Digital technology-based dyadic interventions in patients with mild cognitive impairment or dementia and their caregivers: a scoping review
Mengyao Wang, Yue He, Jinling Song, Hang Li, Nannan Geng, Changying Li, Zhenzhu Jiao, Yu Gao, Yang Wang

TL;DR
This paper reviews digital interventions for dementia patients and caregivers, highlighting benefits and barriers to adoption.
Contribution
A scoping review of digital dyadic interventions for cognitive impairment, summarizing implementation features and barriers.
Findings
Digital dyadic interventions improved patient cognition and emotional well-being.
Caregiver burden was reduced with these interventions.
Barriers included limited technology access and privacy concerns.
Abstract
Cognitive impairment, particularly when progressing to dementia, exerts considerable psychological distress on both patients and their caregivers. Dyadic interventions regard patients and caregivers as a single unit, emphasizing their interdependence in disease management and highlighting its critical relevance to health outcomes. In recent years, digital technology has been increasingly incorporated into dyadic interventions to support individuals with cognitive impairment and their caregivers. While relevant scoping reviews have been conducted in the cancer field, systematic syntheses of digital dyadic interventions for geriatric cognitive impairment remain limited. This study conducts a scoping review to evaluate the use of digital dyadic interventions for individuals with mild cognitive impairment or dementia and their caregivers. It summarizes key implementation features across…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
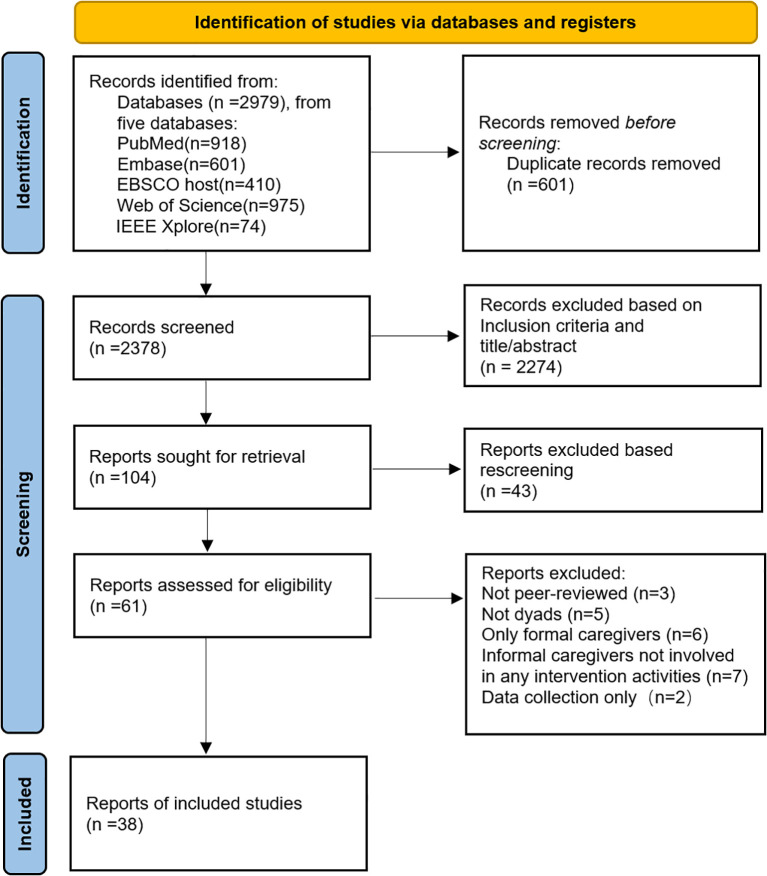 Figure 1
Figure 1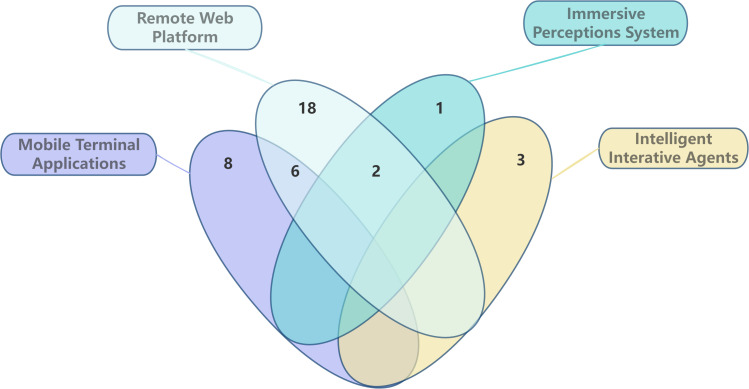 Figure 2
Figure 2| Studies (Lead author, year) | Country | Study design/type | Participants/population of interest | Technology | Synergistic participation (Yes or no) | Type of caregiver | Duration (months/weeks) | Outcomemeasures for patients | Outcome measures for carers |
|---|---|---|---|---|---|---|---|---|---|
| Afifi et al. | USA | Non-randomized study | 21 dyads; MCI/mild-moderate dementia | Rendever VR platform | Yes | Informal caregivers (family members, primarily adult children) | 3 weeks | • QOL-AD: | • Caregiver Burden Index |
| Rochon et al. (2025) ( | USA | Mixed study | 9 dyads; Dementia | Immersive Virtual Environment Technology | Yes | Informal caregivers (spouse, adult child) | N/A | • Feasibility questions | • SUS |
| Hastings et al. (2021) ( | USA | RCT | 40 dyads; MCI | Video Connect on iPad | Yes | Informal caregivers | 12 weeks | •PASE | •SUS |
| Kuzmik, | USA | Qualitative study | 14 dyads; mild-moderate dementia | Mobile application | Yes | Informal caregivers (spouses) | N/A | Thematic Analysis | Thematic Analysis |
| Zubatiy et al. (2021) ( | USA | Mixed study | 10 dyads; MCI | Smart speaker device | Yes | Informal caregivers (spouses, one adult daughter) | 10 weeks | •Logged Interactions independence | •Logged Interactions Independence |
| Rhodus et al. (2023) ( | USA | RCT | 28 dyads; Alzheimer’s disease | Video conferencing technology | Yes | Informal caregivers (family members/primary caregivers) | 6 weeks | •Feasibility | •Feasibility |
| Song, | USA | RCT | 30 dyads; dementia | Video telehealth platform | Yes | Informal caregivers (spouses, daughters, sons, granddaughters) | 5 weeks | •Sleep efficiency | •Sleep efficiency |
| Peterson et al. (2020) ( | USA | Mixed study | 34 dyads; Alzheimer’s Disease and Related Dementias | Web-based Personal Health Record System | Yes | Informal caregivers (spouses, other family members) | 12 months | •PHR-ADRD Feasibility and Utility Checklist | •PHR-ADRD Feasibility and Utility Checklist |
| Peterson, | USA | Mixed study | 16 care partners + 11 drivers with memory loss | video conferencing technology | Yes | Informal caregivers (spouses) | 3 months | •CarFreeMe™-Dementia Intervention Review Checklists | •CarFreeMe™-Dementia Intervention Review Checklists |
| Bannon, | USA | Qualitative study | 16 dyads; dementia | Video conferencing platform, | Yes | Informal caregivers (partners/spouses) | N/A | •Thematic Analysis | •Thematic Analysis |
| Rodriguez, | USA | RCT | 53 dyads; with Alzheimer’s Disease and Related Dementias | mobile telehealth application | Yes | Informal caregivers (family/friends) | 6 months | •NPI | •SUS |
| Bannon et al. | USA | Mixed study Protocol | 20 dyads; Alzheimer’s Disease | Live Video Telehealth + Zoom | Yes (collaborative management of progressive symptoms) | Informal caregivers (spousal care-partners) | N/A | •HADS | •HADS |
| Rochon et al. | USA | Mixed study Protocol | 11 dyads; dementia | Web-based platform | Yes (participates together) | Informal caregivers | N/A | •VC-IOE | •Adapted Feasibility Scale |
| Appel et al. (2023) ( | Canada | Mixed study | 7 dyads; mild-severe dementia | VR headset + tablet | Yes | Informal caregivers (spouse and child-parent pairs) | 4 weeks | • QoL-AD | • QoL-AD |
| Valdivia & Li (2025) ( | Canada | Qualitative study | 17 elders + 16 family caregivers | Voice-reminders app | Not | Informal caregivers (Family caregivers)+Medical Care Providers | N/A | Qualitative Content Analysis | Qualitative Content Analysis |
| Beentjes, | Netherlands | RCT | 59 dyads; mild dementia/MCI | web-based selection tool and errorless learning training program | Yes | Informal caregivers (partners, children) and professional caregivers | 3 months | •SMAS-S | •PES |
| Dröes et al. | Netherlands | RCT | 189 dyads; mild-to-moderate dementia | telephone, web-based learning | Yes | Formal caregivers (professional caregivers) and informal caregivers (family members, relatives) | 6 months | •NPI symptom severity: | •SSCQ |
