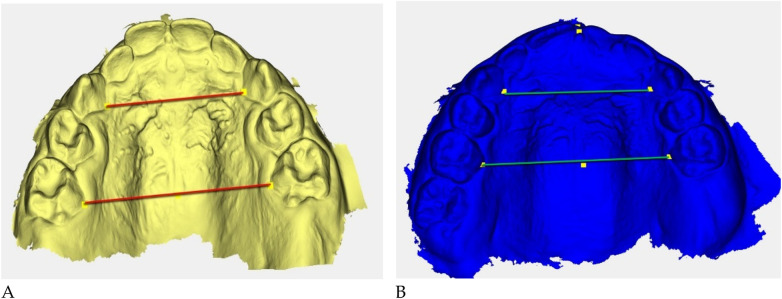 Figure 41
Figure 41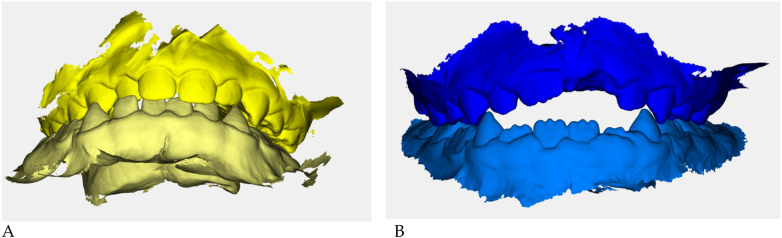 Figure 42
Figure 42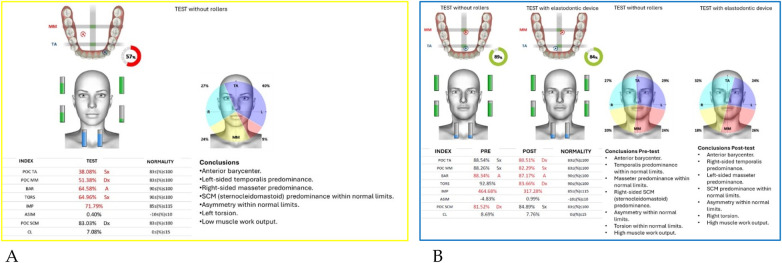 Figure 43
Figure 43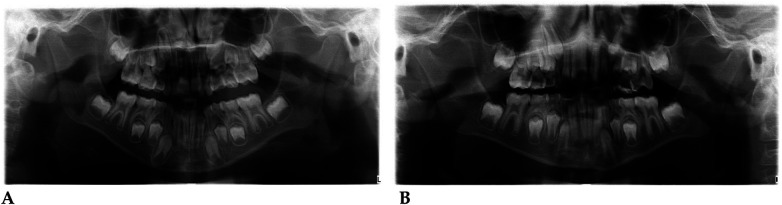 Figure 44
Figure 44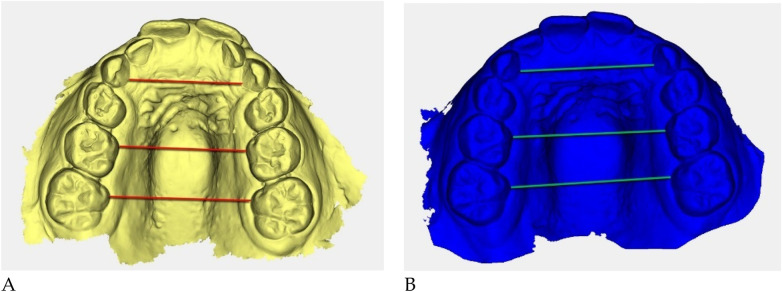 Figure 45
Figure 45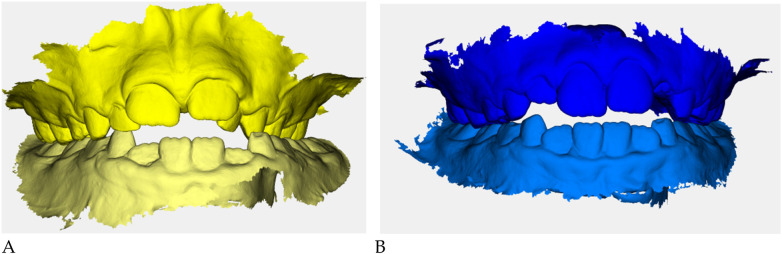 Figure 46
Figure 46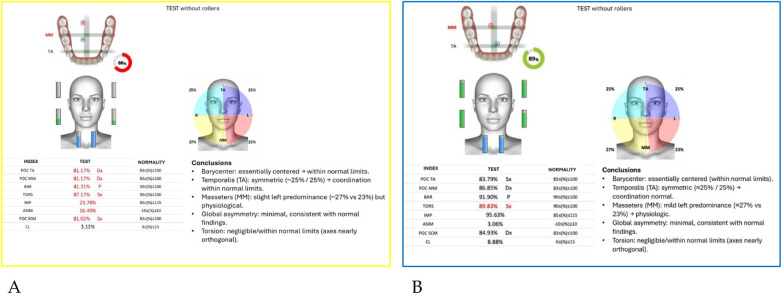 Figure 47
Figure 47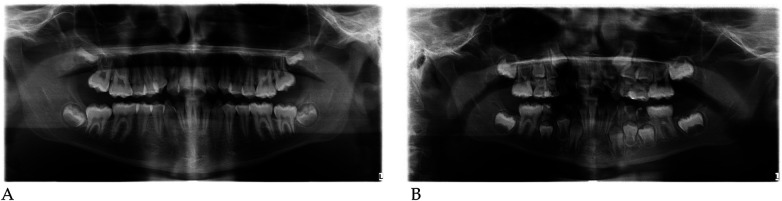 Figure 48
Figure 48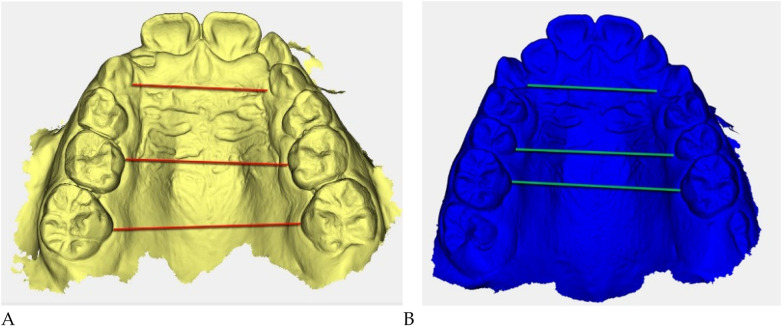 Figure 49
Figure 49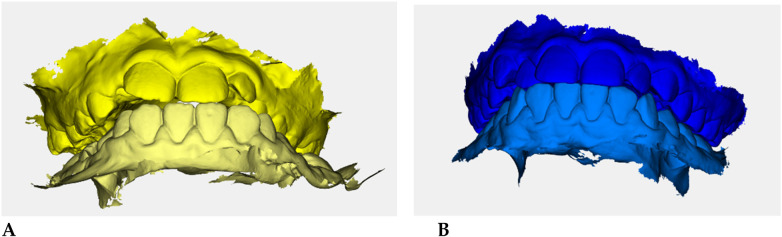 Figure 50
Figure 50 Figure 51
Figure 51| Clinical Feature | Integral Appliance | Class III (TC) Appliance |
|---|---|---|
| Sagittal occlusion class | Class I or no sagittal discrepancy | Skeletal Class III pattern |
| Anterior crossbite | Absent | Present |
| Primary treatment goal | Transverse development and functional reeducation | Transverse development + sagittal guidance |
| Appliance activation | Passive elastodontic function | Passive elastodontic function with sagittal guidance design |
| Size selection | Based on intermolar width and age charts | Based on intermolar width and age charts |
| Arch form selection | S, OS, F, C depending on palatal morphology | Single standardized arch form |
| Abbreviation | Full name | Functional meaning |
|---|---|---|
| POC TA/MM | Percentage of Overlapping Coefficient | Bilateral symmetry of anterior temporalis and masseter muscle activation (%) |
| BAR | Barycenter | Antero-posterior distribution of muscular activity and functional mandibular position |
| TORS | Torsion index | Right–left dominance and mandibular torsional imbalance |
| ASIM | Asymmetry index | Global inter-muscular asymmetry measurement |
| IMP | Impact Index | Muscular recruitment efficiency and contraction strength |
| CL | Co-contraction Level | Degree of synchronized muscle activation during maximal intercuspation |
| POC SCM | Percentage of Overlapping Coefficient SCM | Bilateral symmetry of sternocleidomastoid muscle activation (%) |
| Distance | Pre (mm) | Post (mm) | Δ (mm) | Δ % |
|---|---|---|---|---|
| Intercanine | 27.24 | 30.98 | +3.74 | +13.7% |
| Inter-5 (second deciduous molars) | 30.60 | 34.60 | +4.00 | +13.1% |
| Inter-6 (first molars) | 33.03 | 36.11 | +3.08 | +9.3% |
| Index | Pre | Post | Outcome |
|---|---|---|---|
| POC TA | 81.17% | 88.68% | From below → within range |
| POC MM | 81.17% | 85.57% | Improved |
| BAR (Barycenter) | 41.31% | 92.09% | Normalized |
| TORS | 87.17% (L) | 92.23% | Normalized |
| IMP | 23.78% | 103.27% | Normalized |
| ASIM | 16.49% | 5.26% | Reduced to normal range |
| POC SCM | 81.02% | 82.53% | Slight improvement |
| CL | 3.12% | 6.52% | Within range |
| Distance | Pre (mm) | Post (mm) | Δ % | |
|---|---|---|---|---|
| Intercanine (C–C) | 22.45 | 27.04 | +4.59 | +20.5% |
| Inter–second deciduous molars (5–5) | 29.14 | 34.02 | +4.88 | +16.7% |
| Inter–first molars (6–6) | 30.55 | 35.42 | +4.87 | +15.9% |
| Index | Pre | Post | Outcome |
|---|---|---|---|
| POC TA | 85.41% | 86.33% | Within normal limits |
| POC MM | 56.81% | 88.39% | From below → normalized |
| BAR | 85.12% | 90.62% | Normalized |
| TORS | 79.57% | 90.53% | Normalized |
| IMP | 134.58% | 88.59% | Reduced to normal limits |
| ASIM | 28.89% | 0.55% | Markedly reduced |
| POC SCM | 83.32% | 82.65% | Stable, within range |
| CL | 6.67% | 10.91% | Within normal limits |
| Distance | Pre (mm) | Post (mm) | Δ (mm) | Δ % |
|---|---|---|---|---|
| Intercanine (C–C) | 20.32 | 24.56 | +4.24 | +20.9% |
| Inter–second deciduous molars (5–5) | 25.38 | 28.70 | +3.32 | +13.1% |
| Inter–first molars (6–6) | n.a. | 29.95 | — | — |
| Index | Pre | Post | Outcome |
|---|---|---|---|
| POC TA | 85.41% | 86.33% | Within normal limits |
| POC MM | 56.81% | 88.39% | From below → normalized |
| BAR | 85.12% | 90.62% | Normalized |
| TORS | 79.57% | 90.53% | Normalized |
| IMP | 134.58% | 88.59% | Reduced to normal limits |
| ASIM | 28.89% | 0.55% | Markedly reduced |
| POC SCM | 83.32% | 82.65% | Stable, within range |
| CL | 6.67% | 10.91% | Within normal limits |
| Distance | Pre (mm) | Post (mm) | Δ (mm) | Δ % |
|---|---|---|---|---|
| Intercanine (C–C) | 21.08 | 25.06 | +3.98 | +18.9% |
| Inter–second deciduous molars (5–5) | 24.69 | 30.95 | +6.26 | +25.3% |
| Index | Pre | Post | Outcome |
|---|---|---|---|
| POC TA | 78.74% | 87.26% | From below → normalized |
| POC MM | 89.73% | 83.00% | Within normal limits |
| BAR | 23.74% | 90.00% | Normalized (posterior → anterior) |
| TORS | 91.52% | 90.50% | Stable, within normal limits |
| IMP | 26.31% | 85.00% | Normalized |
| ASIM | 7.41% | 0.00% | Symmetry restored |
| POC SCM | 83.03% | 76.75% | Mild left shift, within tolerance |
| CL | 5.55% | 10.00% | Within normal range |
| Distance | Pre (mm) | Post (mm) | Δ (mm) | Δ % |
|---|---|---|---|---|
| Intercanine (C–C) | 23.92 | 28.65 | +4.73 | +19.8% |
| Inter–second deciduous molars (5–5) | 29.01 | 35.19 | +6.18 | +21.3% |
| Inter–first molars (6–6) | 33.72 | 36.12 | +2.40 | +7.1% |
| Index | Pre | Post | Outcome |
|---|---|---|---|
| POC TA | 75.35% | 84.84% | From below → within range |
| POC MM | 83.50% | 88.93% | Improved symmetry |
| BAR | 66.99% | 68.54% | Slight posterior shift, stable |
| TORS | 90.52% | 91.67% | Within normal limits |
| IMP | 81.73% | 135.59% | Increased muscle efficiency |
| ASIM | −17.76% | 1.15% | Restored symmetry |
| POC SCM | 82.23% | 82.74% | Stable within normal range |
| CL | 1.94% | 4.67% | Within normal range |
| Distance | Pre (mm) | Post (mm) | Δ (mm) | Δ % |
|---|---|---|---|---|
| Intercanine (C–C) | 23.35 | 24.33 | +0.98 | +4.2% |
| Inter–second deciduous molars (5–5) | 25.13 | 28.70 | +3.57 | +14.2% |
| Index | Pre | Post | Outcome |
|---|---|---|---|
| POC TA | 38.08% | 87.63% | From below → normalized |
| POC MM | 51.38% | 86.79% | From below → normalized |
| BAR | 64.58% | 90.51% | Normalized (anterior → central) |
| TORS | 64.96% | 93.12% | Normalized |
| IMP | 71.79% | 140.42% | Marked improvement |
| ASIM | 0.40% | 7.21% | Within normal limits |
| POC SCM | 83.03% | 80.14% | Stable, within range |
| CL | 7.08% | 12.43% | Within normal limits |
| Distance | Pre (mm) | Post (mm) | Δ (mm) | Δ % |
|---|---|---|---|---|
| Intercanine (C–C) | 23.22 | 24.71 | +1.49 | +6.4% |
| Inter-premolar (5–5) | 26.82 | 27.97 | +1.15 | +4.3% |
| Intermolar (6–6) | 27.51 | 29.34 | +1.83 | +6.6% |
| Index | Pre | Post | Outcome |
|---|---|---|---|
| POC TA | 77.89% | 75.47% | Stable, within range |
| POC MM | 86.27% | 85.96% | Stable, within range |
| BAR | 59.33% | 88.94% | Normalized (anterior → posterior) |
| TORS | 83.20% | 89.17% | Normalized |
| IMP | 50.09% | 59.14% | Improved efficiency |
| ASIM | 8.45% | −14.54% | Symmetry restored |
| POC SCM | 81.41% | 79.62% | Within normal limits |
| CL | 18.84% | 6.34% | Normalized |
| Distance | Pre (mm) | Post (mm) | Δ (mm) | Δ % |
|---|---|---|---|---|
| Intercanine (C–C) | 21.99 | 26.91 | +4.92 | +22.4% |
| Inter–second deciduous molars (5–5) | 27.46 | 31.60 | +4.14 | +15.1% |
| Index | Pre | Post | Outcome |
|---|---|---|---|
| POC TA | 61.78% | 82.40% | From below → within normal limits |
| POC MM | 61.64% | 86.06% | From below → normalized |
| BAR | 75.39% | 90.62% | Normalized (anterior → central) |
| TORS | 75.69% | 92.17% | Normalized |
| IMP | 164.42% | 113.94% | From hyperactivation → normal |
| ASIM | −23.60% | −14.17% | Improved symmetry |
| POC SCM | 78.94% | 89.89% | Normalized |
| CL | 6.01% | 7.67% | Stable within normal range |
| Distance | Pre (mm) | Post (mm) | Δ (mm) | Δ % |
|---|---|---|---|---|
| Intercanine (C–C) | 22.74 | 23.24 | +0.50 | +2.2% |
| Inter–second deciduous molars (5–5) | 27.35 | 29.51 | +2.16 | +7.9% |
| Index | Pre | Post | Outcome |
|---|---|---|---|
| POC TA | 85.19% | 75.06% | Within normal limits |
| POC MM | 84.58% | 73.04% | Slight decrease, within range |
| BAR | 55.56% | 87.42% | Normalized (anterior → posterior) |
| TORS | 88.39% | 92.50% | Normalized |
| IMP | 68.81% | 101.09% | Improved muscle efficiency |
| ASIM | 4.46% | 25.78% | Minor residual asymmetry |
| POC SCM | 83.87% | 72.67% | Within acceptable range |
| CL | 9.21% | 6.81% | Normal range |
| Distance | Pre (mm) | Post (mm) | Δ (mm) | Δ % |
|---|---|---|---|---|
| Intercanine (C–C) | 19.17 | 22.88 | +3.71 | +19.4% |
| Inter–second deciduous molars (5–5) | 25.79 | 29.15 | +3.36 | +13.0% |
