Risk factors and mortality rates for children co-infected with HIV and TB in Ethiopia: a systematic review and meta-analysis
Fassikaw kebede Bizuneh, Tsehay Kebede Bizuneh, Biruk Beletew Abate, Atitegeb Abera Kidie, Gataye Tizazu Biwota, Tilahun Gizaw Ayenew

TL;DR
This study finds high mortality rates in Ethiopian children co-infected with HIV and TB, highlighting key risk factors like poor treatment adherence and anemia.
Contribution
The study provides the first pooled mortality rate and identifies specific risk factors for HIV-TB co-infected children in Ethiopia.
Findings
The pooled mortality rate is 11.74% with an incidence of 1.5 deaths per 100 person-years.
Key risk factors include WHO stages III/IV, poor ART adherence, missed IPT, and low hemoglobin levels.
Systematic screening and treatment adherence could reduce premature deaths in co-infected children.
Abstract
This systematic review and meta-analysis aimed to identify risk factors and mortality rates in HIV and TB co-infected children in Ethiopia. An electronic literature search was conducted using multiple databases, including PubMed, Medline, Web of Science, African Journal Online, Google Scholar and university research repositories for gray literature. Weighted inverse variance random-effects meta-regression was employed to calculate pooled mortality rates, utilizing Stata/SE-17 for analysis. The meta-analysis included six eligible studies, encompassing a total of 2025 co-infected children. Among these, 238 deaths were reported over 1670.6 person-years. This made the crude mortality rate 11.74% (95% CI 11.49 to 16.12%) with an incidence of 1.5 deaths (95% CI 1.17 to 1.89) per 100 person-years. Factors including WHO stages III and IV (4.34, 95% CI 2.25 to 8.36), poor antiretroviral therapy…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
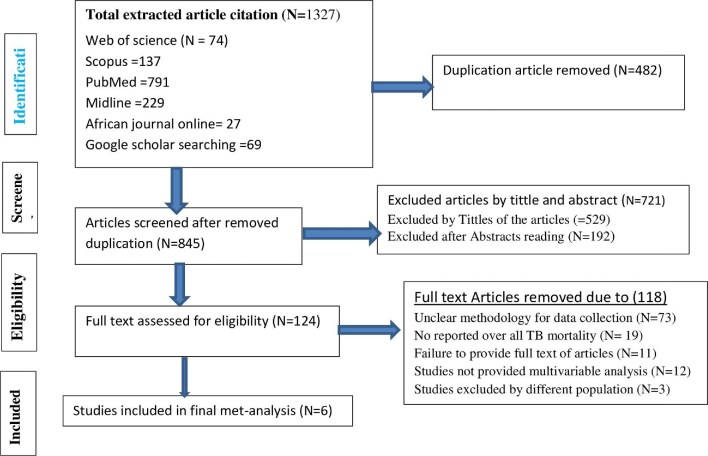 Figure 1
Figure 1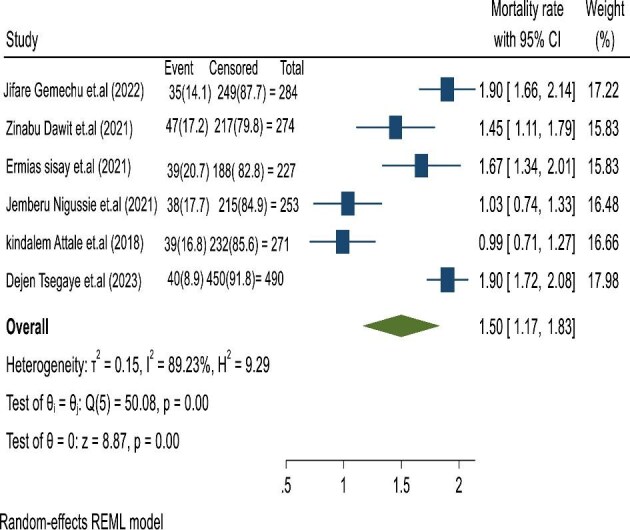 Figure 2
Figure 2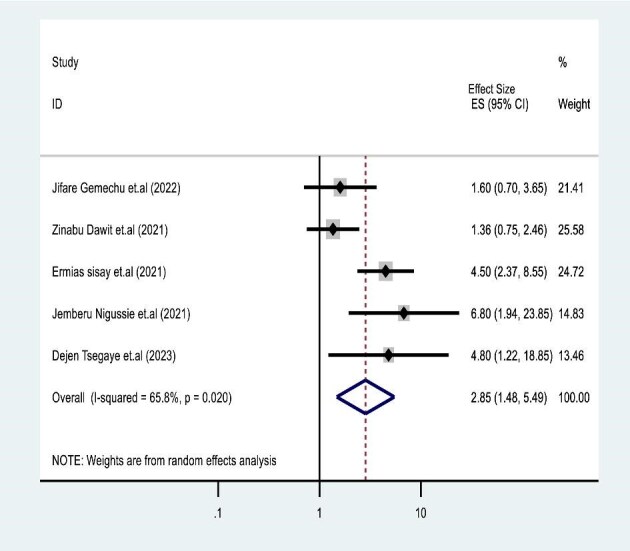 Figure 3
Figure 3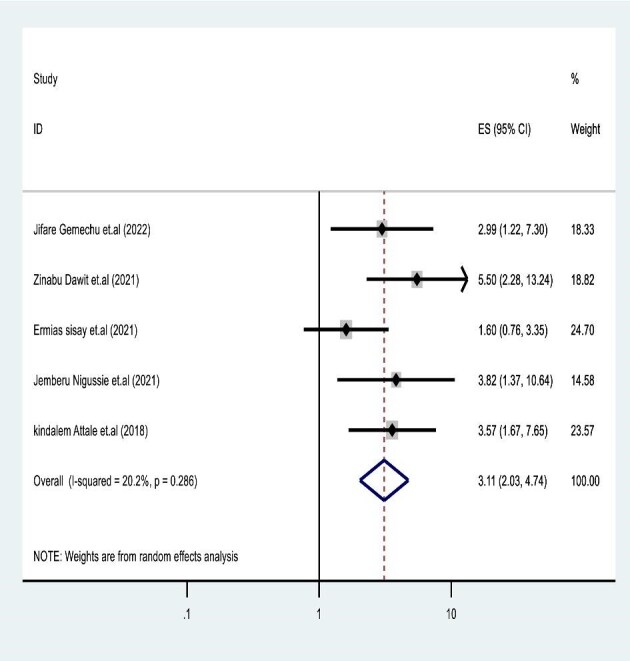 Figure 4
Figure 4| Authors | Year | Region | Design | Population | Setting | Mean age, y | Sample size | Number of deaths | Study period | PPM PPY | Death proportion | Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Jifare Gemechu et al. | 2022 | SNNR | RC | Children | HT | 7.1 (±3.7) | 284 | 35 | 1 January 2009 to 30 December 2019 | 4016.1 | 0.123 239 437 | Low risk |
| 334.6 | ||||||||||||
| Zinabu Dawit et al. | 2021 | SNNR | RC | Children | HT | 8.9 (±3.5) | 274 | 47 | 1 January 2009 to 31 December 2018 | 3331 | 0.171 532 847 | Low risk |
| 277.6 | ||||||||||||
| Ermias Sisay et al. | 2021 | Amhara | RC | Children | HT | 6.70 | 227 | 39 | 1 March 2014 to 12 January 2021 | 2388 | 0.171 806 167 | Low risk |