| Elfrink, | Netherlands | RCT | 42 dyads; mild dementia | Multimedia timeline technology, Online reminiscence tools | Yes | Informal caregivers (spouses, family members) | 6 months | •NPI | •EDIZ |
| Tyack et al., | UK | Mixed study | 12 dyads; dementia | tablet with custom art-viewing app | Yes | Informal caregivers (family/friends) | 2 weeks | • VAS composite well-being Score | •QoL-AD |
| Cooper et al. (2024) ( | UK | RCT | 302 dyads; dementia | Video-call/Telephone | Yes | Informal caregivers (Spouse/partner, Child, Friend, Other) | 12 months | • GAS | • GAS |
| Gonzalez, | UK | RCT | 377 dyads; dementia and sleep disturbance | Actigraphy watches | Yes | Informal caregivers (spouses/partners, children) | 8 months | •EQ-5D-5L proxy | • SDI |
| Fowler-Davis (2020) ( | UK | Mixed study | 30 dyads; mild dementia | Internet of Things monitoring device, | Yes | Informal caregivers (spouses/partners, children) | 4 months | •EFS | •ZBI |
| Howe et al., | UK | Quantitative descriptive study | 37 dyads; mild to moderate dementia/cognitive impairment | A socially-enabled digital content distribution platform | Yes | Informal caregivers (spouses, children, friends) | 6 months | •Logging Data (Platform engagement, informational, etc.) | •Logging Data (Platform engagement, informational, etc.) |
| Killin, | UK | Qualitative study | 10 dyads; Alzheimer’s, vascular, or mixed dementia | Integrated Multi-Component Support System | Yes | Informal caregivers (primarily spouses) | 2 months | •NPT Constructs | •NPT Constructs |
| Wolverson et al., | UK | Qualitative study | 22 dyads; dementia/MCI | Caregivers pro-MMD website platform via tablets | Yes | Informal caregivers (spouses/partners, adult children, friends) | N/A | •Thematic Analysis | •Thematic Analysis |
| Puaschitz et al. (2023) ( | Norway | Mixed study | 82 dyads; dementia | active sensor | Not | Informal caregivers (children, spouses) | 24 months | •SA access | •SA access |
| Laver, | Australia | RCT | 63 dyads; dementia and their | Multi-device Video Conferencing Platform | Yes | Informal caregivers (spouses, children, others) | 4 months | •CAFU | •CMI |
| Lang et al., | Australia | RCT | 9 dyads; dementia | Tablet-delivered Mindfulness and Video Communication System | Yes | Informal caregivers (spouses/partners) | 3 months | •SPPB | •ZBI |
| Muñoz et al., | Australia | Mixed Study | 21 dyads; moderate to advanced dementia | tablet app with 8 games | Yes | Informal caregivers (partners, children) and care staff | 3 months | • Data Logging (Game preference identification, engagement patterns, social interaction facilitation) | • Logging Data (Game preference identification, engagement patterns, social interaction facilitation) |
| Clark et al., | Australia | Qualitative study | 9 people with dementia | Video conferencing platforms | Yes | Informal caregivers (spouses/family carers) and formal carers | 10 weeks | •Thematic Analysis | •Thematic Analysis |
| Lai, | China | Non-randomized study | 60 dyads; Neurocognitive Disorder | Video apps, telephone calls | Yes | Informal caregivers (Spousal, caregivers) | 1 month | •MoCA, | •SF-36v2 |
| Wan Y, | China | RCT protocol | 358 dyads; dementia | Mobile application | Yes | Informal caregivers (family members living with patients) | 18 months | •QOL-AD | •ZBI Reduction |
| Monnet, | Belgium | Mixed study | 21 individuals with mild-moderate dementia + 31 family caregivers | Web-based Interactive Card Platform | Yes | Informal caregivers (partners, adult children) | 2 months | •Logging Data (User engagement | •Logging Data (User engagement |
| Hoel et al., | Germany | Mixed study | 9 dyads; dementia | I-CARE tablet-based activation | Yes | Informal caregivers (spouses, siblings) | 1 month | •QCPR | •Carer-Qol-7D |
| Stara et al. | Italy | Non-randomized study | mild dementia (n=20) + | Embodied Conversational Agent | Yes | Informal caregivers (spouses and sons) | 4 weeks | •SUS score | • SUS score |
| Amabili, | Italy | Non-randomized study | 9 dyads; dementia | Integrated IoT & Social Robotics Ecosystem | Yes | Informal caregivers (family members) | 6 months | • Goal Attainment Scale | • ZBI |
| Guzman-Parra et al. (2020) ( | Spain & Sweden | Quantitative descriptive study | 1086 dyads; MCI/early-stage dementia | Smartphones, tablets | Not | Informal caregivers (relationship not specified in detail) | N/A | •TechPH | •TechPH |
| Notley, | Australia & USA | Qualitative study | 17 dyads; dementia | Integrated Mobile/IoT & Assistive Devices | Yes | Informal caregivers (co-resident, other) | N/A | •Thematic Analysis/Interpretive Description | •Thematic Analysis/Interpretive Description |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDementia and Cognitive Impairment Research · Digital Mental Health Interventions · Technology Use by Older Adults
Introduction
1
With the accelerating aging of the population, mild cognitive impairment (MCI) and dementia have emerged as major global public health challenges (1, 2). MCI represents a transitional stage between normal cognition and dementia (2, 3). Its prevalence increases non-linearly with age: 8.4% among those aged 65–69, 10.1% aged 70–74, 14.8% aged 75–79, and 25.2% aged 80–84 (4), and is associated with an elevated risk of progression to dementia (5). Dementia is characterized by cognitive impairment that severely compromises social and occupational functioning. The global number of individuals living with dementia is projected to reach 152 million by 2050, with approximately 68% residing in low- and middle-income countries (2, 6, 7).
