Safety and efficacy of physical activity in hypertrophic cardiomyopathy patients: a systematic review and metanalysis
Francesco Borrelli, Filippo Tarditi, Alessandro Andreis, Barbara Mabritto, Andrea Silvio Benso, Elisabetta Toso

TL;DR
This study finds that moderate physical activity is safe and beneficial for most people with hypertrophic cardiomyopathy, challenging previous restrictions.
Contribution
The study provides new evidence that structured exercise does not increase risk of major adverse events in low-risk HCM patients.
Findings
Exercise does not increase risk of major cardiovascular events in HCM patients.
Moderate-intensity exercise improves cardiorespiratory fitness in HCM patients.
Current guidelines are shifting toward individualized exercise recommendations for HCM.
Abstract
Hypertrophic Cardiomyopathy (HCM) is a fairly common inherited cardiac disease, with a prevalence of about 1:200–1:500, characterized by left ventricular hypertrophy (LVH ≥15 mm) often associated with microvascular dysfunction, myocardial fibrosis and major ventricular arrhythmic events. Historically, HCM has been managed conservatively, with universal restrictions on vigorous physical activity due to concerns about ventricular arrhythmias and sudden cardiac death (SCD), particularly in the context of competitive sports. These recommendations, once codified in the 2020 AHA and ESC guidelines, led to significant secondary consequences including increased risk of obesity, metabolic syndrome, and psychological distress. The 2023 Italian Cardiology Protocols for Eligibility for Competitive Sport (COCIS), aligned with the European and American guidelines, provide a rigorous diagnostic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
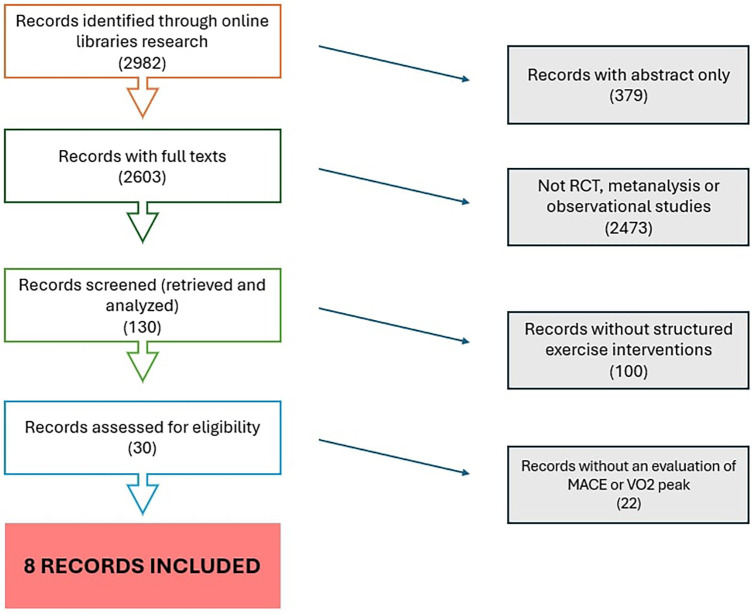 Figure 1
Figure 1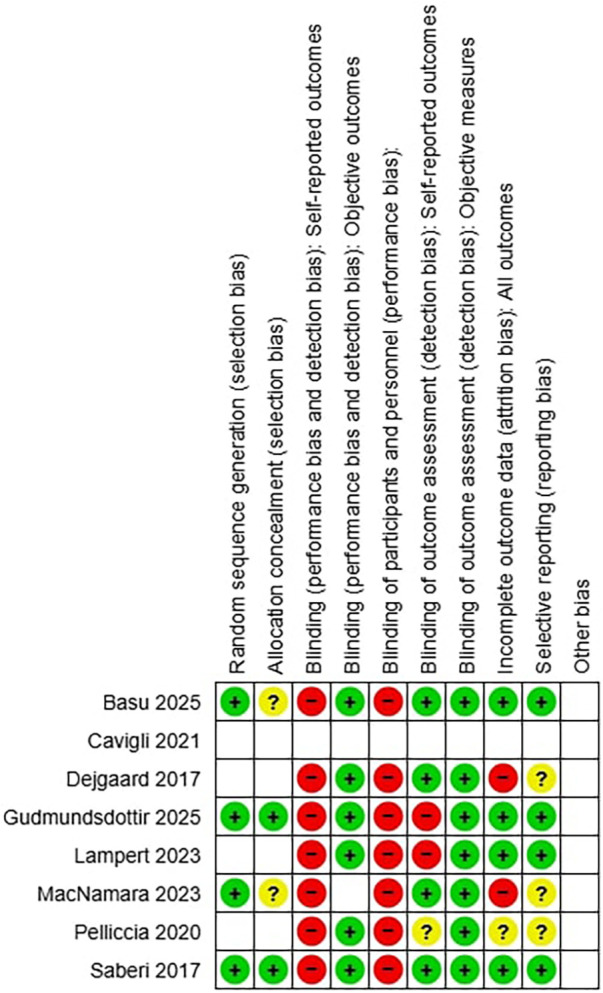 Figure 2
Figure 2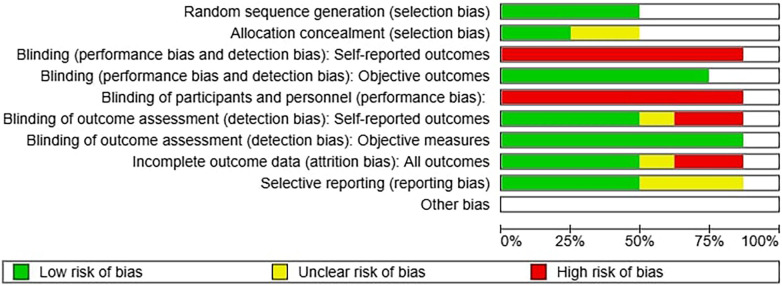 Figure 3
Figure 3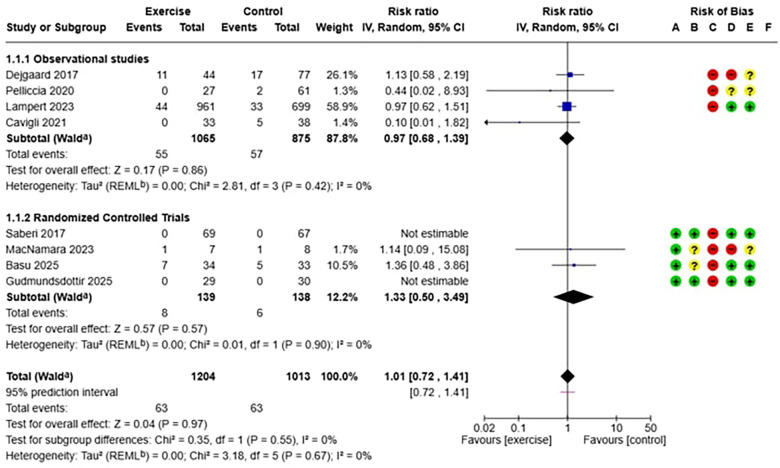 Figure 4
Figure 4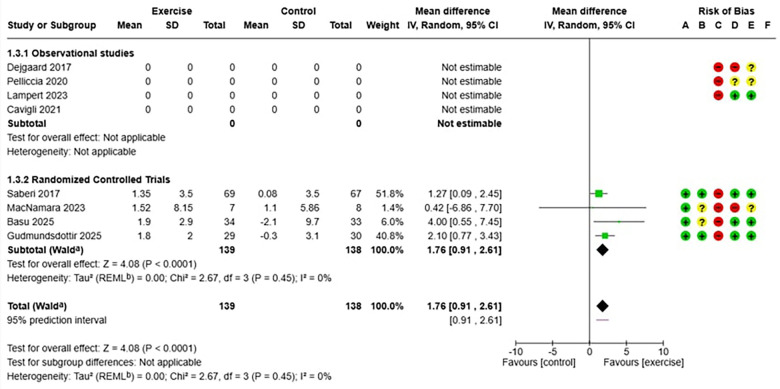 Figure 5
Figure 5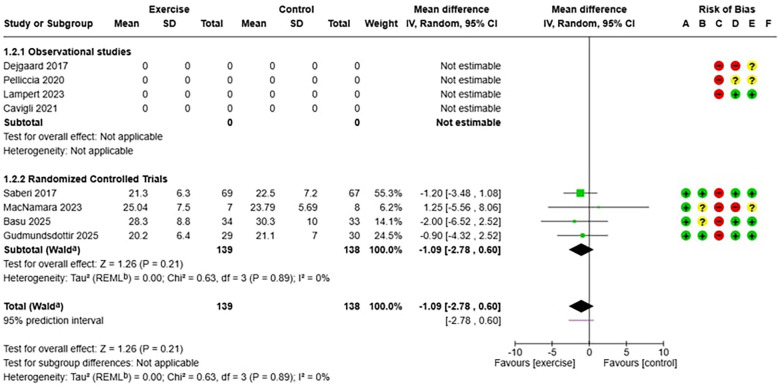 Figure 6
