Associations of Blood Pressure Parameters with Cognitive Decline and Dementia: A Systematic Review of Reviews
Sultana Shajahan, Megan Heffernan, Katie Harris, Cheryl Carcel, Mark Woodward, Craig S Anderson, Ruth Peters

TL;DR
This review summarizes how different blood pressure factors relate to cognitive decline and dementia, highlighting the need for standardized definitions.
Contribution
The study provides a comprehensive umbrella review of existing systematic reviews on blood pressure and cognitive outcomes.
Findings
Higher mid-life blood pressure is linked to increased dementia risk.
Blood pressure variability and pulse wave velocity are associated with cognitive decline.
Most reviews had low quality and inconsistent definitions of blood pressure parameters.
Abstract
Evidence syntheses on the associations between BP parameters and cognitive decline and/or dementia have taken different methodological approaches and targeted different BP parameters and outcomes. The aim of this umbrella review was to provide a high-level synthesis of published systematic reviews with meta-analyses on these associations. PubMed, Embase, PsycINFO, and Cochrane were searched up to April 2025 for eligible reviews. Risk of bias was assessed using the AMSTAR-2 tool, and overlap of constituent studies between reviews was explored. Among 31 included reviews, 8 reported positive associations between higher BP and greater incidence of cognitive decline or dementia, 5 drew neutral conclusions, and 1 reported an inverse relationship. Greater mid-life BP was associated with greater risk of all-cause dementia, whereas late-life hypertension might have a mixed or overall neutral…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
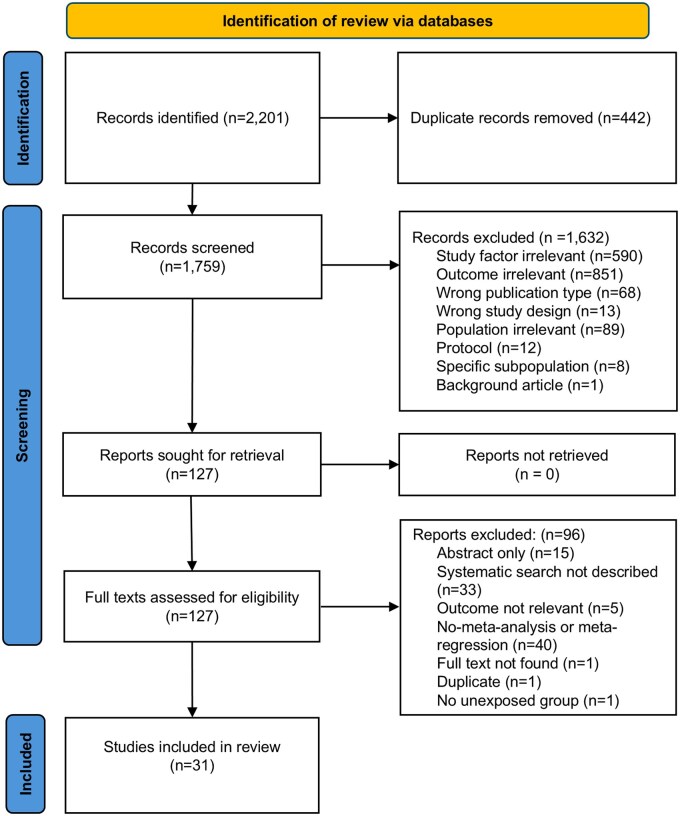 Figure 1
Figure 1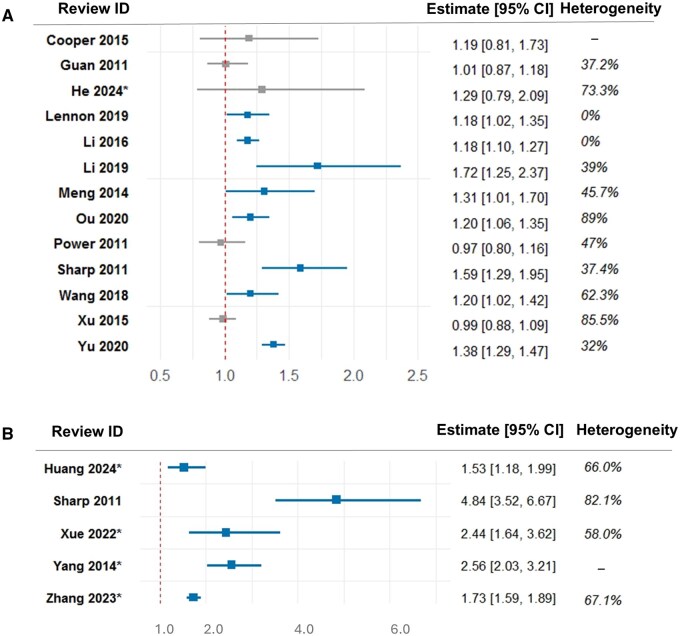 Figure 2
Figure 2| Review ID | Country of study | Population stated as included in the review | Actual mean age range of constituent studies (years) | Source of evidence reported by the reviews | BP parameters identified | Definition of BP parameters | Outcome studied | Criteria for outcome assessment | Follow-up (years) | Number of studies |
|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||
|
| Taiwan | General population without dementia at baseline | 54.3-84.4 | Longitudinal studies | BPV | Ambulatory, home, or visit-to-visit BP monitoring using CV; SD; VIM; average real variability (ARV) | Cognitive decline and dementia |
Cognitive decline: MoCA, CAMCOG Dementia: DSM-IV, DSM-III-R, NINCDS-ADRDA, NINDS-AIREN, or ICD-10 | 1-26 | 8 |
|
| United Kingdom | People with MCI, in the absence of dementia | Not specified | Longitudinal studies | Hypertension | Not specified | Incident dementia | All cause dementia, Alzheimer’s dementia, or other dementias separately | 1.5-9 | 7 |
|
| China | General population | 40- >75 | Longitudinal studies | Hypertension | SBP ≥160 mm Hg or DBP ≥90 mm Hg | Alzheimer’s disease (AD) | Not specified | 1-32 | 9 |
|
| China |
Community-dwelling adults aged 55 years or older with normal cognitive function at baseline | Not specified | Longitudinal studies | Hypertension | Not specified | MCI |
Revised Mayo Clinic Criteria for MCI, Peterson criteria, Winblad criteria, Neuropsychological test battery, Recommendations of the National Institute on Ageing- Alzheimer’s Association | Not specified | 3 |
|
| Hong Kong | Any adults | 50.9-79.9 | Longitudinal studies | BPV | BPV using: SD, CV, VIM, and ARV | Dementia or cognitive decline | DSM III or IV, NINCDS-ADRDA, MMSE, MoCA | 14 | 16 |
|
| Ireland | Adults aged 40-65 years | 48.6-58.6 | Longitudinal studies | Mid-life hypertension |
Hypertension diagnosis by clinician, self-report, and/or by recorded BP metric in line with accepted definitions: the ESC definition ( American Heart Association (AHA) ( | Cognitive decline in memory, attention, executive function, and global cognition | Tests for each domain | Not specified | 15 |
|
| United Kingdom | Not specified | Not specified | Longitudinal studies | High BP | Not specified | Dementia | Not specified | 12 | |
|
| Australia | Any population | 50.4-63 | Longitudinal studies (prospective cohort or nested case control) | Hypertension |
Systolic hypertension: Stage 1 > 140 mm Hg, Stage 2 > 160 mm Hg, Diastolic hypertension: >90 mm Hg, Increments in BP by 10 mm Hg | AD | DSMIV, ICD-9, NINDS | 13-22 | 3 |
|
| United States | With MCI at baseline | 70-80.7 | Longitudinal studies | Hypertension | Not specified | Both AD and dementia | Not specified | Not specified | 60 |
|
| China | Adults aged 35-65 years | 49.2-57 | Longitudinal studies | SBP |
High SBP ≥ 160 mm Hg, Borderline 140 ≤ SBP-160 mm Hg | Dementia | Not specified | 12.8-40 | 7 |
|
| China | Aged >50 years with no dementia at baseline | 73.7-76.4 | Longitudinal population-based studies (prospective/retrospective) | Hypertension | Not specified | Incident dementia | Not specified | 9 | |
|
| China | Aged 40-65 years | 43-60 | Longitudinal studies | Hypertension | SBP/DBP ≥160/95 mm | AD | NINCDS-ADRDA criteria | 13.6-37 | 5 |
|
| China | Adults with no dementia at baseline | 45-83.5 | Prospective longitudinal studies | OH | 1996 consensus statement of OH | Dementia, cognitive impairment (CI), cognitive decline (CD) |
Dementia: ICD-9, DSM-III-R, DSM-IV CI: defined as MMSE <23 in 1 study, as a score of 0 or 1 on the 3 words delayed recall task of the MMSE in another, and as MMSE ≤24 CD: defined as a drop in MMSE score of ≥1 point in 1 study, as a MMSE score drop of ≥3 points in another study | 2-28 years | Total = 13 for worse cognition: - 6 for dementia, 5 for CI, 2 for CD |
|
| China | Participants with normal cognition or MCI | 35.3-93.2 |
Prospective longitudinal studies (cohort, case-cohort, or nested case-control) | Hypertension, SBP, DBP, prehypertension, BPV, BP change, OH, and PP |
