ISDE guidelines on the management of cT2N0 esophageal cancer
Geoffrey P Kohn, Virginia Litle, Yousif Eliya, Samantha Leng, Mohammad Asghari-Jafarabadi, Nicolas Contreras, Andrew Davies, Rudy Lackner, Kimberley S Mak, Tom Mala, Ben Markman, Sarbajit Mukherjee, Christopher Nevala-Plagemann, Elizabeth Smyth, Javed Sultan, Stephanie Worrell

TL;DR
This paper provides guidelines for managing early-stage esophageal cancer, recommending neoadjuvant therapy followed by surgery over immediate surgery for most cases.
Contribution
The paper introduces evidence-based conditional recommendations for managing cT2N0 esophageal cancer from the ISDE.
Findings
Neoadjuvant therapy followed by surgery is conditionally recommended over primary surgery for cT2N0 esophageal cancer.
Preoperative staging remains challenging despite advanced diagnostic tools.
Certain low-risk patients may still be offered primary surgical resection.
Abstract
Esophageal cancer incidence is rising globally, with at least 500,000 new cases diagnosed annually. Management options for non-metastatic disease include primary resection, neoadjuvant or perioperative therapies, or definitive non-surgical treatment, with the choice being guided by tumor staging, histology, patient fitness, and available resources. However, even with the use of advanced diagnostic modalities, preoperative clinical staging is challenging with respect to accuracy of both tumor and nodal assessment. Early-stage esophageal cancer may be managed with local therapies, such as endoscopic mucosal resection or submucosal dissection, while for more advanced tumors managed with curative intent neoadjuvant oncologic therapy is commonly recommended. However, between these two groups lies an infrequent but important subgroup of patients, clinically staged cT2N0M0 esophageal cancer.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
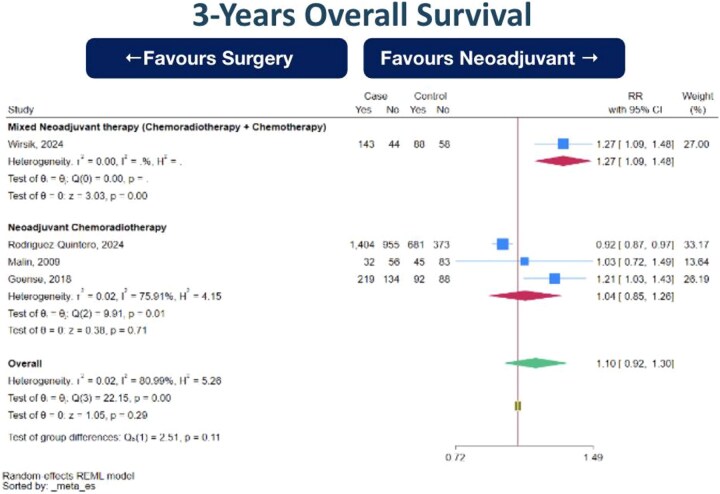 Fig. 1
Fig. 1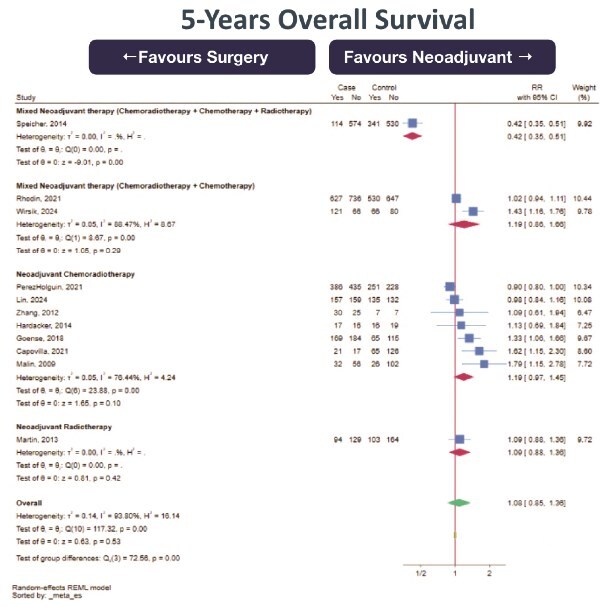 Fig. 2
Fig. 2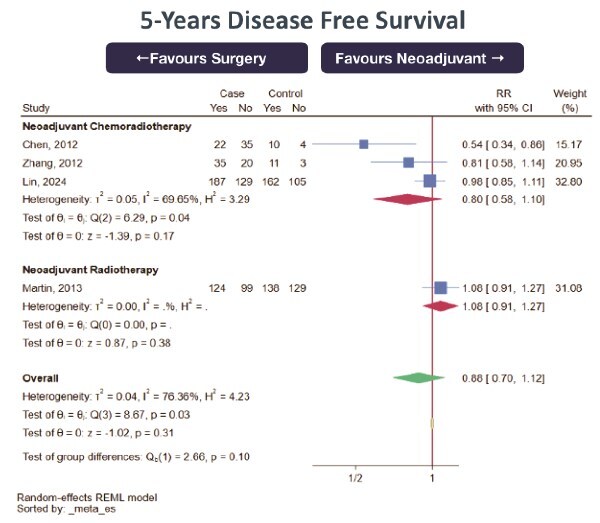 Fig. 3
Fig. 3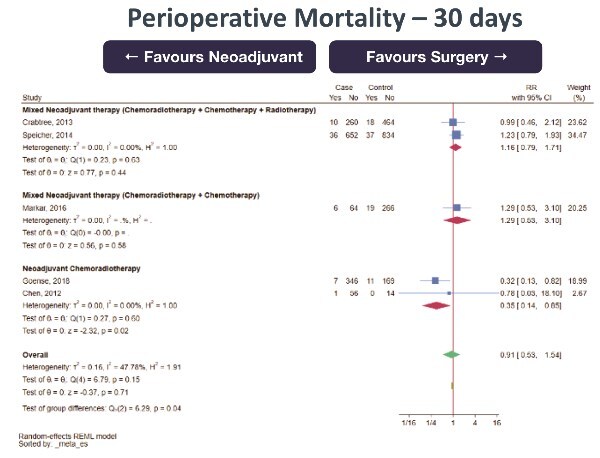 Fig. 4
Fig. 4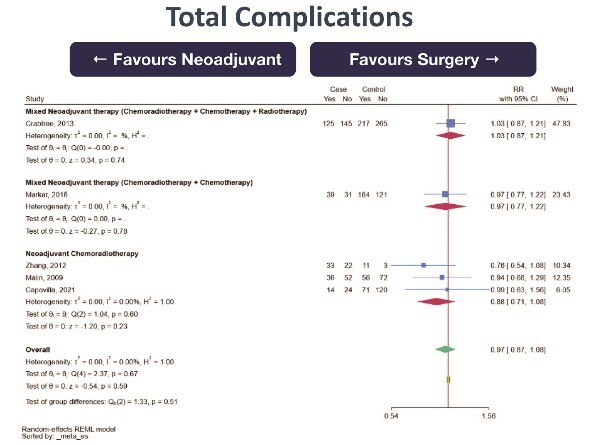 Fig. 5
Fig. 5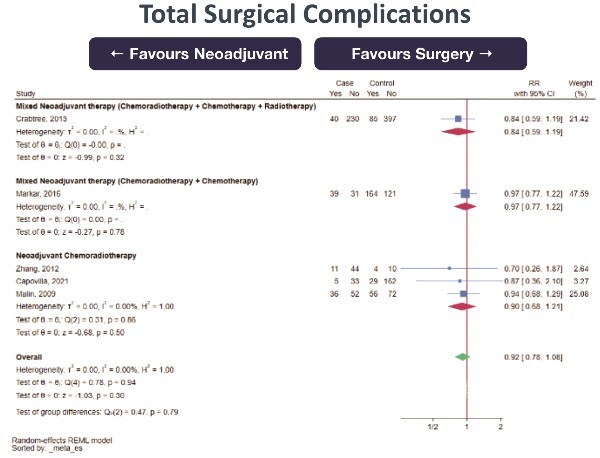 Fig. 6
Fig. 6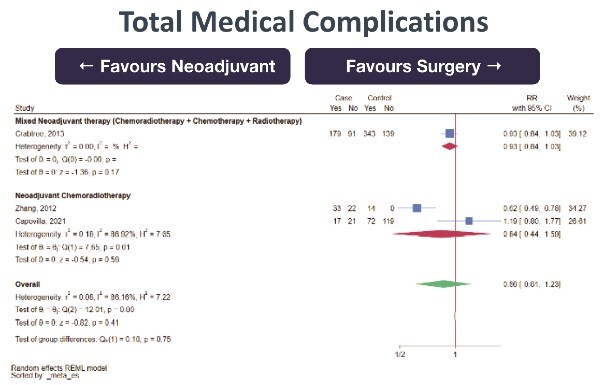 Fig. 7
Fig. 7| Sample size | Histology | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | Year | Country | Design | Total | NeoAdj + S | PSR | Male (%) | Mean age | EAC | SCC | Neoadjuvant therapy type | Risk of bias assessment |
| Capovilla | 2021 | Italy | Retrospective cohort | 229 | 38 | 191 | 83.8 | 61.2 | 96 | 133 | Chemoradiotherapy | High |
| Chen | 2012 | Taiwan (China) | Retrospective cohort | 71 | 57 | 14 | 90.2 | 57.4 | - | 71 | Chemoradiotherapy | Low |
| Crabtree | 2013 | USA | Retrospective cohort | 752 | 270 | 482 | - | 63.8 | 182 | 29 | Chemoradiotherapy + Chemotherapy + Radiotherapy | Moderate-to-high |
