Greater adherence to the Planetary Health Diet is inversely associated with dyslipidemia in children: PASE Study—Brazil
Érica Priulli, Mariana de Santis Filgueiras, Dayane de Castro Morais, Bruna Clemente Cota, Juliana Farias de Novaes

TL;DR
A study in Brazil found that children who followed a healthy, sustainable diet called the Planetary Health Diet had lower cholesterol and fewer heart disease risks.
Contribution
This is the first study to show a link between the Planetary Health Diet and reduced dyslipidemia in children.
Findings
Higher adherence to the Planetary Health Diet was linked to lower total cholesterol and LDL cholesterol in children.
Children with greater diet adherence had fewer altered lipid markers, indicating better heart health.
The diet was associated with higher fiber and carbohydrate intake and lower saturated fat and calorie consumption.
Abstract
Healthy and sustainable diets, such as the Planetary Health Diet (PHD), may contribute to the prevention and control of cardiovascular disease (CVD). However, there is a lack of evidence on this relationship in childhood. This study assessed the association between adherence to the PHD and lipid markers in children. Cross-sectional study with a representative sample of 378 children aged 8 and 9 in Viçosa, Minas Gerais, Brazil. The food consumption was assessed using three 24-h dietary recalls and the adherence to the PHD was measured through the Planetary Health Diet Index (PHDI). Dyslipidemia was defined by the presence of one or more altered lipid markers (total cholesterol—TC, triglycerides—TG, low-density lipoprotein—LDL-c, and high-density lipoprotein—HDL-c). Associations between PHDI and lipid outcomes were assessed using adjusted linear regression models. The mean PHDI was 37.5…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
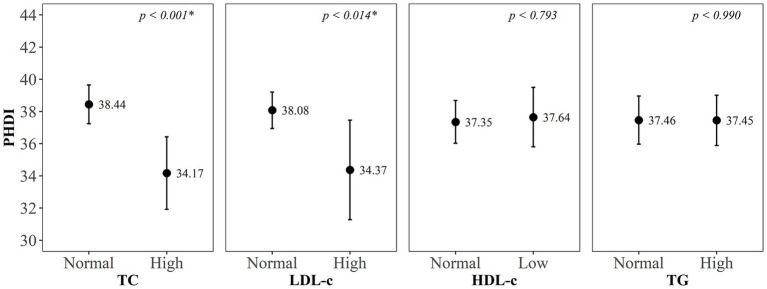 Figure 1
Figure 1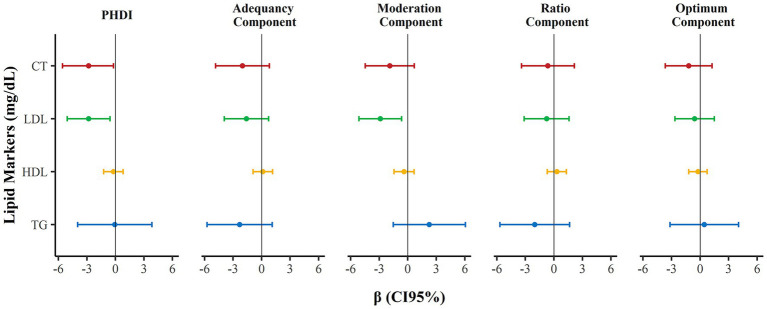 Figure 2
Figure 2| Variable | PHDI terciles | |||
|---|---|---|---|---|
| 1st ( | 2nd ( | 3rd ( | ||
| PHDI total score | 26.00 (5.57) | 37.70 (2.53) | 48.64 (6.45) | |
| Sex¶ | ||||
| Male | 71 (39.23%) | 54 (29.83%) | 56 (30.94%) | 0.064 |
| Female | 55 (27.92%) | 72 (36.55%) | 70 (35.53%) | |
| Skin color¶ | ||||
| White | 42 (35.29%) | 42 (35.29%) | 35 (29.42%) | 0.838 |
| Brown | 72 (34.12%) | 67 (31.76%) | 72 (34.12%) | |
| Black | 11 (25.58%) | 15 (34.88%) | 17 (39.54%) | |
| Asian | 1 (20.00%) | 2 (40.00%) | 3 (40.00%) | |
| Screen time (hours/day)¶ | ||||
| ≤2 | 59 (29.80%) | 71 (35.86%) | 68 (34.34%) | 0.289 |
| >2 | 67 (37.22%) | 55 (30.56) | 58 (32.22%) | |
| Height-for-age ( | 0.48 (1.04) | 0.64 (1.07) | 0.51 (0.99) | 0.619 |
| BMI-for-age ( | 0.28 (1.36) | 0.48 (1.46) | 0.46 (1.40) | 0.534 |
| % BF‡ | 22.42 (9.68) | 25.63 (10.64) | 24.57 (9.71) | 0.196 |