Hypertension: SBP ≥130 mm Hg, DBP ≥80 mm Hg, or use of antihypertensive medications Prehypertension: SBP between 120-139 mm Hg, DBP between 80 and 89 mm Hg | Dementia, cognitive impairment | Not specified | 1.5-43 | 136 |
|
| Australia | Any population | 54-87 | Longitudinal studies | Arterial Stiffness | Validated measure of large artery stiffness, central pressure, wave reflections or large artery compliance | Cognitive decline | Valid assessment of cognitive decline or dementia | 5 | 4 |
|
| Australia | Any population | 45-73.4 | Prospective longitudinal studies | OH | Multiple definitions, most common definition was a fall of ≥20 mm Hg SBP and/or a fall of ≥10 mm Hg DBP after supine rest for 10 minutes and standing for 1 minute | Dementia (used standard diagnostic criteria) | MMSE, neuropsychological battery tests, DSM-IV, DSM-III-R | 1-28 | 5 |
|
| United States | Any population | 50-82 | Prospective longitudinal studies (cohort studies or nested case-control studies) | SBP, DBP | SBP >130 mm Hg DBP >85 mm Hg or self-reported antihypertensive medication use | AD | Not specified | 2-27 | |
|
| China | Any population | 49-94 | Prospective longitudinal studies (nested case-control or prospective cohort studies) | SBP, DBP, hypertension, PP | Not specified | Dementia | No diagnostic criteria provided | 2.1-32 | 21 |
|
| China | General population | 49.6-79.8 | Longitudinal cohort or retrospective case-control studies | High SBP, Low DBP | SBP ≥160 mm Hg, Low DBP (at least <70 mm Hg) | AD | Not specified | Not specified | 323 |
|
| China | No restriction on population except for MCI and special populations (special populations not specified) | Not specified | Prospective longitudinal studies | Mid-life hypertension, OH | Not specified | AD | AD independently diagnosed according to the NINCDS-ADRDA criteria, or an RCT—incidence of AD or AD-related clinical endpoints (dementia or cognitive impairment) | Not specified | Not specified |
|
| ||||||||||
|
| Spain |
Adults aged 46-85 years | 46-85 | Cross-sectional and longitudinal studies | PWV | Measured using carotid-femoral, brachial-ankle or aortic PWV |
Cognitive domains (global cognition, executive function and memory) | Using MMSE and other neuropsychological tests | Not specified | 38 |
|
| The Netherlands | Adults aged ≥ 18 years | 66-80 | Case-control, prospective cohorts, database registries, cross-sectional, and secondary analyses of RCTs | BPV | BPV using repeated measurements of BP at rest | Dementia or cognitive decline | Dementia was criterion-referenced ICD criteria, DSM criteria, an adjudicated expert panel or the prescription of antidementia drugs, and cognitive impairment defined using standardized criterion | 1-13 | 20 |
|
| United States | Participants with hypertension | 43-91 | Observational (cross-sectional or longitudinal prospective study but not RCTs or intervention studies) | SBP, DBP |
Elevated SBP >140 mm Hg and/or DBP >90 mm Hg | Cognitive decline | MMSE and other neuropsychological tests | Not specified | 8 |
|
| China | Adults aged ≥18 years with cognitive impairment after stroke (ischemic or hemorrhagic) | 59.9-75.17 | Longitudinal and cross-sectional combined for hypertension, Only longitudinal for SBP and DBP | Hypertension, SBP | Definition of hypertension not specified. SBP levels <120 mm Hg, 120-139 mm Hg, 140-159 mm Hg, 160-179 mm Hg, ≥180 mm Hg | Cognitive impairment | Clinical Dementia Rating (CDR), Clinical diagnosis at the final follow-up visit, Hodkinson Abbreviated Mental Test (HAMT), MMSE, Clock Drawing Test, MoCA, Vascular Neuropsychological Battery (V-NB) | Discharge-4.4 years |
For hypertension = 6 studies For SBP = 12 studies |
|
| Australia | Adults aged ≥ 65 years | 60.9-88.3 | Cross-sectional and longitudinal studies | OH | Decrease of at least 20 mm Hg SBP and/or 10 mm Hg DBP within the first 3 minutes of standing | Cognition | MMSE and other neuropsychological tests | Not specified | 16 |
|
| China | Adults aged >18 years | 46-80 | Cross-sectional or longitudinal studies | Aortic PWV | Validated PWV measurement along aorta | Cognitive decline and dementia | Validated scales and clinic diagnostic standards or guidelines | 1-15 | 29 |
|
| Mexico | Elderly aged 50-80 years | 34.9-79 | Cross-sectional and longitudinal studies (cohort or case-control) | Arterial hypertension | Medical diagnosis or by antihypertensive medication use | Cognitive decline | At least 2 valid neuropsychological instruments to measure cognitive functions. Cognitive domains were assessed using different tests across studies | Not reported | 8 |
|
| United Kingdom | Total dementia population | 57.8-80.4 | Cross-sectional and longitudinal studies | Arterial hypertension | Hypertension based on either a prior diagnosis or a cross-sectional BP measurement | Vascular dementia |
DSM III or IV, ICD-10, Information-memory-concentration, NINDS-AIREN, Hachinski Ischemia score, Rosen Ischemia score | 3.2-10 | 6 |
|
| China | Patients with type 2 diabetes | Not specified | Cross-sectional and longitudinal studies | Hypertension | Not specified | MCI | MoCA, MMSE, European Alzheimer’s Disease Consortium 2006 MCI criteria, Petersen’s criteria, Chinese expert consensus on cognitive disorder diagnosis and treatment | Not specified | 7 |
|
| China | Chinese population with vascular cognitive impairment (VCI) | Not specified | Cross-sectional and longitudinal studies | Hypertension | Not specified | VCI | Not specified | Not specified | 42 |
|
| China | Chinese elderly aged ≥60 years | Not specified | Case-control or cohort studies | Hypertension | Not specified | MCI | MoCA, MMSE, Petersen’s criteria, Chinese expert consensus, 2006 European Alzheimer’s Disease Consortium MCI criteria | Not specified | Not specified |
| Review ID | Type of meta-analysis | BP parameters identified | Dementia type | Univariate | Multivariate (if applicable) | Adjustments (if applicable) | Overall result |