| Index | Pre | Post | Outcome |
|---|---|---|---|
| POC TA | 38.08% | 80.51% | From below → normalized |
| POC MM | 51.38% | 82.29% | From below → normalized |
| BAR | 64.58% | 87.17% | Normalized (anterior → central) |
| TORS | 64.96% | 83.66% | Improved, within normal limits |
| IMP | 71.79% | 317.28% | From low → high efficiency |
| ASIM | 0.40% | 0.99% | Stable symmetry |
| POC SCM | 83.03% | 84.89% | Within normal limits |
| CL | 7.08% | 7.76% | Normalized |
| Distance | Pre (mm) | Post (mm) | Δ (mm) | Δ % |
|---|---|---|---|---|
| Intercanine (C–C) | 20.50 | 24.72 | +4.22 | +20.6% |
| Inter–second deciduous molars (5–5) | 22.52 | 27.95 | +5.43 | +24.1% |
| Inter–first permanent molars (6–6) | 25.26 | 29.20 | +3.94 | +15.6% |
| Index | Pre | Post | Outcome |
|---|---|---|---|
| POC TA | 81.17% | 83.79% | Normal range, mild improvement |
| POC MM | 81.17% | 86.85% | Normalized |
| BAR | 41.31% | 91.90% | Normalized (anterior → central) |
| TORS | 87.17% | 89.83% | Stable within range |
| IMP | 23.78% | 95.63% | Marked improvement |
| ASIM | 16.49% | 3.06% | Restored symmetry |
| POC SCM | 81.02% | 84.93% | Normalized |
| CL | 3.12% | 8.88% | Within range |
| Distance | Pre (mm) | Post (mm) | Δ (mm) | Δ % |
|---|---|---|---|---|
| Intercanine (C–C) | 21.97 | 25.86 | +3.89 | +17.7% |
| Inter–second deciduous molars (5–5) | 26.30 | 31.21 | +4.91 | +18.7% |
| Inter–first permanent molars (6–6) | 29.59 | 33.49 | +3.90 | +13.2% |
| Index | Pre | Post | Outcome |
|---|---|---|---|
| POC TA | 84.13% | 86.42% | Within normal limits |
| POC MM | 80.71% | 81.93% | Stable within range |
| BAR | 47.17% | 90.07% | Normalized (anterior → central) |
| TORS | 85.02% | 91.03% | Normalized |
| IMP | 65.10% | 102.50% | From below → optimal |
| ASIM | −4.29% | 11.44% | Within normal limits |
| POC SCM | 81.62% | 84.75% | Balanced |
| CL | 12.56% | 3.84% | Within range |
| Measure | Δ mm (mean ± SD) (range) | Mean % change | SMC (effect size) |
|---|---|---|---|
| Intercanine (IC) | +3.42 ± 1.52 (+0.50; +4.92) | +15.5% | 2.25 (very large) |
| Inter-5 (second deciduous molars) | +4.11 ± 1.54 (+1.15; +6.26) | +15.6% | 2.67 (very large) |
| Inter-6 (first molars) | +3.34 ± 1.12 (+1.83; +4.87) | +11.3% | 2.98 (very large) |
| Patient ID | IC T0 | IC T1 | Δ IC | Inter-5 T0 | Inter-5 T1 | Δ Inter-5 | Inter-6 T0 | Inter-6 T1 | Δ Inter-6 | BAR T0 | BAR T1 | POC-TA T0 | POC-TA T1 | POC-MM T0 | POC-MM T1 | TORS T0 | TORS T1 | ASIM T0 | ASIM T1 | IMP T0 | IMP T1 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| P01 | 27.24 | 30.98 | +3.74 | 30.60 | 34.60 | +4.00 | 33.03 | 36.11 | +3.08 | 41.31 | 92.09 | 81.17 | 88.68 | 81.17 | 85.57 | 87.17 | 92.23 | 16.49 | 5.26 | 23.78 | 103.27 |
| P02 | 22.45 | 27.04 | +4.59 | 29.14 | 34.02 | +4.88 | 30.55 | 35.42 | +4.87 | 85.12 | 90.62 | 85.41 | 86.33 | 56.81 | 88.39 | 79.57 | 90.53 | 28.89 | 0.55 | 134.58 | 88.59 |
| P03 | 20.32 | 24.56 | +4.24 | 25.38 | 28.70 | +3.32 | NA | NA | NA | 85.12 | 90.62 | 85.41 | 86.33 | 56.81 | 88.39 | 79.57 | 90.53 | 28.89 | 0.55 | 134.58 | 88.59 |
| P04 | 21.08 | 25.06 | +3.98 | 24.69 | 30.95 | +6.26 | NA | NA | NA | 23.74 | 90.00 | 78.74 | 87.26 | 89.73 | 83.00 | 91.52 | 90.50 | 7.41 | 0.00 | 26.31 | 85.00 |
| P05 | 23.92 | 28.65 | +4.73 | 29.01 | 35.19 | +6.18 | 33.72 | 36.12 | +2.40 | 66.99 | 68.54 | 75.35 | 84.84 | 83.50 | 88.93 | 90.52 | 91.67 | −17.76 | 1.15 | 81.73 | 135.59 |
| P06 | 23.35 | 24.33 | +0.98 | 25.13 | 28.70 | +3.57 | NA | NA | NA | 64.58 | 90.51 | 38.08 | 87.63 | 51.38 | 86.79 | 64.96 | 93.12 | 0.40 | 7.21 | 71.79 | 140.42 |
| P07 | 23.22 | 24.71 | +1.49 | 26.82 | 27.97 | +1.15 | 27.51 | 29.34 | +1.83 | 59.33 | 88.94 | 77.89 | 75.47 | 86.27 | 85.96 | 83.20 | 89.17 | 8.45 | −14.54 | 50.09 | 59.14 |
| P08 | 21.99 | 26.91 | +4.92 | 27.46 | 31.60 | +4.14 | NA | NA | NA | 75.39 | 90.62 | 61.78 | 82.40 | 61.64 | 86.06 | 75.69 | 92.17 | −23.60 | −14.17 | 164.42 | 113.94 |
| P09 | 22.74 | 23.24 | +0.50 | 27.35 | 29.51 | +2.16 | NA | NA | NA | 55.56 | 87.42 | 85.19 | 75.06 | 84.58 | 73.04 | 88.39 | 92.50 | 4.46 | 25.78 | 68.81 | 101.09 |
| P10 | 19.17 | 22.88 | +3.71 | 25.79 | 29.15 | +3.36 | NA | NA | NA | 64.58 | 87.17 | 38.08 | 80.51 | 51.38 | 82.29 | 64.96 | 83.66 | 0.40 | 0.99 | 71.79 | 317.28 |
| P11 | 20.50 | 24.72 | +4.22 | 22.52 | 27.95 | +5.43 | 25.26 | 29.20 | +3.94 | 41.31 | 91.90 | 81.17 | 83.79 | 81.17 | 86.85 | 87.17 | 89.83 | 16.49 | 3.06 | 23.78 | 95.63 |
| P12 | 21.97 | 25.86 | +3.89 | 26.30 | 31.21 | +4.91 | 29.59 | 33.49 | +3.90 | 47.17 | 90.07 | 84.13 | 86.42 | 80.71 | 81.93 | 85.02 | 91.03 | −4.29 | 11.44 | 65.10 | 102.50 |
| Index | T0 Mean ± SD (range) | T1 Mean ± SD (range) | Normalized at T1 |
|---|---|---|---|
| POC TA (%) | 72.8 ± 18.6 (38.1–85.4) | 83.2 ± 4.5 (75.1–88.7) | 9/12 (75%) |
| POC MM (%) | 72.2 ± 15.3 (51.4–89.7) | 84.8 ± 4.5 (73.0–88.9) | 10/12 (83%) |
| BAR (%) | 59.2 ± 19.0 (23.7–85.1) | 88.9 ± 2.7 (87.2–92.1) | 11/12 (92%) |
| TORS (%) | 81.9 ± 9.4 (65.0–91.5) | 90.9 ± 3.2 (83.7–93.1) | 11/12 (92%) |
| ASIM (%) | 5.4 ± 16.2 (−23.6 – + 28.9) | 2.0 ± 11.2 (−14.5 – + 25.8) | 10/12 (83%) |
| IMP (%) | 83.9 ± 42.6 (23.8–164.4) | 120.8 ± 66.5 (59.1–317.3) | 9/12 (75%) |
| POC SCM (%) | 81.3 ± 2.7 (78.9–83.9) | 82.8 ± 4.7 (72.7–89.9) | 9/12 (75%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthodontics and Dentofacial Orthopedics · Craniofacial Disorders and Treatments · Temporomandibular Joint Disorders
Introduction
1
The transverse development of the maxilla is a key determinant in establishing proper craniofacial harmony, occlusal balance, and airway function. This process originates early during embryogenesis, when the maxillary and palatine shelves fuse between the 7th and 12th weeks of gestation to form the hard palate and midpalatal suture (1–5). Following birth, this suture undergoes progressive appositional growth, largely modulated by functional stimuli such as nasal breathing, tongue posture, swallowing, and masticatory loading. The dynamic interplay between skeletal structures and soft tissue function ensures a coordinated increase in the width of the maxilla during early childhood. During the active growth period, particularly between 6 and 12 years of age, the midpalatal suture remains patent, allowing for both spontaneous and therapeutically induced expansion (5–11). This period represents a window of opportunity for orthopedic and functional interventions aimed at redirecting craniofacial growth patterns before skeletal maturation limits adaptive potential. Transverse maxillary discrepancies are defined as conditions in which the maxillary arch width is insufficient relative to the mandibular arch. A well-balanced transverse relationship typically exhibits a maxillary intermolar width 2–3 mm greater than that of the mandible, allowing for optimal occlusal interdigitation (McNamara, 2000). When this proportion is reversed, crossbites and arch constrictions emerge, often classified as mild (<3 mm), moderate (3–5 mm), or severe (>5 mm), depending on the magnitude of discrepancy and the patient's developmental stage (12–18). The etiology of transverse deficiency is multifactorial. Genetic predispositions may be compounded by environmental and functional influences such as chronic mouth breathing, upper airway obstruction (adenoid hypertrophy, allergic rhinitis), atypical swallowing, altered tongue posture, and parafunctional habits including thumb sucking or prolonged pacifier use (19–22). These factors act synergistically to disturb the equilibrium between the maxillary skeletal base and the neuromuscular environment, producing both morphological and functional imbalances (23–29). Epidemiological data indicate that transverse discrepancies affect approximately 8%–22% of children in the early mixed dentition, making them one of the most frequent developmental alterations encountered in pediatric orthodontics. If left untreated, maxillary constriction may contribute to a cascade of secondary problems, posterior crossbite, dental compensation, midline deviation, asymmetric mandibular growth, temporomandibular dysfunctions (TMD), and impaired masticatory efficiency (30–36). Furthermore, the close anatomical and functional interrelationship between the maxilla, nasal cavity, and cranial base implies that transverse deficiency can also influence respiratory patterns and even global postural balance.
