Gut Microbiota Predicts the Risk of Future COVID-19 Hospitalization and Mortality: Insights From the Population-Based HELIUS Study
Robert F J Kullberg, Brent Appelman, Henrike Galenkamp, Maria Prins, Bert-Jan van den Born, Max Nieuwdorp, Bastiaan W Haak, W Joost Wiersinga

TL;DR
This study shows that gut bacteria, especially those producing butyrate, can predict the risk of severe COVID-19 outcomes like hospitalization or death.
Contribution
The study demonstrates that gut microbiota composition before infection can influence future severe COVID-19 risk.
Findings
Baseline gut microbiota composition is associated with future severe COVID-19 risk.
Higher levels of butyrate-producing bacteria are linked to lower risk of severe outcomes.
Microbiota alterations precede severe disease and may serve as a prevention target.
Abstract
Gut microbiota are disrupted in patients hospitalized for COVID-19, with a loss of anaerobic bacteria-producing butyrate. Yet, these disruptions could either be a consequence of the infection itself or increase susceptibility from the outset. Here, we investigated whether gut microbiota influence the risk of future COVID-19 hospitalization and mortality. In 5084 participants of a population-based cohort, gut microbiota composition was associated with the risk of future severe COVID-19. Specifically, increased abundances of butyrate-producing bacteria were associated with a lower risk of severe COVID-19. Together, gut microbiota alterations precede severe COVID-19 and may represent a novel target for prevention. In this large population-based cohort, we found that baseline gut microbiota, especially low levels of butyrate producers, are coupled with a higher risk of hospitalization or…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
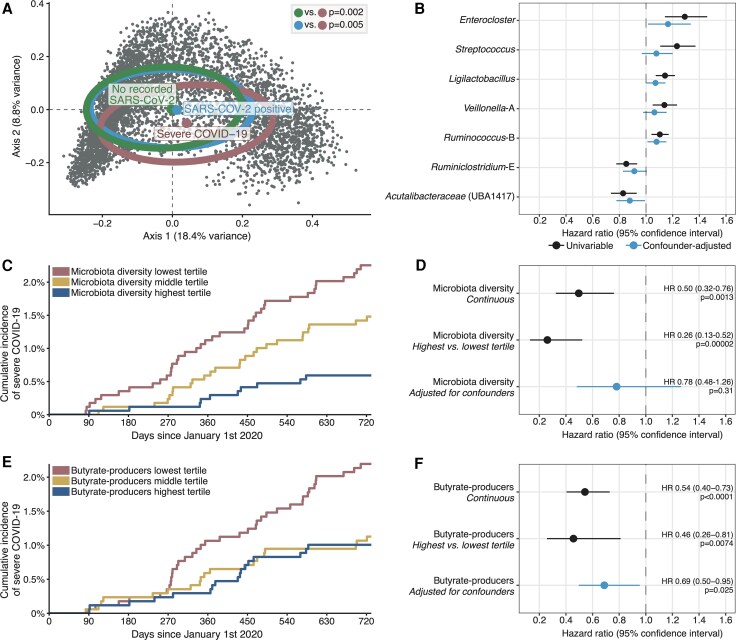 Figure 1
Figure 1| Median (IQR) or No. (%) | |||
|---|---|---|---|
| Severe COVID-19 (n = 73) | No Severe COVID-19 (n = 5011) |
| |
| Age, y | 57 (48–62) | 52 (43–59) | <.001 |
| Female sex | 28 (38.4) | 2618 (52.2) | .025 |
| Ethnicity | <.001 | ||
| Dutch | 2 (2.7) | 1503 (30.0) | |
| African Surinamese | 21 (28.8) | 1190 (23.7) | |
| South-Asian Surinamese | 27 (37.0) | 792 (15.8) | |
| Turkish | 11 (15.1) | 437 (8.7) | |
| Moroccan | 9 (12.3) | 587 (11.7) | |
| Ghanaian and other | 3 (4.1) | 502 (10.0) | |
| Body mass index | 30.5 (27.8–33.9) | 26.5 (23.8–30.0) | <.001 |
| Current or former smoker | 41 (56.9) | 2579 (52.2) | .49 |
| Comorbidities | |||
| Hypertension | 35 (49.3) | 1274 (25.7) | <.001 |
| Diabetes | 22 (30.6) | 526 (10.6) | <.001 |
| Cardiovascular disease | 16 (22.5) | 488 (9.9) | .001 |
| Pulmonary disease | 19 (26.4) | 505 (10.2) | <.001 |
| Gastrointestinal disease | 9 (12.5) | 385 (7.8) | .21 |
| Cancer | 1 (1.4) | 128 (2.6) | .79 |
| Registered positive SARS-CoV-2 PCR result | 73 (100) | 861 (17.2) | |
- —Amsterdam University Medical Centers10.13039/100019573
- —Niels Stensen Fellowship
- —Dutch Heart Foundation
- —Netherlands Organization for Health Research and Development10.13039/501100001826
- —European Union FP-7
- —European Fund for the Integration of Non-EU Immigrants
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGut microbiota and health · Clostridium difficile and Clostridium perfringens research · Immune responses and vaccinations
Gut microbiota are extensively disrupted in patients hospitalized for COVID-19, with a loss of anaerobic bacteria producing the short-chain fatty acid butyrate [1, 2]. While traditionally viewed as a consequence of medical interventions and acute illness (eg, antibiotics, reduced food intake), an alternative explanation has emerged: gut microbiome disruptions may precede infection onset, exacerbate severity, and increase the likelihood of hospitalization. This paradigm shift is supported by preclinical studies demonstrating that obligate anaerobic bacteria strengthen host defenses against viral pneumonia, including COVID-19, through the production of the immunomodulatory metabolite butyrate [3–5]. In murine models of pneumonia, butyrate enhances the functioning of CD8+ T cells and alveolar macrophages while limiting hyperinflammation and tissue damage [4–6]. Yet, whether these preclinical findings translate to humans is unclear. We recently showed that high intestinal levels of butyrate-producing bacteria were associated with a reduced risk of future hospitalizations for infections of any type [7]. However, this relationship with all-cause infections may not explicitly apply to viral pneumonia, including SARS-CoV-2. Here, we investigated whether gut microbiota, specifically low amounts of butyrate-producing bacteria, precede severe COVID-19 and influence the risk of hospitalization in humans.
