Methods and tools used to assess patient experience with healthcare services in prisons: a scoping review
Katherine E McLeod, Amie Hilditch, Amanda Butler, Rith Bal, Fiona G Kouyoumdjian

TL;DR
This review explores how patient experiences of healthcare in prisons are measured, highlighting gaps and the need for better tools.
Contribution
The study identifies gaps in current methods and emphasizes the need for validated, context-specific tools for measuring patient experience in correctional healthcare.
Findings
Most studies used surveys or qualitative methods, but none used validated tools for correctional healthcare.
Fewer studies addressed respect, empathy, and autonomy in patient care assessments.
There is a lack of geographic diversity and attention to confidentiality and compensation in the reviewed studies.
Abstract
Measures of patient experience of healthcare services are important to improving quality of care and health outcomes. In correctional facilities, healthcare is shaped by key features of the environment, including security constraints and uncertain lengths of stay. In this scoping review, we aimed to map the existing literature and identify knowledge gaps to inform efforts to implement and enhance measures of patient experience in correctional settings. We conducted a search of health sciences databases and grey literature for original research articles on 6 December 2024. We included studies in which people currently incarcerated in a correctional facility were asked about their experiences of healthcare received in custody. Two people independently assessed all titles and abstracts, reviewed full texts, and completed data extraction. We assessed how measures of patient experience in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
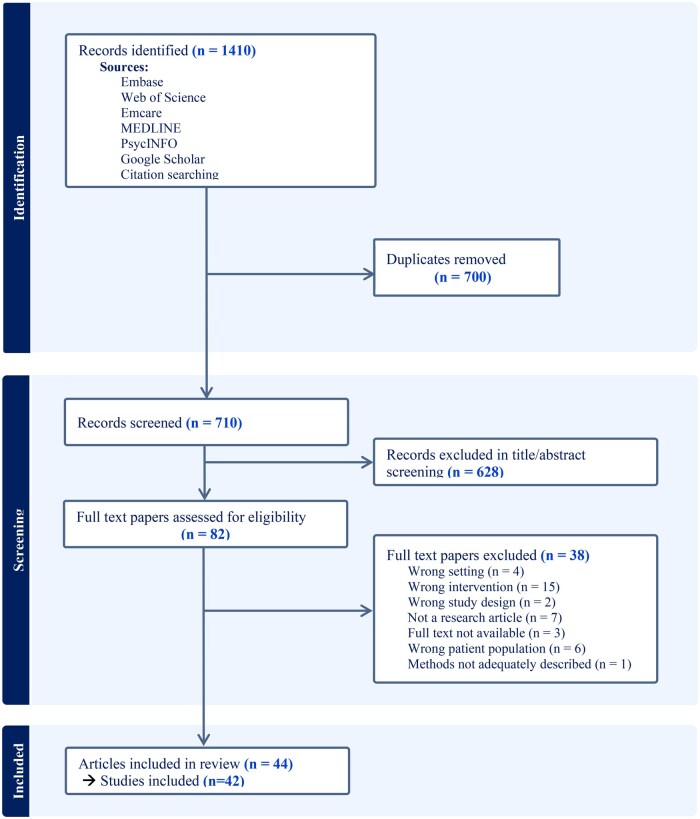 Figure 1
Figure 1| Picker Principles of Person-centred Care | Other question types | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study | Fast access to reliable healthcare advice | Effective treatment by trusted professionals | Continuity of care and smooth transitions | Involvement and support for families and carers | Clear information, communication and support for self-care | Involvement in decisions and respect for preferences | Emotional empathy and respect | Attention to physical and environmental needs | Overall satisfaction | General (qualitative methods) |
| Abbott 2023 [ | x | |||||||||
| Alirezaei 2022 [ | x | |||||||||
| Barling 2005 [ | x | x | x | x | x | |||||
| Besney 2018 [ | x | x | x | |||||||
| Bjorngaard 2009 [ | x | x | x | x | x | |||||
| Butler 2003 [ | x | x | x | x | x | |||||
| Capon 2020 [ | x | x | x | |||||||
| Cheng 2018 [ | x | x | x | |||||||
| Colombo 2022 [ | x | x | x | x | x | |||||
| Condon 2007 [ | x | |||||||||
| Cuadrado 2021 [ | x | x | x | x | x | |||||
| Galli 2019 [ | x | |||||||||
| Hankins 2022 [ | x | |||||||||
| Hsieh 2022 [ | x | x | x | x | x | |||||
| Jaffer 2016 [ | x | x | ||||||||
| Jimenez-Galan 2019 [ | x | x | x | x | x | |||||
| Jordan 2012 [ | x | |||||||||
| Kanbergs 2019 [ | x | x | ||||||||
| Karachaliou 2024 [ | x | x | x | x | x | x | ||||
| Khalaf 2019 [ | x | x | x | |||||||
| Lafferty 2022 [ | x | |||||||||
| Liauw 2021 [ | x | |||||||||
| Magaletta 2000 [ | x | x | x | |||||||
| Marco 2013 [ | x | x | ||||||||
| Mekhjian 1999 [ | x | x | x | |||||||
| Morgan 2008 [ | x | |||||||||
| Motshabi 2011 [ | x | x | x | x | x | |||||
| Myers 2006 [ | x | x | x | x | ||||||
| Plugge 2008 [ | x | |||||||||
| Rogalska 2022 [ | x | |||||||||
| Ross 2011 [ | x | x | x | |||||||
| Russell 2022 [ | x | |||||||||
| Sawasdipanich 2018 [ | x | |||||||||
| Schroeder 2005 [ | x | |||||||||
| Sifunda 2006 [ | x | |||||||||
| Sindicich 2016 [ | x | |||||||||
| Tanguay 2014 [ | x | x | x | x | x | |||||
| Tucker 2005 [ | x | x | x | |||||||
| Way 2007 [ | x | x | x | x | x | x | ||||
| Williams 2022 [ | x | |||||||||
| Wong 2018 [ | x | x | x | x | x | |||||