Individuals with cognitive impairment typically require long-term care provided by family caregivers (8). These caregivers play a critical role in disease management but frequently face substantial economic, physical, and emotional burdens (9). Owing to patients’ cognitive and communication limitations, caregivers often experience physical discomfort in addition to anxiety and depression (10, 11). Dyadic interventions regard patients and caregivers as joint participants within a unified care plan, thereby improving health outcomes for both simultaneously (12–14). Digital health technologies generate and apply health data through electronic platforms, software, and hardware (15, 16), thereby overcoming geographic and economic barriers and enhancing the accessibility and reach of dyadic interventions. Existing research indicates (17, 18) that digital dyadic interventions can help maintain patients’ cognitive and psychological states, enhance family interactions, and strengthen caregivers’ skills and perceived support. Across the continuum from mild cognitive impairment to severe dementia, the format of digital dyadic interventions varies according to disease stage. Beentjes et al. (18) used the tablet-based “FindMyApps” tool to help individuals with MCI or mild dementia and their caregivers identify dementia-friendly applications, thereby improving self-management and social participation. Laver et al. (49) delivered tablet-based videoconferencing interventions in which occupational therapists provided environmental assessment, problem-solving strategies, and skills training for dyads with mild-to-moderate dementia to strengthen caregiver confidence and slow functional decline. Rochon et al. (11) employed a web-based low-immersion virtual environment integrating natural soundscapes and multisensory activities for dyads that included individuals with moderate-to-severe dementia, aiming to reduce caregiver stress and enhance real-time engagement and emotional connectedness. However, existing research predominantly focuses on the effects of dual interventions for cancer patients and caregivers, with limited systematic reviews of digital dual interventions for individuals with MCI or dementia and their caregivers. Particularly, there is a lack of summarization regarding intervention formats, mechanisms of action, and implementation challenges.
Therefore, this study is designed to conduct a scoping review that summarizes digital technology–based dyadic interventions for patients with MCI and dementia, as well as their caregivers. It will organize the main types, technological platforms, mechanisms of action, and the effectiveness and barriers encountered during the implementation of existing digital dyadic interventions. From a dual-interaction perspective, this study describes the characteristics of different intervention formats and analyzes their potential impacts and challenges for patients and caregivers. This approach aims to provide a clearer understanding of various digital dual intervention strategies and their current application status for individuals with cognitive impairment and their caregivers.
Materials and methods
2
Design
2.1
This study employed the five-phase framework for scoping reviews proposed by Arksey and O’Malley (19), sequentially comprising (1): defining research objectives (2); retrieving relevant literature (3); screening studies (4); Data extraction (5); Synthesis, summary, and reporting of findings. The review centers on core issues, including primary types and technological forms of digital dyadic interventions, their mechanisms of action, and outcomes and barriers encountered during implementation. A scoping review systematically maps the breadth and diversity of existing literature, providing a more comprehensive overview of the current state of rehabilitation interventions using digital Dyadic interventions for individuals with mild cognitive impairment or dementia and their caregivers. Accordingly, the core questions addressed in this study are: What specific forms do current digital dual interventions for individuals with cognitive impairment and their caregivers take? How are they implemented? What are the facilitating and impeding factors? What are the primary existing challenges? This review has been registered on the Open Science Framework website: https://osf.io/ftnp2.
Search strategy and eligibility criteria
2.2
A comprehensive literature search was conducted using five major databases: Scopus, PubMed, Web of Science, Embase, EBSCOhost, and IEEE Xplore. Grey literature was identified using the Google Scholar search engine. These databases broadly cover relevant literature in mental health, medicine, and nursing. The search terms used are detailed in Supplementary Table 2. The article selection process was documented using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram (20): (Figure 1).
PRISMA flowchart.
Inclusion and exclusion criteria
2.3
The PCC (Population, Concept, Context) framework guided inclusion criteria (21). Population: Pairs where one member has been diagnosed with dementia of any type or severity or MCI, and the other is their family caregiver. Concept: Interventions delivered in home or community settings using digital technologies—including but not limited to apps, online platforms, remote monitoring, and virtual reality—to both MCI/dementia patients and their caregivers. Context: Interventions must be delivered in home or community settings, either remotely by researchers or self-administered by participants with caregiver assistance. Accordingly, the literature inclusion criteria are (1): Study subjects comprise dyads of MCI/dementia patients and caregivers, with caregivers primarily informal (2); Interventions targeting both patients and caregivers with explicit bidirectional effects or collaborative objectives (3); Interventions delivered via digital technology (4); Reporting at least one health outcome or intervention effect relevant to patients, caregivers, or both.
