The value of health literacy for Global Health and One Health: nurturing the socioecological environment of schools
Orkan Okan, Andrea S Winkler

TL;DR
This paper explores how health literacy in schools can promote global health by considering individual and systemic factors.
Contribution
It introduces the HeLit-School framework to enhance health literacy through a One Health lens in educational settings.
Findings
Health literacy should be understood through a socioecological lens, not just as an individual trait.
The HeLit-School framework supports institutional transformation by integrating health literacy into school systems.
Principals and resources are critical for sustainable health promotion in schools.
Abstract
This perspective examines health literacy through a One Health lens, emphasizing its relevance for developing One Health−literate citizens, as advocated by the Lancet One Health Commission's recommendation on school health literacy. It argues for a comprehensive understanding of health literacy across the socioecological continuum, integrating both individual agency and structural influences. Rather than viewing low health literacy as an individual deficiency, this perspective situates it within broader systemic and contextual factors, particularly pertinent to low- and middle-income countries and underserved populations. Building on this premise, the Health-Literate School (HeLit-School) framework offers a whole-of-school approach to advancing health literacy by embedding the concept of organizational health literacy within school systems. Drawing on socioecological and organizational…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
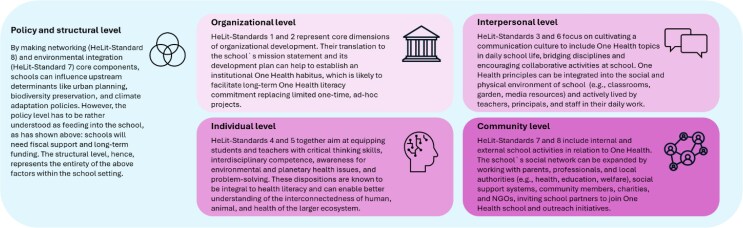 Figure 1
Figure 1| HeLit-School standards ( | HeLit-School adaption to One Health |
|---|---|
| Standard 1: Include health literacy in the school’s mission statement | Evolve the mission statement to explicitly incorporate One Health literacy, emphasizing education about the links between human health, animal health, and the health of the wider ecosystem. |
| Standard 2: Health literacy as part of school development | Integrate One Health principles into school policies and development plans, fostering curriculum development that reflects the interdependence of health across species and environments. |
| Standard 3: Promote and enhance health literacy in daily school life | Include activities and practices in everyday school routines and projects that raise awareness for One Health topics, such as zoonotic diseases, environmental sustainability, and ecosystem and planetary health. |
| Standard 4: Health literacy of students | Promote schoolchildren’s One Health literacy, encompassing not only personal and community health and well-being but also understanding of how animal and environmental health impacts human health and well-being, encouraging systems thinking and transdisciplinary learning. |
| Standard 5: Health-literate school staff | Train teachers and staff, including school principals, on One Health concepts so they can confidently incorporate these themes into teaching and engage schoolchildren in interconnected health topics along the One Health spectrum. |
| Standard 6: Health-literate communication at school | Implement communication that provides precise messages and easy-to-understand information about human, animal, and environmental health issues, fostering a One Health dialogue within and beyond school. |
| Standard 7: Enhance health literacy in the school environment | Create a school environment that includes One Health principles, e.g. supporting biodiversity on school grounds, promoting ecological awareness, and minimizing environmental hazards and health risks, and also encouraging out-of-classroom teaching. |
| Standard 8: Networking and cooperation | Build partnerships involving health professionals, veterinarians, environmental scientists, and the community to support school health initiatives that reflect the One Health approach. |
| Recommendations to achieve a One Health−literate global citizenry ( | HeLit-School standards ( | Socioecological levels ( | Suggested adaptations for LMICs | |
|---|---|---|---|---|
| Goals | prerequisites on policy and governance levels | Goals | actionable interventions at school level | |||
| 1. Advance One Health operationalization, implementation, and institutionalization through public−private partnerships | – | Std 2: School development | Organizational |
Context specificity: adapt school development plans to, e.g. meet local cultural requirements, social norms and roles, community needs, and economic circumstances (also relevant for goal #2 of actionable interventions) Collaborate with local leaders and elders, informal networks, local (traditional) health authorities, and low-cost partnerships with non-governmental organizations, farmers, agencies, community groups, and faith-based organizations (also relevant for goal #2 of actionable interventions) |
| 2. Mainstream One Health knowledge and principles at all levels of preschool, primary, and secondary schooling | Std 1: Mission statement | Organizational |
Adapt programmes and communication to local health promotion and prevention topics, local assessment needs, and infrastructure Consider differences between rural and urban area schools and schools in low-resource districts Empower communities to tell their own ‘health stories’ and drive community-led advocacy projects Integrate indigenous knowledge, take into account wider family environment Translate into informal and non-formal education (radio, storytelling, community workshops) | |