| Dolan | 2016 | USA | Retrospective cohort | 27 | 11 | 16 | 93.4 | 65.9 | 25 | 2 | Chemoradiotherapy | Moderate-to-high |
| Goense | 2018 | Netherlands | Retrospective cohort | 533 | 353 | 180 | 74.4 | 64.3 | 422 | 111 | Chemoradiotherapy | Low |
| Hardacker | 2014 | USA | Prospective cohort | 68 | 33 | 35 | 80.9 | 61.7 | 57 | 11 | Chemoradiotherapy | Moderate-to-high |
| Lin | 2024 | China | Retrospective cohort | 583 | 316 | 267 | 78.6 | - | 423 | 160 | Chemoradiotherapy | Low |
| Malin | 2009 | USA | Prospective cohort | 216 | 88 | 128 | - | - | - | 33 | Chemoradiotherapy | Moderate-to-high |
| Markar | 2016 | France | Retrospective cohort | 355 | 70 | 285 | 80.6 | - | 171 | 184 | Chemoradiotherapy + Chemotherapy | Low |
| Martin | 2013 | USA | Retrospective cohort | 490 | 223 | 267 | 77.6 | 64.9 | - | - | Radiotherapy | Low |
| PerezHolguin | 2021 | USA | Retrospective cohort | 1300 | 821 | 479 | - | - | - | - | Chemoradiotherapy | Moderate-to-high |
| Rhodin | 2021 | USA | Retrospective cohort | 2540 | 1363 | 1177 | 82.8 | 64.4 | - | 461 | Chemoradiotherapy + Chemotherapy | Moderate-to-high |
| Rodriguez-Quintero | 2024 | USA | Retrospective cohort | 3413 | 2359 | 1054 | 88.1 | 64.7 | 3413 | - | Chemoradiotherapy | Moderate-to-high |
| Samson | 2016 | USA | Retrospective cohort | 1785 | 853 | 932 | 82.7 | 65.5 | - | - | Chemoradiotherapy + Chemotherapy | Moderate-to-high |
| Song | 2016 | China | Retrospective cohort | 243 | 151 | 92 | - | - | - | - | Radiotherapy | Moderate-to-high |
| Speicher | 2014 | USA | Retrospective cohort | 1559 | 688 | 871 | 84.0 | 63.8 | - | - | Chemoradiotherapy + Chemotherapy + Radiotherapy | Moderate-to-high |
| Wirsik | 2024 | Germany | Retrospective cohort | 333 | 187 | 146 | 82.3 | 67.3 | - | - | Chemoradiotherapy + Chemotherapy | Moderate-to-high |
| Zhang | 2012 | USA | Retrospective cohort | 69 | 55 | 14 | 85.5 | 62.6 | 54 | 15 | Chemoradiotherapy | Moderate-to-high |
| Study | Design | Selection (4 items, 4 points) | Comparability (1 items, 2 points) | Outcome (3 items, 3 points) | Total risk of bias score |
|---|---|---|---|---|---|
| Capovilla 2021 | Retrospective cohort study | 4 | 0 | 1 | 5 |
|
| Retrospective cohort study | 4 | 2 | 2 | 8 |
| Crabtree 2013 | Retrospective cohort study | 4 | 1 | 1 | 6 |
| Dolan 2016 | Retrospective cohort study | 3 | 1 | 2 | 6 |
|
| Retrospective cohort study | 4 | 2 | 2 | 8 |
| Hardacker 2014 | Prospective cohort study | 3 | 1 | 2 | 6 |
|
| Retrospective cohort study- Propensity matched | 4 | 2 | 2 | 8 |
| Malin 2009 | Prospective cohort study | 3 | 0 | 3 | 6 |
|
| Retrospective cohort study | 4 | 2 | 2 | 8 |
|
| Retrospective cohort study | 4 | 1 | 2 | 7 |
| PerezHolguin 2021 | Retrospective cohort study | 4 | 0 | 2 | 6 |