| 199 | ||||||||||||
| Jemberu Nigussie et al. | 2021 | Tigray | RC | Children | HT | 8 (SD 4–13) | 253 | 38 | 1 January 2008 to 30 December 2018 | 3682 | 0.150 197 628 | Low risk |
| 306.8 | ||||||||||||
| Kindalem Attale et al. | 2018 | Amhara | RC | Children | HT | 6.6 (±3.5) | 271 | 39 | 1 February 2005 to 1 March 2017 | 4412 | 0.143 911 439 | Low risk |
| 367.6 | ||||||||||||
| Dejen Tsegaye et al. | 2023 | Amhara | RC | Children | HT | 9.14 (±3.7) | 498 | 40 | 1 November 2015 to 30 December 2021 | 2222 | 0.080 321 285 | Low risk |
| 185.2 |
| Category | Included studies | IR per 100 PPMO (95% CI) | Heterogeneity (I2, p value) | ||
|---|---|---|---|---|---|
| 1 | Region | Amhara | 3 | 1.53 | 92.32, 0.001 |
| SNNR | 2 | 1.69 | 77.73, 0.03 | ||
| Tigray | 1 | 1.03 | 89.3, 0.001 | ||
| 2 | Follow-up time (y) | ≥10 | 2 | 1.45 | 95.23, 0.001 |
| <10 | 4 | 1.52 | 86.2, 0.001 | ||
| 3 | Sample size | ≤260 | 2 | 1.35 | 87.2, 0.01 |
| >260 | 4 | 1.57 | 91.4, 0.001 |
| Categorical variable | Included studies | HR | 95% CI | Pooled HR | I2 | p | |
|---|---|---|---|---|---|---|---|
| WHO | Jifare Gemechu et al. | 1.6 | 0.71 | 3.7 | 2.85 (1.48 to 5.49) | 65.4% | 0.02 |
| Zinabu Dawit et al. | 1.36 | 0.74 | 2.43 | ||||
| Ermias Sisay et al. | 4.5 | 2.39 | 8.63 | ||||
| Jemberu Nigussie et al. | 6.8 | 2.01 | 24.6 | ||||
| Dejen Tsegaye et al. | 4.8 | 1.2 | 18.56 | ||||
| ART adherence | Jifare Gemechu et al. | 1.25 | 1.25 | 7.46 | 3.11 (2.04 to 4.11) | 20.2% | 0.20 |
| Zinabu Dawit et al. | 2.19 | 2.19 | 12.7 | ||||
| Ermias Sisay et al. | 0.799 | 0.799 | 3.5 | ||||
| Jemberu Nigussie et al. | 1.39 | 1.39 | 10.79 | ||||
| Kindalem Attale et al. | 1.7 | 1.7 | 7.8 | ||||
| CPT | Zinabu Dawit et al. | 1.5 | 1.25 | 7.46 | 2.39 (0.84 to7.2) | 0.01 | 0.09 |
| Ermias Sisay et al. | 3.8 | 2.19 | 12.7 | ||||
| Jemberu Nigussie et al. | 1.79 | 0.799 | 3.5 | ||||
| Dejen Tsegaye et al. | 4.1 | 1.39 | 10.79 | ||||
| IPT | Jifare Gemechu et al. | 0.55 | 0.29 | 2.6 | 3.07 (1.52 to 6.23) | 76.1 | 0.01 |
| Zinabu Dawit et al. | 7.27 | 5.5 | 13.89 | ||||
| Ermias Sisay et al. | 2 | 0.78 | 5.6 | ||||
| Jemberu Nigussie et al. | 3.7 | 1.5 | 10.5 | ||||
| Kindalem Attale et al. | 3.87 | 1.6 | 9.2 | ||||
| Dejen Tsegaye et al. | 4.8 | 1.6 | 10.3 | ||||
| Level of hemoglobin | Jifare Gemechu et al. | 3.6 | 1.39 | 9.56 | 2.84 (2.02 to 3.99) | 0.1 | 0.7 |
| Zinabu Dawit et al. | 2.69 | 1.52 | 5.64 | ||||
| Ermias Sisay et al. | 7.6 | 0.53 | 13.73 | ||||
| Jemberu Nigussie et al. | 3.75 | 1.5 | 13.6 | ||||
| Kindalem Attale et al. | 2.6 | 1.24 | 5.34 | ||||
| Dejen Tsegaye et al. | 2.2 | 1.2 | 4.6 | ||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV/AIDS Impact and Responses · Tuberculosis Research and Epidemiology · Global Maternal and Child Health
Introduction