|---|---|---|---|---|---|---|---|
|
| |||||||
|
| Published data | BPV, office or home BP |
All-cause dementia, AD and vascular dementia |
CV = hazard ratio (HR) 1.45 (95% CI, 1.11-1.90), SD = 1.31 (95% CI, 1.03-1.67), VIM = 1.44 (95% CI, 0.87-2.40),
CV = 1.64 (95% CI, 0.96-2.81),
CV = 1.51 (95% CI, 0.80-2.86), SD = 1.47 (95% CI, 0.81-2.68), VIM = 1.46 (95% CI, 0.82-2.57),
CV = 1.71 (95% CI, 0.68-4.28)
CV = 1.57 (95% CI, 0.71-3.46), SD = 1.83 (95% CI, 0.59-5.63), VIM = 1.24 (95% CI, 0.96-1.60),
CV = 1.78 (95% CI, 0.62-5.11), | Differed by study, including sex, study center, education, diabetes, history of vascular diseases, antihypertensive drug at baseline, and mean BP |
| |
|
| Published data | Hypertension | Only all-cause was pooled | OR 1.19 (95% CI, 0.81-1.73) | No relationship between hypertension and all-cause dementia | ||
|
| Published data | Hypertension, SBP ≥160 mm Hg or DBP ≥ 90 mm Hg | AD | RR 1.01 (95% CI, 0.87-1.18), | No relationship between hypertension and AD | ||
|
| Published data | BPV | All-cause dementia |
1.11 (95% CI, 1.05-1.17),
1.38 (95% CI, 1.23-1.55)
1.14 (95% CI, 1.04-1.25)
1.38 (95% CI, 1.23-1.55) |
| ||
|
| Published data | SBP | Both all-cause dementia and late-onset AD pooled | SBP: OR 0.91 (95% CI, 0.64-0.99), |
| ||
|
| Published data | Hypertension | AD |
Systolic hypertension >160 mm Hg: HR 1.25 (95% CI, 1.06-1.47), Systolic hypertension > 140 mm Hg: 1.18 (95% CI, 1.02-1.35), | Differed between studies, including age, sex, education, cholesterol, non-fasting blood glucose, glomerular filtration rate, body mass index (BMI), waist-to-hip ratio, pulse |
| |
|
| Published data | Hypertension | AD | RR 1.18, (95% CI, 1.1-1.27), |
| ||
|
| Published data | High SBP | All-cause dementia |
High SBP: RR 1.72 (95% CI, 1.25-2.37), Borderline BP: 1.41; (95% CI, 1.23-1.62); |
| ||
|
| Published data | Hypertension | All-cause dementia | OR 0.80 (95% CI, 0.65-0.96) |
| ||
|
| Published data | Hypertension, mid-life SBP or DBP | AD |
|
No relationship between high SBP or hypertension and Alzheimer’s dementia
| ||
|
| Published data | OH | All-cause dementia | 1.30 (95% CI, 1.143-1.48), | Not specified |
| |
|
| Published data | Hypertension, SBP, DBP, BPV, BP change, OH | All-cause dementia |
|
| ||
|
| Individual patient data | OH | All-cause dementia | RR 1.21 (95% CI, 1.09-1.35), | Differed between studies, various covariates including but not limited to age, race/center, gender, education, SBP, DBP, antihypertensive medication, diabetes, ratio of total cholesterol to high density lipoprotein (HDL) cholesterol, lipid lowering medication, smoking status, alcohol intake, anticholinergic medication, BMI, and APOE genotype. |
| |
|
| Published data | SBP, DBP | AD |
History of hypertension: RR 0.98 (95% CI, 0.80-1.19), Combined history of hypertension and hypertension at enrolment: 0.97 (95% CI, 0.80-1.16), A 10 mm Hg-increase in SBP: 0.95 (0.91-1.00), A 10 mm Hg-increase in DBP 0.94 (0.85-1.04), | No relationship between a history of hypertension, current hypertension, higher SBP or DBP and AD | ||
|
| Published data | Hypertension, SBP, DBP |
All-cause AD Vascular dementia |
All-cause pooled results RR: 1.20 (95% CI, 1.02-1.42), Mid-life <65 years: Hypertension and AD: 1.18 (0.75-1.85), Hypertension and vascular dementia: 7.68 (3.50-16.84), Late life ≥65 years: No significant association with AD, only VD: 3.69 (1.57-8.72), Late life 75-85 years: High DBP and AD: 0.52 (0.32-0.85), Very late life >85 years: Hypertension and all-cause dementia: 0.67 (0.48-0.94), | Differed between studies, including age, gender, antihypertensive treatment, smoking, diabetes, prevalent cardiovascular disease, and plasma cholesterol |
| |
|
| Published data | SBP ≥160 mm Hg, Low DBP (at least <70 mm Hg) | AD |
Combined OR and RR: SBP ≥160 mm Hg: 0.99 (0.88-1.09), Low DBP 1.18 (0.97-1.39), |
| ||
|
| Published data | Hypertension in mid-life, OH | AD |
Hypertension in mid-life: RR 1.38 (95% CI, 1.29-1.47) OH: 1.18 (1.02-1.35), | Not specified |
| |
|
| |||||||
|
| PWV | All-cause dementia | Highest category of aortic PWV: 2.10 (95% CI, 1.16-3.80), |
| |||
|
| Published data | Arterial hypertension | Incidence of vascular dementia | OR 1.59 (95% CI, 1.29-1.95), |
| ||
| Prevalence of vascular dementia | OR: 4.84 (95% CI, 3.52-6.67), |
| |||||
| Review ID | Type of meta-analysis | BP parameters identified | Unit of cognition | Univariate | Multivariate (if applicable) | Adjustments (if applicable) | Overall result |
|---|---|---|---|---|---|---|---|
|
| Published longitudinal cohort studies | BPV, office or home BP | Incidence of all common types of dementia or incidence of cognitive decline |
| Differed by study, including sex, study center, education, DM, history of vascular diseases, antihypertensive drug at baseline, and mean BP |
| |
|
| Published longitudinal data | Hypertension | Incidence of MCI | HR 1.29 (95 % CI, 0.79-2.09), | Adjusted for age, sex, education, APOE ε4 genotype, smoking, level of physical, social, or productive activities, race; alcohol use status; BMI; total cholesterol and high-density lipoprotein cholesterol; history of coronary heart disease, heart failure, and stroke | Hypertension not associated with incidence of MCI | |
|
| Published longitudinal data | OH | For the dichotomous outcome of incidence of cognitive impairment or no | OR 1.19 (95% CI, 1.00-1.42), |
| ||
|
| Published longitudinal data | BPV | Incidence of dementia or cognitive impairment as dichotomous outcome. cognitive decline by change in cognitive test scores per SD increase in BPV |
pooled HR 1.10 (95% CI, 1.06-1.15), Change in cognitive test scores: −0.14 (95% CI, −0.20 to −0.08), Diastolic BPV:
|
| ||
|
| Published longitudinal data | Mid-life hypertension | Cognitive domains (memory, attention, executive function, and global cognition), as a continuous outcome, between those with hypertension compared to normotension |