| Rhodin 2021 | Retrospective cohort study | 4 | 0 | 2 | 6 |
| Rodriguez-Quintero 2024 | Retrospective cohort study—propensity matched | 3 | 1 | 2 | 6 |
| Samson 2016 | Retrospective cohort study | 4 | 1 | 1 | 6 |
| Song 2016 | Retrospective cohort study | 4 | 0 | 2 | 6 |
| Speicher 2014 | Retrospective cohort study | 4 | 0 | 2 | 6 |
| Wirsik 2024 | Retrospective cohort study | 4 | 0 | 2 | 6 |
| Zhang 2012 | Retrospective cohort study | 3 | 1 | 2 | 6 |
| Study | Year | Staging modality | Percentage of patients correctly staged | Percentage of total patients upstaged | Percentage of total patients upstaged due to change in nodal status |
|---|---|---|---|---|---|
| Capovilla | 2021 | CT, EUS, PET, Bronchoscopy | 21.4% | 63.4% | 26% |
| Chen | 2012 | CT, EUS, Bone scan, Barium swallow | 42.8% | 25.0% | 7.0% |
| Crabtree | 2013 | No reported | 27.4% | 46.7% | 38.2% |
| Dolan | 2016 | CT, EUS, Endoscopy, ± PET | 6% | 56% | 56% |
| Goense | 2018 | CT, EUS, ± PET | 38% | 62% | 45% |
| Hardacker | 2014 | CT, EUS | 8.5% | 48.5% | 40% |
| Malin | 2009 | CT, Endoscopy, Barium swallow ± EUS/PET ± bronchoscopy | - | - | - |
| Markar | 2016 | CT, EUS, ± PET | - | - | 48.1% |
| PerezHolguin | 2021 | Not reported | 30.1% | 28.7% | 21.3% |
| Rodriguez-Quintero | 2024 | Not reported | - | - | 35.3% |
| Samson | 2016 | Not reported | - | 45.7% | 30.1% |
| Speicher | 2014 | Not reported | 26.7% | 41.6% | 30.2% |
| Wirsik | 2024 | CT, Endoscopy ± PET± EUS | - | - | - |
| Zhang | 2012 | CT ± EUS | 28.6% | 21.4% | 16.05% |
| Summary of conclusions drawn from evidence | Summary of expert consensus beliefs drawn from clinical experience |
|---|---|
| PSR and NeoAdj+S are | Longest overall survival is the most critical outcome for patients |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal Cancer Research and Treatment · Gastric Cancer Management and Outcomes · Gastrointestinal Tumor Research and Treatment
Interpretation of strong and conditional recommendations
Guideline recommendations are typically classified as a ‘strong’ or ‘conditional’ recommendation. The statement ‘the guideline panel recommends’ are used for strong recommendations, and ‘the guideline panel suggests’ for conditional recommendations, as per the Grading of Recommendations Assessment, Development, and Evaluation approach.3 A strong recommendation signals that almost all clinicians should follow the recommended course of action, with the best available evidence suggesting desirable effects clearly outweigh undesirable effects. A conditional recommendation signals that the benefits of adhering to a recommendation probably outweigh the harms although it does also indicate uncertainty. This uncertainty may be due to a lack of high-quality evidence or variability in how individual patients value the outcomes of interest.