The timing of intervention plays a decisive role in the orthopedic management of transverse maxillary deficiencies. In the mixed dentition stage, the midpalatal suture is less mature and more responsive to orthopedic stimuli; therefore, a substantial part of the expansion results from true skeletal distraction rather than mere dento-alveolar remodeling. Comparative data between children and adults show that in pediatric patients, approximately half of the expansion occurs at the skeletal level through palatal separation, whereas in adults the skeletal component is markedly reduced and dental tipping predominates (37–44). Early treatment also benefits from residual growth potential, which facilitates the adaptation of soft tissues and contributes to long-term stability (45–53). Clinical series and longitudinal observations have demonstrated that when expansion is performed during early growth, there are no significant adverse vertical effects or increases in mandibular plane inclination, provided that the expansion protocol is well controlled (54–62). Moreover, early interceptive expansion contributes to an increase in arch perimeter, reducing the need for extractions to resolve mild or moderate crowding. Hence, intervening during the period of high sutural plasticity allows the clinician to achieve greater orthopedic effectiveness with minimal invasiveness, promoting harmonious development of the maxillary complex and the surrounding functional matrices.
Conventional orthopedic expansion techniques are primarily mechanical in nature and aim to separate the midpalatal suture through the application of transverse forces. Rapid palatal expansion (RPE) devices, such as Hyrax and Haas expanders, are well-established tools capable of producing skeletal expansion through a combination of sutural and dental effects. Similarly, slow expansion appliances like the quad-helix and W-arch deliver lighter forces over a longer period, promoting gradual adaptation of the supporting tissues. Although these appliances have demonstrated consistent clinical success in increasing maxillary width, their action is largely limited to the orthopedic domain. They tend to disregard the underlying neuromuscular dysfunctions, altered tongue posture, unbalanced masticatory muscle activity, or dysfunctional swallowing, that frequently accompany skeletal constriction (63–70). Consequently, relapse may occur if the etiologic functional disturbances remain uncorrected. Fixed expansion appliances may also induce unwanted dental tipping, root resorption, and patient discomfort, particularly in younger subjects. Hygiene difficulties and interference with phonation or feeding further limit their acceptance in pediatric populations. These considerations have motivated the search for alternative modalities that can achieve not only skeletal widening but also the restoration of normal orofacial function (71–76).
Recent decades have witnessed the emergence of functional orthopedic philosophies that prioritize the integration of skeletal, muscular, and postural components in the correction of maxillary discrepancies. The AMCOP® (Apparecchi Modulari di Contenzione Ortopedica Personalizzati) system represents a significant innovation in this context. Designed as a modular and elastodontic appliance, AMCOP® combines the mechanical action necessary for orthopedic remodeling with the re-education of the orofacial musculature and proprioceptive control. Constructed from elastic medical-grade materials, the device exerts light, continuous forces that guide growth along physiological trajectories rather than imposing rigid displacement.ts modular design allows customization according to each patient's developmental stage and functional needs (77–84). The appliance promotes correct tongue positioning, enhances nasal respiration, balances mandibular posture, and facilitates neuromuscular reprogramming of swallowing and masticatory patterns. Unlike fixed expanders, AMCOP® acts through neuromuscular activation, stimulating the natural plasticity of craniofacial structures (85–90). By harmonizing the relationship between bone, muscle, and function, it aims to produce more stable and physiologically integrated results. Compared with traditional expanders such as Hyrax or Haas, AMCOP® induces a gradual orthopedic-functional expansion supported by:.
- a functional masticatory plane that decompresses the transverse corridors;
- a more centered and repetitive lingual thrust during swallowing, breathing, and phonation;
- neuromuscular retraining that reduces dysfunctional patterns such as anterior tongue interposition. This approach is less invasive, requires no daily screw activation, and seeks to integrate skeletal, dental, and muscular adaptation within a unified functional framework (91–99).
Craniofacial growth cannot be dissociated from the neuromuscular environment that shapes and sustains it. The coordination of the masticatory muscles, tongue, and cervical musculature forms an integrated system influencing not only occlusion but also postural stability. The concept of functional equilibrium, introduced by Moss within the framework of the functional matrix theory, underscores the principle that skeletal morphology adapts to functional demands. Altered muscle tone or asymmetrical activation patterns, often present in children with transverse deficiencies, may induce postural compensations extending from the stomatognathic system to the cervical and thoracic regions (100–103). Therefore, functional evaluation is essential in both diagnosis and treatment planning. The incorporation of digital technologies such as Teethan® provides objective and quantitative assessment of neuromuscular activity through surface electromyography (sEMG). This system allows clinicians to monitor the coordination of masseter and temporalis muscles during occlusal function, identify asymmetries, and evaluate improvements following therapeutic intervention. In the context of AMCOP® therapy, Teethan® analysis contributes to verifying neuromuscular rebalancing and supports the concept that orthopedic correction should coincide with muscular symmetry and postural improvement (104–109).
Given the high prevalence of transverse maxillary deficiencies in early mixed dentition and their close association with functional alterations such as low tongue posture and oral breathing, an interceptive therapeutic approach addressing both skeletal and neuromuscular aspects is essential. The present study aims to evaluate the efficacy of AMCOP® elastodontic therapy in correcting transverse maxillary deficiencies in growing children aged 4–7 years. The treatment duration ranged from 10 to 18 months, corresponding to an optimal period of skeletal plasticity (104). All patients included in this case series were treated at the Department of Orthodontics, Policlinico of Bari (Italy), following ethical guidelines and with informed parental consent. Pre- and post-treatment digital measurements were performed to quantify the transverse skeletal changes using Deltadent® software (Deltadent S.r.l., Italy), while functional outcomes were supported by neuromuscular analyses obtained with Teethan® sEMG evaluation (110–113). By presenting twelve well-documented clinical cases, this research contributes original data to the field of pediatric orthodontics and underscores the potential of AMCOP® functional elastodontic therapy to harmonize craniofacial growth through physiologic transverse expansion. Ultimately, the goal of this work is to highlight the capacity of AMCOP® devices to promote balanced transverse development, restore functional harmony within the stomatognathic system, and prevent future relapses by addressing the underlying causes of maxillary constriction rather than its morphological consequences (114–116).
Materials and methods
2
Study design and setting
2.1
This was a monocentric, observational case series with retrospective data analysis conducted at the Department of Dentistry and Orthodontics, University Polyclinic of Bari (Italy). The study focused on growing patients with transverse maxillary deficiency treated with functional elastodontic appliances.
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Policlinico of Bari (Protocol No. 971, Prot. 2427/CEL., approved on 1 October 2025, U.O. di Odontostomatologia; Principal Investigator: Prof. F. Inchingolo).
Written informed consent was obtained from all parents or legal guardians before data collection, image publication, and clinical participation.
Patient identification and case selection (retrospective database query)
2.2
Eligible cases were identified retrospectively by querying the institutional clinical database of the Department of Dentistry and Orthodontics, University Polyclinic of Bari, for growing patients treated with AMCOP® elastodontic appliances for transverse maxillary deficiency between January 2022 and december 2024. The search was performed using treatment logs and digital model archives (Deltadent®), cross-checked with Teethan® sEMG records when available. For each potentially eligible patient, the presence of baseline (T0) and end-of-treatment (T1) digital models and the completion of active transverse therapy (minimum 10 months) were verified. Only subjects meeting all inclusion/exclusion criteria and having analyzable T0–T1 records were included in the final case series.
Inclusion and exclusion criteria
2.3
Inclusion criteria:
-
Age between 4 and 7 years at the start of treatment (late deciduous or early mixed dentition).
-
Transverse maxillary deficiency documented clinically and on digital models, including maxillary constriction, unilateral or bilateral posterior crossbite, or posterior reverse bite.
-
No previous orthopedic or orthodontic treatment aimed at transverse correction.
-
Availability of reliable pre- and post-treatment digital models (T0 and T1).
-
Additional inclusion criterion (data completeness): Availability of complete and analyzable T0 and T1 digital models; sEMG availability was required when the neuromuscular outcomes were reported (Teethan® indices). Exclusion criteria:
-
Cleft palate or other craniofacial malformations.
-
Systemic or craniofacial growth disorders affecting bone metabolism or facial development.
-
Severe airway obstruction or medical conditions incompatible with follow-up.
-
Low compliance or anticipated inability to complete at least 10 months of active therapy.
Sample characteristics
2.4
A total of n = 53 growing patients were assessed for eligibility from the archived clinical records. Of these, n = 11 were excluded (reasons: incomplete T0/T1 digital models n = 5; insufficient treatment duration <10 months n = 2; age out of range n = 3; previous transverse orthopedic treatment n = 1). The remaining n = 42 patients had been treated with AMCOP® appliances during the study period. Among these, n = 30 were excluded from the analysis due to missing post-treatment records or incomplete follow-up documentation. The final case series therefore included n = 12 patients (8 females, 4 males; mean age: 5.6 ± 0.8 years) with complete and analyzable paired T0–T1 digital models (and Teethan® sEMG recordings, where applicable) (Figure 1).
CONSORT-style flow diagram of patient selection. Flow diagram illustrating retrospective identification of growing patients treated with AMCOP® elastodontic appliances, exclusions with reasons, follow-up completeness, and inclusion in the final case series.
Functional orthopedic devices (AMCOP® system)
2.5
All patients were treated using AMCOP® (Apparecchi Modulari di Contenzione Ortopedica Personalizzati) elastodontic appliances [Micerium S.p.A. Registered office: Viale Beatrice D'Este 20, 20122 Milan (MI), Italy.
Operational and administrative headquarters: Via Guglielmo Marconi 83, 16036 Avegno (GE), Italy. Ortho Protec S.r.l., Bari, Italy], following the department's standardized functional orthopedic protocol.
Two main device categories were employed according to clinical needs and palatal morphology:
- AMCOP® Integral—used as a first-phase appliance to release transverse compression, restore correct tongue posture, and achieve neuromuscular balance.