Figure 6| Author, Year | Type | Inclusione criteria | Exclusion criteria | Outcomes | Experimental treatment design |
|---|---|---|---|---|---|
| Saberi et al. 2017 ( | RCT | HCM, 18–80 yrs | NYHA IV, arrhytmias, effort syncope, CAD, exercise limitations, FE < 55%; pregnancy | VO2 peak | ET (moderate intensity) vs. usual care |
| Dejgaard et al. 2018 ( | Retrospective/observational | HCM | myectomy | MACE | Athletes (>4 h/wk >6 years) vs. non atheletes (<4 h/w o <6/years) |
| Pelliccia et al. 2020 ( | Retrospective/observational | HCM, regular EF | / | MACE | Continua ET vs. STOP |
| Lampert et al. 2023 ( | Prospective/observational | HCM,8–60 years, | NYHA III-IV,syndromic/infiltrative diseases | MACE | Non vigorous ET (sedentary and moderate) vs. vigorous ET |
| Cavigli et al. 2021 ( | Prospective/observational | HCM, >18 years | NYHA III-IV, effort symptoms, exercise limtations, recent hospitalitation < 3 mesi, myectomy | VO2 peak | ET vs. STOP |
| MacNamara et al. 2022 ( | RCT | HCM | NYHA IV, effort symptoms, LVOT obstruction, pregnancy, myectomy, recent hospitalitation, CAD | vo2peak | HIT vs. MICT |
| Basu et al. 2025 ( | RCT | HCM, 16- 60 years, NYHA I e II, able to ex. | athtletes, arrhytmias, syncope, CAD, myectomy, ICD, LVOT obstruction, FE < 35%, renal diseases, pregnancy | MACE | HIT vs. usual care |
| Gudmundsdottir et al. 2025 ( | RCT | HCM, >18 yrs | LVOT obstruction, effort symptoms, myectomy, valvulopathy, CAD, exercise limitations, athletes | vo2peak | ET vs. usual care |
| Author | N° | Age | GEN (M %) | N° ET | ADV EV. MACE ET | N Contr | ADV EV. MACE Contr. | VO2 peak T0 ET | VO2 peak T1 ET | Delta VO2 ET | VO2 peakT0 Contr | VO2 peak T1 Contr | Delta VO2 Contr |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Saberi et al. 2017 ( | 136 | 50 | 58 | 69 | 0 | 67 | 0 | 21.3 (6.3) | 22.6 (6.3) | 1.27 (3.5) | 22.5 (7.2) | 22.5 (7.2) | 0.08 (3.5) |
| Dejgaard et al. 2018 ( | 121 | 55 | 53 | 44 | 11 | 77 | 17 | – | – | – | – | – | – |
| Pelliccia et al. 2020 ( | 88 | 31 | 81 | 27 | 0 | 61 | 2 | – | – | – | – | – | – |