How to use these guidelines
These guidelines are primarily intended to aid physicians make decisions about management of patients preoperatively diagnosed with cT2N0M0 esophageal cancer of all histological types. They are also intended to educate, inform policy and advocacy, and to identify future research needs. Clinical decision making is multifaceted, and these guidelines are intended to suggest, but not mandate, an acceptable approach to management of this disorder. Finally, these guidelines can also be used by patients as a basis of discussion with their treating physicians.
Key question addressed by these guidelines
Should PSR vs. neoadjuvant therapy followed by surgery be used for cT2N0 esophageal cancer in adults?
Recommendations
Should PSR vs. neoadjuvant therapy followed by surgery be used for cT2N0 esophageal cancer in adults?
Given the limitations of staging accuracy and the absence of direct trial data, the ISDE Guideline panel suggests that NEOADJUVANT THERAPY FOLLOWED BY SURGERY IS PREFERABLE TO PSR FOR MOST PATIENTS WITH cT2N0 ESOPHAGEAL CANCER. (Conditional recommendation, low certainty of evidence.)
Remark: primary surgery alone may be considered in exceptional cases meeting all of the following: small, well-differentiated tumor, no LVI, and high confidence in staging workup.
No separate recommendation is made by histological subtype, as the available evidence was insufficient to show differential effects.
The evidence does not demonstrate a survival advantage for neoadjuvant therapy in cT2N0 esophageal cancer. However, the panel’s consensus was that high rates of nodal upstaging would favor the use of neoadjuvant therapy and avoid under-treatment of patients in real-world practice.
INTRODUCTION
Aim of these guidelines and specific objectives
The purpose of these guidelines is to provide recommendations based on available evidence and expert opinions regarding the management of all histological types of esophageal cancer staged clinically as cT2N0 by AJCC 8th edition. The target audience includes patients, surgeons, and oncologists. Policy makers and insurance providers interested in these guidelines include those involved in delivering local, national, and international health care services aimed at the treatment of esophageal cancer or to evaluate direct and indirect benefits, harms, and costs related to the various procedures used to treat the disease. This document may also serve as the basis for adaptation by local, regional, or national guideline panels.
Description of the health problems
Background
The global incidence of esophageal cancer is increasing, with 2022 data recording at least 511,000 new cases worldwide with 43,571 from Europe, and 2024 data from the USA recording 22,370 new cases.1 Eastern populations report higher rates of squamous cell carcinoma, with adenocarcinoma more common in the Western world, both with a male preponderance.
Preoperative staging is challenging with significant limitations of available diagnostic modalities, and there remains a risk of staging misclassification. Computed tomography (CT) and endoscopic ultrasound (EUS), widely used, have limited both specificity and sensitivity for accurately describing stage data. CT is poor at detecting T stage, with an accuracy of only 40–50%. EUS is better than CT for T stage, though still struggles to differentiate T2 from T3 disease. EUS is also better than CT for detecting nodal status, particularly if cytology is assessed, though accuracy is still under 90%, and occult nodal metastasis rates of up to 50% have been reported.2^,^3 If local treatment is implemented based on under staged disease, particularly under staged nodal stage, then treatment failure is likely.
Early-stage esophageal cancers, particularly those confined to the mucosa, are often successfully treated by local resection. More advanced tumors require more aggressive treatment as lymph node involvement is common. For intermediate stage disease, such as cT2N0, accurate staging becomes of outmost importance and the need to accurately exclude nodal metastasis is paramount. Available diagnostic modalities are not foolproof and therein lies a source of controversy in management of cT2N0 disease.
European and US groups, such as ESMO and the NCCN respectively, have suggested that neoadjuvant treatment should be implemented for cT2N0M0 disease. Previous recommendations were in favor of chemoradiotherapy for all cellular types but more recent recommendations for esophageal adenocarcinoma support neoadjuvant chemotherapy without radiation (e.g. FLOT protocol).
There is data to suggest that some cT2N0 tumors may be at low risk of nodal metastases. Low risk features include well-differentiated cellular grade, small tumor size, lack of lymphovascular invasion on biopsy and other criteria, and these may be amenable to primary resection. In this scenario, confidence in staging remains of utmost importance. The Japanese Esophageal Society, which heavily relies on EUS and preoperative histology for staging, tends to recommend primary surgery for these presumed lower risk groups. If successful, avoiding chemotherapy and radiotherapy would prevent neoadjuvant therapy-related toxicity, avoid overtreatment, decrease costs, and decrease treatment times.
There has been an evidence gap related to perioperative treatment of cT2N0 esophageal cancer, with recognized trials such as the CROSS trial4 and the ESOPEC trial5 not specifically examining cT2N0 disease and only examining this subgroup with limited number on post hoc analysis. No RCT has conclusively compared surgery alone with neoadjuvant therapy for cT2N0 disease.
METHODS
A Working Group within the ISDE Guidelines Committee performed a systematic review of the literature. This working group comprised 2 surgeons, two research fellows and a methodologist. The group encompassed expertise in the management of both esophageal squamous cell cancer and esophageal adenocarcinoma. The search was performed on 25 November 2024.
The systematic review was performed according to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) checklist6 (Fig. 1). Results of the systematic review were presented to a panel of experts selected by the wider Guidelines Committee, and these results informed the panel discussion about the guideline.
Forest plot of 3-years overall survival (OS) between neoadjuvant therapy followed by surgery (NeoAdj+S) and primary surgical resection (PSR), by neoadjuvant therapy type. Abbreviation: risk ratios, RR.