- AMCOP® Class Devices (e.g., Class III)—used, when indicated, only after transverse normalization to refine sagittal relationships. All devices were removable and worn daily according to the prescribed schedule (daytime and nocturnal use). Compliance was assessed through structured verbal parental reporting and chairside questioning during each scheduled 4–6-week follow-up visit. No objective wear-time sensors or electronic monitoring systems were used; therefore, adherence assessment relied solely on subjective reporting. Functional instructions, including nasal breathing, tongue posture and masticatory exercises, were reinforced at each 4–6-week follow-up visit. AMCOP® appliances were selected according to the patient's malocclusion and arch morphology. Device selection followed a standardized clinical protocol based on occlusal classification, palatal morphology, and transverse deficit distribution. Integral appliances were chosen in patients with Class I occlusion or transverse deficiency without sagittal discrepancy, while Class III (TC) devices were selected in the presence of anterior crossbite or skeletal Class III tendency requiring sagittal guidance. Arch form selection (S, OS, F, C) was based on visual and metric assessment of palatal shape (triangular, oval, square/oval, or circular) obtained from intraoral examination and digital models. Device size was determined directly using the manufacturer fitting protocol based on maxillary intermolar width and age-related size charts, aiming for gentle passive insertion without mucosal compression. For Class I malocclusions, the Integral line was used, available in different arch forms (S, OS, F, C); in the present sample, only the S and OS variants were employed. For Class III malocclusions, the TC device was used, which features a single arch form and a specific design of the occlusal plane that promotes maxillary advancement and provides mandibular anchorage. Although all devices share the same elastodontic principles, their morpho-functional differences must be considered when interpreting the clinical and neuromuscular outcomes.
After completion of active treatment, no retention appliances were prescribed, and no standardized post-treatment follow-up visits were scheduled. Therefore, outcome assessment was limited to the active treatment period only.
Device characteristics
2.6
The AMCOP® appliances used in this study are made from a polymer–elastomer blend available in two Shore hardness grades (51 and 60), selected according to functional requirements. The material is elastic and thermoplastic, showing heat-activated adaptability that allows the appliance to conform to individual arch forms. When immersed in hot water at approximately 70 °C for 30 s and then cooled in cold water, the device can undergo controlled expansion and shape stabilization, facilitating individualized fitting.
The AMCOP® bioactivators are available in various sizes, shapes, and colors, corresponding to different skeletal classes and dental arch morphologies. For this study, only devices designed for mixed dentition were used, primarily:
- Class I Integral devices, indicated for basal skeletal discrepancies in the transverse and vertical planes.
- Class III (TC) devices used when transverse contraction was associated with an anterior crossbite tendency. Class I appliances are manufactured with four arch forms and two occlusal plane configurations (Figure 2):
- Arch shapes: F (triangular, dolichocephalic, narrow palate); S (harmonic, mesocephalic, oval palate); OS (oval-square, mesocephalic, broad arch); C (circular, brachycephalic, wide/flat palate).
- Occlusal planes: Integral (flat plane, normal bite) and Basic (thicker anterior plane, increased vertical dimension for deep bites).
AMCOP® class I integral appliances, color-coded for morpho-functional variants: (A) F—triangular, (B) S—harmonic, (C) OS—oval-square, (D) C—circular. Variants differ in buccal contour, transverse width, and flange curvature. Each device differs in transverse width, flange curvature and palatal contour, allowing individualized fitting according to the patient's craniofacial morphology and transverse deficiency pattern.
In patients with anterior crossbite or sagittal discrepancies associated with transverse contraction, the AMCOP® Class III (TC) device was used. This elastodontic bioactivator exerts combined sagittal and transverse functional effects through its inclined occlusal planes and elastic flanges, promoting posterior mandibular repositioning, gradual transverse expansion, and neuromuscular reprogramming.
The Class III device is made of a heat-activated polymer–elastomer blend (Shore 51/60) and features a dual-arch design with inclined occlusal planes guiding mandibular closure. Its flexible flanges promote gradual transverse expansion and neuromuscular rebalancing by centering the tongue and restoring a functional occlusion (Figure 3).
AMCOP® class III (TC) elastodontic appliance. The device features inclined occlusal planes for mandibular repositioning and elastic flanges providing gentle transverse expansion and neuromuscular reprogramming, specifically indicated for early Class III correction associated with maxillary transverse constriction.
Selection of AMCOP® device variants followed a predefined clinical decision protocol based on sagittal occlusal class, presence of anterior crossbite, and transverse deficiency pattern. Integral appliances were selected for patients with Class I occlusion or isolated transverse maxillary deficiency without sagittal discrepancy. Class III (TC) devices were selected for patients presenting anterior crossbite or skeletal Class III tendency requiring sagittal guidance in addition to transverse correction.
Device size selection was based on manufacturer fitting guidelines using maxillary intermolar width measurements obtained from digital models and age-related size charts. The selected appliance size aimed to ensure gentle passive insertion without mucosal compression or excessive deformation. Arch form (S, OS, F, C) was chosen based on visual and metric assessment of palatal morphology derived from digital models (triangular, oval, square/oval, circular) (Table 1).
Digital model acquisition and measurement protocol (Deltadent®)
2.7
Digital dental models were obtained using a 3Shape TRIOS 4 intraoral scanner (3Shape, Copenhagen, Denmark), with a declared accuracy of approximately 20–25 µm according to manufacturer specifications. Scanner calibration was performed following the standard manufacturer protocol prior to each scanning session. Digital impressions were obtained at baseline (T0) and at the end of transverse treatment (T1). Linear transverse measurements were performed on 3D models using Deltadent® software [Manufactured by Outside Format, Via Circonvallazione D 28, 26025 Pandino (CR), Italy].
Reference points and measurements:
- Intercanine width: distance between the palatal gingival margins of upper canines (teeth 13 and 23).
- Inter–second deciduous molar width (“inter-5”): distance between palatal cervical margins of teeth 55 and 65.
- Intermolar width: distance between palatal gingival margins of first permanent molars (16 and 26), when erupted. Intermolar measurements were performed only in patients with fully erupted first permanent molars; no adjustment or imputation was applied for cases without inter-6 data.
- Reference axis: mid-palatal raphe. All measurements were taken by a single calibrated examiner. The examiner was not blinded to treatment stage (T0 vs. T1), due to the retrospective design and the evident chronological features of the digital models. A random subsample (20%) was remeasured after 7 days to assess intra-examiner reliability using the intraclass correlation coefficient (ICC) and Dahlberg's error. Intra-examiner reliability was excellent, with ICC values ranging from 0.92 to 0.98. Dahlberg's error ranged from 0.18 to 0.32 mm. No measurements exceeded the 0.5 mm threshold. Discrepancies > 0.5 mm were re-evaluated, and the average of the two closest values was recorded. The mid-palatal raphe was defined on the 3D models as the sagittal reference line passing through the median palatal suture, visually identified from the posterior nasal spine region to the incisive papilla and digitally traced within the Deltadent® software environment. The measurement plane was oriented perpendicular to this mid-sagittal axis. Transverse distances were recorded between standardized anatomical landmarks identified at the most cervical palatal gingival margin of each reference tooth (canines, second deciduous molars and, when erupted, first permanent molars). Landmark placement was performed in the axial palatal view with the model oriented with the occlusal plane parallel to the horizontal reference plane. Examples of landmark definition and placement on 3D models are shown in Figures 4, 8, 12, and subsequent case figures.
Pre- (A) and post-treatment (B) panoramic radiographs of case 1.
Neuromuscular assessment (Teethan® surface electromyography)
2.8
Neuromuscular balance was assessed through surface electromyography (sEMG) using a portable Teethan® system [Teethan S.p.A. Headquarters: Viale Forlanini 42/A, 20024 Garbagnate Milanese (MI), Italy]. Recordings were obtained at T0 and T1 under standardized conditions (maximum intercuspation in habitual occlusion). Electrode type and placement followed the manufacturer's standardized protocol and SENIAM guidelines for facial sEMG. Disposable Ag/AgCl surface electrodes (diameter 24 mm) were used. After skin cleaning with alcohol, bipolar electrodes were positioned bilaterally over the muscle bellies of the anterior temporalis (TA) and masseter (MM) muscles, with an interelectrode distance of approximately 20 mm, parallel to the muscle fibers. Reference electrodes were positioned according to the system protocol. For postural assessment, electrodes were similarly placed over the sternocleidomastoid (SCM) muscles.
Signals were acquired at a sampling rate of 1,000 Hz and processed using the integrated Teethan® software algorithms, including band-pass filtering and artifact rejection according to the manufacturer's validated protocol. Recordings were obtained during maximal voluntary clenching in habitual intercuspation for 5 s, and three consecutive trials were performed. The trial showing the greatest signal stability was selected for analysis. Data were internally normalized by the Teethan® system using relative bilateral muscle activity ratios, thus no external MVC normalization was required.
All examinations were conducted by the same trained operator following standardized instructions. Although blinding to treatment timing was not feasible due to the clinical design, all recordings were performed under identical acquisition settings to ensure test–retest consistency. The “Impact index” (IMP) provided by the Teethan® system is a normalized, dimensionless score reflecting global muscular efficiency and recruitment quality. According to the manufacturer's validation protocol, IMP is scaled so that a value around 100% corresponds to age- and population-referenced normative mean efficiency; values substantially below 100% indicate reduced muscular recruitment, whereas values above 100% indicate muscular hyperactivity or incoordination beyond normative baseline. Therefore, an increase of 20–30 percentage points in IMP, or a shift from values well below 50% to ≈100%–120%, as observed in most treated cases, can be interpreted as a clinically meaningful improvement in neuromuscular efficiency, consistent with previously published normative data (Rocchetti et al., 2009; Tartaglia et al., 2011).
The following muscles were monitored: anterior temporalis (TA), masseter (MM), and sternocleidomastoid (SCM).
Functional indices analyzed included:
-
POC TA/MM (%): right/left symmetry of activation.
-
BAR (Barycenter): anterior–posterior functional balance.
-
TORS: functional torsion (right/left dominance).
-
ASIM: overall asymmetry index.
-
POC SCM (%): cervical postural symmetry.
-
IMP/CL: global intensity and co-contraction level. Each electromyographic index reflects a specific aspect of neuromuscular balance:
-
POC TA/MM expresses bilateral activation symmetry of the anterior temporalis and masseter muscles (%);
-
BAR (Barycenter) indicates the antero-posterior distribution of muscular activity and functional mandibular positioning;
-
TORS describes right–left dominance and mandibular torsional imbalance;
-
ASIM represents an overall asymmetry coefficient between muscle pairs;
-
IMP (Impact Index) reflects global muscular efficiency and strength of recruitment;
-
CL (Co-contraction Level) represents the degree of muscle coactivation during maximal intercuspation. Values within the physiological range indicate balanced neuromuscular function. Normative thresholds for each index were automatically provided by the validated Teethan® database and were applied consistently across all measurements.
The sEMG data were correlated with morphometric changes (ΔT1–T0) to evaluate neuromuscular rebalancing following transverse correction. A summary of all sEMG functional indices, their definitions, and clinical significance is provided in Table 2.
Normative thresholds and interpretation of teethan® indices
2.9
Interpretation of sEMG indices was based on normative reference values provided by previous validation studies of the Teethan® system [Rocchetti 2009; Tartaglia 2011; Ferrario & Sforza 2012].
The following cut-off values were applied:
- POC TA/MM and POC SCM: values ≥85% indicate physiological bilateral symmetry; values <85% indicate muscular asymmetry.
- BAR (Barycenter): optimal values between 85%–115% indicate balanced antero–posterior distribution of muscular activity; values <85% or >115% indicate posterior or anterior imbalance.
- TORS: physiological range between 85%–115%; values outside this interval indicate mandibular torsional imbalance.
- ASIM: physiological values ≤10%; higher absolute values indicate global muscular asymmetry.
- IMP: optimal efficiency values between 85%–115%; values <85% indicate hypo-activation, while values >115% indicate hyper-activation.
- CL (Co-contraction Level): physiological values ≤15%, reflecting normal muscular synchronization during maximal intercuspation. Accordingly, the terms “normalized” and “within limits” used throughout the manuscript refer to indices shifting into these validated physiological intervals at T1.
Outcomes
2.10.
Primary outcomes:
-
Changes (T1–T0) in intercanine, inter-5, and intermolar widths (mm). Secondary outcomes:
-
Improvement of neuromuscular indices (POC, BAR, TORS, ASIM, POC-SCM, IMP/CL).
-
Clinical correction of posterior crossbite or transverse arch constriction.
Sample size and study power
2.11.
This study was designed as an observational case series of 12 consecutively treated patients, aimed at documenting the clinical and functional effects of AMCOP® therapy.