The following studies will be excluded (1): interventions that target only patients or only caregivers, rather than both (2); interventions or evaluations that are not based on digital technology (3); studies involving exclusively formal caregivers, thereby excluding informal caregivers (4); interventions where informal caregivers did not actively participate in any interactive components (5); secondary literature, including systematic reviews, editorials, commentaries, and narrative reviews, as well as studies without available full texts. This study includes original research providing primary empirical data, as well as research protocols that clearly describe intervention design, participant structure, and implementation processes, thereby ensuring that the results focus on intervention strategies, research methods, and population characteristics, while avoiding redundant summaries of secondary.
Data extraction
2.4
Data extraction was performed in Microsoft Excel 2020. Fields included basic study information (authors, publication year, country), study design, sample characteristics (patients and their caregivers), intervention type, form of digital technology, implementation method, intervention duration, outcome measures, and primary outcomes. A descriptive summary table was constructed based on these data. Data extraction was performed independently by two researchers, W.MY and H.Y. Disagreements were resolved through discussion, with final decisions made by a third researcher, W.Y. The search period was set from January 2000 to July 2025. References from included studies were traced to identify potential additional studies. All records were imported into EndNote X9, deduplicated, and then subjected to the next screening step.
Quality appraisal
2.5
The Mixed-Methods Research Quality Assessment Tool (MMAT, 2018 version) was used to evaluate the quality of included studies (22). The MMAT establishes five methodological criteria for each of five study designs: qualitative research, randomized controlled trials, non-randomized quantitative research, quantitative descriptive research, and mixed-methods research. Response options for each criterion include “Yes,” “No,” and “Can not tell.” Subsequently, the overall quality score was calculated as the percentage of criteria successfully met, assigning studies to one of four quality grades: Grade A (indicating 80–100% compliance), Grade B (60–79% compliance), Grade C (40–59% compliance), and Grade D (below 40% compliance). Quality assessments were conducted independently by W.MY and H.Y. Discrepancies were resolved through discussion; unresolved disagreements were adjudicated by a third researcher, W.Y. To ensure methodological rigor and transparency, the five-step framework proposed by Arksey and O’Malley was strictly followed, and a systematic analysis of the current research status was conducted based on key elements, including intervention formats, participant characteristics, and intervention outcomes.
Analysis
2.6
A descriptive analysis approach was employed to systematically categorize and synthesize the included literature. Two researchers with expertise in the field independently reviewed the full texts and performed open coding to extract quantitative data on intervention duration and key outcomes, as well as qualitative information on intervention experiences, implementation barriers, and facilitating factors. Subsequently, inductive thematic analysis was applied to consolidate similar concepts into overarching themes, which were then organized and interpreted in relation to intervention objectives, content components, collaborative participation methods, technology types, and implementation challenges. Disagreements were resolved through discussion, and adjudication by a third researcher was sought when necessary. Ultimately, the findings were presented in tables, figures, and narrative text to illustrate the typological characteristics, participant demographics, and effectiveness of digital dyadic interventions, thereby providing a reference for the design and optimization of future intervention strategies.
Results
3
Selection and inclusion of studies
3.1
Initial searches across five databases and Google Scholar identified 2,979 records. After deduplication in EndNote X9, 601 duplicate records were removed, leaving 2,378 unique records. Based on the inclusion criteria, a preliminary screening of titles and abstracts retained 104 articles. A total of 2,274 records were excluded: 714 for not involving individuals with dementia or their caregivers; 203 for not being related to digital technology; and 1,357 for not addressing dyadic interventions targeting both patients and caregivers. Subsequent review of titles and abstracts of the 104 articles resulted in the exclusion of 43 articles: 23 because the participants were exclusively formal caregivers, and 20 because the intervention or evaluation was not based on digital technology, yielding 61 articles. After full-text assessment,23 records were excluded: 3 were not published in peer-reviewed journals;5 did not target both patients and caregivers; 6 included only formal caregivers; 7 for interventions where informal caregivers did not engage in interactive components, and 2 for studies collecting data without assessment or intervention Ultimately, 38 studies met the eligibility criteria and were included in the final analysis.
Study characteristics
3.2
Table 1 provides an overview of the included articles. These 38 studies were conducted across 12 countries: 13 from the United States (11, 23–34), 2 from Canada (35, 36), 3 from the Netherlands (17, 18, 37), 7 from the United Kingdom (38–44), 1 from Norway (45), 4 from Australia (46–49), 2 from China (50, 51), 1 from Belgium (52), 1 from Germany (53), 2 from Italy (54, 55), and 2 multinational studies (56, 57). 4 were non-randomized studies (28, 51, 54, 55), 11 were mixed studies (11, 30, 33, 34, 36, 42, 44, 45, 48, 52, 53), 7 were qualitative studies (23, 24, 35, 40, 43, 46, 57), 11 were RCTs (17, 18, 25, 27, 29, 32, 37–39, 47, 49), 2 were quantitative descriptive studies (41, 56), 1 was a randomized controlled trial protocol (50), and 2 were mixed-methods research protocols (26, 31). Further details of the included studies are provided in Supplementary Table 1.
Following full-text assessment, the MMAT tool was used to evaluate the quality of the 35 included studies. Among these, 19 studies were rated as Grade A (11, 23–25, 30, 33–36, 39, 40, 43–46, 51–53, 57), 8 studies were rated as Grade B (27–29, 41, 42, 48, 49, 56), and 8 studies were rated as Grade C (17, 18, 32, 37, 38, 47, 54, 55). Three studies were research protocols (26, 31, 50); as protocols are planning documents rather than outcome reports, they were not subject to quality assessment. Detailed evaluation processes and results are presented in Supplementary Table 3.
Intervention modalities
3.3
Among the included interventions, 35 interventions (11, 17, 18, 23–34, 36–44, 46–55, 57) required joint participation of patients and caregivers, while 3 interventions (35, 45, 56) were patient- or caregiver-led with the other party providing support. In terms of technical implementation, the interventions primarily relied on sensory immersive systems (11), (n=1), mobile applications (18, 24, 27, 30, 35, 44, 48, 53), (n=8), remote web platforms (23, 25, 26, 29, 31, 32, 34, 37–43, 46, 49, 51, 52), (n=18), and intelligent interactive agents (33, 54, 55), (n=3). Two studies combined sensory immersive systems with remote web platforms (28, 36), (n=2), concurrent use of mobile terminal applications and remote network platforms (17, 45, 47, 50, 56, 57), (n=6), as illustrated in Figure 2. Overall, remote interventions utilizing tablet applications alongside video and conferencing platforms are most prevalent, with interaction-based intervention designs demonstrating superior collaborative outcomes. Existing studies predominantly employ remote video communication and reminder functions to deliver psychoeducation and social support.