HIV and TB are the two main deadly pandemics from infectious diseases.^1,2^ There is a strong synergy between HIV infection and TB. People living with HIV (PLHIV) are at a high risk of morbidity and mortality from TB, as HIV infection is the primary risk factor for the incidence of active TB.^3^ Both diseases interact in a complex and synergistic manner. HIV infection weakens the immune system and increases susceptibility to active TB incidence in the lung.^4^ TB infection also accelerates the progression of advanced HIV infection by initiating an immune response that can boost HIV replication and viral load.^5,6^ The immune activation caused by TB leads to inflammation and immune system dysfunction, which can affect the efficacy of antiretroviral drugs.^7^ According to the 2023 Global TB Report, about 1.3 million (12% of 10.6 million) new TB cases were children aged 0–14 y.^2^ Of those, 14.3% were co-infected with HIV and TB.^2^ About 214 000 patients in 2020, and 187 000 in 2021, died during TB and HIV co-infections.^2,8^ Despite advances in diagnostics and the widespread availability of antibiotics, TB infection remains responsible for 40% of deaths, 18% of hospitalizations and 25% of case fatalities for PLHIV.^9^
Previous study findings suggested that TB and HIV co-infection mortality varied across developed and developing countries.^10,11^ One systematic review and meta-analysis (SRM) reported that the mortality rate attributable to TB was as high as 24.9% in adults and 30.1% in children.^12^ A cluster randomized trial study in South Africa indicated that the mortality rate among patients co-infected with TB and HIV was 10.1 per 100 person-years.^13^ A study in Malaysia reported that the mortality rate for TB patients co-infected with HIV was 23.3%.^14^ In sub-Saharan Africa (SSA), the mortality rate for dual TB and HIV co-infection ranges from 10% to 29.8% and varies within each country.^9^ Evidence from Tanzania suggested that the incidence of mortality among patients with TB and HIV was 57.8 per 1000 person-years.^15^ By contrast, the reported death rate during TB and HIV co-infection in Uganda was lower (6.38%) after antiretroviral therapy (ART) was initiated.^16^ In Ethiopia, the true burden of childhood TB is often underestimated.^7,17^ The regional healthcare disparities and sociodemographic differences among caregivers increase the number of premature deaths in children during co-infections.^6^