| TC (mg/dL)‡ | 152.24 (28.67) | 156.18 (26.36) | 148.50 (23.57) | 0.055 |
| LDL-c (mg/dL)‡ | 86.67 (23.57) | 90.20 (23.55) | 84.03 (22.80) |
|
| HDL-c (mg/dL)‡ | 50.62 (10.58) | 50.53 (10.09) | 49.07 (9.27) | 0.368 |
| TG (mg/dL)‡ | 77.08 (31.09) | 81.90 (39.26) | 77.52 (35.53) | 0.721 |
| Family history of dyslipidemia¶ | ||||
| No | 96 (34.66%) | 89 (32.13%) | 92 (33.21%) | 0.796 |
| Yes | 30 (29.70%) | 37 (36.64%) | 34 (33.66%) | |
| PHDI and its components | Maximum score | Number of dyslipidemia markers | ||||||
|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | Per 1 SD‡ | p-trend | ||
| PHDI total score | 150 | 38.86 (10.46) | 37.18 (10.35) | 37.96 (10.16) | 33.90 (11.60) | 34.31 (12.73) |
|
|
| Adequacy component | 50 | 16.95 (4.79) | 15.72 (4.81) | 16.06 (5.10) | 14.55 (5.40) | 14.74 (5.92) |
|
|
| Ratio component | 10 | 4.38 (2.35) | 4.08 (2.20) | 4.11 (2.37) | 3.80 (2.46) | 2.70 (2.70) |
|
|
| Moderation component | 40 | 5.23 (5.54) | 5.85 (5.79) | 5.57 (5.63) | 4.64 (5.47) | 5.07 (5.61) | −0.04 (−0.13; 0.06) | 0.484 |
| Optimum component | 50 | 12.29 (6.90) | 11.54 (5.80) | 12.22 (6.07) | 10.40 (5.82) | 11.80 (6.78) | −0.03 (−0.14; 0.07) | 0.542 |
| Nutrients* | PHDI terciles (mean and standard deviation) | Per 1 SD | p-trend | ||
|---|---|---|---|---|---|
| 1st (26.00 ± 5.57) | 2nd (37.70 ± 2.53) | 3rd (48.64 ± 6.45) | |||
| Energy (kcal) | 1644.42 (401.66) | 1628.44 (447.46) | 1542.35 (385.99) |
|
|
| Carbohydrate (g) | 141.32 (18.07) | 144.37 (16.67) | 148.49 (16.62) |
|
|
| Fiber (g) | 8.93 (2.94) | 10.44 (3.04) | 12.11 (4.21) |
|
|
| Protein (g) | 36.84 (10.65) | 35.63 (8.66) | 35.85 (7.33) | −0.03 (−1.07; 1.01) | 0.955 |
| Total fat (g) | 44.27 (25.49) | 39.53 (13.47) | 35.88 (14.96) | −2.34 (−5.11; 0.42) | 0.096 |
| SFA (g) | 15.35 (5.24) | 13.24 (3.32) | 11.95 (3.55) |
|
|
| MUFA (g) | 13.08 (6.80) | 11.90 (3.85) | 10.73 (4.12) | −0.63 (−1.37; 0.11) | 0.097 |
| PUFA (g) | 11.18 (13.39) | 10.37 (7.03) | 9.54 (7.86) | 0.03 (−1.41; 1.47) | 0.965 |
| Trans fat (g) | 1.17 (0.67) | 0.98 (0.66) | 0.99 (0.62) | −0.05 (−0.11; 0.01) | 0.134 |
| Cholesterol (mg) | 195.13 (108.38) | 154.54 (70.14) | 130.79 (67.56) |
|
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAgriculture Sustainability and Environmental Impact · Nutritional Studies and Diet · Antioxidant Activity and Oxidative Stress
Introduction
1
Dyslipidemia in childhood, characterized by elevated concentrations of total cholesterol (TC), triglycerides (TG), low-density lipoprotein (LDL-c) and/or reduced concentrations of high-density lipoprotein (HDL-c) (1), is associated with the early development of atherosclerotic lesions (2), persisting into adulthood (3). In Brazil, the prevalence of dyslipidemia is high, affecting around 70% of children (4) and 78.2% of adolescents (5).