Type of digital technology. (18 used remote web platforms, 8 used mobile applications, 1 utilized immersive systems, 3 employed intelligent agents, 6 applied both mobile applications and web platforms, and 2 combined immersive systems with web platforms).
Sensory immersive technologies are often realized through virtual environment techniques and are generally classified into three levels of immersion. Low-immersion systems present simulated scenarios on electronic screens, enabling simple joint interactions between patients and caregivers; medium-immersion systems employ multi-screen or surround-projection displays to enhance audiovisual engagement (11); and high-immersion systems, or immersive virtual reality (IVR), utilize head-mounted displays and sensory devices to deliver fully multisensory environments (58). Existing research has explored these three categories of sensory-immersion applications. In Afifi et al.’s study (28), elderly participants used standalone head-mounted devices to engage in immersive scenario exercises, while family caregivers participated remotely. Results indicated that the intervention enhanced patients’ sense of social presence and promoted shared reminiscence among caregivers, although no significant improvement was observed in overall dyadic relationship quality. In Appel et al.’s study (36), individuals with dementia viewed 360-degree videos through VR headsets, while caregivers monitored their responses in real time via tablets to facilitate synchronized experiences. Another study employing low-immersion technology (11) used computer-generated natural soundscapes and virtual travel scenarios to facilitate shared participation, with content tailored to participants’ preferences and cognitive abilities. This approach was shown to alleviate patient loneliness and enhance caregiving experiences.
Compared to VR technology, tablet- or smartphone-based mobile applications have been more frequently used in home settings owing to their lower cost and wider accessibility (24, 56). Current interventions typically include cognitive training, self-management, symptom monitoring, and social interaction. Muñoz et al.’s study (48) reported that tablet-based applications incorporating competitive and cooperative games facilitated shared participation through nonverbal gameplay between patients and caregivers. This format allowed caregivers to more intuitively observe patients’ abilities and engagement levels, thereby improving their understanding of behavioral patterns. Other studies have promoted positive dyadic interactions through shared physical-exercise activities, contributing to improved relationship quality (24, 48). However, several usability limitations have been identified for mobile applications. User-anonymity protections often restrict the collection of usage data, making it difficult to accurately determine participation levels and intervention dosage (35). In terms of interactivity, the absence of real-time dialogue functions requires some older adults to replay prompts multiple times to fully understand the content (35). Application stability also affects the overall intervention process, as unexpected application crashes or forced updates may interrupt sessions or require restarting. Operational issues—such as battery failures, overly sensitive touch screens, or screen glare—are also commonly reported (44). Furthermore, most existing mobile applications are not specifically designed for individuals with cognitive impairments, limiting their ability to sustain engagement or adapt to fluctuating cognitive capacities (56).
Remote web platforms generally comprise video-conferencing systems and online educational portals and are primarily used for remote support and psychosocial interventions. They facilitate triadic interactions among patients, caregivers, and professionals, allowing patients to receive cognitive and emotional support at home while simultaneously providing guidance to caregivers (39, 51). Compared with telephone-based interventions, video-based communication overcomes spatial barriers and has been shown to yield higher adherence, greater engagement, better communication quality, and deeper interaction, while more effectively eliciting synchronous exchanges (29, 32). The flexibility of remote platforms enables intervention content to be tailored to different stages of disease progression. For example, individuals in early stages typically receive enhanced social-activity and resource-related information, whereas those in middle-to-late stages rely on simplified interactions to maintain basic communication (43). Furthermore, online platforms offer informational and social-support resources for community-dwelling individuals with mild-to-moderate dementia or cognitive impairment and their informal caregivers, helping both parties remain connected beyond daily care and expanding the scope of dyadic interactions (34). A range of technical and operational barriers has been reported, including poor audiovisual quality, frequent platform updates that compromise usability (32), caregiver dropout caused by login difficulties (37), and patient challenges arising from technological complexity or the absence of ongoing training (43). Additionally, some intervention protocols lack clearly defined follow-up procedures, leaving users uncertain about subsequent steps (52).
AI-powered interactive agents are primarily used to support daily care through voice-based interaction, reminder functions, and environmental monitoring, with three studies investigating this intervention format (33, 54, 55). Research indicates that these systems can provide cognitive support to patients (55) and identify and signal abnormalities to caregivers (54), thereby enhancing collaborative health management. Stara et al. (55) implemented a 4-week intervention using a tablet-based interactive agent, “Anne,” and results demonstrated significant improvements in patient–caregiver closeness, indicating enhanced relational connectedness. However, the study also reported technical limitations, including inadequate voice-recognition performance, which diminished usability and user trust and increased operational burden for both patients and caregivers. Amabili et al. (54) developed the eWare system, which integrates sensor-based monitoring with social-robot interactions to track and intervene in patients’ lifestyle patterns while delivering personalized reminders. Simultaneously, the system supports caregivers by facilitating burden management and enabling real-time monitoring, thereby establishing a collaborative care mechanism.
Characteristics of participants
3.4
Participants included in this review primarily comprised individuals with mild cognitive impairment or dementia and their informal caregivers. Informal caregivers were predominantly spouses or adult children of patients (11, 17, 18, 23–25, 28, 30–33, 35, 38–43, 45–49, 51–53, 55) (n=27), with a minority are other family members or close friends (26, 34, 36, 44, 57) (n=5). Some studies simply describe them as family members (27, 29, 37, 50, 54, 56) (n=6). In some studies, professional or semi-formal caregivers participated alongside informal caregivers in the intervention (18, 35, 37, 46, 48) (n=5). These formal caregivers included nursing home attendants, caregivers, and healthcare professionals, who primarily assumed guiding and supportive roles (18). Examples included assisting with baseline data collection, providing patient information, and facilitating patient and family caregiver engagement in the intervention (36). Based on the role configuration of the dyad in the intervention, three categories can be identified (1): Informal caregiver-oriented dyads, where the caregiver is the primary user and assumes the intervention execution role (2); Collaborative dyads, where the patient and caregiver jointly access the system and participate synergistically (3); Patient-oriented dyads, where the intervention focuses on the patient themselves, with the caregiver providing auxiliary support.