| Lampert et al. 2023 ( | 1,660 | 39 | 69 | 961 | 44 | 699 | 33 | – | – | – | – | – | – |
| Cavigli et al. 2021 ( | 71 | 38.5 | 90 | 33 | 0 | 38 | 5 | 32.9 (7.4) | – | – | 25.2 (7.4) | – | – |
| MacNamara et al. 2022 ( | 15 | 47.5/8.7 | 67 | 7 | 1 | 8 | 1 | 25.04 (7.5) | 26.56 (8.67) | 1.52 (8.15) | 23.79 (5.69) | 24.89 (6.01) | 1.1 (5.86) |
| Basu et al. 2025 ( | 67 | 48/44 | 90/77,5 | 34 | 7 | 33 | 5 | 28.3 (8.8) | 30.2 (8.7) | 1.9 (9.7) | 30.3 (10) | 28.2 (8.7) | −2.1 (9.7) |
| Gudmundsdottir et al. 2025 ( | 59 | 58 | 73 | 29 | 0 | 30 | 0 | 20.2 (6.4) | 22 (7.6) | 1.8 (2.0) | 21.1 (7) | 20.8 (9) | −0.3 (3.1) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Effects of Exercise · Cardiomyopathy and Myosin Studies · Physical Activity and Health
Introduction
Hypertrophic cardiomyopathy (HCM) is one of the most prevalent inherited structural heart diseases, with an estimated prevalence of 1:500 in the general population (1–5). Characterized by unexplained left ventricular hypertrophy, HCM presents a broad phenotypic and prognostic spectrum, ranging from asymptomatic forms to severe clinical manifestations, including heart failure, ventricular arrhythmias, and sudden cardiac death (6–12).
Traditionally, international sports cardiology guidelines have recommended restricting vigorous physical activity for patients with HCM, based primarily on observational data suggesting an increased risk of arrhythmic events during vigorous exercise (13–15). Recent studies have reported significantly elevated rates of SCD in high-physiological-stress disciplines such as competitive bodybuilding in both males and females (16, 17). However, this restrictive approach has resulted in significant limitations on patients' quality of life, particularly for young and physically active individuals (18).
In recent years, growing evidence has increasingly challenged this paradigm, suggesting that structured and supervised exercise may not only be safe but also beneficial for patients with HCM (19–23). Several studies have demonstrated improvements in functional capacity (24), quality of life, and cardiometabolic parameters (25, 26), without any corresponding rise in major adverse cardiovascular events (MACE) (10, 14, 18–22, 27–29) also with the use of CPET (30, 31).