Historically, the dietary management of dyslipidemia emphasized specific nutrients, such as saturated fat and fiber, as well as isolated foods. In recent years, sustainable dietary patterns have been recognized as effective strategies in the prevention and treatment of dyslipidemia and cardiovascular disease (CVD) (6). Within this framework, a sustainable diet pattern offers additional benefits, contributing to the reduction of malnutrition, chronic diseases and the impacts of climate change on human health (7).
In 2019, the co-occurrence and interaction of obesity (including other chronic non-communicable diseases), undernutrition and climate change were described as Global Syndemic, highlighting the required integrated actions to address the common drivers of these three public health challenges (8). Therefore, the EAT-Lancet commission report proposed the Planetary Health Diet (PHD), a dietary pattern that prioritizes plant-based and whole foods, and limits the consumption of animal-based foods and added sugar (7).
Although evidence in adolescents and adults indicates that greater adherence to PHD is associated with lower TC concentrations (9, 10) and reduced risk of CVD mortality (11), there is a lack of studies evaluating this relationship in childhood. In this context, this study aimed to evaluate the association between adherence to PHD and lipid markers in children. The hypothesis is that greater adherence to PHD is inversely associated with dyslipidemia in childhood.
Materials and methods
2
Study design and participants
2.1
This is a cross-sectional study of the “Schoolchildren Health Assessment Survey” (PASE, in Portuguese) that aimed to assess the cardiometabolic risk and its associated factors in children from Viçosa, Minas Gerais, Brazil. In 2015, a random sample of 378 children aged 8 and 9 years old was selected, representative according to age and sex, from a total of 1,464 children in this age group enrolled in all public (n = 17) and private (n = 7) urban schools in the municipality. Viçosa is a city of approximately 72,000 inhabitants, located 227 km from Belo Horizonte, capital of Minas Gerais. Children with health conditions that affected nutritional status or body composition, those chronically using medications that interfered with glucose and/or lipid metabolism, and cases without successful contact with guardians after three attempts were not included in the study.
This study was conducted according to the guidelines established in the Declaration of Helsinki and approved by the Human Research Ethics Committee of the Universidade Federal de Viçosa (n° 663.171/2014). All guardians signed the Informed Consent Form.
Data collection
2.2
The information of sex, age, skin color, screen time (hours/day), per capita household income and family history of dyslipidemia was collected through a semi-structured questionnaire applied to parents or guardians. The skin color of participants was self-reported and categorized as White, Brown, Black, or Asian, according to Brazilian Institute of Geography and Statistics (IBGE).
The weight and height were measured to calculate the body mass index for age (BMI-for-age), classified in z-scores according to World Health Organization criteria (12). The body fat percentage was estimated by Dual-Energy X-Ray Absorptiometry (DXA) (Lunar Prodigy, GE Healthcare^®^, Madison, USA).