Several predicting factors^3,17–21^ have been identified as contributors to mortality during co-infection for children living with HIV/AIDS: missed isoniazid preventive therapy (IPT),^22,23^ poor ART adherence^11,14^ and immune reconstitution inflammatory syndrome^9,24^ were predictors for premature death. Recent findings suggest that a CD4 count of ≤200 cells/mL and a viral load of ≥400 copies/mL during TB co-infection in children with HIV are proxy indicators for premature death.^14,25,26^ In Ethiopia, efforts have been made to reduce morbidity and mortality during co-infections through community-based case training, provision of free ART and anti-TB drugs and free provision of IPT, resulting in significant progress being recorded.^17,27^ However, in Ethiopia, there is a lack of aggregated mortality data of co-infected children. Therefore, an SRM was conducted for estimating the incidence rate and predictors of mortality among ART-taking TB and HIV co-infected children in Ethiopia.
Methods
Reporting and protocol registration
This SRM was conducted following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Supplementary Data 1)^28^ and was prospectively registered on Prospero with the registration number CRD42024502038.
Data-searching strategy
Primary studies in English and other languages were retrieved from internationally reputable electronic databases in Ethiopia. PubMed, Medline, Web of Science, African Journal Online, Google Scholar and university research repositories were searched to find pertinent articles from 16 October to 21 November 2024. We employed free text, keywords and Medical Subject Headings (MeSH) for searching eligible studies from electronic databases. The search terms included keywords, free texts and MeSH terms used to access the eligible studies as follows: ‘Incidence’, ‘Incidence’ [Mesh], ‘incidence rate’, ‘incidence density’, magnitude, ‘Survival’ [Mesh], ‘Mortality’ [Mesh], predictors, ‘TB-HIV co-infection’, ‘Child’ [Mesh], ‘pediatrics’ [Mesh], ‘children’ [Mesh], ‘Adolescent’ [Mesh] and Ethiopia.
The search terms and keywords were combined using ‘AND’ and ‘OR’ Boolean operators to yield sufficient and appropriate search results (Supplementary Data 2). This SMR followed the PICO—Population, Intervention, Comparison and Outcomes—framework to evaluate the eligibility of published articles for developing evidence-based clinical research. This is outlined as Population (P): children co-infected with TB and HIV in Ethiopia; Intervention (I): HIV-infected children who had undergone ART; Comparison (C): children co-infected with TB and HIV; and Outcome (O): the primary outcome of interest was TB-associated death while under care.
Eligibility: criteria of articles
Inclusion and exclusion criteria
This review encompasses all published observational studies, regardless of language and publication date, conducted in Ethiopia and focusing on co-infected children aged ≤15 y who were considered eligible. However, papers that did not report the outcomes of interest, as well as those lacking the full text, were excluded from the analysis.