Memory: MD = −0.06 (95% CI, −0.20 to 0.08), Attention: MD = 0.41 (95% CI, 0.26-0.56), Executive function: MD= −0.02 (95% CI, −0.08 to 0.03), Global cognition: MD= −0.24 (95% CI, −0.28 to −0.21), |
| ||
|
| Published longitudinal data | OH | OH defined as a sustained reduction in SBP of at least 20 mm Hg and/or DBP decreasing by at least 10 mm Hg for the first 3 minutes of standing or head tilting at least 60° | Worse cognition (HR): 1.18 (95% CI, 1.0-1.35), |
| ||
|
| Published longitudinal data | Hypertension (SBP ≥130 mm Hg, DBP ≥80 mm Hg, or use of AH medications). Mid-life vs late life hypertension (>65 years) | Global cognition, episodic memory and executive function (Dichotomous) | N/A |
Global cognition: RR: 1.55 (95% CI, 1.19-2.03), Executive function: 1.22 (95% CI, 1.06-1.41), |
Gender, ethnicity, publication year, educational level, alcohol and tobacco consumption, geographic region, and cerebrovascular or cardiovascular diseases |
|
|
| Individual patient data and published data | PWV | Change in MMSE scores—Extracted regression coefficients and CIs were pooled in a meta-analysis along with the regression coefficients and CIs calculated where individual patient data were available | Change in MMSE = −0.03 (95% CI, −0.06 to 0.01) | Age, sex, education, mean arterial pressure, and MMSE scores at baseline | No relationship between PWV and cognitive decline | |
|
| Published data | PWV |
Change in cognitive test scores as a continuous outcome, cross-sectional association: ESs and 95% CIs were calculated for each observed correlation using Cohen’s |
Global cognition: −0.53 (95% CI, −0.67 to −0.39) Executive function: −0.35 (95% CI, −0.50 to −0.19), Memory: −0.39 (95% CI, −0.70 to −0.09) |
Global cognition: −0.21 (95% CI, −0.30 to −0.11) Executive function: −0.08 (95% CI, −0.14 to −0.03) Memory: −0.13 (95% CI, −0.20 to −0.05) | Not specified |
|
|
| Published data, cross-sectional | Hypertension defined by SBP > 140 mm Hg and/or DBP > 90 mm Hg |
Pearson’s correlation co-efficient ( for each selected study as SBP or DBP) and cognition, weighted by the sample size of each individual study |
Global cognition:
Episodic memory:
Language: Executive functioning: Attention: Information processing speed: Visuo-perceptual abilities: |
Global cognition: Episodic memory:
Language: Executive functioning: Attention: Information processing speed: Visuo-perceptual abilities: | Age, education, sex, and vascular factors |
Mixed result:
No association with language, executive functioning or processing speed |
|
| Published data | SBP, DBP, hypertension. Different levels of SBP and DBP |
For hypertension and DBP, prevalence of cognitive impairment For SBP, incidence of cognitive impairment |
Prevalence: OR= 1.53 (95% CI, 1.18 to 1.99), Incident cognitive impairment = 1.13 (95% CI, 1.05, 1.23), SBP <120 mm Hg: 1.15 (95% CI, 1.07-1.25), 120-139 mm Hg: 1.26 (95% CI, 1.06-1.49), 140-159 mm Hg: 1.15 (95% CI, 1.00-1.32), 160-179 mm Hg: 1.02 (95% CI, 1.01-1.04), SBP ≥ 180 mm Hg: 1.17 (95% CI, 0.63-2.17), DBP and prevalence of cognitive impairment = OR 1.38 (95% CI, 1.11-1.72), DBP <80 mm Hg 1.22 (95% CI, 0.95-1.58), 80-99 mm Hg: 1.18 (95% CI, 0.86-1.61), DBP ≥100 mm Hg: 1.96 (95% CI, 1.51-2.56), |
| ||
|
| Published data | OH | Means and SDs were used for continuous cognitive assessment scale outcomes. |
MD −0.51 (95% CI, −0.85 to −0.17), |
| ||
|
| Published data | Aortic PWV | For cross-sectional studies, Pearson’s |
Attention: Global cognitive function: Memory: Processing speed: MMSE: |
| ||
|
| Published data | Arterial hypertension | All ESs were calculated using standardized MDs, as all studies used a wide variety of scale measures (continuous), group with uncontrolled hypertension compared to the control group |
Processing speed: standardized MDs = –0.40 (95% CI, −0.25 to −0.54), Working memory: −0.28 (95% CI, −0.15 to −0.41), Short-term memory and learning:—0.27 (95% CI, −0.37 to −0.17), Delayed recall: −0.20 (95% CI, −0.35 to −0.05), |
| ||
|
| Published data | Hypertension | Prevalence of MCI | OR 2.44 (95% CI, 1.64-3.62), |
| ||
|
| Published data | Hypertension | Prevalence of vascular cognitive impairment | OR 2.56 (95% CI, 2.03-3.21), |
| ||
|
| Published data | Hypertension | Prevalence of MCI | RR 1.73 (95% CI, 1.59-1.89) |
|
- —University of New South Wales and the George Institute for Global Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDementia and Cognitive Impairment Research · Cardiovascular Health and Disease Prevention · Blood Pressure and Hypertension Studies
Introduction
It is estimated that over 55 million people are living with dementia globally, over two-thirds of whom are living in low-and middle-income countries.1 This figure is expected to nearly double over the next few decades owing to ongoing ageing of populations.2 Dementia is now one of the leading causes of death and disability, affecting approximately 5%-7% of the population, mostly among those aged over 60 years.2 Elevated BP is well recognized as being associated with an increased risk of cognitive decline and/or dementia,3-9 and there is increasing evidence that BP lowering treatment can reduce these risks.3-5^,^7^,^10
Over the 2 decades since Qiu et al11 published their seminal review on the association of BP with cognition/dementia, additional systematic reviews and meta-analysis have sought to draw together epidemiological and/or clinical trial data to refine the precision of effects.3^,^12-14 However, each evidence synthesis approach has had a slightly different focus, and used different methods and criteria for BP parameters, treatments and outcomes. As the definitions of hypertension have changed as the evidence-base has increased, it would appear appropriate that an overview be undertaken to reevaluate the evidence, assess the risk of bias, synthesize the results, and highlight important new findings in this area.