Food consumption
2.3
The food consumption was assessed using the average of three 24-h dietary recalls (R24h), applied two on weekdays and one at the weekend, with a minimal interval of 15 days between them. The interviews were conducted with the children, in the presence of their guardians, with the help of household utensils and a photo album (13) to facilitate the accuracy of food portion estimates. The Brazilian Food Composition Table, version 7.0 (14), was used to quantify nutrients. The TBCA was developed in accordance with the guidelines of the International Network of Food Data Systems (INFOODS). For recipe breakdown, we used a database containing nutritional composition and standardized Brazilian recipes, according to the TBCA (14).
The food consumption data were entered into the Diet Pro^®^ 5i software, version 5.8 (DIET PRO, 1997) and later exported to a Microsoft Excel^®^ spreadsheet (Microsoft Corp., Redmond, USA). The link to the Brazilian Food Composition Table (TBCA, in Portuguese) version 7.0 (14) was performed using the extensions of Power Query (15) and Visual Basic for Applications (16). All nutrients were presented by total caloric intake using the energy density method, expressed in grams or milligrams per 1,000 Kcal.
Planetary Health Diet Index
2.4
The Planetary Health Diet Index (PHDI) is a validated Brazilian instrument to assess adherence to the Planetary Health Diet (PHD) recommendations (17). First, all mixed dishes and processed foods were disaggregated into their basic ingredients using a Brazilian database of standard recipes. For highly processed products that are mainly composed of a single base ingredient, such as those made primarily from maize starch or wheat flour, the energy contribution of these ingredients was estimated based on their fat and added sugar content. This procedure was applied to most processed products, except for processed meats, which were categorized based on their main ingredient or commonly marketed formulation into the respective groups of red meat (e.g., sausage, ham, and salami) or chicken and substitutes (e.g., nuggets) (17).
The PHDI scores were calculated following the method described by Cacau et al. (17). The PHDI uses cutoff points based on energy intake to calculate the score for 16 food groups, organized into four components: 1) Adequacy (nuts and peanuts, legumes, fruits, vegetables and whole cereals), 2) Moderation (red meat, chicken and substitutes, animal fats and added sugars), 3) Ratio (ratio of the dark green vegetables, and red and orange vegetables to total vegetables), and 4) Optimum (eggs, dairy, fish and seafood, tubers and potatoes, and vegetable oils). After classifying the foods, the percentage of caloric contribution for each group was calculated (group calories ÷ total calories consumed on the day × 100). The Adequacy, Moderation and Optimum components can each reach up to 10 points, while the Ratio component reaches a maximum of 5 points, resulting in a total score from 0 to 150, with higher values indicating greater adherence. The details of the cutoff points and scoring criteria were previously described by the authors who developed and validated the PHDI in Brazil (17).
Lipid markers
2.5
The dyslipidemia was defined by the presence of one or more of the following altered parameters, according to Faludi (1): TC ≥ 170 mg/dL, LDL-c ≥ 110 mg/dL, TG ≥ 75 mg/dL and HDL-c < 45 mg/dL. The sum of the altered markers was classified on a scale from zero (no alterations) to four (presence of all alterations).
Blood samples were collected after 12 h of fasting at the Clinical Analysis Laboratory of the Health Division of the Universidade Federal de Viçosa and stored at −80 °C until analysis. The lipid markers were measured in serum using an automatic analyzer (BioSystems 200 Mindray^®^, Nanchang, China) and Bioclin^®^ reagent (Belo Horizonte, Brazil), following the manufacturer’s recommendations.
Data analysis
2.6
- Exposure: Total score of the Planetary Health Diet Index (PHDI) and its components (Adequacy, Moderation, Ratio and Optimum).
- Outcome: Presence and number of altered lipid markers (dyslipidemia).
- Covariates: Age, sex, per capita household income, skin color, body fat percentage, total caloric intake, screen time, and family history of dyslipidemia.
The PHDI score and its components were analyzed as continuous variables and presented as mean and standard deviation (SD). In the descriptive analysis, the means (SD) or absolute and relative frequencies (n, %) were calculated for each variable, according to the PHDI terciles. Pearson’s chi-square test and linear regression were used to analyze proportions or means, respectively.