Outcome ascertainments
The dependent variable is death during TB and HIV co-infected children. This was calculated by extracting mortality proportions from each eligible study and dividing by the person per months of risk observation using Pro-Command in STATA version 17 (StataCorp LLC, Texas, USA).
Article quality assessment and appraisal
The methodological quality of the retained publications was assessed by two authors (FKB and GTB) using the Joanna Briggs Institute (JBI) checklist for cohort studies (Supplementary Data 3).^29^ The tool has the following criteria for each study: appropriate statistical analysis, strategies to address incomplete follow-up, sufficient follow-up time, valid and reliable measurement of outcomes, participants free of the outcome at the beginning of the study, identification of confounding factors and strategies to reduce missing dates. Questions that meet these criteria are labeled as ‘1’, while those that do not meet the criteria are labeled as ‘0’. During labeling of the eligible studies, scoring ≥50% on the quality assessment tools was considered to be a low risk/high quality score. Studies scoring <49% on the quality assessment checklist were categorized as high risk/low quality based on the average positive score of the JBI checklist.
Data extraction and screening process
Two authors (FKB and GTB) screened the article titles and abstracts against the inclusion and exclusion criteria. Four reviewers (FKB, AAK, BBA and TGA), according to predetermined exclusion and inclusion criteria from 16 October to 21 November 2024, then extracted relevant data. Any disagreements were resolved through discussion through involvement of a third author (TKB) to address uncertainties. Two authors (FKB and GTB) were assigned to remove unrelated studies based on their titles and abstracts. Discrepancies between the authors were settled by discussion. Author group, publication year, study region, study design, study setting, sample size, outcome, response rate, incidence rate of mortality and predictors' effect size were extracted to a Microsoft Excel spreadsheet before analysis was started.
Handling of missing dates
During meta-analysis reports, missing data were addressed using the complete case analysis method. Given that the missing values were <5%, there was no indication to carry out single or multiple imputations.^30^
Software and statistical analysis
Using EndNote version 8.1, all potentially suitable published article citations were exported and duplications were removed during the screening process. Microsoft Excel (Meta-XL) version 5.3 was employed to extract relevant data from included studies before they were exported to STATA version 17 statistical software for further analysis.^31^ The pooled mortality rate among children co-infected with TB and HIV and its predictors was estimated using weighted inverse variance random-effects meta-regression combined with DerSimonian–Laird model weight.^32,33^ Descriptive statistical results are presented in tables and funnel plots.
Publication of bias and sensitivity analysis
The presence of heterogeneity between included studies was evaluated using the Cochrane Q-test and I^2^ statistics. Publication bias was checked through graphical inspection (funnel plot) and quantitatively using Egger's weighted regression test.^32,33^ In addition, we performed a leave-one-out sensitivity analysis to confirm a study with a biased direction of pooled estimates of Beggs and Eggers tests.^30^ Subgroup analysis was performed to adjust random variation in the presence of significant heterogeneity between primary studies.
Results
Screening of included studies
Our search using the prespecified strategies resulted in 1327 published articles. During the initial article screening process, 482 duplicates were removed. After thoroughly reviewing the titles and abstracts of 845 articles, we excluded 721 articles that did not meet the criteria. During the full-text review, we evaluated 124 publications, of which 118 articles were excluded for various reasons, including unclear methodology (N=73), insufficient data collection and reporting format (N=19), inaccessibility of full texts (N=11), absence of multivariable predictors (N=12) and differences in the population (N=3) (Figure 1).
Article selection flowchart by PRISMA for children co-infected with TB and HIV in Ethiopia.
Descriptive reports of included studies
In this SRM, six primary studies^34–39^ were included to estimate the pooled incidence of mortality rate among children co-infected with TB and HIV. The included articles were from three regions: there were three from Amhara,^34,35,39^ two from the Southern Nation Nationalities Region (SNNR)^36,37^ and one from Tigray.^38^ The study-specific sample sizes ranged from 227 in Debre Tabor^35^ to 498 in Woldia^39^ hospitals, both located in the Amhara region. On the other hand, the estimated effect sizes of mortality from the individual studies ranged from 47 (17.2%)^36^ to 35 (12.3%)^37^ multi-sites of the SNNR. All of the studies employed a retrospective cohort and were conducted in a hospital set-up. The follow-up period for the included studies ranged from 30 June 2021 to 30 September 2023.^34–39^ Regarding article quality, all the studies were of high quality, scoring ≥80%.^34–39^ The mean age of participants ranged from 6.6 (±3.5)^34^ to 9.14 (±3.7) y^39^ (Table 1).