METHODS
We used data from the large-scale, population-based Healthy Life in an Urban Setting (HELIUS) study. Details on study design have been published [7]. Briefly, HELIUS is a multiethnic, population-based, prospective cohort study conducted in Amsterdam, the Netherlands. Adults (aged 18–70 years at inclusion) were randomly sampled from the municipality register, stratified by ethnicity, and invited to participate. Participants completed questionnaires, underwent a physical examination, and provided fecal samples at inclusion (May 2011–November 2015). Fecal microbiota were profiled by 16S rRNA gene sequencing (V4 region) and subsequently preprocessed in Deblur (version 1.1.1) and Greengenes2 (release 2022.10), as previously described [7]. Ethical approval was obtained from the Academic Medical Center Ethical Review Board (protocol 10/100; amendment 10/100#10.17.1729; NL32251.018.10), and all participants provided written informed consent.
Our primary outcome was severe COVID-19, defined as hospitalization or mortality. Outcome data were retrieved from national registries (Statistics Netherlands) [7]. We focused on events during the first 2 years of the pandemic (between 1 January 2020 and 31 December 2021), given the widespread vaccination uptake afterward and to limit the effects of differing pathogenicity of circulating SARS-CoV-2 variants (eg, patients hospitalized with Omicron are older, of different ethnic backgrounds, and have more comorbidities) [8].
We assessed associations between our outcome and 3 predefined gut microbiota features: community composition (β-diversity and individual genera), community diversity, and the cumulative relative abundance of key butyrate-producing bacteria (given the loss of butyrate producers in hospitalized patients with COVID-19 and the protective effects of butyrate in animal experiments) [1, 2, 4–6]. Butyrate-producing taxa were categorized as previously described, which accurately predicts fecal butyrate concentrations (Pearson r = 0.76) [7, 9, 10]. Time-to-event analyses with Cox proportional hazards models were used to examine the relationship between the primary outcome and individual genera (restricted to genera with a minimum abundance of 0.005% in at least 10% of participants), microbiota diversity, or butyrate-producing bacteria. Relative abundances were centered log ratio transformed to correct for the inherent compositional nature of microbiome data. To adjust for potential confounders, multivariable models included baseline age, sex, ethnicity, body mass index, time between baseline and 1 January 2020, and comorbidities (hypertension, diabetes, and cancer, as well as cardiovascular, pulmonary, and gastrointestinal disease). Additionally, we used nationwide SARS-CoV-2 testing data to compare the microbiota of participants with severe COVID-19 against those with mild to moderate SARS-CoV-2 infection (ie, positive polymerase chain reaction result not resulting in hospitalization or mortality). The χ^2^ test was used to compare categorical variables. Continuous variables were compared with Wilcoxon rank sum tests. Two-tailed level of significance was set at P < .05.
RESULTS
In total, 5084 HELIUS participants had gut microbiota sequenced, consented for linkage with national registries, and were alive at 1 January 2020. During follow-up, 73 participants reached the primary outcome (COVID-19–related hospitalization or mortality). Participant characteristics are depicted in Table 1. Characteristics subset by several clinical and microbiota features are provided in the supplementary material.