| 3. Build capabilities and capacity among youth (leadership, communication, negotiation, teamwork, innovative problem-solving) | Std 3: Daily school life | Individual |
Prioritize local health and well-being topics, combine with local health knowledge, adapt materials to meet local context and norms, and acknowledge interests and attitudes of children Use locally relevant, low-tech solutions (e.g. learning and teaching modes, school gardening, agriculture and sustainable farming, water harvesting, waste management, and hygiene) If necessary, adapt to implementing distant- and peer-learning techniques Run student-led advocacy and environmental projects, involve local councils, and integrate indigenous knowledge, experience, and attitudes | |
| 4. Facilitate professional lifelong learning and development | Std 5: Health-literate staff | Organizational |
Hands-on teaching strategies, workforce development, communication techniques Evaluate curriculum for in-service and pre-service teachers and adapt training materials to local (health, social, and cultural) context Use peer-to-peer teacher training, mobile learning platforms, and adapt/blend technology to context (e.g. low-bandwidth digital resources) Flexibility to account for low resources, balancing quality with scale regarding cost-effectiveness Mentorship for more effective practical experience | |
| 5. Build One Health literacy across all levels of the political spectrum for governance transformation | Relevant across Std 1–8 | Organizational |
Advocate for policies and funding across the political spectrum and for school health promotion, use tailored messages (also relevant for goal #1 of actionable interventions) Form alliances that include all relevant actors, empower communities, enable meaningful participation and ownership, and engage the media and civil society (also relevant for goal #1 of actionable interventions) Translate evidence from successful case studies benefitting long-term population health goals, provide reasons for legitimacy, highlight the return-on-investment effects, seek low-cost solutions if necessary and consider local realities, including traditional knowledge (also relevant for goal #1 of actionable interventions) Use grassroots movements and bottom-up and top-down strategies (also relevant for goal #1 of actionable interventions) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsZoonotic diseases and public health · Public Health Policies and Education · Global Public Health Policies and Epidemiology
Introduction
The recently published report of the ‘Lancet’ One Health Commission links One Health closely to the Global Health agenda (Winkler et al. 2025) and, in addition, presents a pathway for a new public health. A key commonality between the two concepts, i.e. One Health and Global Health, is the drawing on traditional health promotion concepts and methodologies, including equity-driven socioecological and upstream determinant-based approaches, collective and collaborative action, systemic transformation, interdisciplinary and intersectoral thinking, and setting-based, whole-of-environment frameworks, to improve population health outcomes. Both concepts also seek to tackle complex health challenges across disciplinary fields and sectors that have become inherent in the 21st century resulting from globalization and the diminishing of disciplinary and sectoral boundaries, as well as the complex, often opaque interaction of socioeconomic, environmental, geographical, political, commercial, technological, digital, and social determinants. While those determinants and their influence on people's lives, including their impact on health and well-being, are well documented (Marmot et al. 2012, Donkin et al. 2018, World Health Organization 2025), contrary to their impact on animal health and welfare, they may seem intangible or imperceptible in everyday life but hint at the need for system-level structural interventions to address the root causes of ill health and health inequities (Marmot et al. 2012, Winkler et al. 2025 , World Health Organization 2025). Interestingly, both concepts also recommend utilizing health literacy as a key strategy to achieve their overarching goals. Echoing the World Health Organization’s recommendations to incorporate health literacy into school education (Kickbusch et al. 2013, McDaid 2016, World Health Organization 2017, 2021), the Lancet One Health Commission also advocates for One Health literacy in schools, preschools, and tertiary education (Winkler et al. 2025 ). Similarly, further Lancet Commissions and Series are emphasizing the adaptation of health literacy strategies in schools (Patton et al. 2016, Baird et al. 2025) and for improving primary care delivery in low- and middle-income countries (LMICs; Lilford et al. 2025). Widespread low levels of health literacy among schoolchildren in many countries underscore the urgent need to invest in school health literacy (Paakkari et al. 2020, Stauch et al. 2025), especially because higher health literacy levels are linked to improved health and behaviour outcomes (Fleary et al. 2018 ) and at school, all school-aged children can be reached regardless of their social background (World Health Organization 2021, Kirchhoff et al. 2025). However, most existing population-based studies in child and adolescent populations have been conducted in the European Region or North America, making it difficult to make assumptions about child and adolescent health literacy in LMICs and non-Western countries. Nevertheless, findings across studies reveal that children’s low health