This study was designed as an exploratory observational case series of 12 consecutively treated patients. No a priori sample size calculation was performed, as the primary aim was descriptive: to document morphometric and neuromuscular trends associated with AMCOP® therapy in early mixed dentition.
Considering the absence of inferential analysis, post-hoc evaluation focused on the magnitude of observed changes (effect size in a clinical sense). Mean transverse gains ranging from approximately 3 to 5 mm represent clinically meaningful effects for interceptive orthopedic therapy in this age group.
Data management and quality control
2.12.
All data were pseudonymized and securely stored in the department's protected database.
Digital models, sEMG recordings, and clinical photographs were analyzed within a standardized workflow.
Periodic quality checks verified the consistency of landmark identification and the reproducibility of measurements.
Statistical considerations
2.13.
Given the retrospective case-series design and the limited sample size, no inferential statistical analyses were planned or performed. No hypothesis testing, confidence intervals, or significance thresholds were applied. Data were summarized descriptively as mean ± standard deviation and range to describe within-subject pre–post variations. In addition, post-hoc standardized mean change (SMC) effect sizes were calculated for the primary transverse outcomes using the ratio of mean change to standard deviation of the change scores. Effect size values were interpreted according to Cohen's thresholds (0.2 small, 0.5 moderate, 0.8 large). Results should therefore be considered exploratory and descriptive rather than evidence of treatment efficacy.
Case series
3
Case 1—C.S., female, 5 years
3.1
Dentition stage: Early mixed dentition.
Diagnosis: Maxillary transverse deficiency with mild unilateral posterior crossbite.
Appliance: AMCOP® Integral S; worn 1 h per day plus every night, for a total of 12 months.
Radiographic assessment
3.1.1
Pre- and post-treatment panoramic radiographs confirmed normal root development and eruption pattern.
The post-treatment image showed adequate space for the eruption of the permanent incisors and early molars, without dental or skeletal asymmetries (Figures 4A,B).
Digital model analysis
3.1.2
Digital 3D models obtained with Deltadent® were analyzed for transverse measurements (Figures 5A,B).
Digital 3D models: (A) pre-treatment (yellow), (B) post-treatment (blue). Colored guidelines correspond to the measured inter-dental distances and are shown for visual reference only.
The reference landmarks corresponded to the palatal gingival margins of the upper canines, second deciduous molars, and first permanent molars when erupted.
Transverse measurements (Table 3) were associated with increases observed in both the anterior and posterior maxillary regions.
Qualitative 3D inspection confirmed a symmetrical transverse expansion, improved occlusal interdigitation, and enhanced arch coordination (Figure 4).
Digital bite evaluation
3.1.3
Color-coded occlusal digital models were generated for qualitative comparison of the maxillary and mandibular arches (Figures 6A,B).
Digital occlusal models at pre- (A) and post-treatment (B) Pre-treatment models (A) are color-coded in yellow, with two shades (darker = maxillary, lighter = mandibular) to distinguish the arches; post-treatment models (B) are color-coded in blue. These renders provide a qualitative overview of transverse coordination and occlusal improvement obtained with elastodontic therapy.
Surface electromyography (Teethan®) assessment
3.1.4
Neuromuscular activity was recorded at baseline and after 12 months of treatment using Teethan® sEMG.
The analysis revealed marked improvement in muscle symmetry and coordination, particularly in the temporalis (TA) and masseter (MM) pairs (Table 4, Figure 7).
Teethan® surface electromyography [(A): pre-treatment; (B): post-treatment]. Post-treatment data show restoration of muscle symmetry and improved functional barycenter distribution.
Interpretation
3.1.5
After 12 months of AMCOP® Integral S therapy, the patient showed:
- Clinically significant transverse widening (+3.1 to +4.0 mm at all reference points);
- Balanced arch form with improved occlusal coordination;
- Neuromuscular normalization on sEMG, including restored barycenter position and reduced asymmetry indices. Minor residual variability in SCM activation (≈82.5%) was interpreted as within physiological limits for a 5-year-old, likely influenced by cooperation during EMG recording rather than by true dysfunction.
Overall, the observed combination of transverse dimensional changes and neuromuscular index variations was associated with early elastodontic intervention.
Case 2—V.S., male, 7 years
3.2
Dentition stage: Early mixed dentition.
Diagnosis: Maxillary transverse deficiency associated with a mild skeletal Class III pattern.
Appliance: AMCOP® Class III (TC); worn 1 h per day plus every night, for a total of 10 months.
Radiographic assessment
3.2.1
Panoramic radiographs (Figure 8) were obtained to document dental development and eruption sequence.
Pre- (A) and post-treatment (B) panoramic radiographs of case 2.
No skeletal anomalies or asymmetric root morphology were noted, confirming suitability for functional elastodontic therapy.
Digital model analysis (palatal view)
3.2.2
Digital 3D models obtained with Deltadent® were analyzed at baseline (T0) and after 10 months (T1).
Quantitative measurements (Table 5) show homogeneous anterior and posterior expansion, with a gain of approximately **+**4.6 mm intercanine and +4.9 mm intermolar, indicating a balanced and effective transverse correction.
Clinical interpretation
3.2.3
The patient exhibited a harmonic transverse expansion, with comparable anterior and posterior widening.
Given the patient's age (7 years) and the 10-month therapy duration with an AMCOP® Class III device, the increase is clinically significant; a small portion may reflect normal growth, but the magnitude clearly suggests a therapeutic effect (Figure 9).
Digital 3D models of case 2 [(A): pre-treatment; (B): post-treatment]. Yellow = pre-treatment; blue = post-treatment. Colored guide lines correspond to the inter-dental distances measured with Deltadent®.
Digital bite evaluation
3.2.4
Color-coded occlusal digital models (Figures 10A,B) were used to qualitatively assess changes in occlusal coordination.
Digital occlusal models at pre- (A) and post-treatment (B) Pre-treatment model (A) = yellow (darker = maxillary, lighter = mandibular); post-treatment (B) = blue.
The post-treatment model shows improved arch form balance, correction of anterior crossbite tendency, and better interdigitation between upper and lower arches (Figure 10).
Surface electromyography (Teethan®) assessment
3.2.5
Neuromuscular function was analyzed with Teethan® sEMG at baseline and after 10 months of treatment.
Functional indices demonstrated a marked normalization of muscle coordination and barycenter alignment (Table 6, Figures 11A,B).
Teethan® surface electromyography [(A): pre-treatment; (B): post-treatment]. Post-treatment data show normalization of the barycenter, balanced temporalis and masseter activity and reduction of asymmetry and torsion indices.
Interpretation
3.2.6
After 10 months of AMCOP® TC therapy, the patient demonstrated:
- Significant and uniform transverse expansion (+4.5 to +4.9 mm at all levels);
- Resolution of anterior crossbite tendency and improved transverse coordination;
- Restoration of neuromuscular symmetry, with normalization of POC, BAR, and TORS values. The marked improvement in interarch coordination and muscle balance supports the functional orthopedic efficacy of AMCOP® Class III elastodontic therapy in guiding early craniofacial growth.
Case 3—M.P., female, 6 years
3.3
Dentition stage: Early mixed dentition.
Diagnosis: Maxillary transverse deficiency with anterior constriction tendency, associated with mild skeletal Class III pattern.
Appliance: AMCOP® Integral, shape S; worn 1 h per day plus every night, for a total of 16 months.
Radiographic assessment
3.3.1
Panoramic radiographs (Figure 12) confirmed regular dental development and symmetric root morphology.
Pre- (A) and post-treatment (B) panoramic radiographs of case 3.
The eruption sequence was appropriate for the age, with adequate space for the eruption of permanent incisors and first molars.
No skeletal asymmetries were detected.
Digital model analysis (palatal view)
3.3.2
Digital 3D models were obtained at baseline (T0) and after 16 months of therapy (T1) using Deltadent® software.
Transverse measurements revealed a more pronounced anterior than posterior expansion, consistent with the expected action of the Integral device (Table 7, Figures 13A,B).
Digital 3D models of case 3 [(A): pre-treatment; (B): post-treatment]. Yellow = pre-treatment; blue = post-treatment. Colored guidelines correspond to the transverse distances analyzed.
Clinical interpretation
3.3.3
The transverse expansion was greater in the anterior region (≈+4.2 mm) than posteriorly (≈+3.3 mm), in accordance with the selective anterior action of the Integral appliance.
The intercanine increase corresponds to an average of 0.42 mm/month, representing a clinically meaningful gain for widening the anterior corridor and improving the sagittal relationship typical of Class III cases.
Digital bite evaluation
3.3.4
Color-coded occlusal models (Figures 14A,B) showed improved anterior arch coordination and increased transverse width.
Digital occlusal models at pre- (A) and post-treatment (B). Pre-treatment models (A) are color-coded in yellow (darker shade for maxillary, lighter for mandibular arches); post-treatment models (B) are color-coded in blue. The images provide a qualitative overview of transverse improvement and occlusal balance.
Post-treatment images demonstrated enhanced occlusal interdigitation and symmetry between the maxillary and mandibular arches.
Surface electromyography (Teethan®) assessment
3.3.5
Neuromuscular recordings using Teethan® sEMG were obtained before and after treatment.
Functional indices indicated a clear improvement in muscle coordination, with normalization of barycenter and asymmetry parameters (Table 8, Figures 15A,B).
Teethan® surface electromyography [(A): pre-treatment; (B): post-treatment]. Post-treatment values show normalization of the barycenter, reduction of asymmetry and torsion, and balanced activation of temporalis and masseter muscles.
Interpretation
3.3.6
After 16 months of AMCOP® Integral S therapy, the patient showed:
- Greater anterior than posterior expansion, consistent with the appliance's selective effect;
- Transverse gain of 4.2 mm intercanine and 3.3 mm intermolar, with visible improvement in occlusal coordination;
- Normalization of neuromuscular indices, including balanced masseter and temporalis activation and corrected barycenter position. The treatment resulted in a stable transverse expansion and functional rebalancing, confirming the efficiency of AMCOP® elastodontic therapy in early mixed dentition.
Case 4—I.R., female, 6 years
3.4
Dentition stage: Early mixed dentition.
Diagnosis: Maxillary transverse deficiency with constricted arch form and mild functional imbalance.
Appliance: AMCOP® Integral OS; worn 1 h per day plus every night, for a total of 12 months.
Radiographic assessment
3.4.1
Panoramic radiographs (Figure 16) revealed normal root morphology and symmetrical eruption paths of both arches.
Pre- (A) and post-treatment (B) panoramic radiographs of case 4.
No skeletal asymmetries or pathologic findings were detected.
Adequate eruption space for permanent incisors and molars was observed after treatment.
Digital model analysis (palatal view)
3.4.2
Digital 3D models were analyzed using Deltadent® software.
Quantitative data demonstrated a uniform and clinically significant expansion of the maxillary arch both anteriorly and posteriorly (Table 9, Figure 17).
Digital 3D models of case 4 [(A): pre-treatment; (B): post-treatment]. Yellow = pre-treatment; blue = post-treatment. Colored reference lines correspond to the inter-dental distances measured in the analysis.
Clinical interpretation
3.4.3
After 12 months of AMCOP® Integral OS therapy, the patient showed marked skeletal widening, particularly in the posterior region (+6.3 mm), indicating a balanced orthopedic response and correction of the maxillary constriction.
The expansion pattern was harmonic, with well-maintained symmetry and improved palatal morphology.
Digital bite evaluation
3.4.4
Color-coded occlusal digital models (Figures 18A,B) demonstrated improved arch coordination and occlusal interdigitation following treatment.
Digital occlusal models at pre- (A) and post-treatment (B). Pre-treatment models (A) are color-coded in yellow (darker = maxillary, lighter = mandibular); post-treatment models (B) are in blue. Images illustrate improved transverse coordination and occlusal balance after therapy.
The post-treatment model (blue) shows balanced alignment between upper and lower arches and a wider anterior arch form.
Surface Electromyography (Teethan®) assessment
3.4.5
Neuromuscular activity was recorded using Teethan® sEMG before and after AMCOP® therapy.
At baseline, electromyographic data revealed a posterior barycenter and mild right-side predominance.
After treatment, all indices normalized, with barycenter repositioning and muscle symmetry restoration (Table 10, Figures 19A,B).
Teethan® surface electromyography [(A): pre-treatment; (B): post-treatment]. The post-treatment sEMG showed normalization of the barycenter, improved temporalis–masseter coordination, and reduction of asymmetry indices.
Interpretation
3.4.6
After 12 months of AMCOP® Integral OS therapy, the patient exhibited:
- Significant transverse expansion, particularly posteriorly (+6.3 mm);
- Balanced arch development and restoration of occlusal coordination;
- Normalization of neuromuscular activity, with barycenter repositioned from posterior to anterior and reduced torsional asymmetry. The combined morphometric and sEMG data confirm the efficacy of elastodontic functional therapy in harmonizing both skeletal and neuromuscular parameters in growing patients.