In the Italian regulatory framework, eligibility for competitive sports is governed by the COCIS protocols (3). While international guidelines increasingly promote shared decision-making for sport participation, this principle does not apply to competitive sports in Italy, where the final judgment lies exclusively with the sports medicine physician. Shared decision-making is instead fully applicable in determining safe levels of recreational and therapeutic exercise.
Several systematic reviews have previously examined the relationship between exercise and hypertrophic cardiomyopathy, but these analyses have been limited by smaller samples, narrower inclusion criteria, or outdated evidence. For example, the 2025 meta-analysis by Albulushi et al. (32). included fewer randomized trials and did not integrate the most recent high-intensity training trials published in 2024–2025. Moreover, prior reviews focused predominantly on safety outcomes, whereas the present study concurrently evaluates both efficacy (VO₂ peak changes) and safety (MACE incidence), using the most comprehensive dataset to date, updated to May 2025.
Importantly, the studies included in this meta-analysis evaluate individuals involved in recreational, moderate, or supervised structured exercise, not competitive athletic participation, which limits the generalizability of findings to decisions regarding competitive eligibility.
Objectives
The primary aim of this review is to assess the safety of exercise in patients with HCM by analyzing the incidence of MACE, including sudden cardiac death, resuscitated cardiac arrest, sustained ventricular tachycardia, and appropriate implantable defibrillator shocks.
A secondary objective is to evaluate the efficacy of exercise in improving cardiorespiratory fitness, measured by changes in peak oxygen consumption (VO_2_ peak) between the exercise training group and the control group.