literacy levels consistently follow a social gradient, disproportionately affecting children from low socioeconomic family households and reinforcing pre-existing inequalities (Paakkari et al. 2019, Kirchhoff et al. 2025). Therefore, a global One Health−oriented citizenry, an ambition stemming from the call to enable One Health−literate citizens (Winkler et al. 2025), requires a system-wide adaption of early health-promoting school interventions supported by policies dedicating explicit commitment, funding, and social investment. This call has recently been echoed by scholars who emphasize the importance of planetary and One Health literacy in tackling current environmental, health, and social challenges (Jochem et al. 2025). One Health literacy is based on the generic concept of health literacy as defined by the European Health Literacy Survey Consortium (Sørensen et al. 2012) and describes it as a set of prerequisites ‘to access, understand, appraise and apply all relevant information that are related to One Health in order to make judgments, take decisions and actions in everyday life concerning healthcare, disease prevention and health promotion to sustainably balance the health and quality of life of us humans, the animals and the environment’ (Blankart et al. 2024). Public health strategies exclusively focusing on individual-level, behavioural health literacy programmes at school and not accounting for prevalent social and health inequalities are unlikely to achieve sustainable improvements in child and adolescent health literacy across the gradient (Kickbusch et al. 2013, Kirchhoff et al. 2025). Instead, equity-driven school health literacy requires a structural, setting-based, and policy-level approach as a starting point. However, the systemic-level intervention will on its own not solve the challenges in implementing school health literacy, but it is the quintessential step to foster a climate that enables meaningful action on the ground to improve health literacy, alongside policy support, sustainable funding, improvements in the environment, and professional training.
Given these observations, this viewpoint aims to elucidate the various facets and multiple meanings of health literacy with a focus on One Health and how those can actually support developing One Health−literate citizens, as recommended by the Lancet One Health Commission. In doing so, the focus is on expanding on the recommendations to embrace the full socioecological spectrum provided by health literacy. This perspective will add to Global Health and One Health education frameworks by drawing on health literacy’s inherent attributes of upstream, setting-based, and environmental characteristics, combining behaviour and structure perspectives.
Understanding health literacy
Health literacy is often referred to as an information management skill enabling people to navigate complex health information ecosystems and healthcare service environments (Nutbeam and Muscat 2021). It represents a rather new tool in the larger public health toolbox of concepts to improve individual and population health outcomes through health-promoting and preventive measures. Conceptually, commonly stressed features of health literacy include information seeking, understanding, critical thinking and appraisal, as well as using information to influence decision-making processes and eventually behaviour (Sørensen et al. 2012). Health-literate individuals are also empowered to comprehend public health topics, concepts, and strategies and discern health facts from health mis- and disinformation, which has become more important since the COVID-19 pandemic and the associated infodemic (Okan et al. 2020a, Paakkari and Okan 2020). Health literacy draws upon knowledge and competencies, yet it is a separate construct. Like most other educational, pedagogical, or psychological constructs, health literacy integrates knowledge and competencies into its own fabric and even presupposes them (Nutbeam and Muscat 2021, Sørensen et al. 2021), but it is oriented towards and shaped by its objective to enable individuals, especially to make informed health choices rather than just possess factual health knowledge without being able to use information.
However, this conceptualization falls short of the true depth of health literacy that could contribute to achieving the goals set out in the Global Health and One Health agendas (Winkler et al. 2025). Aside from understanding health literacy as a prerequisite set of health skills (Nutbeam and Muscat 2021), health literacy has been conceptualized as a relational model shifting from viewing low health literacy as a behavioural deficit to account for the impact of systems, environmental conditions, and upstream determinants (Parker and Ratzan 2010, Brach et al. 2012, Sørensen et al. 2021, Kirchhoff et al. 2025). Health literacy reflects both behavioural and structural aspects, which can be beneficial, especially for LMICs and further underserved communities, as the individual is viewed in the light of the interactions with systems and available resources. Setting the relational model as a conceptual backbone, health literacy’s full scope includes two interdependent facets: (i) agency and behaviour change models linked to knowledge and competency approaches addressing individual-level factors (e.g. personal health literacy) and (ii) structure and social change models linked to socioecological and setting approaches addressing environmental-level factors (e.g. systemic or organizational health literacy; Brach et al. 2012, Abel and Benkert 2022, Kirchhoff et al. 2025).