Outcome measurement
3.5
The primary outcomes for dyadic interventions in the included studies were measured across domains such as quality of life, psychological outcomes, relationship quality, physical functioning, caregiver burden, and technology-related indicators. Quality of life was the most frequently evaluated outcome (n=16) (17, 28, 29, 31, 32, 35–37, 39, 44, 50, 51, 53–56), assessed using instruments including EQ-5D-5L, QoL-AD, SF-36V2, Care QoL, and QUALIDEM. Psychological outcomes were assessed in 19 studies (n=19) (17, 27–29, 31, 32, 34, 36, 37, 39, 44, 45, 47, 49–51, 53, 55, 56) using tools such as SMS, WEMWBS, VAS, NPI-RMBPC, MoCA, CDR, GDS, RMBDC, GAD-7, CES-D, PSS, GDS-SF, MHI-5, and PANAS-SF. Relationship and interaction quality was evaluated in 8 studies (26, 28, 31, 32, 44, 48, 52, 53) using instruments including URCS, RSS, PPS, MPC-D, MSC-D, INTERACT, and CSI. Physical functioning was assessed in 9 studies (17, 39, 42, 45, 49–51, 53, 56) using measures such as SPPB, PSQI, SE, and IADL. Caregiver burden was assessed in 15 studies (17, 27–29, 34, 37, 39, 42, 47, 49–51, 53, 54, 56) commonly using ZBI, RMBPC, NPI Caregiver Distress, EDIZ, CAFU, PSS, MOS-S, and PCS. Technology-related outcomes were prominent, with feasibility evaluated in 22 studies (11, 17, 23, 26, 27, 29, 30, 32, 34–37, 39, 41–46, 52, 54, 55, 57), often assessed based on telemedicine session completion rates, retention rates, SUS scales, usage logs, and study-defined feasibility metrics (41, 48); Technology acceptance was assessed in 17 studies (26–28, 31, 33, 35, 36, 41–46, 48, 52, 56, 57), predominantly through questionnaires such as the Usefulness and Usability Questionnaire and through interviews guided by the Unified Theory of Acceptance and Use of Technology (41, 43, 55), User engagement and experience were documented in 8 studies (35, 41–43, 45, 46, 52, 57), involving interactions with applications, virtual reality systems, or social robots. Overall, the studies encompassed outcomes across both patient and caregiver levels, including quality of life, psychological status, relational dynamics, care experiences, and technology adaptability.
Summary of intervention outcomes
3.6
Digital technology–based dyadic interventions were reported to demonstrate positive outcomes in most studies. Among these, 3 studies reported statistically significant beneficial effects (30, 33, 34), whereas 5 reported no significant outcomes (25, 27, 29, 42, 55). Additionally, 14 studies reported mixed results, demonstrating both beneficial effects and non-significant differences (17, 18, 28, 37–39, 44, 45, 47, 49, 51, 53, 54, 56). These mixed outcomes often arose from comprehensive evaluations of clinical efficacy, including caregiver burden, quality of life, and cognitive function, as well as technology acceptance, trust, and relationship quality. Studies with beneficial outcomes showed effect sizes that were predominantly in the moderate-to-high range (29, 39, 47, 51). 6 studies indicated that patient improvements were primarily observed in cognitive function, emotional regulation, and social interaction (27, 28, 32, 36, 51, 54), whereas 8 studies reported reductions in behavioral and psychological symptoms (17, 29, 37, 39, 42, 47, 49, 55). 6 studies also documented caregiver benefits, including reduced psychological burden, enhanced self-efficacy, and increased caregiving confidence (29, 37, 39, 42, 47, 49). Furthermore, the available evidence predominantly relies on short-term follow-up assessments, capturing only immediate post-intervention improvements; long-term effects remain insufficiently examined and require further verification.
Facilitating and barrier factors
3.7
Among the included studies, facilitating and hindering factors related to the implementation of digital dyadic interventions for patients with mild cognitive impairment or dementia and their caregivers were summarized across three dimensions: user engagement, technology and resource constraints, and regional economic conditions. Regarding user engagement, 14 studies reported that cognitive decline, sensory deficits, and attention impairments in patients were found to affect task comprehension and device operation (17, 23, 28, 30, 32, 33, 35, 44–46, 48, 49, 56, 57), the degree of cognitive decline, sensory deficits, and attention impairments in patients were reported to affect task comprehension and device operation (56, 59).Technical proficiency challenges were reported among spousal caregivers of older adults, and disparities in caregivers’ digital skills were found to influence mutual engagement and the quality of interactions (n=9) (32–36, 40, 43, 52, 53). Economic status was examined in 2 studies (28, 57), while distance from patients and relational closeness were also identified as critical factors affecting caregiver participation (25, 34, 35). The impact of internet connectivity was examined in 5 studies (23, 28, 29, 34, 41). Inadequate connectivity was commonly reported among individuals living alone or in rural households (28), thereby compromising the stability of remote interventions. The high cost of acquiring and maintaining equipment, together with frequent platform updates, was reported to increase resource burden (32, 45). A total of five studies also reported that privacy and data-security concerns adversely affected participant engagement (17, 33, 34, 42, 57). Geographically and economically, existing literature was predominantly derived from high-income regions such as North America, Europe, and Oceania, where healthcare infrastructures and digital-health ecosystems are more mature. As a result, the available evidence is skewed toward developed countries, which may limit its applicability in low- and middle-income regions. Additionally, most studies were still in developmental or pilot phases, thereby contributing to uncertainty about intervention effectiveness and scalability.
Discussion
4
This scoping review evaluated the current application of digital-based dyadic interventions for individuals with MCI or dementia and their caregivers. The findings indicated that these interventions encompassed diverse formats and demonstrated high overall feasibility and acceptability. These interventions were found to improve patients’ cognitive and psychosocial functioning while enhancing caregivers’ disease understanding and coping abilities, thereby strengthening mutual interaction and emotional bonds. Furthermore, studies have revealed (60) that when technology was applied solely to patients, discontinuation or insufficient engagement frequently occurred due to cognitive impairment and operational difficulties. In contrast, the collaborative dual-participation model was shown to more effectively facilitate consensus building, supportive relationship establishment, and improvements in quality of life and relationship satisfaction through interaction (18). Therefore, building upon the above foundations, this study will examine different types of digital intervention technologies while exploring their mechanisms of action, cross-cultural implementation, and practical implications.
Sensory immersive technologies
4.1
Sensory immersive technologies are considered to offer shared immersive experiences in dyadic interventions for individuals with cognitive impairment, although the existing evidence base remains limited and largely exploratory. Current findings indicate that VR was not associated with significant improvements in family relationship quality in the study by Afifi et al. (28). This outcome may be attributable to participants’ strong baseline relationships and higher socioeconomic status, indicating that future samples should include more socioeconomically diverse populations to strengthen external validity. Furthermore, to accommodate users with varying cognitive abilities, system design should integrate multiple interaction modalities, including voice-command functions (11). Currently, the adoption of sensory-immersion systems remains limited by network conditions, equipment costs, and operational complexity. In addition, head-mounted IVR devices may pose safety risks such as motion sickness and falls (36), while the associated sense of isolation may reduce natural caregiver–patient interaction. High-quality VR video has also been shown to affect users’ long-term willingness to engage with dual-device systems (36), yet immersive content specifically tailored to individuals with cognitive impairment remains limited. Therefore, future research should prioritize the optimization of both immersive content and device design, including the development of more personalized, high-quality content and improvements in device portability and safety. These advancements would facilitate the stable implementation and long-term adoption of immersive systems in home and community settings.