Pooled incidence density rate of TB and HIV co-infected mortality
This study comprised 2025 TB and HIV co-infected children aged ≤15 y. During mortality screening, 238 deaths were reported within 1670.6 persons per year of risk observation.
We found a crude mortality rate of 11.74% (95% CI 11.49 to 16.12%) and an incidence of 1.5 (95% CI 1.17 to 1.89) cases per 100 person-years (Figure 2).
Pooled incidence of mortality rate for children co-infected with TB and HIV in Ethiopia.
Handling heterogeneity and subgroup analysis
To address the observed heterogeneity among studies, subgroup and sensitivity analyses were conducted based on follow-up time, study region, sample size and study setting. The mortality rate for children during co-infection was higher in the SNNR (1.69%) compared with the Tigray region (1.03%). Subgroup analysis concerning sample size and mortality during co-infection was elevated for pooled studies with sample sizes of ≥260 participants (1.57%) compared with sample sizes of <260 (1.35%). Interestingly, consistent mortality rates were found across different follow-up times in pooled studies with rates of 1.45% for ≤120 mo and 1.52% for >120 mo (Table 2).
Forest plots for association with WHO clinical stages III and IV and mortality in co-infected children.
Predictors for mortality during TB and HIV co-infected mortality
To identify risk factors for mortality during TB co-infection in HIV-infected children, significant categorical risk factors were pooled from each study. After employing weighted inverse variance random-effects meta-regression, four statistically significant variables were identified, consisting of advanced WHO clinical stages III and IV, poor/fair ART adherence, missed IPT and low levels of hemoglobin (Hgb), as presented in Table 3.
Effects of WHO stages III and IV on TB and HIV co-infected mortality
Five studies^35–39^ were used to test the association of advanced WHO stages III and IV with TB co-infection mortality of HIV-infected 1527 participant children. In the final review of this SRM, TB co-infection and advanced WHO stages III and IV were associated with a fourfold increased mortality risk (pooled HR 4.34; 95% CI 2.25 to 8.36) with significant heterogeneity (I²=95.50%, p=0.001) (Figure 3).
Effect of poor ART adherence on TB and HIV co-infected mortality
A total of five individual studies^34–38^ were used to assess the association between poor ART adherence and mortality in 1487 children co-infected with TB and HIV. The report indicated a strong correlation of premature deaths in children with poor or fair ART adherence during co-infection. The final random-effects model analysis revealed that children with poor and fair ART adherence had an HR of 3.11 (95% CI 2.04 to 4.15) for mortality compared with those with good adherence (Figure 4).
Forest plot showing poor ART adherence and mortality incidence in children co-infected with TB and HIV. ART: antiretroviral therapy.
Effects of missed IPT on TB and HIV co-infected mortality
Six studies^34–39^ were used to investigate the association between missed IPT and deaths due to TB incidence following ART initiation. All the included studies reported a significant risk of TB-associated death and missed IPT after ART initiation among children. Random-effects model analysis indicated that patients co-infected with TB and HIV who had missed IPT experienced a threefold hazard of death (pooled HR=3.07; 95% CI 1.52 to 6.23) with significant heterogeneity (I^2^=96.6%).
Effects of low Hgb level on TB and HIV co-infected mortality
Low Hgb levels and TB-associated mortality among HIV-infected children were assessed using a pooled risk ratio from six studies.^34–39^ The final SRM regression finding reported that children with Hgb≤10 mg/dl had a threefold higher risk of death during TB co-infection compared with Hgb>10 mg/dl (pooled HR=2.84; 95% CI 2.02 to 3.99).
Impacts of missed cotrimoxazole preventive therapy on TB and HIV co-infected mortality
The association between missed cotrimoxazole preventive therapy (CPT) and TB and HIV co-infected mortality was examined using 1229 participants from five studies.^34–36,38,39^ However, the final meta-regression report indicated that missed CPT had no significant correlation with TB and HIV co-infected mortality of children.