As the literature around BP and dementia is considerable, it can be difficult for health professionals and policy makers to determine which BP parameters are the most important in defining those at highest risk, and which therapeutic targets are appropriate for preventing cognitive decline and/or dementia. Umbrella reviews or “review of reviews” methodology allows a systematic high-level summary of the evidence. The aim of this umbrella review was to summarize the content and quality of the current body of evidence on the relationship between the most commonly used BP metrics in clinical settings and cognitive decline or dementia, and calculate overlap of constituent studies between reviews.
Methods
Registration
A review protocol was developed and registered on the PROSPERO international prospective register of systematic reviews (registration number CRD42023380633), and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guideline.15 The protocol provides full details of the methods used and any changes invoked subsequent to original registration.
Inclusion and exclusion criteria
We included systematic reviews with meta-analyses or meta-regressions which examined associations with prevalent (cross-sectional) or incident (longitudinal) cognitive decline/dementia. Reviews were excluded if they focused on pregnancy-related BP changes (eg, preeclampsia and eclampsia) or distinct subpopulations (eg, those with schizophrenia). The included reviews were restricted to published articles including a systematic search (identified the data source, last date of search, inclusion and exclusion criteria) and analysis plan (how the results were pooled and if any tests for heterogeneity and publication bias were done); gray literature and abstracts from conference presentations were not searched. Analysis plans were scrutinized in the published articles and accompanying supplementary files. Studies using self-reported outcome measures were ineligible, since self-reported dementia-related diagnosis can inaccurately estimate the prevalence of dementia in older adults.16
BP parameters
To capture commonly used and emerging BP parameters that have been reported as having a role in an increased risk of cognitive decline or dementia, the exposures included: hypertension, mean SBP; mean DBP; BP variability; PP; mean arterial pressure (MAP); carotid-femoral pulse wave velocity (PWV); orthostatic hypotension (OH), and cumulative SBP load. Detailed definitions are provided in Appendix S1.
Outcomes
The primary outcomes of interest were cognitive decline, incidence or prevalence of dementia, or a composite of both. Cognitive function may be measured using any clinical cognitive assessment tool(s), including but not limited to the Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), and neuropsychological tests. Dementia may be diagnosed by any widely accepted diagnostic tools, such as the Diagnostic and Statistical Manual of Mental Disorders, Fourth or Fifth Edition, or International Classification of Diseases (ICD) codes.
Databases and selection of studies
PubMed, Embase, PsycINFO, and Cochrane databases were searched on April 15, 2025, using a combination of key words and MeSH terms for BP, hypertension, PWV, variability, MAP, PP, cognitive dysfunction, dementia, and Alzheimer’s disease (AD) (details are provided in Appendix S2). Two reviewers (S.S. and M.H.) independently selected studies against the eligibility criteria and any conflicts between the 2 reviewers were resolved by a senior third reviewer (R.P.).
Data extraction, quality assessment, and synthesis
Data were extracted in duplicate (S.S. and M.H.) and comprised the following items: lead author and publication year, methodology (systematic reviews with meta-analyses and/or meta-regression), number and sample size of constituent studies, range of follow-up lengths and population age and sex breakdown in each review/meta-analysis, dates/databases and search terms used to populate reviews or source of data/key data parameters for meta-analyses, BP measures, measures of diagnosis of cognition and dementia, statistical measures, assessment of bias, pooled relative risk (RR), or similar, for cognitive impairment or dementia (unadjusted and adjusted) with 95% confidence intervals (CIs), and list of covariates if adjusted results were included. Reviews were evaluated in duplicate using the AMSTAR 2 checklist (Appendix S3). Any disagreements were resolved by discussion with a senior author (R.P.). The data extracted and findings were summarized in a narrative synthesis including detailed tables. Overlap of the constituent studies across reviews reporting the same BP parameters was quantified using the Corrected Covered Area Index.17
Results
Search results
In total, 2,201 articles were identified from database searching (Figure 1). After removing 442 duplicates, 1,759 articles remained. After title abstract screening, 127 articles were identified for full text screening. Finally, 31 reviews were eligible for inclusion. A list of excluded studies after full text screening is provided in supplementary Table S1.
Flow chart showing the study selection process.
Characteristics of the included reviews
Table 1 summarizes the characteristics of the included reviews that covered various BP parameters for hypertension,3^,^14^,^18-30 SBP and/or DBP,14^,^22^,^27^,^31-36 BP variability,14^,^37^,^38 PWV,39-41 and OH.42-44 No reviews were found for PP, MAP, or cumulative BP load. Reviews included constituent studies ranging in size from 319 to 323,36 with the total numbers of participants ranging from 1,972 to over 7 million. Two reviews focused on only participants with mild cognitive impairment (MCI),3^,^20 1 included either those with normal cognition or MCI,14 1 included participants with hypertension only,31 and 2 included only older participants, age ≥ 6542 or 50-8023 years. Eighteen of the 31 reviews were published in the last 5 years.14^,^19^,^21^,^23^,^25-30^,^32^,^33^,^37-4443^,^45 Nineteen reviews examined dementia as an outcome,3^,^14^,^18-22^,^24^,^25^,^32-38^,^40^,^43^,^44 while the others examined cognitive ecline overall or decline within specific cognitive domains.14^,^23^,^26-31^,^37-43^,^45 Twenty-two reviews excluded baseline impairment and/or dementia, or explicitly stated that they investigated incident dementia.3^,^14^,^18^,^20-28^,^31^,^33-37^,^41^,^43-45 Only 1 review combined cognitive decline or dementia as an outcome.45 Two reviews included trials combined with observational studies,25^,^45 19 reviews included only cohort studies with longitudinal follow-up and/or nested case-control studies,3^,^14^,^18-22^,^26^,^28^,^32-38^,^41^,^43^,^44 and 10 reviews included both cross-sectional and longitudinal articles.23^,^24^,^27^,^29-31^,^39^,^40^,^42^,^45 No reviews were restricted to a single sex. Most reviews drew constituent studies from North American, European and Chinese populations, but some included Australian, Taiwanese, Japanese and Korean populations;14^,^19^,^22^,^33^,^35^,^36^,^38 2 studies did not specify a particular geographical distribution.23^,^31 Further details are provided in supplementary Table S2.
Associations of BP parameters with cognitive outcomes
Hypertension
Twenty-one systematic reviews reported results for hypertension or raised BP. Fourteen reviews included meta-analyses of only longitudinal data to report on incident dementia (all-cause), AD, or vascular dementia (VD),3^,^14^,^18-22^,^24^,^25^,^32-36 1 reported longitudinal and cross-sectional associations separately for VD,24 3 reported longitudinal associations with cognitive decline,14^,^26^,^28 and 6 combined cross-sectional and longitudinal studies in their meta-analyses and reported on the prevalence of cognitive decline23^,^27^,^29-31^,^46 (Tables 2 and 3).