This panel used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach to deliberate and formulate recommendations, in a manner similar to that reported elsewhere.7 Reporting of this guideline was structured as per the Essential Reporting Items for Practice Guidelines in Healthcare (RIGHT) checklist.8
Guideline panel organization
International experts on esophageal cancer were invited to participate in the ISDE Guideline Panel. All panel members were experienced clinicians with training in either esophageal surgery, medical oncology or radiation oncology, and submitted disclosures on potential conflicts of interest. A non-voting patient from the Queen Elizabeth Hospital Birmingham Oesophageal Cancer Patient Support Group was also included in discussion and decision-making. A methodologist with extensive guideline development experience (MAJ) and the ISDE working group research fellows (YE, SL) participated in the panel as non-voting members and facilitated appraisal of the evidence and formulation of the recommendations. A full list of all contributors to the guideline development is provided in Appendix A.
The panel reviewed the literature presented by the fellows and met via video conference to create the recommendation. The panel reviewed evidence tables populated by the systematic review results and voted on components of Evidence tables to reach final recommendations.
Guideline funding and declaration and management of competing interests
Funding for the methodologist was provided by Cabrini Hospital, as was a research stipend for one research fellow (YE). No industry support was used to create this guideline, nor was any industry input used for any stage of the development, dissemination, or implementation of this guideline. Standard disclosure forms from the journal Diseases of the Esophagus were completed by all guideline contributors to evaluate for potential conflict of interest. Evaluation was made by the panel Chair, and no potential conflicts were deemed to have affected the decision.
Selection of questions and outcomes of interest
The Guidelines Update Task Force performed a literature search on management of cT2N0 esophageal cancer using the systematic review search syntax detailed in Table 1. PSR and (neoadjuvant therapy followed by surgery) were identified as comparators of interest, and key questions were formulated according to the patient-intervention-comparator outcome (PICO) format. Outcomes that were selected ‘critical’ or ‘important’ for patients were selected a priori as outcomes potentially critical or important for decision-making after evidence had been collected. These outcomes centered on efficacy, safety, and side effects associated with esophagectomy, chemotherapy, radiotherapy, and combined modality therapy. These outcomes included overall survival (OS), disease-free survival (DFS) rates, and complication rates.
Evidence appraisal
Results from the ISDE systematic review and meta-analysis were presented to the Panel in the form of Forest plots and associated metrics, to facilitate evidence appraisal and panel decision-making.
Methods outlined in the GRADE handbook were used to judge the certainty of evidence for each outcome of interest. Evidence tables were created. The highest level of data available was used for the tables; less rigorous data that addressed the same outcomes was reviewed but not used in decision making. In brief, the research fellows and methodologist judged the certainty of the body of evidence across the domains of risk of bias, inconsistency, indirectness, and imprecision. The Newcastle-Ottawa Scale (NOS) was used for assessing the risk of bias of nonrandomized studies. If there was concern in any one of these domains, the certainty was downgraded.
Assumed values and preferences
As this guideline have a patient-centered rather than a societal perspective, the panel members used their collective patient experience to make judgements about patient values and preferences. The target audience includes patients, surgeons, and oncologists.
Development of clinical recommendations
The outcomes from the evidence table deemed critical and important to decision-making were determined by the panel. The panel discussed desirable effects, undesirable effects, the certainty of evidence, the potential variation in values of key stakeholders, balance of these effects, and acceptability and feasibility of the option favored by the balance of effects. After discussing the available evidence for each of these components, as well as pertinent additional considerations noted by the panelists based on interpretation of the evidence or expert experience, the panel would vote on each component. Finally, a vote was conducted on the final recommendation for that key question. The recommendation was made when ≥70% of cast votes were in favor.
The panel addressed subgroups such as cancer histological subtypes and grades, molecular markers, and tumor length and location within the esophagus during a discussion for the justification for their recommendation. These considerations are specified below. The evidence, additional considerations, and final judgements for each step in the decision-making process are summarized in the recommendations that follow.
Meta-analysis
This study followed PRISMA guidelines. For categorical outcomes, proportions with confidence intervals were extracted; for continuous outcomes, means and standard deviations were used, converting medians or ranges when necessary. Pooled estimates were obtained using random-effects models with restricted maximum likelihood to account for between-study variability. Heterogeneity was assessed with Q, τ^2^ and I^2^ statistics. Publication bias was evaluated with funnel plots and tested using Egger’s and Begg’s methods, with the trim-and-fill approach applied when bias was detected. Where possible, meta-regression and subgroup analyses explored potential sources of heterogeneity. Sensitivity analyses were performed using a leave-one-out approach. All analyses were conducted in Stata (version 18.5).
Guideline document review
This guideline was drafted based on the evidence tables created by panel voting and discussion. All panel members and working groups members then edited the guideline. The final version of the guideline was then submitted to ISDE leadership for approval before being published online for public comment for 2 weeks. After this public comment period, the final version of this guideline was submitted for final publication.
KEY QUESTION Should PSR OR neoadjuvant therapy followed by surgery be used for cT2N0 esophageal cancer in adults?
Recommendations. Given the limitations of staging accuracy and the absence of direct trial data, the ISDE Guideline panel suggests thatNEOADJUVANT THERAPY FOLLOWED BY SURGERY IS PREFERABLE TO PSR FOR MOST PATIENTS WITH cT2N0 ESOPHAGEAL CANCER. (Conditional recommendation, *low certainty of evidence.)*Remark: primary surgery alone may be considered in exceptional cases meeting all of the following: small, well-differentiated tumor, no LVI, and high confidence in staging workup.No separate recommendation is made by histological subtype, as the available evidence was insufficient to show differential effects.The evidence does not demonstrate a survival advantage for neoadjuvant therapy in cT2N0 esophageal cancer. However, the panel’s consensus was that high rates of nodal upstaging would favor the use of neoadjuvant therapy and avoid under-treatment of patients in real-world practice.