| Young 2000 [ | x | |||||||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCriminal Justice and Corrections Analysis · Healthcare Decision-Making and Restraints · Patient-Provider Communication in Healthcare
Introduction
Patient experience is a key aspect of healthcare quality and enhancing patient experience of care is one of the core pillars of improving health systems outlined in the Quintuple Aim [1]. Positive patient experiences are associated with higher levels of patient safety and clinical effectiveness, greater adherence to treatment, better health outcomes, and reduced burden on healthcare resources [2]. In correctional facilities, where delivery of healthcare services is shaped by structural and security constraints unique to the carceral environment, understanding and measuring patient experience is especially important.
People who experience incarceration have a higher burden of mental and physical health conditions and often have complex healthcare needs [3, 4]. They also face systemic barriers to accessing healthcare both in custody and in the community, including stigma based on their history of criminalization [5–7]. While in community healthcare settings measures of patient-reported experience or satisfaction with healthcare are used, and in some cases required [8, 9], to monitor quality of care, they are uncommon in the context of correctional facilities. Frameworks of patient-centred care, such as the Picker Principles of Person-Centred Care [10] highlight key dimensions of person-centred healthcare including involvement in decision-making, respect, communication, and access to care. In prisons, these principles may be in tension with policies and priorities of security and control. Therefore, tools used in community settings to measure patient experience may not capture the distinct realities of people receiving care in the carceral context such as lack of privacy or confidentiality, altered access to medications, and interactions with healthcare that are compelled by procedure rather than choice [11–13]. The carceral environment also presents unique challenges to data collection such as access to potential participants and perceptions of confidentiality or coercion [14].
There is a need for robust, context-specific methods and tools for measuring patient experience of healthcare in custody in order to improve healthcare services and address health inequities. In this context, the objective of this scoping review is to map the existing literature and to identify and analyse knowledge gaps related to measuring patient-reported experience of healthcare services in correctional facilities.
Materials and methods
We conducted this scoping review following the JBI guidelines [15] and we report methods in alignment with the Preferred Reporting Items for Systematic Reviews and Meta-analysis extension for scoping review checklist [16]. This review was guided by the research question: how have studies reported processes and tools used to measure patient experience of healthcare services in correctional facilities?
Eligibility criteria
We included full-text, original research articles which described methods of understanding or measuring patient experiences of healthcare services delivered in correctional facilities. Specifically, study participants had to be incarcerated at the time of the study in facilities related to the administration of criminal justice (i.e. we excluded studies with people previously incarcerated, or currently in secure mental health facilities, or immigration detention centres, or prisoners of war). We considered ‘healthcare services’ to be the fundamental functions of healthcare services including testing, diagnosis, condition management, and treatment. We excluded studies investigating ancillary programmes (e.g. stress management or domestic violence workshops) as these are outside the scope of fundamental functions of healthcare services, and we also excluded studies in which the primary focus was describing experiences of a particular illness or condition rather than the healthcare received.