The agency dimension of health literacy
On the agency side of the equation, an increased understanding of health information and the knowledge of how to utilize information is meant to improve people’s health and well-being outcomes (Sørensen et al. 2012, Nutbeam and Muscat 2021, Abel and Benkert 2022, Levin-Zamir et al. 2025). Health-literate individuals are better equipped to access and navigate healthcare and information systems, understand health messages and see through false health claims, reflect on treatment options and medication instructions, communicate confidently about health, and frequently engage in health-promoting and preventive measures (Parker and Ratzan 2010, Sørensen et al. 2012, Paakkari and Okan 2020). Improved personal health literacy may also mediate between unequally distributed socioeconomic factors and personal resources in disadvantaged and underserved populations, contributing to reducing health disparities and promoting health equity (Paakkari et al. 2019, Stormacq et al. 2019). The Lancet One Health Commission suggests that health literacy presupposes media literacy (Winkler et al. 2025) and both concepts indeed represent conceptual synergies, even overlapping in some of their dimensions (Schulenkorf et al. 2021, World Health Organization 2021). A most welcome side effect is that a media or digital literacy curriculum at school can be used to teach health literacy (Schulenkorf et al. 2021, Stauch et al. 2025), while avoiding putting additional burden on schools and their already overcrowded curriculum, low resources, and often understaffed workforce (Schulenkorf et al. 2021, Kirchhoff et al. 2025). If linked to health-related topics, media or digital literacy education at school can reinforce children’s abilities to, e.g. distinguish correct information and facts from health misinformation, critically assess health claims, and recognize underlying, often hidden commercial interests (Stauch et al. 2025). This will empower children and adolescents in their own right and enable them to act more autonomously, independently, and self-determinedly, capable of managing uncertainty and fear more effectively and reducing their susceptibility to propagandist and populist messages—as called for by the Lancet One Health Commission (Winkler et al. 2025).
The structural dimension of health literacy
The structural side of health literacy mirrors the agency aspect by focusing on how health systems and policy environments can make it easier for individuals—in particular those with low resources—to act on health information and receive the services they need by serving the user demand perspective. This paradigm of health literacy is linked to health equity thinking and suggests planning and implementing structural and upstream health-promoting and preventive interventions to create health literacy−friendly, −supportive, and −responsive environments (Parker and Ratzan 2010, Kickbusch et al. 2013, Kirchhoff et al. 2025). Effective policy and system-level interventions can ensure the creation of user-centric settings and structures to enable people to navigate environments (healthcare and information systems) more easily, access care services, choose between care options, and engage in overall healthy behaviours so that these actions are not solely dependent on the individual's skill, behaviour, or responsibility (Parker and Ratzan 2010, Kickbusch et al. 2013, Sørensen et al. 2021). This may include addressing several avenues for improvement, among which are making health information more accessible and actionable through clear, culturally appropriate health communication programmes and redesigning healthcare and information systems to reduce complexity and support informed decision-making (Brach et al. 2012, Sørensen et al. 2021). The exact design will depend on the cultural and geographical context and might also be fundamentally different between LMICs and high-income countries (HICs). Further strategies to tackle the structural dimension of health literacy include harnessing the potential that lies in developing health-literate organizations and programmes to train highly skilled workforces in (public) health and education (Brach et al. 2012, Kickbusch et al. 2013, Sørensen et al. 2021, Kirchhoff et al. 2025). This approach has been included in the WHO definition of health literacy, highlighting that health literacy is ‘mediated by the organisational structures and availability of resources’ (Nutbeam and Muscat 2021). In addition, sustaining needs-based and equity-driven health literacy programmes will also require engaging the public, private, and community sectors in coordinated policy developments and multi-sectoral partnerships (Kickbusch et al. 2013 , Sørensen et al. 2021), also reflected well by the Lancet One Health Commission (Winkler et al. 2025). This strategy draws on socioecological and health promotion assumptions (e.g. settings, contexts, environments, and ‘Health in All Policies’), which are connected to ensuring that health literacy capacities are developed and supported across different sectors of society (Kickbusch et al. 2013) and in relation to planetary and one health (Jochem et al. 2025).