Methods
Research strategy and study selection process
A systematic search of literature was conducted in major biomedical databases (PubMed/MEDLINE, Embase, Cochrane Central Register of Controlled Trials) updated to May 2025. The following search strings were used:
- -PubMed/MEDLINE: “hypertrophic cardiomyopathy"[MeSH] OR “HCM” AND (“exercise” OR “physical activity” OR “training” OR “rehabilitation”) AND (“clinical trial” OR “cohort” OR “observational study”)
- -Embase: ‘hypertrophic cardiomyopathy'/exp AND (‘exercise'/exp OR ‘physical activity’ OR ‘training’) AND (‘clinical trial'/exp OR ‘cohort study'/exp)
- -Cochrane CENTRAL: (hypertrophic cardiomyopathy) AND (exercise OR training). A comprehensive search strategy was developed according to PRISMA-S guidelines (Figure 1).
PRISMA flow diagram. PRISMA, preferred reporting items for systematic reviews and meta-analyses.
Two independent reviewers screened titles, abstracts, and full texts. Disagreements were resolved by consensus or by a third reviewer when necessary. Data extraction was performed independently by the same reviewers using a standardized form.
The protocol was registered on PROSPERO with the ID 1149432 created on the 16 September 2025.
Inclusion ed exclusion criteria
Inclusion criteria
-Randomized controlled trials (RCTs) and observational studies (cohort, case-control)-Patients with confirmed diagnosis of hypertrophic cardiomyopathy-Structured exercise interventions of any intensity and duration-Presence of a control group-Safety outcomes (MACE events) and/or efficacy outcomes (VO₂ peak) reported
Exclusion criteria
-Case reports, case series, editorials, letters-Studies on pediatric populations (<18 years)-Patients with secondary hypertrophic cardiomyopathy-Lack of extractable data for meta-analysis-Duplication of already included cohorts
Risk of bias assessment
Risk of bias was assessed using validated tools appropriate for each study design. Randomized controlled trials were evaluated with the Cochrane RoB 2 tool, whereas observational studies were assessed using ROBINS-I. Two reviewers independently performed the assessments, with discrepancies resolved through discussion. Risk-of-bias judgments did not influence study weighting in the meta-analysis, which followed methodological conventions of aggregating effect sizes irrespective of quality; however, results were interpreted in light of the identified limitations. Sensitivity analyses excluding studies at high risk of bias were considered but not performed due to the small number of available randomized trials and the consequent loss of statistical power. Risk of bias assessment is summarized in Figures 2, 3.
(on the left): types of bias of each study, green+ if the bias is present, red—if the bias is absent, yellow? if the bias is uncertain.
(above): summary of bias considering all studies.
Data
The extracted information included:
- -Study characteristics: authors, year, design, and follow-up duration
- -Population characteristics: sample size, age, sex, HCM phenotype, and presence of left ventricular outflow tract obstruction
- -Intervention details: type, intensity, duration, and frequency of exercise
- -Primary and secondary outcomes: safety outcomes (MACE events) and efficacy outcomes (VO₂ peak)
- -Data for risk of bias assessment: information to evaluate the risk of bias in included studies
Statistical analysis
The meta-analyses were conducted using Review Manager 5.4 software. For dichotomous outcomes (MACE events), risk ratios (RR) with 95% confidence intervals were calculated, while for continuous outcomes (VO₂ peak), mean differences (MD) or standardized mean differences (SMD) were used when appropriate. Given the clinical heterogeneity among included studies, a random-effects model (DerSimonian–Laird) was chosen a priori for all analyses. Zero-event studies were handled using a continuity correction of 0.5 added to each cell of the 2 × 2 table. Heterogeneity was assessed using I² and Cochran's Q, and potential sources of heterogeneity were explored through subgroup analyses (RCTs vs. observational studies, exercise intensity categories). Publication bias was evaluated through visual inspection of funnel plots and, when applicable (≥10 studies), Egger's regression test. Because only eight studies met inclusion criteria, formal statistical testing for funnel-plot asymmetry was interpreted with caution.
Studies included
The systematic search identified eight eligible studies published between 2017 and 2025, including four randomized controlled trials (RCTs) and four observational studies. The studies enrolled a total of 2,217 patients with hypertrophic cardiomyopathy, with a mean age ranging from 42 to 58 years. The exercise protocols included moderate- to vigorous aerobic training, with durations ranging from 12 to 24 weeks for the RCTs and long-term follow-up evaluations for the observational studies.