Student’s t-test was used to compare the means of PHDI according to lipid markers, classified as normal or high/low. Linear regression models were used to estimate associations between the PHDI (and its components) and lipid markers, as well as with energy and nutrient intake. The adjustment variables were selected based on the literature (4, 17, 18). Statistical analyses were carried out using Stata^®^ 17.0 software. Figures were created using R software version 4.3.2 (R Core Team, 2024) and ggplot2 package. The significance level considered was 5%.
Results
3
This study included 378 children with a mean age of 8.5 years [Standard Deviation (SD) = 0.5] and a mean per capita income of US$ 234.28 (SD = 267.48). The mean of PHDI score was 37.45 (SD: 10.58) points. An inverse association was observed between PHDI and LDL-c concentrations (p-trend = 0.039) (Table 1).
We observed that 70% of the children (n = 263) presented dyslipidemia. The prevalence of high TC, LDL-c and TG, and low HDL-c, were, respectively, 23.1, 15.4, 47.2, and 35.0% (Supplementary Figure S1). The mean PHDI scores were lower in children with elevated TC and LDL-c, when compared to those with normal values of these markers (Figure 1).
Means and standard deviations of the Planetary Health Diet Index (PHDI) score according to markers of dyslipidemia in children (Viçosa, Minas Gerais, Brazil, 2015–2016). TC, total cholesterol; LDL-c, low-density lipoprotein; HDL-c, high-density lipoprotein; TG, triglycerides. Student’s t-test (p < 0.05).*
For each increase of one standard deviation in the PHDI, reductions were identified in the concentrations of TC (β = −2.81, 95% CI: −5.57; −0.05, p-trend = 0.046) and LDL-c (β = −2.81, 95% CI: −5.07; −0.56, p-trend = 0.015). Additionally, each increase of one standard deviation in the Moderation component of the PHDI was associated with a reduction in LDL-c (β = −2.88, 95% CI: −5.13; −0.64, p-trend = 0.012). These associations were not found for HDL-c and TG (Figure 2).
Association of the Planetary Health Diet Index (PHDI) and its components (adequacy, moderation, ratio and optimum) with markers of dyslipidemia in children (Viçosa, Minas Gerais, Brazil, 2015–2016). Linear regression with PHDI and its components as exposure and markers of dyslipidemia as outcome. Adjustment for age, sex, per capita household income, skin color, body fat percentage, total caloric intake, screen time, and family history of dyslipidemia. Robust variance estimates were specified in all models (p < 0.05).
The total PHDI score (β = −0.15, 95% CI: −0.26; −0.04), the Adequacy component (β = −0.16, 95% CI: −0.27; −0.06), and the Ratio component (β = −0.15, 95% CI: −0.25; −0.04) were inversely associated with the highest number of dyslipidemia markers (Table 2).
In addition, a higher PHDI score was associated with lower consumption of total calories (β = −47.76; 95% CI: −86.20; −9.32), saturated fat (β = −1.37; 95% CI: −1.95; −0.80) and cholesterol (β = −24.58; 95% CI: −36.02; −13.14). On the other hand, positive associations were observed between PHDI and consumption of carbohydrates (β = 3.11; 95% CI: 1.09, 5.13) and fibers (β = 1.67; 95% CI: 1.25, 2.09) (Table 3).
Discussion
4
This study confirms the hypothesis that children with higher adherence to PHDI presented lower serum concentrations of TC and LDL-c, and low number of altered lipid markers. These results reinforce that a more sustainable diet can also benefit cardiovascular health in childhood.
Our findings are consistent with the multicenter study “Healthy Lifestyle in Europe by Nutrition in Adolescents” (HELENA), which demonstrated an association between higher PHDI scores and lower probability of hypercholesterolemia in European adolescents (10). Similarly to our study, in another investigation developed with Brazilian adults (9), no significant associations were found of PHDI with serum TG and HDL-c concentrations. Contrasting with our findings, in the “National Health and Nutrition Examination Survey” (NHANES 2015–2018) with adults from the United States (≥20 years), the adherence to the PHD was associated with lower TG and higher HDL-c levels (19). Therefore, although the PHD contributes to a lower atherogenic risk, its influence on the lipid profile may differ according to age and geographic region.