Summary of the evidence
A total of eighteen studies were included in this analysis. To the extent possible, it was determined that no data were double-counted from any of the included large databases. No randomized controlled trials (RCTs) were identified. Fourteen were retrospective cohort studies, two were retrospective cohort studies with propensity score matching, and two were prospective cohort studies. All included studies were comparative studies between PSR and neoadjuvant therapies followed by surgery (NeoAdj+S). Among these, neoadjuvant chemoradiotherapy was used in ten studies, neoadjuvant radiotherapy alone was used in two studies, and the remaining six studies were a mixture of chemotherapy alone, radiotherapy alone, or combined modality therapy (Table 1).
Risk of bias was considered to be high among studies included in this analysis. Of the 18 included studies only five studies (28%) were rated as low risk of bias, scoring above 7 on the NOS (Table 2). The other 13 studies received a moderate-high or high risk of bias rating. In particular, studies were weakest in the Comparability domain of the NOS which assesses the degree to which studies have been controlled for confounding (Table 2).
Benefits
PSR had similar effectiveness as neoadjuvant therapy (all combinations) followed by surgery (NeoAdj+S) with regards to:
3-year OS (0 RCT, 1 prospective cohort study, 3 retrospective cohort studies; total 4495 subjects, very low certainty of evidence, RR 1.10 [95%CI 0.92–1.30] favoring NeoAdj+S) with high heterogeneity (Fig. 1)5-yearr OS (0 RCT, 2 prospective cohort studies, 9 retrospective cohort studies; total 7920 subjects, very low certainty of evidence, RR 1.08 [95%CI 0.85–1.36] favoring NeoAdj+S) with high heterogeneity (Fig. 2).5-year DFS (0 RCT, 4 retrospective cohort studies; total 1213 subjects, very low certainty of evidence, RR 0.88 [95%CI 0.70–1.12] favoring PSR) with high heterogeneity (Fig. 3)
Forest plot of 5-years overall survival (OS) between neoadjuvant therapy followed by surgery (NeoAdj+S) and primary surgical resection (PSR), by neoadjuvant therapy type. Abbreviation: risk ratios, RR.
Forest plot of 5 disease-free survival (DFS) between neoadjuvant therapy followed by surgery (NeoAdj+S) and primary surgical resection (PSR), by neoadjuvant therapy type. Abbreviation: risk ratios, RR.
The combined magnitude of these effects was thought by the panelists to be small. Additional supplementary figures may be found in supplementary Appendix B.
Harms and burden
PSR had similar harms as neoadjuvant therapy (all combinations) followed by surgery (NeoAdj+S) with regards to:
30-day mortality (0 RCT, 5 retrospective cohort studies; total 3270 subjects, very low certainty of evidence, RR 0.91 [95%CI 0.53–1.54] favoring NeoAdj+S) with moderate heterogeneity (Fig. 4)Total complications (0 RCT, 1 prospective cohort studies, 4 retrospective cohort studies; total 1621 subjects, very low certainty of evidence, RR 0.97 [95%CI 0.87–1.08] favoring NeoAdj+S) with low heterogeneity (Fig. 5)Surgical complications (0 RCT, 1 prospective cohort study, 4 retrospective cohort studies; total 1621 subjects, very low certainty of evidence, RR 0.92 [95%CI 0.78–1.08] favoring NeoAdj+S) with low heterogeneity (Fig. 6)Medical complications (0 RCT, 3 retrospective cohort studies; total 1050 subjects, very low certainty of evidence, RR 0.86 [95%CI 0.61–1.23] favoring NeoAdj+S) with high heterogeneity (Fig. 7)
Forest plot of 30-day mortality between neoadjuvant therapy followed by surgery (NeoAdj+S) and primary surgical resection (PSR), by neoadjuvant therapy type. Abbreviation: risk ratios, RR.
Forest plot of total complications between neoadjuvant therapy followed by surgery (NeoAdj+S) and primary surgical resection (PSR), by neoadjuvant therapy type. Abbreviation: risk ratios, RR.
Forest plot of surgical complications between neoadjuvant therapy followed by surgery (NeoAdj+S) and primary surgical resection (PSR), by neoadjuvant therapy type. Abbreviation: risk ratios, RR.
Forest plot of medical complications between neoadjuvant therapy followed by surgery (NeoAdj+S) and primary surgical resection (PSR), by neoadjuvant therapy type. Abbreviations: risk ratios, RR.
The combined magnitude of these effects was thought by the panelists to be small. Additional supplementary figures may be found in Appendix B.
Certainty of evidence
The certainty in these effects was rated as very low owing to the risk of bias and imprecision of the estimates. The overall certainty of evidence was deemed very low.
Decision criteria and additional considerations
The panel considered the value for decision-making that well-informed patients would place on the main outcomes based on their experience and the available evidence. Direct patient input was also incorporated in this discussion regarding the assignment of relative values of outcomes.
Longest OS data was deemed by the panel as the most critical outcome, though the patient advocate ranked this second to 30-day mortality, with other complications being ranked less important by both panel and patient. Our analysis found that OS, 30-day mortality rates, and total complication rates were largely equivalent in both PSR patients and NeoAdj+S patients.
The panel acknowledged the results of the meta-analysis. However, the poor accuracy of preoperative clinical staging was of concern, particularly understaging of nodal disease, as knowledge of lymph node involvement would strongly support neoadjuvant therapy before operation. Also, certain biological features of the tumor, such as poorer differentiation, large size and lymphovascular invasion would tend to direct experts in favor of NeoAdj+S, irrespective of actual clinical TNM staging.