Definitions of hypertension or raised BP varied from SBP ≥130 mm Hg and DBP ≥80 mm Hg,14^,^34 borderline (140 mm Hg ≤SBP, <160 mm Hg)22^,^33 up to SBP ≥160 mm Hg or DBP ≥ 90 mm Hg,18^,^36 SBP >140 mm Hg and/or elevated DBP >90 mm Hg,31 with some reviews also including treatment with antihypertensive medication or a history of hypertension as indicating presence of hypertension,14^,^23^,^24^,^28^,^34 and 10 systematic reviews reporting hypertension only as a binary exposure3^,^20^,^21^,^25-27^,^29^,^30^,^32^,^35 (Tables 1 and 2). Four reviews included constituent studies that reported on baseline ages in mid-life (<65)19^,^22^,^28^,^33, 7 in mid- and late-life,14^,^18^,^24^,^27^,^34-36 2 in later life only (>65),20^,^21 and 6 did not define an age range of their constituent studies.3^,^26^,^29^,^30^,^32^,^46
Overall, 8 out of 13 systematic reviews using longitudinal data reported associations between higher BP and incident dementia;14^,^19^,^20^,^22^,^24^,^25^,^33^,^35^,^36 3 for all-cause dementia,14^,^33^,^35 4 for AD,19^,^20^,^22^,^25 and 1 for VD24 (Figure 2A). One review reported a lower risk of incident dementia with no history of hypertension.21 Most found that hypertension or higher SBP was associated with poorer cognitive outcomes, but Meng et al found higher DBP (but not SBP) to be associated with AD.22 Reviews that separated mid- and late-life exposures reported greater mid-life SBP to be associated with a greater risk of all-cause dementia.14^,^35 Additionally, Ou et al14 found no association of late-life hypertension and all-cause dementia, while Wang et al35 found late-life hypertension or high DBP to be protective for dementia (Table 2).
Risk estimates with 95% confidence intervals (CI) for hypertension and cognitive decline or dementia in (A) longitudinal studies and (B) combined studies.*
Five reviews drew neutral conclusions, neither negative nor positive associations between BP and cognitive decline or dementia.3^,^18^,^22^,^26^,^34 One review on strictly Mendelian randomization studies reported higher BP to be associated with better cognition.32
Ou et al reported on the longitudinal association of high BP on cognitive domains and found varied results: Hypertension was significantly associated with worse global cognition (RR 1.55, 95% CI, 1.19-2.03; I^2^ = 18%) and executive function (RR 1.22, 95% CI, 1.06-1.41; I^2^ = 0%), but not episodic memory (1.13, 95% CI, 0.98-1.30; I^2^ = 0%) (Table 3). Joyce et al28 reported that hypertension was negatively associated with global cognition but positively with attention.
Systematic reviews which combined longitudinal and cross-sectional data all reported associations between higher BP and higher prevalence of dementia or cognitive decline; 1 for VD24 and 4 for cognitive imapairment27^,^29^,^30^,^46 (Figure 2B). However, mixed results were found for different domains of cognition: hypertension being associated with poorer global cognition and episodic memory but with enhanced attention performance; and no association with language, executive functioning or processing speed in 1 review.31 Poorly controlled hypertension was associated with poorer cognition: working and short-term memory, delayed recall, and processing speed.23 Hypertension was also associated with the prevalence of vascular cognitive impairment.46 Appendix S4 provides a detailed description of the systematic reviews that reported on hypertension.
BP variability
Four systematic reviews reported results for the association between BPV, and dementia or cognitive decline.14^,^37^,^38^,^45 Three reviews included meta-analyses of only longitudinal data on incident dementia or cognitive decline separately14^,^37^,^38 (all-cause,14^,^37^,^38 AD,37 or VD37), while 1 reported longitudinal and cross-sectional associations for combined dementia or cognitive decline45 (Tables 2 and 3). Of the various BPV indices, only Chiu et al37 specified the inclusion of constituent studies adopting a mixture of office BP, home BP, and ABP measures. In regard to BPV timeframes, reviews included constituent studies with different timeframes, such as short-term/day-to-day to long-term/visit-to-visit BPV.37^,^38 For BPV indices, coefficient of variation (CV) or standard deviation (SD) were the most frequently used ones for SBP and DBP variability.37^,^38
All 3 systematic reviews with longitudinal data reported associations between higher BPV and all-cause dementia, and 2 reported similarly for cognitive decline.37^,^38 All 3 reviews found higher SBP variability to be associated with poorer cognitive outcomes, but Ou et al and Jia et al also found DBP variability to be associated with all-cause dementia or cognitive decline (Tables 2 and 3). Jia et al38 also found that both SBP and DBP visit-to-visit and day-to-day variability were associated with dementia and cognitive decline. Chiu et al37 demonstrated that BPV measured through either CV or SD was associated with poorer cognitive outcomes. Further details on BPV are provided in Appendix S4.
Pulse wave velocity
Pulse wave velocity was used to look at the association of arterial stiffness with dementia or cognitive decline in 3 systematic reviews and meta-analyses.39-41 All 3 reviews included meta-analyses of longitudinal data to report on incident dementia or cognitive decline separately,39-41 while 2 reported separate cross-sectional associations for dementia or cognitive decline combined39^,^40 (Tables 2 and 3). Arterial stiffness was measured in the constituent studies of these reviews using carotid-femoral PWV,39-41 brachial-ankle PWV,39 or aortic PWV.39^,^40
Two systematic reviews used longitudinal data to report associations of higher PWV and all-cause dementia40 or for cognitive decline.37^,^38 Greater PWV was associated with poorer global cognition,39^,^40 memory,39^,^40 executive function,39 and processing speed.40 One review found no relationship between PWV and cognitive decline.41
Two systematic reviews reporting on cross-sectional studies also reported that higher PWV was associated with all-cause dementia,40 poorer global cognition,39^,^40 memory,39^,^40 executive function,39 and processing speed.40 Further details are provided in Appendix S4.
Orthostatic hypotension
Five systematic reviews reported results for OH related to dementia or cognitive decline.14^,^25^,^42-44 All reviews included meta-analyses of longitudinal data to report on incident dementia14^,^25^,^43^,^44 or cognitive decline separately,14^,^42-44 while 1 also reported the cross-sectional association of OH with cognitive decline42 (Tables 2 and 3, Appendix S4). The most widely accepted definition of OH, across the constituent studies of the reviews, was falls of >20 mm Hg SBP and/or >10 mm Hg DBP within the first 3 minutes of standing from a supine position.14^,^25^,^42^,^44
All 5 systematic reviews reported associations between higher OH and a greater incidence of all-cause dementia,14^,^43^,^44 AD,25 cognitive impairment (dichotomous outcome),42 and poorer cognition.43 Meta-analysis of cross-sectional data showed that OH was significantly associated with a lower mean MMSE score.42
Risk of bias and overlap
According to the AMSTAR-2 criteria, 23/31 (74%) reviews were of critically low quality: The remainder were split between high 5/31 (16%), and low 3/31 (10%) quality (supplementary Table S3). All the included reviews provided an appropriate PICO description (population, intervention, control group, and outcome) for organizing the framework of their study question and the eligibility criteria for their selection of studies. Only 10/31 (32%) reviews contained an explicit statement that the methods were established prior to the conduct of the review.