Results
The meta-analysis included eight studies conducted in various geographic and clinical settings. Four randomized controlled trials (7, 29, 33, 34) provided evidence on the efficacy of exercise, while four observational studies (6, 11, 20, 27) primarily contributed to the evaluation of long-term safety, including larger populations and extended follow-up periods (Tables 1, 2). The analysis of safety and efficacy of exercise in patients with hypertrophic cardiomyopathy (HCM) included a total of 2,217 patients, with 1,204 assigned to the exercise group and 1,013 to the control group. The heterogeneity between studies was very low (I^2^ = 0%), suggesting consistency of results across different populations and exercise protocols. In the analysis of the relationship between exercise and major adverse cardiovascular events (MACE) in HCM (Figure 3), the overall risk ratio was 1.01 (95% CI: 0.72–1.41) with a p-value of 0.97, indicating no statistically significant differences between the two groups. Subgroup analysis showed consistent results in both observational studies (RR 0.97, 95% CI: 0.68–1.39) and randomized trials (RR 1.33, 95% CI: 0.50–3.49), although the latter showed wider confidence intervals due to smaller sample sizes. Regarding efficacy analysis, no significant differences were observed in baseline VO₂ peak values between the intervention and control groups (mean difference: −1.09 ml/kg/min, 95% CI: −2.78 to 0.60, p = 0.21), confirming the adequacy of randomization in controlled clinical studies (Figure 5). However, at the end of the exercise programs, a statistically significant and clinically relevant improvement was observed in the group undergoing physical training. The mean difference in VO₂ peak change was +1.76 ml/kg/min (95% CI: 0.91–2.61) in favor of the exercise group, with a p-value < 0.0001 (Figure 6). This improvement, documented in four high-quality randomized trials (7, 29, 33, 34), represents a clinically significant increase in functional capacity, translating to improved quality of life and exercise tolerance in patients.
(below): forest plot which shows the relationship between exercise and major adverse cardiovascular events (MACE) in HCM.
(on the top): forest plot which shows the mean difference in term of peak oxygen consumption (VO2 peak) between exercise and control group before the training.
(above): forest plot which shows the mean difference in term of peak oxygen consumption (VO2 peak) between exercise and control group after the training.
In conclusion, our meta-analysis provides robust and reassuring evidence on the safety and efficacy of structured exercise in this population. The results demonstrate that exercise does not increase the risk of major adverse cardiovascular events (RR 1.01, 95% CI: 0.72–1.41, p = 0.97) and, at the same time, leads to a clinically significant improvement in cardiorespiratory functional capacity (+1.76 ml/kg/min in VO₂ peak, p < 0.0001).
Discussion
A crucial point in interpreting these findings is that the majority of the included studies did not investigate competitive athletes but rather patients engaging in moderate-intensity or supervised structured exercise. Only a minority of studies (21, 23, 27, 29) evaluated individuals performing vigorous training, and even in these cases, competitive participation was not systematically assessed. Therefore, while the results support the safety of exercise in low-risk HCM patients, they cannot be directly extrapolated to high-intensity competitive sports participation.
The most relevant finding from this analysis concerns the cardiovascular safety of exercise in patients with hypertrophic cardiomyopathy (HCM). The absence of a statistically significant increase in MACE incidence represents a clinically important outcome, challenging traditional restrictive recommendations based primarily on outdated case reports. The low heterogeneity observed (I^2^ = 0%) further strengthens this finding, suggesting consistency across different populations, exercise protocols, and clinical settings.
The 1.76 ml/kg/min improvement in VO₂ peak observed in the exercise group represents a clinically significant increase in functional capacity. This improvement, equivalent to approximately 7%–10% compared to baseline values typical of patients with HCM (7, 34) translates into tangible benefits in daily life, including increased tolerance to physical activities, reduced exertional dyspnea, and improved perceived quality of life.
The mechanisms underlying this improvement are multifaceted and involve both central and peripheral adaptations. At the cardiac level, aerobic exercise can lead to improvements in diastolic function, reduced ventricular stiffness, and optimized ventricular filling.