Accuracy of preoperative clinical staging, that is the correlation of cTNM with pTNM, was noted to be poor, even in the modern era with accessibility of EUS, MRI, flexible bronchoscopy, and PET scans. Accurate staging was reported in approximately 6–42.8% of cases across the reviewed studies.9^,^10
Upstaging after histopathological review of the resected specimen was common (range 21.4–63.4% of cases)11 (Table 3). Most concerningly, among all patients presumed to be cT2N0M0, upstaging occurred secondary to unexpected nodal disease in up to 48% of cases, highlighting limitations in preoperative nodal assessment. The panel agreed that PSR of the tumor, but leaving lymph nodes involved with tumor as would be seen when node-negative disease is unexpectedly upstaged to node-positive disease, would predictably lead to recurrent disease. The frequency of postoperative adjuvant treatment for pathologically upstaged tumors was unclear in some studies, introducing a confounder into the analysis.
Poor differentiation of the primary cancer was thought by the panel to be a factor suggesting the need for a NeoAdj+S approach, and this is reflected in current AJCC 8th edition staging for esophageal cancer, wherein T2N0M0 adenocarcinoma is upstaged from Stage IC to IIA in the presence of poor differentiation, and squamous cell cancer is upstaged from Stage IB to IIA unless the cells are well-differentiated. Beyond poor differentiation, the panel agreed that size and lymphovascular invasion are additional high-risk features. The panel considered tumors ≥2 cm in length to be considered large.
The panel recognizes that cancer patterns differ between geographical locations, with a panel member from Japan emphasizing the higher percentage of squamous cancer in the Japanese population. Moreover, there is greater patient awareness of the disease in Japan, and some well-informed patients may request organ preservation techniques with definitive chemoradiation even for cT2N0 disease.12
There were also subgroups of patients for whom the panel members expressed a preference for PSR, such as in elderly patients deemed unfit for neoadjuvant therapy based on physiological parameters. The corollary held true, in that the panel confirmed their preference for NeoAdj+S for younger patients, particularly those thought fit enough by physiological metrics to be able to tolerate FLOT protocol chemotherapy. However, even in this group, shared decision making with the patient is of utmost importance, because in a very selected subgroup of young healthy patients, with well-differentiated cancers, no high-risk features (such as lymphovascular invasion), and a very small tumor (suggested by the panel to be defined as <2 cm in length), some experts would consider PSR as a preferable option. When deciding upon a PSR approach, preoperative staging should utilize best available modalities, thought by the panel to be routine FDG-PET and EUS.
For the intermediate group, those patients (particularly with adenocarcinoma) thought unable to tolerate full course neoadjuvant FLOT chemotherapy, there was some preference for the less effective, but better tolerated CROSS protocol chemoradiation. Specific physiologic criteria were not able to be agreed upon, and the importance of multidisciplinary review by surgeons, oncologists, and radiologists, in conjunction with the patient, was stressed.
Finally, the panel agreed that a preferred comparative study would be clinical staging with all available modalities, matched for high-risk features of size, grade, and lymphovascular invasion, and then comparing the neoadjuvant FLOT protocol chemotherapy with CROSS chemoradiation, and both against primary resection. Emerging data reviewing cancers deficient in DNA mismatch repair (dMMR) and its effect on choice of treatment were discussed without definitive recommendations being formulated. Subgroup analysis was considered in this guideline, particular examining histological subtype, but comparative data was minimal and clear description of protocols limited in the included publications, and therefore this analysis was not performed.
It was re-emphasized by the panel that there was evidence to support some of the above findings, while other findings lacked evidence and relied heavily on expert opinion (Table 4).
Values
The panel voted that there was certainty that OS from esophageal cancer was the most important outcome of treatment of cT2N0 disease, with 75% of the panel voting that there was either ‘probably no important uncertainty’ or only ‘possible uncertainty’ in how much patients might value the main outcome. DFS, quality of life issues, and perioperative complications were thought to be less important. However, the patient representative was most concerned with perioperative complications, in particular perioperative mortality, though the representative felt that the list of outcomes was comprehensive, and representative of what patients care about.
Balance of effects
The balance between desirable and undesirable effects in the data reviewed does not favor either PSR or NeoAdj+S.
Acceptability
The panel voted that NeoAdj+S is an acceptable intervention for patients and clinicians.
Feasibility
The panel voted that NeoAdj+S is feasible to implement relative to PSR.
Conclusion
The panel suggests, even though pooled data from the metanalysis seem to demonstrate equivalence between PSR and NeoAdj+S for cT2N0 esophageal cancer, and based on concerns related to accuracy of clinical staging and inadequacy of defining higher risk groups, that NeoAdj+S should be preferred as a conditional recommendation and subject to shared decision making with the patient.
This decision making will consider the absence of strong data supporting this position, as well as the difference in values of the panel and the patient representative around prioritizing OS versus minimizing perioperative complications, and particularly the patients’ views on organ preservation and their acceptance of neoadjuvant therapy in general. Subgroups, particularly those patients deemed unlikely to tolerate neoadjuvant treatment protocols, may reasonably be offered primary resection. Occasionally, certain groups deemed to be of lower risk of undiagnosed nodal disease, such as patients with no high-risk features and tumors of short length, may reasonably be offered PSR in an effort to avoid potential ineffective neoadjuvant therapy. Definitive chemoradiation should be reserved only for those patients unfit for resection.
With the high risk of bias arising from the multiple potential confounding factors, any actual difference in effect between the two treatment strategies may have been masked, and the conditional recommendation was made despite these biases, driven by clinical reasoning and of the inherent risk of understaging of thereby of undertreatment.
Subgroup considerations
Staging factors related to poor accuracy of clinical staging methods.High-risk tumor factors such as tumor grade, disease length, lymphovascular invasion, dMMR status.13Older patients and those with poor physiological parameters.Younger, fitter patients with no high-risk factors.