Mobile applications
4.2
Mobile applications for caregiving are designed with intuitive interfaces and instructional guidance, enabling caregivers to support patients while acquiring care-related knowledge under professional oversight (18). This approach has been shown to enhance patient independence and strengthen caregivers’ competence and confidence. Existing research indicates that although mobile apps are widely accessible in home environments, their effectiveness is shaped by device stability, functional adaptability, and patients’ motivation to engage. Future research should prioritize improvements in system stability and personalized adaptability by optimizing app design (53), streamlining interaction processes, and ensuring sustained technical support. This approach is better suited to the evolving functional capacities of individuals with cognitive impairment and their caregivers. Additionally, more secure data-collection strategies should be implemented to ensure full protection of privacy, such as capturing only anonymized usage frequency and interaction patterns. Simultaneously, the integration of wearable devices or other biofeedback technologies could facilitate the dynamic assessment of collaborative engagement between patients and caregivers, thereby supporting improvements in intervention effectiveness and scalability (27, 48).
Remote online platforms
4.3
Remote online platforms have been shown to offer advantages in delivering cognitive support, facilitating family communication, and strengthening caregiver capabilities. Their tripartite interaction model is considered to extend professional support into the home environment, helping to maintain cognitive function, enhance intrafamilial communication, and improve caregivers’ comprehension and application of health-related information, thereby facilitating more effective emotional co-regulation. Research has indicated that internet-based co-creation or content-sharing activities may enable caregivers to gain deeper insight into patients’ identities and emotional experiences, thereby enhancing empathic understanding and strengthening relationship quality (17). However, existing research remains predominantly developmental, and practical outcomes are largely contingent on technological infrastructure and platform design. Current platforms do not incorporate operational logic specifically tailored to individuals with cognitive impairment, and both patients and caregivers often lack sustained and accessible technical support. Moreover, individuals with declining cognitive abilities incur greater cognitive and practical demands when attempting to learn new technologies. Without clear, step-by-step guidance, discontinuation of use is more likely to occur. Therefore, future platform designs should prioritize optimizing user experience by minimizing operational steps, incorporating more structured navigation prompts, and ensuring continuous technical assistance. This includes providing clear, manualized intervention procedures (39) to improve procedural coherence and strengthen task-completion feedback mechanisms.
AI interaction agents
4.4
Artificial intelligence (AI) interactive agents constitute a class of digital technologies or physical entities capable of interacting with humans via voice and other linguistic modalities. These agents can provide information, execute tasks, or serve as companions (55). As an emerging form of digital intervention, AI interactive agents are increasingly applied to assist in the daily care of individuals with cognitive impairment and their informal caregivers. Currently, these interventions remain exploratory, as most studies feature small sample sizes and predominantly quasi-experimental or cohort designs, lacking large-scale randomized controlled trials. Their effectiveness requires further validation. Furthermore, the effectiveness of these interventions depends on caregivers’ initial parameter configuration and guidance (33). When caregivers face substantial care burdens, their limited availability may hinder proper system use and undermine the intended effectiveness of the intervention. Patients may also experience reduced engagement as cognitive abilities decline, thereby limiting intervention continuity. Technical performance substantially influences user experience, and existing studies indicate that unstable voice-recognition functions disrupt interaction flow and diminish system usability and perceived trustworthiness (55). Future research should include validation through larger-scale studies and prioritize system enhancements, including greater personalization and simplified operational workflows. Adaptability for users with differing cognitive abilities should be strengthened to reduce operational burden. Concurrently, attention should be directed toward how contextual factors—such as residential distance, family structure, and emotional closeness—shape user experience, in order to identify optimal applications for alleviating caregiver isolation and fostering stronger family connections.
Mechanisms of action and synergistic effects of dyadic interventions
4.5
The mechanism of action of Dyadic interventions can be classified into two primary pathways (1): patient-oriented and (2) caregiver-oriented approaches. Patients are engaged in regular cognitive training through video conferencing, mobile applications, or virtual reality to support cognitive functioning and independence. Caregivers are provided with educational resources and psychological support through remote platforms, which help alleviate burden, improve emotional well-being, and enhance caregiving competence. Second, Dyadic interventions directly affect the dyadic relationship by promoting cooperation and intimacy through emotional co-regulation, shared goal-setting, and synchronous interaction (25), thereby enhancing overall relationship quality Overall, the value of Dyadic interventions is reflected in the transformation of individual improvements into relational synergies through reciprocal interaction. Preserving patients’ cognitive and emotional well-being helps to alleviate caregiver stress, while improvements in caregivers’ competence and psychological health, in turn, foster patient engagement. This ultimately establishes a virtuous cycle that strengthens mutual understanding and support, thereby enhancing the overall effectiveness of the intervention. Future intervention designs should consider incorporating technological support and caregiver assistance to facilitate patient expression and participation, while accounting for individual capacity differences, thereby preserving the bidirectional nature of interaction to the greatest extent possible.
Cross-cultural implementation and technology accessibility
4.6
Existing research indicates that the implementation status of digital dual interventions varies among countries with varying levels of economic development. In high-income countries, including the United States, the United Kingdom, Canada, the Netherlands, Norway, Italy, and Sweden, well-established healthcare systems and widespread adoption of digital devices provide favorable conditions for the implementation of digital dual interventions. However, research data indicate that 68% of dementia cases are reported in low- and middle-income countries (2), highlighting a mismatch between intervention needs and resource availability. Some high-income countries also exhibit the phenomenon of “high installation rates but low actual usage” (45), suggesting that hardware accessibility does not necessarily translate into effective utilization. Cost burdens, privacy and ethical concerns, and the lack of sustained technical support can all undermine the effectiveness of interventions. In contrast, research conducted in developing countries, such as China, tends to favor lower-cost and more widely accessible mobile applications, including collaborative care systems based on WeChat mini-programs (50), to address rapidly increasing care demands and resource constraints in the context of an aging population. Cultural contexts are also known to influence technology acceptance and usage patterns. Cultural contexts are also known to influence technology acceptance and usage patterns. Research conducted by Valdivia et al. (35) indicates that, within South Asian cultures characterized by multigenerational households and strong familial obligations, caregiving is frequently regarded as an extension of emotional duty. Families in these cultures may approach external technological assistance with increased caution, thereby reducing proactive adoption. Conversely, in cultures that emphasize individual autonomy, digital technologies are more readily perceived as tools to enhance personal independence and to alleviate caregiving burdens. Furthermore, cross-national comparisons have highlighted variations in digital literacy across different cultural contexts. For instance, significant differences in technological proficiency have been observed among patients with mild cognitive impairment in Sweden and Spain (56). These disparities suggest that identical interventions may result in distinct usage behaviors, levels of dependency, and technical support requirements across different countries. Consequently, the design and implementation of digital interventions must comprehensively consider local cultural backgrounds, family structures, and healthcare infrastructures to enhance both acceptability and sustained utilization.