Information sources
We developed and refined our search strategy in consultation with a health sciences research librarian. We used index records of relevant articles identified in an initial search of MEDLINE and Embase to develop a full search strategy for MEDLINE (Appendix 1). The search strategy, including keywords and index terms, was translated to Embase, Emcare, PsycInfo, and Web of Science Core Collection. We also searched the first 10 pages of Google Scholar and the reference lists of all articles included in our study for relevant studies. We included studies published in any language, though we used only English-language search terms. Articles not in English were translated using Google Translate, which has been shown to be accurate for the purpose of extracting data for systematic reviews [17]. There were no date limitations imposed on our search. The most recent search was conducted on 6 December 2024.
Selection of articles
We uploaded all identified records into Covidence [18], a web-based collaboration platform designed to streamline review processes. After duplicates were removed, two project team members independently assessed all titles and abstracts for eligibility using predetermined inclusion criteria. Articles included for full review were independently assessed by two project team members. At both stages, reviewers discussed any disagreements until consensus was reached.
Data charting
To collect data, a charting form was developed by the research team. Two team members independently applied the charting form to the same five articles and then met to discuss and refine the charting form prior to its use on the full data set, as recommended by Levac et al. [19]. Two reviewers independently extracted data from each included study. Consistent with standards for scoping reviews, we did not conduct any quality appraisals [16]. We collected data on study location, number/type of correctional facilities, participant characteristics, the specific healthcare services studied, study design (including recruitment and sampling methods, data collection, compensation, and confidentiality considerations), the study’s data collection tool(s), data collected, major topics of inquiry, study limitations reported by authors, and intended application of study findings.
To assess the aspects of healthcare explored in studies of patient experience, we examined topics of inquiry presented in data tools (e.g. interview scripts, survey questions) or, when tools were not provided, questions investigated as reported by study authors. We categorized topics using the eight Picker Principles of Person-Centred Care [10]. These principles set out a framework for high-quality person-centred care across patient pathways: (i) fast access to reliable healthcare advice; (ii) effective treatment by trusted professionals; (iii) continuity of care and smooth transitions; (iv) involvement and support for family and carers; (v) clear information, communication, and support for self-care; (vi) involvement in decisions and respect for preferences; (vi) emotional support, empathy, and respect; (vii) attention to physical environment and needs. Examples of questions categorized within each principle are provided in Appendix 2.
Findings
After duplicates were removed, our search identified 710 records for title and abstract screening. Of these, 82 articles were advanced to full text review. One article in German [20] was translated to English using Google Translate. We found two papers reporting the same findings from the same study and published in the same year. We retained the original research article for data extraction [21] and excluded the shorter summary article [22]. Finally, 44 papers reporting on 42 studies were included in this study (Fig. 1).
PRISMA flow diagram of study selection process.
Study design
A summary of included studies is provided in Appendix 3. Studies were conducted in 16 countries, with more than half conducted in one of three countries: the USA (n = 10, 24%) [21, 23–31], UK (n = 8, 19%) [11, 32–38], and Australia (n = 6, 14%) [39–45]. Three studies were conducted in each of Canada [46–48], and Spain [49–51], two studies were conducted in South Africa [52, 53] and one study was conducted in each of China [54], Germany [20], Greece [55], Iran [56], Lebanon [57], Norway [58], Poland [59], Switzerland [60, 61], Taiwan [62], and Thailand [63]. Surveys were the most common method of data collection and were used in 24 studies [20, 23, 25–30, 36, 37, 39, 40, 45, 48–52, 54, 55, 57–59, 62] including three studies which used a combination of survey and qualitative methods [20, 48, 52]. Eighteen studies used qualitative methods, including interviews (n = 10) [21, 24, 31–34, 42–44, 56, 61], focus groups (n = 5) [38, 41, 46, 47, 53], or a combination of both (n = 3) [11, 35, 63]. Studies measured experiences of healthcare generally (n = 19) [11, 20, 24, 26, 29, 31, 33, 35–41, 45, 46, 53, 58–63], mental healthcare (n = 7) [25, 27, 28, 30, 34, 54, 55], reproductive healthcare including pregnancy care (n = 4) [14, 21, 47, 56], substance use and addictions care (n = 4) [44, 48, 51, 57], specialist care (n = 2) [26, 37], care for hepatitis C (HCV; n = 2) [42, 43, 50], and testing for sexually transmitted and blood-borne infections (n = 2) [42, 43, 52]. Additionally, one focus group study examined methods of gathering patient feedback on experiences of healthcare in custody used in two English prisons [33], and one study examined experiences of care among transgender people taking hormones in custody [23]. Nine studies examined the acceptability of telemedicine or telepsychiatry [20, 25–28, 49, 50, 54, 55]. The midpoint for data collection for just under half of studies (17/42, 40%) was within the last 10 years (between 2015 and 2021) [20, 24, 33, 38, 41–43, 45–50, 54–57, 59]. Twelve studies did not report study dates [21, 23, 26, 27, 29, 31, 32, 34, 35, 37, 53, 63].