The overall gut microbiota composition of participants who reached the primary outcome differed from participants without severe COVID-19 (Figure 1A). Higher relative abundances of the anaerobic gut symbiont Enterocloster were, among other genera, associated with an increased risk of future severe COVID-19, whereas members of the butyrate-producing Oscillospirales order were associated with a lower risk (Figure 1B). Higher gut microbiota diversity was associated with a reduced risk of severe COVID-19 (Figure 1C). However, this was not significant when adjusted for potential confounders (age, sex, ethnicity, body mass index, time between inclusion and 1 January 2020, and comorbidities; Figure 1D). In line with the protective effects in mice [4, 5], increased relative abundances of butyrate-producing bacteria were associated with a lower risk of severe COVID-19 when analyzed as a continuous variable and when comparing the lowest and highest tertiles (Figure 1E and 1F). The association between butyrate-producing bacteria and a reduced risk of severe COVID-19 remained when corrected for potential confounders in the multivariable model (Figure 1F). Associations between characteristics of our participants and the abundance of butyrate-producing bacteria have been described [7]. Three sensitivity analyses yielded similar results. First, we added antibiotic exposure in the 3 months prior to sample collection as a potential confounder to our multivariable model. Second, we focused solely on events in 2020. Third, participants were censored at the date of their first SARS-CoV-2 vaccination.
Gut microbiota are associated with the risk of future severe COVID-19. A, Baseline gut microbiota composition differed between participants with future severe COVID-19 (hospitalization or mortality, n = 73) and participants without severe COVID-19 during follow-up (those with a registered positive PCR result for SARS-CoV-2, n = 861; those with no recorded positive SARS-CoV-2 PCR, n = 4150). Permutational multivariate analysis of variance with Bray-Curtis dissimilarities at the species level were used to assess differences between groups. Smaller points represent individual participants. Larger points depict the group centers and ellipses the 50% confidence interval. B, Higher relative abundances of Enterocloster and several facultative anaerobic bacteria (eg, Streptococcus, Limosilactobacillus, Ligilactobacillus) were associated with an increased risk of severe COVID-19, whereas several members of the Oscillospirales order (eg, Ruminiclostridium-E, Acutalibacteraceae UBA1417) were associated with a lower risk. Individual bacterial genera associated with the primary outcome were identified through Cox proportional hazards models. Significant univariable associations are shown (Benjamini-Hochberg adjusted P < .05). Confounder-corrected analyses were adjusted for age, sex, ethnicity, body mass index, time between inclusion and 1 January 2020, and comorbidities (hypertension, diabetes, and cancer, as well as cardiovascular, pulmonary, and gastrointestinal disease). C, Cumulative incidence of severe COVID-19, stratified by tertiles of gut microbiota diversity (Shannon index at the species level). Participants who died from causes other than COVID-19 were censored. Lower diversity was associated with an increased risk of the primary outcome. D, This was not significant after correction for potential confounders. E, Participants with higher relative abundances of butyrate-producing bacteria had a decreased risk of severe COVID-19 as compared with participants with lower abundances, when analyzed as continuous feature and when stratified by tertiles of butyrate producer abundance. F, The association between the relative abundance of butyrate-producing bacteria and severe COVID-19 remained significant when corrected for potential confounders in a multivariable Cox proportional hazards model.
Finally, we restricted our analysis to participants with registered SARS-CoV-2 infection during follow-up (n = 934). Among these participants, gut microbiota differed between those with and without severe COVID-19 (P = .005; Figure 1A). The abundance of butyrate producers was lower in participants with severe COVID-19 as compared with participants with mild SARS-CoV-2 infection (no hospitalization or mortality; Wilcoxon rank sum test, P = .0099; data not shown).
DISCUSSION
In this large population-based cohort, we found that gut microbiota are associated with the risk of future severe COVID-19. Baseline gut microbiota composition differed between participants with and without hospitalization or mortality due to COVID-19 during follow-up. Specifically, high amounts of butyrate-producing bacteria were associated with a reduced risk of future severe COVID-19, even after adjustment for potential confounders.