Small study effects and publication bias assessment
We tested for publication bias using graphical and statistical tests. In graphical assessments, asymmetric distributions of articles were observed in the funnel plot upon visual inspection. In addition, we performed quantitative Egger regression to investigate small study effects: the statistical test revealed that there was no significant publication bias, with an intercept of slope at 1.081 and p=0.074 with a bias co-efficient of -5.073 at p=0.214.
Sensitivity analysis
We also conducted a leave-one-out sensitivity analysis to investigate the influence of individual studies, and the results indicated that no single study significantly influenced the overall estimation rate (incidence density rate=1.41%).
Discussion
The rate was found to be 1.5 (95% CI 1.17 to 1.89) cases per 100 person-years among TB and HIV co-infected children in Ethiopia. This description is higher than those previously reported in Congo^40^ and China.^11^ Possible reasons for this could be disparities in healthcare services, as well as differences in socioeconomic status, study populations and methodologies.^41^ However, the finding was lower than those reported by a systematic review conducted in low- and middle-income countries (10.8%^12^) and in Ethiopia (3.54%^17^). These discrepancies may stem from sociodemographic factors, differing study periods and cultural disparities. Another factor could be substandard healthcare and TB treatment guidelines during co-infection treatment. Conversely, the estimated mortality rate was consistent with those reported in Finland^42^ and in SSA.^10^ This may be linked to the positive effects of early initiation of ART in Ethiopia and some SSA countries (e.g. Kenya, Uganda and Tanzania) for children aged ≤15 y resulting in better health outcomes.^21^
The subgroup analysis by region revealed that the highest mortality rate was observed in studies from the SNNR (1.69%) compared with those from Amhara (1.53%) and Tigray (1.03%). This variance may be due to the inclusion of a limited number of studies for rate estimation and differences in sample sizes. On the other hand, fragmentation of the SNNR into three subregions during the COVID-19 pandemic led to reduced healthcare provision in each area, affecting the quality of health services for PLHIV.^43^
Unlike previous study findings^17,21^ in Ethiopia, TB-associated mortality rates for HIV co-infected children remained consistent, irrespective of follow-up duration (≤10 y: 1.45%; >10 y: 1.52%). This might be due to the rapid disease progression, co-infection complications and inconsistent healthcare access across each region.^17,18^ It might also be directly linked to a prolonged conflict spanning nearly 4 y in Ethiopia between the Tigray, Afar and Amhara regions that has led to 94% of medical equipment being stolen and destruction in each region, with 92% of HIV care services being severely disrupted, including care provision for children.^25^ The disruption to healthcare services has impacted care for PLHIV and increased co-infection mortality in each region.
The findings of this review indicate that children co-infected with TB and HIV in advanced WHO clinical stages III and IV experienced fourfold hazards of death compared with other groups. This is consistent with previous findings in Wolaita Sodo,^44^ Gondar,^17^ Tanzania,^45,46^ South Africa^9^ and SSA,^10^ as well as a global systemic review.^12^ As HIV progresses to later clinical stages, patients become more vulnerable to deadly opportunistic infections such as TB due to compromised immunity, leading to reduced survival rates in co-infected individuals.^4^ On the other hand, evidence suggests that in children with HIV at advanced clinical stages (III and IV), there is a sharp decline in cellular immunity and rapid viral replication, indirectly indicating a significant decrease in CD4 counts below the threshold, which serves as a proxy indicator for premature death during co-infection.^4,7^
Consistent with previous SMR findings^4,6,47^ and results from Kazakhstan,^23^ co-infected children who missed IPT experienced a significant risk of mortality. In this review, TB and HIV co-infected children who missed IPT had a threefold increased risk of death compared with those who received IPT. A primary study^41^ and a meta-analysis^47^ in Ethiopia reported that IPT can reduce the risk of latent TB reactivation and prevent 90% of TB-associated deaths when administered concurrently with ART. However, drug complexity, side effects and the forgetfulness of caregivers reduced the completion rates of IPT and increased susceptibility to TB infection among children.
The hazard of death for children with TB co-infected with HIV with Hgb≤10 g/dl were increased threefold compared with those groups with Hgb>0 mg/dl. This is congruent with previous reports in South Africa,^48^ Tanzania,^46^ Malaysia^14^ and SSA.^49^ Anemia during TB and HIV infection impairs the immune response, hastening disease progression and leading to treatment failure, loss to follow-up and death.^50^ It also increases viral load, decreases CD4 count, progresses HIV to advanced stages and contributes to overall mortality.