Case 5—D.I., female, 6.5 years
3.5
Dentition stage: Early mixed dentition.
Diagnosis: Maxillary transverse deficiency with posterior constriction and functional Class I tendency.
Appliance: AMCOP® Integral OS; worn 1 h per day plus every night, for a total of 12 months.
Radiographic assessment
3.5.1
Panoramic radiographs (Figure 20) confirmed symmetrical dental development and absence of structural anomalies.
Pre- (A) and post-treatment (B) panoramic radiographs of case 5.
The eruption sequence of permanent incisors and first molars was appropriate for the patient's age, with no skeletal or dental asymmetries observed after treatment.
Digital model analysis (palatal view)
3.5.2
Digital models acquired using Deltadent® software demonstrated significant transverse expansion in both the anterior and posterior regions, with a slightly higher posterior gain (Table 11, Figure 21).
Digital 3D models of case 5 [(A): pre-treatment; (B): post-treatment]. Yellow = pre-treatment; blue = post-treatment. Reference lines show measured transverse distances.
Clinical interpretation
3.5.3
After 12 months of AMCOP® Integral OS therapy, the patient achieved showed a trend toward improved symmetry across the entire maxillary arch.
The intercanine gain (+4.7 mm) and intermolar gain (+6.2 mm) indicate effective anterior and posterior remodeling, consistent with the appliance's biomechanical design.
A minor posterior predominance was noted, suggesting a balanced skeletal and functional response.
Digital bite evaluation
3.5.4
Color-coded occlusal models (Figures 22A,B) confirmed improved arch symmetry, enhanced transverse dimension, and better occlusal interdigitation following elastodontic therapy.
Digital occlusal models at pre- (A) and post-treatment (B). Pre-treatment models (A) are color-coded in yellow (darker = maxillary, lighter = mandibular); post-treatment models (B) are in blue.
The post-treatment occlusal view demonstrated a stable arch shape and proper coordination between upper and lower arches.
Surface electromyography (Teethan®) assessment
3.5.5
Neuromuscular evaluation with Teethan® sEMG was conducted before and after AMCOP® therapy.
The pre-treatment test revealed a posterior barycenter with left-side temporalis predominance and reduced global muscle efficiency. At the end of treatment, symmetry and coordination markedly improved, as shown in Table 12 and Figures 23A–C.
Teethan® surface electromyography. (A) Pre-treatment (without rollers), (B) post-treatment (without rollers), (C) post-test with elastodontic device. Post-treatment data indicate enhanced neuromuscular activation and reduced asymmetry, with improved barycenter distribution and temporalis–masseter balance.
Interpretation
3.5.6
At 12 months of follow-up, the patient exhibited:
- Increases in transverse skeletal dimensions anterior +4.7 mm, posterior +6.2 mm;
- Restoration of transverse arch symmetry and proper occlusal coordination;
- Improved neuromuscular function, with normalization of POC indices and increased global muscle efficiency (IMP 135.6%);
- Stable barycenter and balanced temporalis–masseter activation. The overall morphometric and sEMG findings were associated with favorable transverse and neuromuscular changes observed following AMCOP® elastodontic therapy in early mixed dentition.
Case 6—E.V., male, 7 years
3.6
Dentition stage: Early mixed dentition.
Diagnosis: Maxillary transverse deficiency with anterior constriction and functional imbalance.
Appliance: AMCOP® Integral S; worn 1 h per day plus every night, for a total of 14 months.
Radiographic assessment
3.6.1
Panoramic radiographs (Figure 24) revealed symmetrical dental development and absence of pathologic findings.
Pre- (A) and post-treatment (B) panoramic radiographs of case 6.
Post-treatment imaging confirmed improved maxillary width and adequate space for the eruption of permanent teeth.
Digital model analysis (palatal view)
3.6.2
Digital 3D models were analyzed using Deltadent® software to assess transverse dimensional changes.
The expansion pattern was more pronounced posteriorly, with significant improvement at the level of the deciduous molars (Table 13, Figure 25).
Digital 3D models of case 6 [(A): pre-treatment; (B): post-treatment]. Yellow = pre-treatment; blue = post-treatment. Colored reference lines indicate measured transverse distances.
Clinical interpretation
3.6.3
The patient showed a modest anterior expansion (+1 mm) and a greater posterior gain (+3.6 mm), indicating a physiologic, fan-shaped widening of the maxilla.
This pattern reflects the expected biomechanical response to the Integral S device, aimed at promoting posterior development and transverse symmetry.
Digital bite evaluation
3.6.4
Color-coded occlusal digital models (Figures 26A,B) confirmed improved coordination between maxillary and mandibular arches, with increased posterior transverse dimension and more stable occlusal interdigitation.
Digital occlusal models at pre- (A) and post-treatment (B). Pre-treatment models (A) are color-coded in yellow (darker = maxillary, lighter = mandibular); post-treatment models (B) are in blue.
Surface electromyography (Teethan®) assessment
3.6.5
sEMG evaluation was performed before and after 14 months of elastodontic therapy.
At baseline, muscle recruitment was asymmetric, with a markedly anterior barycenter and low global muscle efficiency.
Post-treatment data revealed normalized activation patterns, improved symmetry, and balanced temporalis–masseter coordination (Table 14, Figures 27A–C).
Teethan® surface electromyography. (A) Pre-treatment (without rollers), (B) post-treatment (without rollers) and with elastodontic device. After therapy, a significant increase in muscle efficiency and normalization of barycenter position were recorded.
Interpretation
3.6.6
After 14 months of AMCOP® Integral S therapy, the patient exhibited:
- Posteriorly predominant transverse expansion (+3.6 mm at deciduous molars);
- Improved arch coordination and occlusal stability;
- Marked neuromuscular improvement, with normalization of temporalis–masseter symmetry and restoration of balanced barycenter position;
- Increased muscle efficiency (IMP +68%), reflecting better recruitment quality. These findings confirm that the AMCOP® Integral S appliance effectively supported both skeletal and functional balance in mixed dentition.
Case 7—A.D.V., male, 7 years
3.7
Dentition stage: Early mixed dentition.
Diagnosis: Maxillary transverse deficiency with mild posterior constriction.
Appliance: AMCOP® Integral S; worn 1 h per day plus every night, for a total of 12 months.
Radiographic assessment
3.7.1
Panoramic radiographs (Figure 28) revealed normal dental and skeletal development for age.
Pre- (A) and post-treatment (B) panoramic radiographs of case 7.
No asymmetries or eruption disturbances were observed at baseline or after treatment.
Post-treatment evaluation confirmed an increased maxillary width and adequate spacing for the eruption of permanent teeth.
Digital model analysis (palatal view)
3.7.2
Digital 3D models acquired with Deltadent® software were analyzed for transverse changes.
Quantitative data demonstrated mild but uniform expansion across the entire maxillary arch (Table 15, Figure 29).
Digital 3D models of case 7 [(A): pre-treatment; (B): post-treatment]. Yellow = pre-treatment; blue = post-treatment. Colored reference lines correspond to inter-dental measurements used for quantitative analysis.
Clinical interpretation
3.7.3
After 12 months of AMCOP® Integral S therapy, the patient exhibited mild but consistent transverse gain in all regions of the arch, with the greatest widening at the molar level (+1.8 mm).
This pattern reflects a balanced expansion of the maxillary base with preservation of arch symmetry and improved coordination of occlusal planes.
Digital bite evaluation
3.7.4
Color-coded occlusal digital models (Figures 30A,B) showed enhanced coordination between the upper and lower arches, with improvement in posterior intercuspation and a more stable transverse relationship following therapy.
Digital occlusal models at pre- (A) and post-treatment (B). Pre-treatment models (A) are color-coded in yellow (darker = maxillary, lighter = mandibular); post-treatment models (B) are in blue. The visualization highlights improved arch coordination and occlusal symmetry.
Surface electromyography (Teethan®) assessment
3.7.5
Neuromuscular analysis with Teethan® sEMG was performed before and after AMCOP® therapy.
The baseline test revealed anterior barycenter displacement and right-sided muscular predominance (temporalis and SCM), with low overall muscle efficiency.
After treatment, barycenter repositioning and improved bilateral coordination were observed, as detailed in Table 16 and Figures 31A,B.
Teethan® surface electromyography. (A) Pre-treatment (without rollers); (B) post-treatment (without rollers). Post-therapy evaluation demonstrated normalization of barycenter position and improved temporalis–masseter balance, with overall enhancement in neuromuscular coordination.
Interpretation
3.7.6
After 12 months of AMCOP® Integral S therapy, the patient showed:
- Mild but consistent transverse gain across all maxillary regions (+1.1–1.8 mm);
- Improved occlusal stability and coordination between arches;
- Neuromuscular improvement, with normalization of barycenter position, reduction of asymmetry indices, and enhanced muscle efficiency (IMP +9%). The results support the role of AMCOP® Integral S therapy in guiding physiological maxillary development and promoting functional balance in early mixed dentition.
Case 8—M.M., female, 5 years
3.8
Dentition stage: Early mixed dentition.
Diagnosis: Maxillary transverse deficiency with mild anterior constriction.
Appliance: AMCOP® TC; worn 1 h per day plus every night, for a total of 18 months.
Radiographic assessment
3.8.1
Panoramic radiographs (Figure 32) confirmed a regular dental development for age and symmetry of skeletal structures.
Pre- (A) and post-treatment (B) panoramic radiographs of case 8.
No signs of asymmetry, rotation, or delayed eruption were observed after treatment.
Digital model analysis (palatal view)
3.8.2
Digital 3D models were analyzed using Deltadent® software to quantify the transverse expansion of the maxillary arch.
Substantial anterior and posterior gains were recorded, indicating a broad and homogeneous maxillary response to treatment (Table 17, Figure 33.
Digital 3D models of case 8 [(A): pre-treatment; (B): post-treatment]. Yellow = pre-treatment; blue = post-treatment. Transverse reference lines illustrate the measured intercanine and intermolar distances.
Clinical interpretation
3.8.3
The patient exhibited significant expansion, more pronounced in the anterior region (+4.9 mm intercanine vs. + 4.1 mm posterior), resulting in an overall widening of the upper arch and a more favorable anterior corridor.
The magnitude of the increase suggests both a functional and skeletal contribution of the AMCOP® TC appliance.
Digital bite evaluation
3.8.4
Color-coded digital occlusal models confirmed a marked improvement in arch symmetry and occlusal balance (Figure 34).
Digital occlusal models at pre- (A) and post-treatment (B). Pre-treatment models (A) are color-coded in yellow (darker = maxillary, lighter = mandibular); post-treatment models (B) are in blue.
Post-treatment visualization revealed smoother arch curvature and greater intercuspation between maxillary and mandibular teeth.
Surface electromyography (Teethan®) assessment
3.8.5
sEMG analysis was performed using Teethan® before and after the AMCOP® TC treatment.
At baseline, the patient presented anterior barycenter displacement, low muscle efficiency, and left-sided predominance in temporalis and masseter activation.
After 18 months, muscle symmetry and coordination improved substantially, as summarized in Table 18 and Figures 35A,B.
Teethan® surface electromyography. (A) Pre-treatment (without rollers); (B) post-treatment (without rollers). The post-therapy pattern shows normalization of barycenter position, balanced temporalis–masseter activity and improved overall neuromuscular coordination.
Interpretation
3.8.6
After 18 months of AMCOP® TC therapy, the patient demonstrated:
- Marked transverse expansion, particularly anteriorly (+4.9 mm), with posterior improvement (+4.1 mm);
- Restoration of arch symmetry and improved interarch coordination;
- Normalization of sEMG indices, with balanced temporalis and masseter activity;
- Improved barycenter position and reduced asymmetry;
- Overall neuromuscular optimization, consistent with efficient functional adaptation. The combined morphometric and electromyographic outcomes confirm the efficacy of AMCOP® TC in promoting balanced skeletal and muscular development during early mixed dentition.
Case 9—L.L., female, 5 years
3.9
Dentition stage: Early mixed dentition.
Diagnosis: Maxillary transverse deficiency with anterior constriction and functional imbalance.
Appliance: AMCOP® TC; worn 1 h per day plus every night, for a total of 14 months.
Radiographic assessment
3.9.1
Panoramic radiographs (Figure 36) revealed normal root morphology and symmetric development of both dental arches.
Pre- (A) and post-treatment (B) panoramic radiographs of case 9.
No asymmetries or delayed eruptions were noted before or after therapy.
Digital model analysis (palatal view)
3.9.2
Three-dimensional digital models were obtained and analyzed with Deltadent® software.