Participants
The number of people included in each study ranged from 4 [34] to 4887 [36] [median 75, interquartile range (IQR) 25–200]. One study did not specify number of participants [53]. Eighteen studies examined experiences of men in custody [23, 25, 27, 30, 34, 37, 38, 42, 43, 45, 49–55, 57, 62], eight studies explored experiences of women [21, 31, 32, 35, 46, 47, 56, 63], and the remaining 16 included both men and women with the proportion of women ranging from 3.3% [39] to 66.7% [33] (median 8.6%, IQR 0%–30.8%). One study reported on the healthcare experiences of transgender people in custody [23].
Three Australian studies [40, 42–44] reported compensating participants 20 [21], and one Canadian study reported giving participants edible items from the canteen worth $10 [46]. Nine studies reported that compensation was not provided, with two Canadian studies [47, 48] and one US study [31] specified that compensation was not allowed by correctional authority policy. The remaining 28 studies did not report whether people participating in the research received any compensation.
Confidentiality
In 17 studies, data collection was conducted by an external researcher. For 11 studies using surveys, data collection was facilitated or collected by staff [28–30, 37, 39, 40, 45, 51, 57–59]; including two studies in which healthcare staff collected data in facilities in which they did not routinely practice [39, 64], one study where staff were deployed from a correctional services central office [29] and one study in which surveys were distributed by correctional staff [59]. Fourteen studies did not specify who collected data [20, 21, 23, 25–27, 36, 44, 49, 52, 54, 55, 62, 63]. Nine studies (seven qualitative and two survey) reported that data collection took place in a private space within the prison, such as clinic rooms, or specified that staff were not present [11, 23, 24, 31, 35, 39, 42, 43, 56, 60, 61], including one study reporting that a correctional officer was positioned outside the room but in line-of-sight [39].
Three studies reported evaluation processes that were not confidential: one conducting focus groups in the presence of prison officers [41], another reported that staff wrote participants names across questionnaires as they were distributed [28], and one reported conducting interviews in the presence of the person’s mental healthcare clinician and submitting transcripts to the prison’s security department [34]. Fifteen studies did not report on how confidentiality was addressed [21, 25–27, 32, 38, 46, 49, 52–54, 56–58, 63].
Patient experience measurement
A wide variety of tools was used among the 24 studies that reporting using surveys (including three studies that used a combination of survey and qualitative methods). Four studies [25, 36, 39, 45] used tools that had been previously developed specifically for use in custody, including the Measuring the Quality of Prison Life Instrument, [36] but none reported whether or how these tools had been validated in the carceral context. Six studies reported using a survey tool developed for or as part of the study based on the literature, community surveys, or patient complaints [20, 23, 26, 28, 29, 54] and eight used or adapted tools from community settings including for psychiatric outpatient care [27, 30, 37, 51, 55, 57, 58, 62]. Of these, three studies reported piloting the survey with a small number (10 or fewer) of people in custody [20, 37, 55] and one engaging experts regarding surface validity but did not describe the five experts [62]. The remaining six studies did not report how surveys were developed.