The current review indicates that patients with fair/poor ART adherence experienced threefold the hazard for death than those with good ART adherence among TB and HIV co-infected patients (pooled HR: 3.11). Studies in Cameroon and Ethiopia support this report.^4,46^ This might be related to caregivers lack of commitment, low education levels and forgetfulness about daily ART drugs, which may lead to poor outcomes; this and non-adherence results in drug resistance, treatment failure and increased healthcare costs.
In contrast to previous SRM findings,^14,48,51,52^ particularly in resource-limited settings such as Nigeria and Malaysia,^14^ reported findings in the Caribbean, Central and South America and West Africa^53^ have shown a significant association between declining CD4 counts (≤200 cells/mL) and mortality in TB and HIV co-infection. However, in the current study, CD4 counts below the threshold and treatment failure did not show an association with the mortality of co-infected children. This discrepancy may be attributed to methodological variations, including a limited number of studies with sample size constraints.
Strengths and limitations
Sensitivity and subgroup analyses were conducted to explore heterogeneity among the eligible studies. In addition to English language publications, articles in other languages were considered for inclusion. Despite these strengths, this review has its limitations, such as the exclusion of qualitative studies and limited access to primary studies from all regions of Ethiopia. Furthermore, some included articles had small sample sizes that could have impacted the accuracy of the pooled estimates.
Conclusions
The review shows high mortality rates among individuals co-infected with TB and HIV. The contributing factors included poor ART adherence, advanced WHO staging, no IPT and anemia. Scaling up IPT, ART counseling and early treatment for anemia are key. Collaborative efforts and close patient follow-ups are crucial to reduce mortality and improve survival rates.
Supplementary Material
ihaf085_Supplemental_Files
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kegne TW, Anteneh ZA, Bayeh TL, et al. Survival rate and predictors of mortality among TB-HIV co-infected patients during tuberculosis treatment at public health facilities in Bahir Dar City, northwest Ethiopia. Infect Drug Resist. 2024;17:1385–95.38618582 10.2147/IDR.S 446020 PMC 11015844 · doi ↗ · pubmed ↗
- 2WHO . Global Tuberculosis Report. 2023. Available at: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2023 [accessed September 2024].
- 3Bizuneh FK, Bizuneh TK, Masresha SA, et al. Tuberculosis-associated mortality and risk factors for HIV-infected population in Ethiopia: a systematic review and meta-analysis. Front Public Health. 2024;12:1386113.39104893 10.3389/fpubh.2024.1386113 PMC 11298472 · doi ↗ · pubmed ↗
- 4Kebede Bizuneh F, Tsegaye D, Negese Gemeda B, et al. Proportion of active tuberculosis among HIV-infected children after antiretroviral therapy in Ethiopia: A systematic review and meta-analysis. P Lo S Glob Public Health. 2024;4(8):e 0003528.39093892 10.1371/journal.pgph.0003528 PMC 11296650 · doi ↗ · pubmed ↗
- 5Gesesew H, Tsehayneh B, Massa D, et al. Predictors of mortality in a cohort of tuberculosis/HIV co-infected patients in Southwest Ethiopia. Infect Dis Poverty. 2016;5(1)109.27915999 10.1186/s 40249-016-0202-1PMC 5137204 · doi ↗ · pubmed ↗
- 6Girma D, Abita Z, Shifera N, et al. Incidence rate of tuberculosis among HIV infected children in Ethiopia: systematic review and meta-analysis. BMC Pediatric. 2024;24(1):363.10.1186/s 12887-024-04819-7PMC 1112728538790006 · doi ↗ · pubmed ↗
- 7GBD 2021 Causes of death . Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2100–32.38582094 10.1016/S 0140-6736(24)00367-2PMC 11126520 · doi ↗ · pubmed ↗
- 8Uppal A, Rahman S, Campbell JR, et al. Economic and modeling evidence for tuberculosis preventive therapy among people living with HIV: A systematic review and meta-analysis. P Lo S Med. 2021;18(9):e 1003712.34520463 10.1371/journal.pmed.1003712 PMC 8439468 · doi ↗ · pubmed ↗