Implications for future research
4.7
Future research should prioritize the enhancement of personalization and user experience in digital dual interventions, the improvement of accessibility and sustainability of digital technology utilization, and the further reduction of cognitive load for individuals with cognitive impairment during technology interaction. This necessitates a more in-depth investigation into how technology can be integrated into individuals’ daily lives and experiential practices (57). Building upon this foundation, further research may investigate the role of digital health technologies, including immersive virtual environments and voice reminders, that enhance emotional well-being, communication, and relationship quality among patients and caregivers. The efficacy of combining technological interventions with non-pharmacological measures, such as sleep education, mindfulness training, or home-based exercise, should also be examined. Additionally, communication and emotional management training for patients and caregivers should be strengthened to enhance dyadic resilience in coping with caregiving stress and evolving demands. Enhancement of cybersecurity awareness and privacy protection capabilities among patients and caregivers is equally essential. Future research should investigate combined security mechanisms—such as message verification codes and biometric authentication—to reinforce system security. Concurrently, cybersecurity training should be provided to equip users with the ability to identify fraud risks and appropriately configure privacy settings, thereby minimizing information leakage and fostering trust.
Overall, the enhancement of accessibility and sustainability requires continuous improvements in user training, technology adaptation, network infrastructure, and privacy protection. Simultaneously, incorporating sensory adaptation and contextual customization into design, which provides personalized support based on individuals’ economic status, relationship type, living conditions, cultural background, and levels of technological proficiency as reported in prior studies (57) facilitates more effective interactions between dyads with differing cognitive abilities. This approach ultimately enhances compliance and the effectiveness of interventions. Future efforts should aim to establish more standardized and inclusive implementation approaches that accommodate diverse cultural and economic contexts, as highlighted in previous research.
Limitations
5
This study has certain limitations. First, the included studies varied considerably in technology type, intervention content, implementation frequency, and follow-up duration, with no uniform standards. These variations hindered the integration and comparability of findings and may have affected the overall conclusions drawn from this review. Most studies reported only short-term outcomes, making it difficult to demonstrate the sustained effects of digital dual interventions in long-term care. Intervention effectiveness is influenced by participants’ digital literacy. Elderly patients and caregivers often encounter difficulties operating digital devices, which may lead to accessibility gaps and introduce sampling bias. Furthermore, the majority of included studies originated from high-income regions, including North America, Europe, and Oceania, which limits the applicability of the conclusions to low- and middle-income settings.
Second, methodological limitations are inherent to this review. The included studies may have been affected by publication availability, as some existed only as preprints, dissertations, or institutional reports rather than formally published articles. Future research should enhance the robustness and generalizability of findings by employing standardized study designs, conducting long-term follow-up, providing skill training, and expanding literature sources.
Conclusions
6
The reviewed studies suggest that digital dyadic interventions are effective in enhancing quality of life, cognitive function, and emotional well-being among individuals with MCI or dementia, as well as their caregivers. They also show distinct advantages in reducing caregiver burden and fostering relational interactions. However, limited technological accessibility, disparities in user proficiency, and inconsistent participation in dyadic interaction models remain major challenges influencing their implementation and effectiveness. Overall, digital dyadic interventions represent an innovative and potentially sustainable approach to dementia care, with promising applications in home and community settings that warrant further investigation and rigorous validation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hao M Chen J . Trend analysis and future predictions of global burden of alzheimer’s disease and other dementias: a study based on the global burden of disease database from 1990 to 2021. BMC Med. (2025) 23:378. doi: 10.1186/s 12916-025-04169-w, PMID: 40597083 PMC 12220445 · doi ↗ · pubmed ↗
- 2Jia L Du Y Chu L Zhang Z Li F Lyu D . Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: a cross-sectional study. Lancet Public Health. (2020) 5:e 661–71. doi: 10.1016/S 2468-2667(20)30185-7, PMID: 33271079 · doi ↗ · pubmed ↗
- 3Petersen RC Doody R Kurz A Mohs RC Morris JC Rabins PV . Current concepts in mild cognitive impairment. Arch Neurol. (2001) 58:1985. doi: 10.1001/archneur.58.12.1985, PMID: 11735772 · doi ↗ · pubmed ↗
- 4Petersen RC Lopez O Armstrong MJ Getchius TSD Ganguli M Gloss D . Practice guideline update summary: Mild cognitive impairment [RETIRED]: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology. (2018) 90:126–35. doi: 10.1212/WNL.0000000000004826, PMID: 29282327 PMC 5772157 · doi ↗ · pubmed ↗
- 5Hugo J Ganguli M . Dementia and cognitive impairment: epidemiology, diagnosis, and treatment. Clin Geriatr Med. (2014) 30:421–42. doi: 10.1016/j.cger.2014.04.001, PMID: 25037289 PMC 4104432 · doi ↗ · pubmed ↗
- 62024 Alzheimer’s disease facts and figures. Alzheimers Dement. (2024) 20:3708–821. doi: 10.1002/alz.13809, PMID: 38689398 PMC 11095490 · doi ↗ · pubmed ↗
- 7International AD Patterson C . World Alzheimer Report 2018: The state of the art of dementia research: New frontiers (2018). Available online at: https://www.alzint.org/resource/world-alzheimer-report-2018/ (Accessed July 23, 2025).
- 8Richardson TJ Lee SJ Berg-Weger M Grossberg GT . Caregiver health: health of caregivers of alzheimer’s and other dementia patients. Curr Psychiatry Rep. (2013) 15:367. doi: 10.1007/s 11920-013-0367-2, PMID: 23712718 · doi ↗ · pubmed ↗