Table 1 provides a summary of how measures of patient experience reported in each study align with the Picker Principles of Patient Centred Care. No studies asked any questions regarding the involvement and support of family members and carers. Studies most frequently included questions within the domain of clear information, communication and self-care (n = 17), followed by access to healthcare services (n = 16), and effective treatment by trusted professionals (n = 15), attention to the physical environment (n = 9), patient’s perceptions of emotional empathy and respect from staff (n = 9), patient’s involvement in decision-making (n = 6), and continuity of care (n = 4). Other common measures of patient experience included overall satisfaction with care (n = 19), asking people to compare services in custody to services in the community (n = 7) [11, 25, 35, 40, 41, 46, 50] and how people gained knowledge of how to access healthcare services in custody (n = 3) [11, 39, 41]. Additionally, 24 studies collected demographic information, [11, 20, 21, 24, 36, 40–44, 46–48, 50–62], 20 asked about health history or previous use of healthcare [21, 23, 24, 28, 31, 33, 37, 39, 40, 42, 43, 46–49, 54, 57–62], and 14 collected custody data (such as sentence length) [11, 20, 36, 40, 41, 44, 48, 52, 55, 56, 58–62].
Discussion
Statement of principle findings
In this global scoping review, we identified 44 papers describing 42 studies of patient-reported experiences of healthcare received in correctional facilities. Surveys were used to understand patient experience in 21 studies, 18 studies used qualitative methods (focus groups and/or interviews), and three studies used a combination of survey and qualitative methods.
Interpretation within the context of the wider literature
Though surveys were used in just over half of studies (n = 24, including three studies which used survey and qualitative methods), there was a lack of tools tailored to, or validated in, correctional facilities. Surveys designed for other settings may result in inaccurate or incomplete measures of patient experience by overlooking elements of the carceral environment which shape healthcare services. For example, correctional officers are directly responsible for security and control, but often participate in providing or facilitating access to healthcare [65]. There is a need for validated patient experience measures within correctional institutions to support benchmarking and quality improvement. Qualitative methods may offer more opportunity to capture complexity, but have other limitations; for example, they traditionally require more time and resources, as well as research expertise to collect and analyse data [66]. Additionally, like studies of qualitative methods in prisons more generally, this review highlighted challenges to qualitative methods of patient experience data collection in correctional facilities including lack of privacy and confidentiality and the involvement of correctional and healthcare staff in recruitment [14].
In this review, questions about clear information, communication, and self-care were explored in 17 studies, but questions about respect (n = 9) and agency or involvement in care (n = 6) were less commonly explored. Qualitative studies have described prevalent negative interpersonal relationships with healthcare staff in which people in custody feeling they are being treated disrespectfully and not being listened to by providers [11, 67, 68]. Some have also found that people in custody expect lower-quality care from healthcare providers in prison than from community providers. These findings highlight how structural stigma (defined as conditions, norms, and policies which constrain resources, opportunities, and wellbeing of people being stigmatized [69]) and the inherent imbalance of power between providers and people in custody may shape experiences of care and health outcomes. This suggests that though it has been limited in published studies to-date, exploring respect and control or autonomy in decision-making may be particularly important to understanding and improving experiences of care in custody. Questions about satisfaction with services, an outcome measure of patient experience [70] were the most common type of question in included studies (n = 19) and 15 studies explored the domain of effective treatment by trusted professionals. However, outcome measures may be complicated to interpret in this setting as satisfaction is influenced by other factors including need, and expectations of care [70]; previous qualitative studies have reported that people in custody may have lower expectations of healthcare in custody compared to services in the community [67].
No studies included a measure of the involvement of support or families in care, despite being recognized as an essential component of high-quality person-centred healthcare [10]. In a US study, nurses reported that institutional policies restrict or prohibit sharing information with families, but that opportunities to engage with families as part of care would improve nursing practice and patient outcomes [71]. Beyond family, there exist supportive relationships between people in custody including informal supports, like friendships, and formal peer support roles [72]. The absence of any recognition of the role of personal support in experiencing healthcare needs or services in custody is a significant limitation in work to assess or improve patient-centred care.
Strengths and limitations
More than half of studies in this review came from three countries (USA, UK, and Australia). The lack of studies from some regions may be partially explained by our use of English-language search terms which may have missed studies in other languages. However, this pattern is not unique to our review, other reviews of studies of patient experience measures in emergency departments [73] for people experiencing homelessness [74] and patient satisfaction with mental health services in prisons [75] also found that most studies came from these three countries, with more than half originating in the USA, suggesting that this concentration could also reflect interest or other factors in the healthcare and/or research environments.