Most of the studies failed to obtain a positive quality assessment because they lacked an established protocol prior to conduct of the review, gave insufficient detail explaining their selection of the study designs for inclusion in the review, did not provide a list of excluded studies with justification, or did not use satisfactory techniques for assessing the risk of bias or publication bias. Moreover, there was considerable heterogeneity in the study characteristics which were not adjusted for, and/or considerable heterogeneity in the study-specific results contributing to meta-analysis. Some reviews did not specify whether cognitive decline was defined using any internationally accepted criteria. The percentage of overlap of constituent studies across the reviews for each BP parameter was for hypertension/SBP/DBP with dementia due to any cause: 6.6%; specific domain of cognition: 2.7%; and cognitive decline or impairment: 0% (supplementary Table S4). The eligibility criteria for reviews focusing on cognitive impairment as the outcome varied widely: Huang et al27 included exclusively post-stroke patients, Xue et al29 restricted to those with MCI and type 2 diabetes, Yang et al46 included only vascular cognitive impairment among Chinese populations, and Zhang et al30 restricted to Chinese elderly patients. Overlap of constituent studies among the other parameters was higher: BPV 33.3%, PWV 24.5%, and OH 10.1%.
Discussion
This umbrella review was designed to facilitate informed understanding and decision-making through the provision of a rigorous summary of the content and quality of the current evidence from systematic reviews and meta-analyses of the relationship between different BP parameters and cognitive decline and/or dementia. Despite some heterogeneity in the evidence base, the weight of the evidence supports an association of higher SBP, DBP, BPV, PWV, and OH on incidence of dementia and cognitive decline, especially for the domains of global cognitive function, executive function, and working memory.
The included reviews support there being a strong association between hypertension, and high SBP or high DBP, with both the incidence and prevalence of cognitive decline or dementia,14^,^19^,^20^,^22-25^,^31^,^33^,^35 with various plausible mechanisms being suggested.7 Chronic hypertension results in a number of maladaptive and degenerative changes in the cerebral vasculature which may lead to reduced cognitive function. Firstly, hypertension induces atherosclerosis in both extracranial and intracranial arteries supplying the brain.7^,^47 Hypertension also leads to increased stiffness of large cerebral arteries through hypertrophic and inward remodeling of the cerebral vessels and deposition of collagen and fibronectin and elastin fragmentation of the vessel wall.7^,^48 In smaller arterioles, hypertension induces endothelial dysfunction and disruption of the blood-brain barrier, triggering inflammatory responses, oxidative stress, and microvasculature injury7 and—by altering small penetrating arterioles supplying the subcortical white matter and basal ganglia—promotes small vessel disease with increased risk of lacunar infarction and white matter leasions.49 Furthermore, hypertension disrupts cerebral autoregulation, by shifting the autoregulation curve of the cerebral blood flow to the right, allowing a similar level of cerebral perfusion at higher levels of BP, but ischemic brain injury if there are sudden or large reductions in BP.7
Reviews which stratified the associations of high SBP/DBP by age provide a clear association between high mid-life BP and the incidence of cognitive decline and dementia. However, there is some evidence that late-life hypertension may have no association or even a “protective” effect.14 This reflects previous work highlighting concerns over intense lowering of BP in older adults and suggestions that this group may require a slightly different approach to maintaining optimal BP for adequate cerebral perfusion.50-54 It should be noted, however, that associations of lower BP with dementia risk in late life might also indicate impairment in homeostasis, potentially as part of the dementia prodrome by being a marker of cognitive impairment beyond normal biological aging.55 Even so, there is now considerable high-quality clinical trial evidence to support the benefits and minimal risks of BP lowering treatment for dementia in the early to mid-phases of later life (mean age 69.1 years).10^,^56^,^57 Our overview of the evidence also revealed an association with poorer function in the domains of global cognitive function, executive function, and memory, although the number of included reviews were small. However, there was heterogeneity around the association with executive function, which is consistent with other studies.7 These inconsistencies could be the results of a lack of standardized assessment of cognitive function across studies.31 Gifford et al31 suggests that this variability in the findings could be due to different tests used in the assessment of executive functioning which might include inhibition or set-shifting measures, cognitive tasks designed to measure 1 domain may be tapping other cognitive processes, increasing variability in findings, test sensitivity, sample selection, and the specific task implemented in each study.
We also found evidence of the relationship of newer BP parameters, raising the potential for future studies to explore the additional risk of these parameters on top of raised SBP/DBP. One of these parameters—BPV—was found to be associated with both cognitive impairment and dementia.14^,^37^,^38 Our summary of the evidence around visit-to-visit systolic BPV shows that higher BPV increases the risk of dementia and increases the risk of cognitive impairment.38 While the evidence was strongest for systolic BPV, visit-to-visit diastolic BPV also increased the risk of dementia and cognitive decline, and a meta-regression revealed a linear relationship between higher systolic BPV and risks of dementia and cognitive impairment.38 Similar findings were observed in the studies with day-to-day BPV.38 Reducing BPV may be a fruitful target to explore for early prevention of dementia.58 There are several suggested mechanisms on how higher BPV leads to cognitive impairment. Firstly, repeated BP fluctuations can cause white matter hyperintensities and brain infarctions as shown in magnetic resonance imaging studies,59 which can in turn lead to loss of cognitive function.60 Higher BPV may also be associated with increased oscillatory shear stress and damage to the vascular endothelium, promoting early atherosclerosis compared to steady blood flow.61 This endothelial dysfunction can damage the blood-brain barrier, and impair cerebral autoregulation, leading to loss of cognitive function.62
There was also limited evidence for a relationship between PWV and cognition.63-65 Higher PWV can cause damage to the brain vasculature and increases the risk of dementia or cognitive decline via several pathological mechanisms. Large arteries lose elasticity with vascular aging, which in turn exposes target organs, including the brain, to higher pulsatile hemodynamic pressure, such as higher blood flow pulsatility.66 Excessive blood flow and low resistance to flow in the brain can expose the small arterial vessels to the high-pressure fluctuations, leading to microvascular damage and cognitive decline/dementia.63 Small vessels tend to progressively reduce their diameter to counteract these changes, increasing microvascular resistance, and eventually leading to loss of brain function.65 Arterial stiffening has also been hypothesized to be associated with tau pathology, β-amyloid plaque deposits, and atrophy of the brain tissue, increasing the risk of MCI or dementia.67