Moreover, we found high prevalence of dyslipidemia in our sample (70%) and this finding is consistent with other study involving Brazilian adolescents (78.2%) (5) and children aged 2 to 9 years old (68,4%) (20), although different cutoff points were used to classify the lipid markers (1). Diet and physical inactivity are the main causes of dyslipidemia in childhood, except for cases of genetic dyslipidemia, which require a specific approach (1). In our sample, we identified that 27% of the participants had a family history of dyslipidemia and 48% presented sedentary behavior, demonstrated by screen time exceeding 2 h per day. Furthermore, the children presented high consumption of ultra-processed foods (21) and low PHDI score.
We observed that the total PHDI score, as well as its Adequacy and Ratio components, were associated with lower number of altered lipid markers, while the Moderation component showed an inverse association with LDL-c. The Adequacy component reflects greater consumption of foods that promote health and sustainability, such as fruits, vegetables, whole grains, legumes and nuts and peanuts. The Ratio component assesses the proportion of dark green vegetables and red-orange vegetables in relation to the total vegetables consumed, an indicator linked to the diversity and quality of the diet (17). Furthermore, the Moderation component, which presents an inverse score, reflects a lower quality and sustainability of diets, being composed of red meat, chicken and substitutes, animal fats and added sugars (17).
In this context, the benefits of higher PHDI scores and the Adequacy and Ratio components can be attributed to the higher intake of fiber, micronutrients, bioactive compounds and unsaturated fatty acids present in the predominant foods in these groups (6), in addition to the lower intake of animal fats and sugars, present in the foods in the Moderation group (17). In other previous study, our research group found that the inflammatory diet (rich in ultra-processed foods) was associated with atherogenic profile in children, confirming that the unhealthy diet can contribute to the worsening of lipid markers (4, 21).
The benefits of a sustainable diet for improved TC and LDL-c parameters may be explained by the inverse association between PHDI and intake of saturated fatty acids and cholesterol, as well as the positive association between PHDI and fiber intake, as demonstrated in this study. These findings are consistent with other study conducted with Brazilian adults, in which greater adherence to the PHDI was associated with similar nutritional profiles (17).
Furthermore, observational studies have indicated that the PHD, characterized by a high intake of fiber, unsaturated fats, fruits, and vegetables, was associated with lower risk of mortality from cardiovascular diseases (11), and better clinical conditions, including lower BMI, waist circumference (22), blood pressure, TC (9, 10), LDL-c, non–HDL-cholesterol (9), and triglycerides, as well as higher HDL-c levels (19). In contrast, a diet characterized by the Western dietary pattern, rich in highly processed, refined foods, red and processed meats, added sugars and saturated and trans fats, in addition to low consumption of fruits, vegetables, whole grains and nuts, has been associated with higher serum concentrations of LDL-c and inflammatory markers, and lower HDL-c, contributing to the development of the atherosclerotic process (23).
The greater adherence to the Mediterranean diet has beneficial effects on TC, LDL-C, HDL-C, and TG in childhood, as demonstrated by meta-analysis of intervention studies (24); in addition, the PHDI was positively associated with this dietary pattern (25). These results underscore the importance of adhering to a healthy diet, which, although not widely followed in many regions (26, 27), is crucial for cardiovascular health. Additionally, the PHDI was positively associated with the Diet Quality Index – Revised for the Brazilian population (IQD-R) and inversely associated with estimated dietary greenhouse gas emissions (17) and ultra-processed food consumption (28). These findings emphasize the relevance of considering sustainability in dietary guidelines, promoting benefits for human and planetary health.
This study has some limitations. The PHDI was developed and validated for Brazilian adults, and its application to children requires specific validation. However, its formula based on percentages of total caloric value allows it to be adapted to different age groups. Thus, considering the recent approach of the PHD and the scarcity of studies in children, this investigation contributes to demonstrating the possible benefits of the PHD in the prevention of childhood dyslipidemia, reinforcing the need for new validation studies of this index for the pediatric public. In addition, the cross-sectional design prevents the inference of causal relationships between the variables.