A socioecological lens to school health literacy in the context of the One Health agenda
While the agency approach to health literacy may support the One Health education framework to teach children One Health knowledge and skills (Winkler et al. 2025), it will need the structural health literacy framework to effectively contribute to the socioecological health promotion thinking and institutionalization of society-wide implementation as endorsed by the Lancet One Health Commission. Transformative systemic change and sustained efforts in education will require a whole-of-school implementation plan, informed by key organizational development theories and concepts, which have guided the development of the Health-Literate School (HeLit-School) framework. Incorporating the organizational health literacy model (Brach et al. 2012) and synergetic to the WHO Health Promoting School (HPS) framework (World Health Organization and UNESCO 2021), HeLit-School represents the setting approach to promote health literacy and create a supportive school environment. HeLit-School provides eight interconnected standards, each including six measurable indicators, to support the school setting to develop into a health-literate school (Kirchhoff et al. 2025). HeLit-School addresses four target points in the socioecological environment of the school, including schoolchildren, teachers and staff, school principals, and the wider school environment. The framework can be utilized to strategically guide comprehensive One Health literacy school interventions (Table 1), while the HeLit-School standards and indicators also reflect the five levels of influence of the socioecological model (Golden and Earp 2012). For the implementation of socioecological school interventions, the school principal is a key influential authority to enable health activities in the school setting. Principals with higher levels of health literacy implement school health promotion programmes more frequently (Dadaczynski et al. 2020, Betschart et al. 2022, Meyer et al. 2025), positioning them as a key intervention target at the structural level, where system-level influences on child/adolescent health outcomes and health literacy are addressed indirectly. However, the available resources, more precisely, financial, personnel, and time resources, represent a primary success factor for any school health activity (Kirchhoff et al. 2025), which is why school health literacy programmes must be underpinned by binding legislative and fiscal policies to be effective in the long term.
This integrated expansion of the HeLit-School framework is aligned with the One Health principles but expands the suggested education framework of the Lancet One Health Commission to support a holistic, socioecological school health literacy framework, encouraging schoolchildren, teachers, staff, principals, parents, and educational administrators and policymakers to understand and act on the interconnected determinants of One Health in their communities and beyond. Standards 4 and 5 of the HeLit-School framework already address several aspects of the Commission’s Recommendation 9 to achieve a One Health−literate global citizenry (Winkler et al. 2025). In the report, these standards are especially reflected by One Health literacy ‘[…] must be mainstreamed within all levels of preschooling and primary and secondary schooling’, ‘One Health literacy implies building capabilities and capacity among the younger generation’ (Recommendations 9B and 9C, p. 51), and ‘One Health literacy entails professional lifelong learning and development’ (Recommendation 9D, p. 51; Winkler et al. 2025). The remaining HeLit-School standards go beyond these elements and introduce multiple new dimensions across the socioecological spectrum by which the One Health goals, e.g. socioecological transformation, health-promoting synergies, and social and environmental determinants of health, could be supported more effectively. When situating the HeLit-School framework and One Health within the socioecological model, they can be merged and examined across the five levels of socioecological influence: individual, interpersonal, organizational/institutional, community, and policy/structural levels (Fig. 1; Golden and Earp 2012).
One Health integrated into the HeLit-school framework and embedded in the socioecological model. The four squares depict four levels of influence as suggested by the socioecological model (individual, interpersonal, community, and organizational). Those influences occur and are located directly at the school setting. They are embedded in the wider societal structures where policies and legislations (the fifth level of influence) shape funding, investment, support, and commitment to education. The policy and structural level of influence shapes whether activities can be implemented at school, meaning that the other four levels of influence are highly dependent on the directions and strategies set out at the policy and structural level.
While the HeLit-School framework was developed especially with German schools in mind, and in collaboration with German and Austrian research, practice, and policy experts from education, public health, and medicine, the integral framework indicators (Kirchhoff et al. 2025) might need to be adapted to meet needs, norms, requirements, standards, and languages available in LMICs (Table 2). The implementation of the HeLit-School framework has to consider several aspects that may support the success of the programme (World Health Organization 2021), including whole-school anchoring of health literacy, policy support, committed school leadership, cross-sector networks, alignment with existing HPS structures (Dadaczynski et al. 2020, Schulenkorf et al. 2021, Meyer et al. 2025 ), and the use of self-assessment instruments such as the Organisational Health Literacy of Schools Questionnaire (OHLS-Q) (Kirchhoff et al. 2025). At the same time, typical challenges, including competing curricular priorities, limited resources, the need for sustained leadership and professional development, lack of time, fragmented responsibilities, and insufficient monitoring mechanisms (Okan et al. 2020b, World Health Organization 2021), should be carefully considered before transferring and adapting the framework to LMIC contexts. Especially, teaching content for health literacy learning materials will need to be carefully revised, modified, and also adapted to culturally fit the LMIC context. Nevertheless, the general multi-level standard-based approach of the HeLit-School framework may remain and serve as a structural foundation to deliver a whole-of-school intervention rather than an individual-level intervention.