A mild yet consistent transverse gain was observed in both anterior and posterior regions of the maxilla (Table 19, Figure 37).
Digital 3D models of case 9 [(A): pre-treatment; (B): post-treatment]. Yellow = pre-treatment; blue = post-treatment. Reference lines indicate transverse measurement levels.
Clinical interpretation
3.9.3
The arch displayed a predominantly posterior widening pattern, with a larger increase at the molar level (+2.2 mm) compared to the anterior region (+0.5 mm).
The result reflects a controlled expansion of the maxillary base consistent with the biomechanical action of the AMCOP® TC appliance.
Digital bite evaluation
3.9.4
Occlusal color-coded digital models confirmed enhanced posterior coordination and improved intercuspation, particularly in the right molar region, with balanced development of the transverse dimension (Figure 38).
Digital occlusal models at pre- (A) and post-treatment (B) Pre-treatment models (A) are color-coded in yellow (darker = maxillary, lighter = mandibular); post-treatment models (B) are in blue.
Surface electromyography (Teethan®) assessment
3.9.5
Surface EMG (Teethan®) analysis was performed before and after 14 months of AMCOP® TC therapy.
At baseline, the patient exhibited an anterior barycenter, right-sided temporalis predominance, and low overall muscle efficiency.
After treatment, barycenter position improved, and muscular balance between sides was restored (Table 20, Figures 39A,B).
Teethan® surface electromyography. (A) Pre-treatment (without rollers); (B) post-treatment (without rollers) and with elastodontic device. The post-treatment trace showed normalization of barycenter position and improved activation symmetry, consistent with enhanced neuromuscular control.
Interpretation
3.9.6
After 14 months of AMCOP® TC therapy, the patient demonstrated:
- Posteriorly predominant expansion, especially at the deciduous molar level (+2.16 mm);
- Improved occlusal coordination and arch symmetry;
- Neuromuscular rebalancing, with normalization of barycenter position and increased efficiency (IMP +32%);
- Functional stabilization, indicating restored temporalis–masseter coordination and improved postural muscle control. The combined morphometric and electromyographic results confirm that AMCOP® TC therapy effectively harmonized skeletal and functional parameters, supporting stable maxillary development in early mixed dentition.
Case 10—A.G.V., female, 4 years
3.10
Dentition stage: Early mixed dentition (emerging first permanent molars).
Diagnosis: Maxillary transverse deficiency with reduced anterior arch width.
Appliance: AMCOP® Integral S1; worn 1 h per day plus every night, for a total of 12 months.
Radiographic assessment
3.10.1
Panoramic radiographs (Figure 40) revealed normal eruption patterns and symmetric skeletal growth.
Pre- (A) and post-treatment (B) panoramic radiographs of case 10.
No pathological findings or asymmetries were detected pre- or post-treatment.
Digital model analysis (palatal view)
3.10.2
Digital 3D models obtained through Deltadent® software were used to evaluate transverse changes.
A marked anterior and posterior expansion was observed after therapy (Table 21, Figure 41).
Digital 3D models of case 10 [(A): pre-treatment; (B): post-treatment]. Yellow = pre-treatment; blue = post-treatment. Colored guidelines represent the transverse reference points for measurement.
Clinical interpretation
3.10.3
The patient exhibited a harmonic anterior and posterior expansion, with slightly greater widening in the intercanine region (+3.7 mm) than posteriorly (+3.4 mm).
This pattern is consistent with the expected action of the AMCOP® S1 Integral device, which promotes anterior development and corrects transverse deficiency while maintaining arch symmetry.
Digital bite evaluation
3.10.4
Qualitative analysis of color-coded occlusal models revealed improved arch coordination, increased transverse width, and enhanced intercuspation between maxillary and mandibular arches (Figure 42).
Digital occlusal models at pre- (A) and post-treatment (B). Pre-treatment models (A) are color-coded in yellow (darker for the maxillary arch, lighter for mandibular); post-treatment models (B) are in blue. Visualization confirms improved symmetry and transverse coordination following elastodontic therapy.
Posterior occlusal balance improved markedly after therapy.
Surface electromyography (Teethan®) assessment
3.10.5
Surface electromyographic recordings (Teethan®) were performed before and after AMCOP® therapy.
At baseline, the patient exhibited markedly anterior barycenter, low muscle efficiency, and asymmetric temporalis–masseter activation.
After 12 months, a significant improvement was observed in muscle recruitment balance, despite a persistent mild right predominance (Table 22, Figures 43A,B).
Teethan® surface electromyography. (A) Pre-treatment (without rollers); (B) post-treatment (with elastodontic device). Post-therapy traces demonstrate restored muscle balance, normalization of barycenter position, and a shift toward efficient neuromuscular recruitment.
Interpretation
3.10.6
After 12 months of AMCOP® Integral S1 therapy, the patient showed:
- Significant transverse gain, both anteriorly (+3.7 mm) and posteriorly (+3.4 mm);
- Improved occlusal coordination and arch symmetry;
- Marked neuromuscular rebalancing, with normalization of POC indices and barycenter alignment;
- Enhanced muscle efficiency, consistent with optimal adaptation to the elastodontic correction. Overall, the treatment led to a functional and morphological normalization of the maxillary arch and masticatory system in early mixed dentition.
Case 11—L.P., male, 7 years
3.11
Dentition stage: Early mixed dentition.
Diagnosis: Skeletal Class III with maxillary transverse deficiency.
Appliance: AMCOP® Class III device; worn 1 h per day plus every night, for a total of 12 months.
Radiographic assessment
3.11.1
Panoramic evaluation (Figure 44) confirmed proper eruption timing, normal root morphology, and symmetrical skeletal development.
Pre- (A) and post-treatment (B) panoramic radiographs of case 11.
No anomalies or dental asymmetries were observed after treatment.
Digital model analysis (palatal view)
3.11.2
Transverse maxillary dimensions were analyzed using Deltadent® software.
A uniform anterior–posterior expansion was recorded, indicating effective correction of transverse deficiency (Table 23, Figure 45).
Digital 3D models of case 11 [(A): pre-treatment; (B): post-treatment]. Yellow = pre-treatment; blue = post-treatment. Colored reference lines highlight transverse width measurements.
Clinical interpretation
3.11.3
The patient achieved a broad and harmonic maxillary expansion, greater in the premolar region (+5.4 mm), suggesting optimal stimulation of the midpalatal suture and dentoalveolar remodeling.
The intercanine gain (+4.2 mm) reflects balanced anterior development, suitable for early Class III correction.
Digital bite evaluation
3.11.4
Qualitative 3D analysis demonstrated correction of anterior constriction and posterior crossbite tendency.
The post-treatment model revealed improved transverse coordination and symmetrical intercuspation (Figure 46).
Digital occlusal models at pre- (A) and post-treatment (B). Pre-treatment model (A) in yellow; post-treatment model (B) in blue, showing enhanced arch symmetry and occlusal integration.
Surface electromyography (Teethan®) assessment
3.11.5
Surface electromyography (Teethan®) was used to evaluate neuromuscular balance before and after AMCOP® therapy.
At baseline, muscle activity was within normal limits but characterized by slightly anterior barycenter and moderate asymmetry.
After 12 months, a significant improvement in barycenter position and muscle coordination was detected (Table 24, Figures 47A,B).
Teethan® surface electromyography. (A) Pre-treatment (without rollers); (B) post-treatment (without rollers). The post-therapy trace demonstrates restored barycenter position, enhanced temporalis and masseter coordination, and normalization of muscle efficiency.
Interpretation
3.11.6
After 12 months of AMCOP® Class III therapy, the patient demonstrated:
- Marked transverse expansion, especially at the premolar level (+5.4 mm);
- Functional correction of anterior maxillary constriction;
- Normalization of barycenter position and muscle symmetry;
- Improved neuromuscular efficiency (IMP ↑ from 23.8% → 95.6%);
- Stable occlusal and muscular balance, consistent with functional adaptation. These findings describe transverse dimensional changes and neuromuscular pattern variations observed in association with early AMCOP® Class III therapy in growing patients.
Case 12—G.D.D., female, 7 years
3.12
Dentition stage: Early mixed dentition.
Diagnosis: Maxillary transverse deficiency with mild anterior constriction and neuromuscular imbalance.
Appliance: AMCOP® OS Integral; worn 1 h per day plus every night, for a total of 14 months.
Radiographic assessment
3.12.1
Panoramic radiographs (Figure 48) revealed a regular eruption sequence, normal root morphology, and symmetric skeletal growth.
Pre- (A) and post-treatment (B) panoramic radiographs of case 12.
No dental anomalies were detected before or after treatment.
Digital model analysis (palatal view)
3.12.2
Three-dimensional Deltadent® analysis showed a marked improvement in transverse maxillary dimensions following AMCOP® OS Integral therapy (Table 25, Figure 49).
Digital 3D models of case 12 [(A): pre-treatment; (B): post-treatment]. Yellow = pre-treatment; blue = post-treatment. Reference lines indicate the measurement planes for transverse analysis.
Clinical interpretation
3.12.3
The digital analysis demonstrates uniform maxillary widening, with the greatest transverse gain observed in the premolar region (+4.9 mm).
This reflects a harmonic skeletal and dentoalveolar response, typical of AMCOP® OS Integral therapy, which effectively corrects posterior constriction while preserving anterior arch form.
Digital bite evaluation
3.12.4
Color-coded occlusal models confirmed improved transverse coordination and symmetry.
Post-treatment evaluation revealed normalized posterior occlusal contacts and functional alignment of the maxillary arch (Figure 50).
Digital occlusal models at pre- (A) and post-treatment (B). Pre-treatment models (A) are shown in yellow, post-treatment models (B) in blue. Post-treatment changes include increased posterior width and improved occlusal interdigitation.
Surface electromyography (Teethan®) assessment
3.12.5
Surface electromyography (Teethan®) was performed before and after AMCOP® OS Integral therapy.
At baseline, findings indicated an anterior barycenter, reduced impact index (IMP), and left-side predominance.
After 14 months of treatment, muscle balance and coordination improved significantly, with normalization of barycenter position and functional indices (Table 26, Figures 51A,B).
Teethan® surface electromyography. (A) Pre-treatment (without rollers); (B) post-treatment (with elastodontic device). After treatment, the barycenter shifted posteriorly, torsion normalized, and the impact index increased, indicating improved neuromuscular coordination and work efficiency.
Interpretation
3.12.6
After 14 months of AMCOP® OS Integral therapy, the patient exhibited:
- Significant maxillary expansion across all reference points (Δ + 3.9–4.9 mm);
- Improved transverse and occlusal symmetry, particularly in the premolar and molar regions;
- Marked neuromuscular rebalancing, with normalization of barycenter (BAR ↑ from 47% → 90%) and IMP (↑ from 65% → 102%);
- Physiological muscle activation, indicating restoration of functional equilibrium. The combination of morphometric and sEMG results confirms that AMCOP® OS Integral therapy effectively harmonized both skeletal and neuromuscular parameters in this early mixed dentition case.
Results
4
Sample and treatment overview
4.1
Twelve growing patients (8 females, 4 males; mean age 5.6 ± 0.8 years) completed treatment with AMCOP® elastodontic appliances. Therapy duration ranged from 10 to 18 months (per-protocol wear: 1 h/day + night-time use).
Patient selection was based exclusively on the presence of transverse maxillary deficiency; sagittal class was not considered an inclusion or exclusion criterion.
Intra-examiner reliability
4.2
Intra-examiner reliability analysis demonstrated excellent agreement for all transverse measurements. Intraclass correlation coefficient (ICC) values ranged from 0.92 to 0.98. Dahlberg's measurement error ranged between 0.18 and 0.32 mm. No repeated measurements exceeded the predefined tolerance threshold of 0.5 mm; therefore, no additional remeasurement or correction procedures were required.
Primary outcome: transverse changes on digital models
4.3
All patients exhibited an increase in transverse dimensions at the intercanine level, at the second deciduous molars (inter-5), and—when erupted—at the first permanent molars (inter-6). Aggregate data are summarized in Table 27.
The transverse gain was generally homogeneous between anterior and posterior regions.
In cases treated with Class III (TC) devices, a slightly greater anterior expansion was observed, consistent with the functional design rationale, whereas Integral and OS devices showed a more harmonic or slightly posterior-dominant pattern. No reduction in transverse width was recorded in any patient. All repeated measurements fell within the pre-defined tolerance limit (≤0.5 mm). Data are presented descriptively without inferential statistical testing.measurements and sEMG indices for all patients are reported in Table 28.
Individual transverse
Missing cells indicate unavailable or non-recorded data (e.g., unerupted molars or incomplete sEMG documentation).