These results emphasize the importance of appropriately structured and supervised exercise programs, preceded by accurate individual risk stratification. This methodological approach reflects optimal clinical practice and highlights the need for specialist evaluation before starting any exercise program.
The prescription of exercise in patients with HCM requires specialized expertise and a multidisciplinary approach. Evaluation should include a thorough family and personal history, physical examination, electrocardiogram, echocardiogram, cardiopulmonary exercise testing (CPET), and, when indicated, Holter monitoring and cardiac magnetic resonance imaging.
The cardiopulmonary exercise test (CPET), CPET, possibly combined with stress echocardiography, is essential for the functional assessment of patients with hypertrophic cardiomyopathy and for individualized exercise prescription. VO₂peak reflects maximal aerobic capacity, while the anaerobic threshold (AT/VT1) delineates the upper limit of sustainable effort and guides the selection of safe training intensities. The second ventilatory threshold (VT2/RCP) identifies the high-intensity domain, to be used only in selected and closely supervised protocols. Parameters such as the VE/VCO₂ slope, ventilatory graphs, and pulse oximetry quantify ventilatory efficiency and help tailor interventions targeting respiratory muscle strength when limitations are present. The O₂ pulse trend supports the detection of left ventricular dysfunction and the definition of thresholds beyond which exercise may become harmful. CPET also enables identification of chronotropic incompetence, abnormal blood pressure responses, and exercise-induced arrhythmias, thereby establishing safe heart rate and blood pressure ranges for training.
While the physiological rationale for exercise benefits is well established, the actual clinical evidence remains limited by short intervention periods, heterogeneous training programs, and incomplete assessment of disease progression. These factors underscore the need for cautious interpretation.
The findings of this meta-analysis support a paradigm shift in the clinical management of patients with HCM, moving from a universally restrictive approach to a personalized strategy based on individual risk stratification. This shift is already reflected in recent international guidelines, which recognize the possibility of participation in recreational and competitive physical activities for selected low-risk patients.
The clinical message proposed by our review is also supported by Albulushi et al. (32). The two studies converge on a central point: physical activity, when structured and supervised, appears to be generally safe in patients with HCM and is associated with functional and quality of life benefits. The common idea is to move away from generalized prohibitions and towards personalized prescriptions, with risk stratification, monitoring, and gradual progression of intensity. For both studies, gray areas remain, such as the optimal dose, the role of high intensity, the duration needed to consolidate benefits, and management in carriers of ICDs or in the presence of extensive fibrosis.
Despite increasing evidence supporting exercise in HCM, there remain no clear, harmonized recommendations for prescribing physical activity in patients with obstructive hypertrophic cardiomyopathy. Optimal exercise modalities, safe intensity thresholds, and contraindications for this subgroup remain areas of uncertainty. Dedicated studies focusing on obstructive phenotypes are urgently needed.
Conclusions
The meta-analysis included 8 studies on 2217 patients with HCM, of whom 1204 were in the exercise group and 1013 in the control group.
In summary, this meta-analysis provides encouraging evidence that structured and supervised exercise appears safe and improves functional capacity in patients with hypertrophic cardiomyopathy, particularly in those classified as low-risk. However, these conclusions must remain conditional given the limited follow-up duration, variability in exercise protocols, and risk of bias in several included studies. Exercise prescription should therefore be individualized, guided by specialist evaluation, and not extrapolated to vigorous or competitive sports participation without further evidence.
Study limitations
The main limitations of this meta-analysis are as follows:
The overall risk of bias was substantial across multiple domains, affecting both randomized control trials (RCTs) and observational studies. In particular, limitations in randomized procedures, blinding and outcome assessment may have introduced systematic error and influenced effect estimates.
Another important limitation concerns the small sample sizes of most available studies. Except for the large observational cohort by Lampert et al. (20), the remaining trials and cohort studies enrolled relatively few participants, which reduces statistical power and widens confidence intervals, particularly for rare outcomes such as arrhythmic events or sudden cardiac death. This limitation restricts the generalizability of the safety conclusions, especially regarding vigorous-intensity activities.