Positive aspects of this study include the use of three 24-h recalls, supported by a photo album to better estimate portion sizes, and the use of a Brazilian database to standardize the breakdown of recipes and classification of the PHDI food groups (14). In addition, the statistical analyses were adjusted for potential confounding factors.
Finally, although the associations between PHDI and markers of dyslipidemia appear small, they may have clinical relevance. A meta-analysis suggested that a reduction of approximately 1 mmol/L (≈38.7 mg/dL) in LDL-C was associated with a 19% reduction in major cardiovascular events (29). In this context, considering that a 1 standard deviation increase in PHDI was associated with a − 2.8 mg/dL reduction in both TC and LDL-C in our sample, a lower cardiometabolic risk is expected over time with higher adherence.
Conclusion
5
We conclude that the greater adherence to PHD was associated with better lipid profile, including lower serum concentrations of TC and LDL-c and a lower number of dyslipidemia markers in children. These findings reinforce the role of sustainability-based dietary guidelines in promoting cardiovascular health from childhood. Longitudinal studies are essential to clarify causal relationships between higher adherence to PHD and the prevention of dyslipidemia in pediatric populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Faludi AA Izar MC d O Saraiva JFK Chacra APM Bianco HT Neto AA . Atualização da Diretriz Brasileira de Dislipidemias e Prevenção da Aterosclerose – 2017. Arq Bras Cardiol. (2017) 109:1–76. doi: 10.5935/abc.2017012128813069 · doi ↗ · pubmed ↗
- 2Berenson GS Srinivasan SR Bao W Newman WP Tracy RE Wattigney WA. Association between multiple cardiovascular risk factors and atherosclerosis in children and young adults. N Engl J Med. (1998) 338:1650–6. doi: 10.1056/nejm 199806043382302, 9614255 · doi ↗ · pubmed ↗
- 3Raitakari O Pahkala K Magnussen CG. Prevention of atherosclerosis from childhood. Nat Rev Cardiol. (2022) 19:543–54. doi: 10.1038/s 41569-021-00647-9, 34987194 · doi ↗ · pubmed ↗
- 4Suhett LG Vieira Ribeiro SA Hermsdorff HHM Silva MA Shivappa N Hébert JR . Dietary inflammatory index scores are associated with atherogenic risk in Brazilian schoolchildren. Public Health Nutr. (2021) 24:6191–200. doi: 10.1017/S 1368980021001816, 33902777 PMC 11148590 · doi ↗ · pubmed ↗
- 5Faria Neto JR Bento VFR Baena CP Olandoski M Gonçalves LG d O Abreu G d A . ERICA: prevalence of dyslipidemia in Brazilian adolescents. Rev Saude Publica. (2016) 50:10s. doi: 10.1590/S 01518-8787.2016050006723 PMC 476704126910544 · doi ↗ · pubmed ↗
- 6Trautwein EA Mc Kay S. The role of specific components of a plant-based diet in management of dyslipidemia and the impact on cardiovascular risk. Nutrients. (2020) 12:2671. doi: 10.3390/nu 12092671, 32883047 PMC 7551487 · doi ↗ · pubmed ↗
- 7Willett W Rockström J Loken B Springmann M Lang T Vermeulen S . Food in the anthropocene: the EAT–lancet commission on healthy diets from sustainable food systems. Lancet. (2019) 393:447–92. doi: 10.1016/s 0140-6736(18)31788-4, 30660336 · doi ↗ · pubmed ↗
- 8Swinburn BA Kraak VI Allender S Atkins VJ Baker PI Bogard JR . The Global Syndemic of obesity, undernutrition, and climate change: the lancet commission report. Lancet. (2019) 393:791–846. doi: 10.1016/S 0140-6736(18)32822-8, 30700377 · doi ↗ · pubmed ↗