Animal experiments showed protective effects of the microbiota-derived immunomodulatory metabolite butyrate against viral pneumonia. Butyrate enhances epithelial barrier function and prevents translocation of pathogens from the gut into the bloodstream [3, 6, 11]. In addition, butyrate influences systemic and pulmonary immune responses through the activation of G protein–coupled receptor signaling and inhibition of histone deacetylase activity, resulting in increased CD8^+^ T cell–intrinsic antiviral responses and reduced airway neutrophilia, thereby limiting lung damage [4, 6]. Our findings align with these experiments, translating the preclinical evidence to humans. Moreover, we expand on previous studies showing that colonization with butyrate producers is associated with protection against infections in hematopoietic stem cell transplant recipients and the general population [7, 9]. Here, we found that the role of butyrate-producing gut microbiota is not limited to high-risk groups or all-cause infections but also applies to viral pneumonia. Combined with the preclinical evidence, our findings suggest that microbiome-directed therapies aimed at increasing intestinal abundances of butyrate producers might limit the risk of future severe viral pneumonia. For example, recent murine studies showed that the delivery of butyrate-producing bacteria (eg, Faecalibacterium prausnitzii or other Oscillospiraceae) dampened inflammation and improved the outcomes of bacterial and viral pneumonia—motivating studies investigating the clinical potential of such novel probiotics [5, 12, 13].
Among participants with a documented positive SARS-CoV-2 polymerase chain reaction result, gut microbiota differed between those with and without severe COVID-19, with a loss of butyrate-producing bacteria associated with severe COVID-19. Contracting SARS-CoV-2 is probably mainly driven by exposure to the virus, while gut microbiota are linked with development of severe disease following infection (we did not examine associations between microbiota and the risk of acquiring SARS-CoV-2). This work is limited by the time between sample collection and the start of the COVID-19 pandemic. Microbiota probably changed over time, which may obscure the relationship with outcomes, although microbiota reportedly are stable for years [14]. Moreover, although previous studies showed that relative abundances of butyrate-producing bacteria strongly correlate with actual fecal butyrate concentrations [7, 9, 10], butyrate production depends on strain-level differences in gut bacteria and environmental context, which we did not account for here.
In conclusion, we showed that gut microbiota, especially low levels of butyrate producers, are coupled with a higher risk of severe COVID-19. Butyrate-producing gut microbiota may represent a novel therapeutic target for the prevention of viral pneumonia.
Supplementary Material
jiaf541_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yeoh YK, Zuo T, Lui GC, et al Gut microbiota composition reflects disease severity and dysfunctional immune responses in patients with COVID-19. Gut 2021; 70:698–706.33431578 10.1136/gutjnl-2020-323020 PMC 7804842 · doi ↗ · pubmed ↗
- 2Zhang F, Lau RI, Liu Q, Su Q, Chan FKL, Ng SC. Gut microbiota in COVID-19: key microbial changes, potential mechanisms and clinical applications. Nat Rev Gastroenterol Hepatol 2023; 20:323–37.36271144 10.1038/s 41575-022-00698-4PMC 9589856 · doi ↗ · pubmed ↗
- 3Bernard-Raichon L, Venzon M, Klein J, et al Gut microbiome dysbiosis in antibiotic-treated COVID-19 patients is associated with microbial translocation and bacteremia. Nat Commun 2022; 13:5926.36319618 10.1038/s 41467-022-33395-6PMC 9626559 · doi ↗ · pubmed ↗
- 4Trompette A, Gollwitzer ES, Pattaroni C, et al Dietary fiber confers protection against flu by shaping Ly 6c- patrolling monocyte hematopoiesis and CD 8+ T cell metabolism. Immunity 2018; 48:992–1005.e 8.29768180 10.1016/j.immuni.2018.04.022 · doi ↗ · pubmed ↗
- 5Chollet L, Heumel S, Deruyter L, et al Faecalibacterium duncaniae as a novel next generation probiotic against influenza. Front Immunol 2024; 15:1347676.38590519 10.3389/fimmu.2024.1347676 PMC 11000806 · doi ↗ · pubmed ↗
- 6Kullberg RFJ, Haak BW, Chanderraj R, Prescott HC, Dickson RP, Wiersinga WJ. Empirical antibiotic therapy for sepsis: save the anaerobic microbiota. Lancet Respir Med 2024; 13:92–100.39401510 10.1016/S 2213-2600(24)00257-1 · doi ↗ · pubmed ↗
- 7Kullberg RFJ, Wikki I, Haak BW, et al Association between butyrate-producing gut bacteria and the risk of infectious disease hospitalisation: results from two observational, population-based microbiome studies. Lancet Microbe 2024; 5:100864.38909617 10.1016/S 2666-5247(24)00079-X · doi ↗ · pubmed ↗
- 8Hyams C, Challen R, Marlow R, et al Severity of Omicron (B.1.1.529) and Delta (B.1.617.2) SARS-Co V-2 infection among hospitalised adults: a prospective cohort study in Bristol, United Kingdom. Lancet Reg Health Eur 2023; 25:100556.36530491 10.1016/j.lanepe.2022.100556 PMC 9742675 · doi ↗ · pubmed ↗