A limitation is that our search and screening process included studies with an explicit reference to understanding patient experiences or satisfaction with healthcare services in custody in the title and/or abstract. This may have missed studies including patient experience measures as a component of other work (e.g. studies seeking to understanding experiences of disease in custody). As noted, we worked with a research librarian to obtain a feasible number of records enriched for relevance. We mitigated this limitation by hand-searching reference lists of included articles for additional relevant studies.
Implications for policy, practice, and research
This review identified opportunities for enhanced practices and in research engaging people in custody in patient experience work, including attention to potential risks and benefits. Researchers have a responsibility to protect the rights and dignity of participants and to avoid doing harm [76, 77]. This review included examples of research in which participant identities and their responses were known to correctional and/or healthcare staff which may have affected people’s confidence and trust in the process, as well as the potential risk of negative impact on participants. A third of studies did not report any considerations related to confidentiality. Additionally, few studies reported on the provision of compensation for people participating in research. Low reporting on compensation has been found in other reviews of health research in carceral settings [4] and may be affected by institutional policy explicitly prohibiting compensation for research participants in some jurisdictions [78]. These gaps highlight opportunities to improve standards for, and reporting of, how people may be affected by participating in studies of patient experience measures in custody. As a minimum, to support transparency, researchers should provide detailed reporting of study protocols for protecting participant confidentiality, as well as identify any institutional policies impacting participant compensation.
The lack of tools measuring patient experiences of healthcare that are specific to, or validated in, carceral contexts has implications for healthcare policy and practice. Tools designed to understand healthcare in community settings may overlook distinct features of the prison environment and as a result data may not reflect the realities of experiences of care. Additionally, tools developed in community may not appropriately consider and address aspects of the collection of patient experience data in correctional institutions—such as lack of privacy, autonomy or power imbalances—which may have implications for the safety and wellbeing of participants and the validity of data collected. Patient experience measures used by studies in this review emphasized communication and information-sharing, while largely overlooking critical dimensions such as autonomy and shared decision-making, areas shaped by the constraints of incarceration. There is a need for tools and processes for measuring patient experience that are designed with the leadership of people with lived experience of incarceration to appropriately reflect and capture experiences of care in custody.
Conclusion
Patient experience is a core measure of healthcare quality. This review highlighted critical gaps and opportunities for validated tools tailored to healthcare in the correctional environment. Addressing these gaps is essential to advancing person-centred, equitable healthcare in prisons, strengthening quality improvement efforts, enhancing accountability, and addressing health inequities faced by people experiencing incarceration.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nundy S , Cooper LA, Mate KS. The quintuple aim for health care improvement: a new imperative to advance health equity. JAMA 2022;327:521–2.35061006 10.1001/jama.2021.25181 · doi ↗ · pubmed ↗
- 2Doyle C , Lennox L, Bell D. A systematic review of evidence on the links between patient experience and clinical safety and effectiveness. BMJ Open 2013;3:e 001570.10.1136/bmjopen-2012-001570 PMC 354924123293244 · doi ↗ · pubmed ↗
- 3Fazel S , Baillargeon J. The health of prisoners. Lancet 2011;377:956–65.21093904 10.1016/S 0140-6736(10)61053-7 · doi ↗ · pubmed ↗
- 4Mc Leod KE , Wong KA, Rajaratnam S et al. Health conditions among women in prisons: a systematic review. Lancet Public Health 2025;10:e 609–24.40516562 10.1016/S 2468-2667(25)00092-1 · doi ↗ · pubmed ↗
- 5Green S , Foran J, Kouyoumdjian FG. Access to primary care in adults in a provincial correctional facility in Ontario. BMC Res Notes 2016;9:131–8.26923923 10.1186/s 13104-016-1935-4PMC 4770553 · doi ↗ · pubmed ↗
- 6Fahmy N , Kouyoumdjian FG, Berkowitz J et al. Access to primary care for persons recently released from prison. Ann Fam Med 2018;16:549–51.30420371 10.1370/afm.2314 PMC 6231934 · doi ↗ · pubmed ↗
- 7Redmond N , Aminawung JA, Morse DS et al. Perceived discrimination based on criminal record in healthcare settings and self-reported health status among formerly incarcerated individuals. J Urban Health 2020;97:105–11.31628588 10.1007/s 11524-019-00382-0PMC 7010870 · doi ↗ · pubmed ↗
- 8Government of Ontario. Excellent Care for All Act. In: SO 2010, c 14. 2010. https://www.ontario.ca/laws/statute/10e 14 (10 February 2026, date last accessed).