The short duration of follow-up limits the ability to evaluate long-term safety and sustainability of benefits. RCTs with follow-up periods of only 12–24 weeks cannot adequately capture the persistence of physiological adaptations, potential disease progression or hard clinical endpoints such as mortality and MACE.
Finally, the absence of standardized exercise interventions led to considerable heterogeneity in training modality, intensity, frequency, session duration and supervision. This variability hampers the identification of an optimal exercise prescription and reduces the generalizability of the findings to clinical practice.
Future research directions
The results of this meta-analysis highlight multiple perspectives for future research in the field of exercise for patients with hypertrophic cardiomyopathy. Future studies should focus on conducting adequately powered RCTs with larger sample sizes and extended follow-up durations to assess the long-term effects of exercise on disease progression, quality of life, and cardiovascular prognosis. Research should investigate the efficacy of different types of training (aerobic, resistance, combined) in specific subgroups of patients.
In addition, future research should aim to develop precision-based algorithms for exercise prescription that integrate genetic, phenotype and functional data, thereby enabling truly individualized exercise programs aligned with each patient's physiological and clinical profile.
The studies included in this meta-analysis primarily assessed functional outcomes (VO₂ peak) and clinical safety events (MACE). However, they did not systematically evaluate disease progression markers such as left ventricular wall thickness, extent of late gadolinium enhancement, atrial remodeling, or arrhythmic burden during follow-up. To determine whether vigorous or competitive-level exercise may influence the natural history of HCM, future studies should incorporate longitudinal imaging and electrophysiological endpoints.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ommen SR Mital S Burke MA Day SM Deswal A Elliot P 2020 Aha/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: executive summary: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation. (2020) 142(25):E 533–57. 10.1161/CIR.000000000000093833215938 · doi ↗ · pubmed ↗
- 2Ommen SR Ho CY Asif IM Ackerman MJ Brunckhorst C Caleshu C 2024 Aha/ACC/AMSSM/HRS/PACES/SCMR guideline for the management of hypertrophic cardiomyopathy: a report of the American Heart Association/American College of Cardiology joint committee on clinical practice guidelines. (2024) 149:1043-8. 10.1161/CIR.0000000000001250 · doi ↗
- 3FMSI, SIC sport A. Protocolli Cardiologici per Il Giudizio Di Idoneità Allo Sport Agonistico. (2023).
- 4Arbelo E Protonotarios A Gimeno JR Arbustini E Barriales-Villa R Basso C 2023 Esc guidelines for the management of cardiomyopathies: developed by the task force on the management of cardiomyopathies of the European Society of Cardiology (ESC). Eur Heart J. (2023) 44(37):3503–626. 10.1093/eurheartj/ehad 19437622657 · doi ↗ · pubmed ↗
- 5Maron BJ Gardin JM Flack JM Gidding SS Kurosaki TT Bild DE. Prevalence of hypertrophic cardiomyopathy in a general population of young adults: echocardiographic analysis of 4111 subjects in the CARDIA study. Circulation. (1995) 92(4):785–9. 10.1161/01.CIR.92.4.7857641357 · doi ↗ · pubmed ↗
- 6Pelliccia A Caselli S Pelliccia M Lemme E Squeo MR Italiano G Clinical outcomes in adult athletes with hypertrophic cardiomyopathy: a 7-year follow-up study. Br J Sports Med. (2020) 54(16):1008–12. 10.1136/bjsports-2019-10089032532845 · doi ↗ · pubmed ↗
- 7Mac Namara JP Dias KA Hearon CM Sarma S Fadel PJ Cornwell WK Limits to submaximal and maximal exercise in patients with hypertrophic cardiomyopathy. J Appl Physiol. (2022) 133(4):787–97. 10.1152/japplphysiol.00566.202135952351 · doi ↗ · pubmed ↗
- 8Lee HJ Gwak SY Kim K Park J Kim YJ Lee SP Factors associated with high-intensity physical activity and sudden cardiac death in hypertrophic cardiomyopathy. Heart. (2025) 111(6):253–61. 10.1136/heartjnl-2024-32492839848653 · doi ↗ · pubmed ↗