Secondary outcomes: neuromuscular balance (Teethan® sEMG)
4.4
Pre- and post-treatment surface electromyography (sEMG) analysis demonstrated systematic improvement across all functional indices:
- Barycenter (BAR): normalization toward the desired zone in 11/12 patients; one case showed improvement without full normalization but with better recruitment quality.
- POC TA/MM: transition from below-range to within-range values in most cases, particularly in patients with more pronounced baseline asymmetry; in the remaining cases, values stayed within the physiological range with improved bilateral coordination.
- Torsion (TORS): reduction or normalization of torsion in > 80% of patients.
- Global asymmetry (ASIM): decreased in 10/12 cases, returning to symmetry or physiological limits.
- Impact/Co-contraction (IMP/CL): increased muscular efficiency (higher IMP) in most cases, with CL values remaining within the normal range. Overall, post-treatment traces described neuromuscular rebalancing consistently with the transverse expansion documented on 3D models. post-hoc standardized mean change (SMC) effect sizes were calculated for the primary transverse outcomes using the mean change divided by the standard deviation of change scores. Very large standardized effects were observed for intercanine width (SMC = 2.25) and inter-5 width (SMC = 2.67). Inter-6 width, available in 6 patients, also showed a very large effect size (SMC = 2.98).
Aggregated pre- and post-treatment values for all sEMG functional indices, including variability ranges and normalization rates, are summarized in Table 29.
Radiographic overview and clinical course
4.5
Pre- and post-treatment panoramic radiographs were obtained to document dental eruption status but were not used for transverse measurements. Overall, they showed symmetric eruption patterns and absence of pathological findings. Adverse events were actively monitored throughout the treatment period and at each scheduled follow-up visit (every 4–6 weeks). At every appointment, parents were questioned and children were clinically examined for the occurrence of potential side effects, including soft tissue irritation or ulceration, speech or swallowing discomfort, feeding difficulties, abnormal tooth mobility, dental pain, or appliance intolerance. Panoramic radiographs obtained for routine monitoring were also inspected for signs of pathological root changes. No additional follow-up beyond the active treatment period was available.
Individual case highlights
4.6
The twelve individual cases are detailed in the Case Series section, including pre-/post-palatal 3D scans, digital bite models, and pre-/post-sEMG reports. In summary:
- Intercanine expansion: ↑ in 12/12 cases (+0.5 – + 4.9 mm);
- Inter-5 expansion: ↑ in 12/12 cases (+1.15 – + 6.26 mm);
- Inter-6 expansion (measurable in 6 cases): ↑ in 6/6 cases (+1.83 – + 4.87 mm).
Intra-examiner reliability
4.7
Intra-examiner reliability was assessed on a random 20% subsample of models remeasured after 7 days.
Excellent agreement was observed for all transverse measurements.
The intraclass correlation coefficient (ICC) values were:
- Intercanine width: ICC = 0.94 (95% CI: 0.90–0.98)
- Inter–second deciduous molar width (inter-5): ICC = 0.92 (95% CI: 0.88–0.97)
- Inter–first molar width (inter-6, when available): ICC = 0.98 (95% CI: 0.95–0.99) Dahlberg's method error ranged between 0.18 and 0.32 mm across all measurements.
No discrepancies exceeded the pre-defined tolerance threshold of 0.5 mm.
Accordingly, measurement reliability was considered clinically acceptable for all evaluated levels.
Discussion
5
Given the retrospective case-series design, the findings describe associations rather than causal effects. The observed transverse improvements and neuromuscular changes should therefore be interpreted as exploratory trends within this sample, without assuming treatment efficacy. Future controlled and randomized studies are necessary to confirm causal relationships.
Main findings and clinical interpretation
5.1
Early orthodontic intervention plays a decisive role in the management of malocclusions and associated orofacial dysfunctions. The present case series suggests that AMCOP® elastodontic appliances are associated with physiological transverse development in growing patients, with consistent transverse and neuromuscular improvement documented through digital models and sEMG. The protocol adopted in this study, beginning with the Integral masticatory plane to correct transverse and vertical dimensions, followed by class-specific devices for sagittal refinement—proved clinically successful (117–121). Digital model analysis confirmed significant increases in intercanine, inter-premolar, and intermolar widths, while sEMG traces (Teethan®) documented restoration of muscular symmetry, barycenter normalization, and improved coordination between the temporalis and masseter muscles. The functional design of AMCOP®, characterized by an elastic thermoplastic blend and dedicated occlusal planes, allows the appliance to work simultaneously on the skeletal base, dental elements, and musculature, promoting stable orthopedic and neuromuscular remodeling. The use of different AMCOP® designs (Integral S/OS and TC) reflects individualized treatment needs and introduces some heterogeneity in the intervention, which may partly explain the variability in clinical and sEMG responses. Importantly, the results were obtained without the need for adjunctive myofunctional exercises, since the natural swallowing reflex ensured continuous functional activation during use.
Comparison with existing concepts and clinical approaches
5.2
The present findings align with the established understanding that traditional expansion appliances, such as Hyrax, Haas, or quad-helix, are primarily mechanical devices designed to achieve rapid transverse widening through orthopedic forces. While effective in separating the midpalatal suture, these appliances do not directly address the neuromuscular and postural components that influence long-term stability (122–128).
Functional appliances such as Activator or Twin Block mainly focus on sagittal correction and show limited influence on the transverse plane. In contrast, the AMCOP® system operates through gentle elastic stimulation that integrates skeletal, dental, and muscular adaptation within a single protocol. This approach, as emphasized in previous conceptual frameworks of functional orthopedics, prioritizes tongue posture normalization, balanced muscle recruitment, and physiologic guidance of craniofacial growth.
The transverse increases observed in our cases (average 3–5 mm) are consistent with what can be expected from gradual functional expansion during early mixed dentition (129–135). The concurrent improvement in electromyographic symmetry supports the notion that skeletal correction and muscular rebalancing can occur simultaneously when treatment is started early and conducted under functional control. Overall, these results strengthen the rationale for elastodontic and biofunctional methods as complementary tools in the modern management of transverse maxillary deficiencies (136–144).
Clinical implications
5.3
The presented protocol underlines the importance of addressing transverse deficiency before sagittal correction. Treating the transverse plane first ensures that subsequent class-oriented elastodontic therapy (e.g., Class III or II AMCOP®) acts on a balanced and coordinated craniofacial base. Failure to correct the transverse component beforehand is one of the most frequent causes of suboptimal outcomes in functional orthopedic therapy. AMCOP® therapy was well tolerated, with high compliance thanks to its non-invasive design, passive nocturnal use, and minimal discomfort. The versatility of the system allows adaptation to individual growth stages, providing a flexible, phase-oriented approach suitable for both children and adults (12, 145–154).
Limitations and future perspectives
5.4
This study is limited by its case-series design, small sample size, and absence of a control group, which precludes inferential statistical conclusions. Furthermore, no orthopedic or orthodontic retention appliances were prescribed after the active phase, and no standardized post-treatment follow-up beyond the end-of-treatment evaluation was performed to assess stability or relapse; therefore, the lack of long-term follow-up does not allow assessment of post-treatment stability. Future research should include prospective, controlled trials comparing AMCOP® with conventional expansion protocols using randomized allocation or matched cohort designs and integrating three-dimensional CBCT analysis with sEMG and postural assessments to further characterize the anatomical correlates of the transverse dimensional changes observed. The present findings describe transverse skeletal changes and neuromuscular pattern variations observed following AMCOP® elastodontic therapy in growing patients. The device features, including functional mechanism, comfort, and adaptability, support its consideration as a potential early interceptive option for the management of transverse maxillary deficiencies and related functional disturbances, pending confirmation from controlled clinical studies (155–157). Surface EMG in pediatric patients presents inherent variability due to cooperation, immature neuromotor patterns, difficulty maintaining standardized occlusal posture, and behavioral fluctuations. These factors may influence signal stability and must be considered when interpreting sEMG changes. Another limitation of this study concerns the non-uniform orientation of some digital occlusal images, which were retrieved from archived clinical material and could not be fully standardized due to lack of access to original raw data. In addition, treatment compliance was assessed subjectively through parental reporting rather than by objective wear-time monitoring systems, which may have introduced reporting bias. Since no CBCT or radiographic angular measurements were performed, the present investigation cannot characterize the biological nature of the transverse dimensional changes observed on digital dental models. Furthermore, part of the transverse increases observed may be attributable to physiological craniofacial growth and dental eruption expected in the 4–7 year age range. Longitudinal growth studies report spontaneous transverse maxillary increases in untreated children of approximately 0.5–1.0 mm per year at the intercanine and intermolar levels during early mixed dentition, depending on sex and developmental stage. Therefore, without an untreated control group, it is not possible to quantify precisely the relative contributions of natural growth vs. appliance-induced orthopedic and dentoalveolar effects. Additionally, the absence of examiner blinding may have introduced a potential measurement bias, although high intra-examiner reliability values reduce this concern. From a clinical standpoint, these findings support the early use of elastodontic functional appliances as a conservative interceptive approach for transverse deficiencies in growing patients. Early interception may contribute to restoring both skeletal dimensions and neuromuscular balance during phases of high biological plasticity, potentially reducing the need for more invasive orthopedic or orthodontic procedures in later stages. Moreover, the combined use of digital model analysis and sEMG monitoring may provide clinicians with an objective tool to evaluate functional adaptation throughout treatment.
Conclusions
6
The present study confirms that AMCOP® elastodontic appliances represent a valid and innovative approach for the early correction of transverse maxillary deficiencies in growing patients. Digital model measurements and surface electromyographic analyses showed transverse dimensional changes and neuromuscular pattern variations associated with the use of the bioactivators. The observed improvements in transverse width and in muscle symmetry parameters (barycenter, torsion, and impact indices) highlight the transverse and neuromuscular changes observed in patients treated with AMCOP® devices, which were characterized by more balanced transverse dimensions and improved neuromuscular indices, although causal inferences cannot be drawn. Compared with traditional mechanical expanders, the AMCOP® system provides a more comfortable, compliant, and biologically oriented therapy, particularly suitable for the interceptive phase of craniofacial growth. From a scientific perspective, these findings contribute to the growing evidence supporting elastodontic approaches as a valuable frontier in functional orthodontics. Given the limited sample size and the observational case-series design, the present findings refer exclusively to the investigated cases and cannot be generalized to the broader pediatric population. Further controlled studies with larger samples and long-term follow-up are encouraged to consolidate these preliminary results and to deepen the understanding of the interplay between skeletal, muscular, and postural components during growth.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nanda R Snodell SF Bollu P. Transverse growth of maxilla and mandible. Semin Orthod. (2012) 18:100–17. 10.1053/j.sodo.2011.10.007 · doi ↗
- 2Zheng G Wang L Su Y Liao G Zhang S Lao X. Maxillary reconstruction assisted by preoperative planning and accurate surgical templates. Oral Surg Oral Med Oral Pathol Oral Radiol. (2016) 121:233–8. 10.1016/j.oooo.2015.10.01026768077 · doi ↗ · pubmed ↗
- 3Wong ME Kau CH Melville JC Patel T Spagnoli DB. Bone reconstruction planning using computer technology for surgical management of severe maxillomandibular atrophy. Oral Maxillofac Surg Clin North Am. (2019) 31:457–72. 10.1016/j.coms.2019.03.00831126730 · doi ↗ · pubmed ↗
- 4Wu Y Wang F Huang W Fan S. Real-time navigation in zygomatic implant placement: workflow. Oral Maxillofac Surg Clin North Am. (2019) 31:357–67. 10.1016/j.coms.2019.03.00131113696 · doi ↗ · pubmed ↗
- 5Inchingolo AM Inchingolo AD Carpentiere V Del Vecchio G Ferrante L Di Noia A Predictability of dental distalization with clear aligners: a systematic review. Bioengineering (Basel). (2023) 10:1390. 10.3390/bioengineering 1012139038135981 PMC 10740623 · doi ↗ · pubmed ↗
- 6Rengasamy Venugopalan S Allareddy V. Craniofacial growth and development. In: Miloro M Ghali GE Larsen PE Waite P, editors. Peterson’s Principles of Oral and Maxillofacial Surgery. Cham: Springer International Publishing (2022). p. 1729–65. ISBN 978-3-030-91920-7.
- 7Schaurich CG Saraco AN Oruganti MH Tamber MS Haetinger RG Dixit I Allometry of human calvaria bones during development from birth to 8 years of age shows a nonlinear growth pattern. Sci Rep. (2024) 14:26205. 10.1038/s 41598-024-77315-839482456 PMC 11528049 · doi ↗ · pubmed ↗
- 8Galea GL Zein MR Allen S Francis-West P. Making and shaping endochondral and intramembranous bones. Dev Dyn. (2021) 250:414–49. 10.1002/dvdy.27833314394 PMC 7986209 · doi ↗ · pubmed ↗