Research recommendations
The panel made several recommendations for future research considerations:
To refine our recommendations, prospective studies are needed focusing on cT2N0 in high risk subgroups, including poorly differentiated tumors or tumors with lymphovascular invasion, as well as length of tumor.Explore biomarkers such as circulating tumor DNA, PD-L114 in the context of staging of cT2N0 cancers.No specific data on neoadjuvant immunotherapy exist yet for this population, but emerging trials should assess its role,15 such as for patients with cancers deficient in dMMR.
Cost analysis studies
No data was available to make a recommendation, but cost-effectiveness might be particularly relevant if intensive neoadjuvant regimens (such as FLOT or chemoradiation) are used without a clear survival benefit.
IMPLEMENTATION OF THESE GUIDELINES
In order to implement neoadjuvant therapies prior to esophagectomy, it is necessary for facilities to have adequate infrastructure and clinician training. It is thought likely that the majority of centers capable of performing esophagectomy would have the necessary facilities and expertise to provide all forms of neoadjuvant therapy. There will be some centers, mainly in resource-poor locations of low- and middle-income countries where certain treatment options, such as radiotherapy facilities, are lacking. In such situations, weighing the benefits of local treatment versus transfer to a larger center will need to be considered.
In addition to local institutional resources, health equity considerations such as third-party payer denials (e.g. in the preoperative prescription of immune checkpoint inhibitors) may also be a barrier to implementation and should be considered by the clinician and facility managing esophageal cancers.
MONITORING AND EVALUATION
The panel agreed that detailed clinical staging investigations with at least FDG-PET and EUS should be performed before initiating treatment by either PSR or NeoAdj+S.
Facilities performing esophagectomy should be clear about which patient populations are being selected for the respective techniques, and their comorbidities.
Tumor characteristics such as lymphovascular invasion, tumor length, MMR status, and tumor grade should be monitored. It is also suggested to monitor clinical findings and investigations which are used to evaluate the physiological suitability for various treatment regimens. Quality of life should also be measured using validated instruments at follow-up appointments.
UPDATING THESE GUIDELINES
The ISDE Guidelines Committee plans to re-evaluate these guidelines three years post-publication.
LIMITATIONS OF THESE GUIDELINES
The literature search strategy was limited to English language publications which introduced the risk of language bias, though with the global span of included from Europe, the Americas, and Asia, this is probably minimal. The limitations of these guidelines are inherent to the very low certainty of the evidence for the Key Question. The recommendations are thus to large extent restricted to the level of expert opinion. Furthermore, data is limited by known challenges with the accuracy of preoperative clinical staging for cT2N0 esophageal cancer. Additionally, factors which might preoperatively better determine the risk of undiagnosed nodal disease are not well understood.
Risk of Bias assessment with the NOS showed greatest weakness in the Comparability domain, with many studies lacking adjustment for prognostic factors. In particular, patients selected for primary surgery (PSR) versus neoadjuvant therapy (NeoAdj+S) may have differed systematically (e.g. tumor biology or fitness), potentially biasing outcomes. Additionally, analysis of patients upstaged by pathologic nodal status (pN+), and who subsequently received adjuvant treatment, might dilute any survival difference and confound results.
Supplementary Material
Supplementary_material_doag019
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Commission E . European Cancer Information System. 2025. https://ecis.jrc.ec.europa.eu, accessed on 18 October 2025.
- 2Goense L, Visser E, Haj Mohammad N et al. Role of neoadjuvant chemoradiotherapy in clinical T 2N 0M 0 esophageal cancer: a population-based cohort study. Eur J Surg Oncol 2018; 44(5): 620–EP–5. 10.1016/j.ejso.2018.02.005.29478739 · doi ↗ · pubmed ↗
- 3Markar S R, Gronnier C, Pasquer A et al. Role of neoadjuvant treatment in clinical T 2N 0M 0 oesophageal cancer: results from a retrospective multi-center European study. Eur J Cancer 2016; 56: 59–EP–68.26808298 10.1016/j.ejca.2015.11.024 · doi ↗ · pubmed ↗
- 4Noordman B J, Verdam M G E, Lagarde S M et al. Effect of neoadjuvant chemoradiotherapy on health-related quality of life in esophageal or junctional cancer: results from the randomized CROSS trial. J Clin Oncol 2018; 36(3): 268–75. 10.1200/JCO.2017.73.7718.29161204 · doi ↗ · pubmed ↗
- 5Hoeppner J, Lordick F, Brunner T et al. ESOPEC: prospective randomized controlled multicenter phase III trial comparing perioperative chemotherapy (FLOT protocol) to neoadjuvant chemoradiation (CROSS protocol) in patients with adenocarcinoma of the esophagus (NCT 02509286). BMC Cancer 2016; 16: 503.27435280 10.1186/s 12885-016-2564-y PMC 4952147 · doi ↗ · pubmed ↗
- 6Tugwell P, Tovey D. Prisma 2020. J Clin Epidemiol 2021; 134: A 5–6. 10.1016/j.jclinepi.2021.04.008.34016443 · doi ↗ · pubmed ↗
- 7Rogers A T, Dirks R, Burt H A et al. Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) guidelines development: standard operating procedure. Surg Endosc 2021; 35(6): 2417–27. 10.1007/s 00464-021-08469-z.33871718 · doi ↗ · pubmed ↗
- 8Yaolong Chen, Kehu Yang, Ana Marušić, et al. for the RIGHT (Reporting Items for Practice Guidelines in Healthcare) Working Group . A Reporting Tool for Practice Guidelines in Health Care: The RIGHT Statement. Ann Intern Med 2017;166:128–132.