Orthostatic hypotension has also been found to be associated with worse cognition.42^,^43 However, the only 2 reviews in this area included studies that used the MMSE to assess change in cognitive scores. While MMSE is a good screening tool for dementia outcomes, it is less sensitive than other cognitive assessment tools in diagnosing changes in cognition.68 Thus, future studies are needed with a consistent battery of neurocognitive tests to improve the estimate of the magnitude of association between OH and cognition. Peters et al44 highlight how insufficient data were available from the previously published studies to allow separate meta-analysis for systolic, diastolic, or subclinical OH, which warrants further research. There is some evidence to suggest an underlying mechanism relating OH to increased risk of loss in cognition. Repeated cerebral hypoperfusion due to OH may lead to regional structural changes, such as atherosclerosis, hyperintensities in the deep white matter or leukoaraiosis, and cortical watershed microinfarcts, which may underlie the neurodegeneration process in dementia.69^,^70 Repeated episodes of hypotension can also lead to cerebral hypoxia and increased production of ß-amyloid protein and neuroinflammation, which in turn can be potentially responsible for cognitive impairment.71^,^72
Heterogeneity and risk of bias
There was some evidence of heterogeneity and risk of bias in the included reviews. Variation in the definition of hypertension and/or raised SBP/DBP was present across the reviews, or the definitions were not clearly specified. Gifford et al defined their criteria for hypertension as elevated SBP (>140 mm Hg),31 whereas another review defined their criteria as SBP ≥160 mm Hg or DBP ≥90 mm Hg.18 One review defined their criteria as SBP 130 mm Hg and DBP 85 mm Hg, or self-report of antihypertensive medication use.34 This inconsistency can reduce comparability of the outcomes across different studies. The relationship between high SBP/DBP and cognitive decline and/or dementia is also age-dependent, yet few of the meta-analyses reported estimates for mid- and late-life hypertension. Several reviews also reported on cross-sectional outcomes of dementia and/or cognitive decline, which cannot rule out reverse causality, especially since VD may cause low BP due to loss of sympathetic drive.73 Outcomes also varied with some reviews defining their outcome as AD; however, clinical dementia is often a mix of AD and VD, with specific neurodegenerative pathology and cerebrovascular pathology recognized in 61% and 54% of cases, respectively.74 Future studies should broaden their criteria to include patients with evidence for mixed causes of dementia, rather than aiming to identify only pure AD or VD, or select only constituent studies that report pure imaging defined pathology to better guide the prevention of dementia. Most studies on variability focused on visit-to-visit variability, which is more useful for measuring long-term variability. Short-term variability measured using 24-hour ABP monitoring has been shown to be useful at detecting subclinical target organ damage and incidence of cardiovascular events, but remains under-researched in dementia.75^,^76 There are gaps in the populations across the constituent studies in the meta-analyses, such as a lack of data in the oldest old (age ≥75 years) and younger people (<45 years). Constituent studies of the reviews were also predominantly from North America and Europe, with few studies conducted in other countries. Future studies are needed to conclude whether geographical variation can alter the associations between mid- or late-life BP and poorer cognitive outcomes. Finally, there was low overlap in studies for hypertension/SBP/DBP, which was likely due to the differences in selection criteria/process of each review. The reviews encompassing BPV, PWV and OH, showed greater overlap than the others, as their selection criteria were similar.
The strengths of this review are the systematic approach to the search of the evidence, review selection, data extraction and quality assessment, and the use of 2 independent reviewers to reduce potential selection bias. A robust quality assessment was undertaken using internationally recognized criteria, and multiple databases were screened to maximize the inclusion of relevant articles. This review included a range of BP parameters and associated hemodynamic measures. Finally, we assessed the overlap of constituent studies of the included reviews for each BP parameter. There were, however, some limitations. We were unable to reliably perform or reperform any meta-analysis of the individual studies due to the heterogeneity of the data and their reporting; thus, a common point estimate is unavailable. Studies were identified using established databases; however, gray literature was not reviewed, raising the potential for some potential reviews being missed during the screening process.
Directions for future research
Our overview of the literature reinforces the importance of high BP as a risk factor for cognitive decline and dementia but there is a lack of definitive evidence as to which BP parameter has the strongest association with cognitive decline or dementia across different age groups. Furthermore, as the evidence base emerges for the relationship between nontraditional BP parameters, such as BPV, OH and PWV, and dementia risk, additional research may be required to identify accurate and simple approaches to measure these parameters or risk indicators to gain a greater understanding of their role in cognition. Future cohorts with standardized assessments of BP and cognition and long periods of follow-up across the life course are required to address this research gap. A greater understanding of the emerging BP parameters may indicate potential pathways that, if causal, could indicate a potential novel direction for future risk reduction. Further studies are also needed to consider the effect of short-term BPV on cognitive outcomes using 24-hour ABP monitoring, as well as PP, MAP, and cumulative BP load. There is also a need to study specific risk cohorts, such as those with MCI, to understand which parameters more strongly predict dementia outcomes.
Conclusion
High BP is associated with worse cognitive outcomes, but the evidence remains scarce regarding which BP thresholds and population groups are the most vulnerable to dementia. Higher BPV, PWV and OH, in addition to hypertension, are also significantly associated with cognitive decline or dementia, and may be useful for risk assessment of cognitive outcomes. Future studies are required to further clarify pathological pathways by which these parameters lead to further cognitive decline or the incidence of dementia, and design novel interventions to address these pathways. For better comparability, studies should use standardized criteria for defining both BP parameters and cognitive outcomes.
Supplementary Material
hpaf213_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organisation. Dementia. 2021. Accessed September 26, 2025. https://www.who.int/news-room/fact-sheets/detail/dementia
- 2Livingston G , Huntley J, Sommerlad A, et al Dementia prevention, intervention, and care: 2020 report of the lancet commission. Lancet. 2020;396:413-446.32738937 10.1016/S 0140-6736(20)30367-6PMC 7392084 · doi ↗ · pubmed ↗
- 3Cooper C , Sommerlad A, Lyketsos CG, Livingston G. Modifiable predictors of dementia in mild cognitive impairment: a systematic review and meta-analysis. Am J Psychiatry. 2015;172:323-334. 10.1176/appi.ajp.2014.14070878.25698435 · doi ↗ · pubmed ↗
- 4Corrada MM , Hayden KM, Paganini-Hill A, et al Age of onset of hypertension and risk of dementia in the oldest-old: the 90+ study. Alzheimers Dement. 2017;13:103-110. 10.1016/j.jalz.2016.09.0072017/01/2228108119 PMC 5318224 · doi ↗ · pubmed ↗
- 5Ding J , Davis-Plourde KL, Sedaghat S, et al Antihypertensive medications and risk for incident dementia and Alzheimer’s disease: a meta-analysis of individual participant data from prospective cohort studies. Lancet Neurol. 2020;19:61-70. 10.1016/S 1474-4422(19)30393-X 31706889 PMC 7391421 · doi ↗ · pubmed ↗
- 6Canavan M , O'Donnell MJ. Hypertension and cognitive impairment: a review of mechanisms and key concepts. Front Neurol. 2022;13:821135. 10.3389/fneur.2022.82113535185772 PMC 8855211 · doi ↗ · pubmed ↗
- 7Iadecola C , Yaffe K, Biller J, et al; American Heart Association Council on Hypertension; Council on Clinical Cardiology; Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; Council on Quality of Care and Outcomes Research; and Stroke Council. Impact of hypertension on cognitive function: a scientific statement from the American heart association. Hypertension. 2016;68:e 67-e 94. 10.1161/hyp.000000000000005327977393 PMC 5361411 · doi ↗ · pubmed ↗
- 8Launer LJ , Ross GW, Petrovitch H, et al Midlife blood pressure and dementia: the Honolulu-Asia aging study. Neurobiol Aging. 2000;21:49-55. 10.1016/s 0197-4580(00)00096-810794848 · doi ↗ · pubmed ↗