Conclusion
The HeLit-School framework becomes an incubator to promote aspects of One Health as a whole-of-school approach, aiming at influencing the next generation to become One Health advocates and champions. However, in order to achieve this goal, this viewpoint has shown that schools themselves need to be ‘influenced’ on their structural levels, which can only be achieved if governments value them and their mandate for education by guaranteeing continuous funding and including health and education in all policies. Investing in education is a core requirement for any sustainable strategy to promote Global Health and One Health. While the former focuses on improving health equity and addressing widespread health challenges worldwide, the latter recognizes the interconnectedness of human, animal, plant, and ecosystem health and is firmly based on the One Health ethics as described in the Introduction. Health literacy connects both concepts by its integral socioecological lens to address these problems in a highly information-based and -saturated 21st century world. Health literacy strategies in general, and especially when implemented early in schools in both LMICs and HICs, can contribute to achieving the goals of Global Health and One Health. However, this will require shifting from a behavioural to a systemic perspective, which organically includes human behaviour, and moving beyond the sole individual focus towards adopting a socioecological perspective, in particular at school. While individuals may have the responsibility for engaging with their health and well-being, only systems and policymakers can establish enabling and supportive environments and sustainable health and education policies. The flourishing of health literacy within the socioecological environment not only enables its full potential and maximizes its impact but also represents a clear added value if adapted systematically to Global Health and One Health strategies. Ahead of the 40th anniversary of the Ottawa Charter for Health Promotion in 2026, it is worth to recite the then Director General of the WHO, Dr Halfdan Mahler, who urged to ‘recognize health and its maintenance as a major social investment that is part of the overall process of social learning and support health literacy as a major aspect of personal learning and development’ (Mahler 1986, p. 411). The report of the Lancet One Health Commission represents a paradigm shift through the adoption of key health promotion principles, grounded in interdisciplinary and multi-sectoral, (socio)ecological, and equity-driven frameworks. Taking into account the convergence of human, animal, and environmental factors, the Ottawa Charter's mandate to implement a ‘new public health’ is being revived. Long-term investment in health literacy will support the agendas of Global Health and One Health and contribute to tackling challenges across the health spectrum in this age of new public health.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abel T, Benkert R. Critical health literacy: reflection and action for health. Health Promot Int 2022;37:2022. 10.1093/heapro/daac 114 · doi ↗
- 2Baird S, Choonara S, Azzopardi PS et al A call to action: the second Lancet Commission on adolescent health and wellbeing. Lancet 2025;405:1945–2022. 10.1016/S 0140-6736(25)00503-340409329 · doi ↗ · pubmed ↗
- 3Betschart S, Sandmeier A, Skedsmo G et al The importance of school leaders’ attitudes and health literacy to the implementation of a health-promoting schools approach. Int J Environ Res Public Health 2022;19:14829. 10.3390/ijerph 19221482936429547 PMC 9690102 · doi ↗ · pubmed ↗
- 4Blankart CR, Gani SM, de Crimlisk H et al Health literacy, governance and systems leadership contribute to the implementation of the One Health approach: a virtuous circle. Health Policy 2024;143:105042. 10.1016/j.healthpol.2024.10504238518391 · doi ↗ · pubmed ↗
- 5Brach C, Keller D, Hernandez LM et al Ten attributes of health literate health care organizations. 2012. https://nam.edu/perspectives-2012-ten-attributes-of-health-literate-health-care-organizations/ (7 August 2025, date last accessed).
- 6Dadaczynski K, Rathmann K, Hering T et al The role of school leaders’ health literacy for the implementation of health promoting schools. Int J Environ Res Public Health 2020;17:1855. 10.3390/ijerph 1706185532178457 PMC 7142764 · doi ↗ · pubmed ↗
- 7Donkin A, Goldblatt P, Allen J et al Global action on the social determinants of health. BMJ Glob Health 2018;3:e 000603. 10.1136/bmjgh-2017-000603 · doi ↗
- 8Fleary SA, Joseph P, Pappagianopoulos JE. Adolescent health literacy and health behaviors: a systematic review. J Adolesc 2018;62:116–27. 10.1016/j.adolescence.2017.11.01029179126 · doi ↗ · pubmed ↗