Presence of Lassa Virus RNA in Cerebrospinal Fluid Indicating Neuroinvasive Lassa Fever in Pediatric Patients From Edo State, Nigeria
Hannah Caroline Sophie Müller, Cyril Oshomah Erameh, Joseph Okoeguale, Sheila Ojor Ileli, Imonifome Frank Onyeke, Adewale Elijah Adetunji, Lilian Omoyemen Akerele, Rita Esumeh, Ebo Benevolence Ohomoime, Mette Hinrichs, Jonas Müller, Ujiagbe Moses Aiterebhe

TL;DR
This study shows that Lassa virus is commonly found in the cerebrospinal fluid of children with Lassa fever and neurological symptoms, suggesting the virus invades the brain.
Contribution
The study provides evidence that Lassa virus frequently invades the central nervous system in pediatric patients and replicates actively there.
Findings
86% of pediatric Lassa fever patients with CNS symptoms had Lassa virus RNA in their cerebrospinal fluid.
Lassa virus RNA concentration was significantly higher in cerebrospinal fluid than in plasma in most patients.
Abstract
Neurological complications of Lassa fever (LF) are associated with fatal outcome. In this study, we aimed to provide further evidence of Lassa virus (LASV) infection of the central nervous system (CNS) by assessing LASV in cerebrospinal fluid (CSF). We retrospectively screened the database of the LF diagnostic unit at Irrua Specialist Teaching Hospital in Nigeria for patients with suspected or confirmed LF who underwent lumbar puncture as part of their routine clinical management due to CNS symptoms and had CSF samples tested by LASV reverse-transcription polymerase chain reaction (RT-PCR). RT-PCR results for CSF were available for 153 patients, all children. LF was confirmed in 49 of 153 (32%) patients, of whom 42 (86%) were LASV RNA positive in CSF. Of the 42 patients, 33 (79%) were LASV RNA positive in CSF and plasma, whereas 9 (21%) patients were positive in CSF only. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
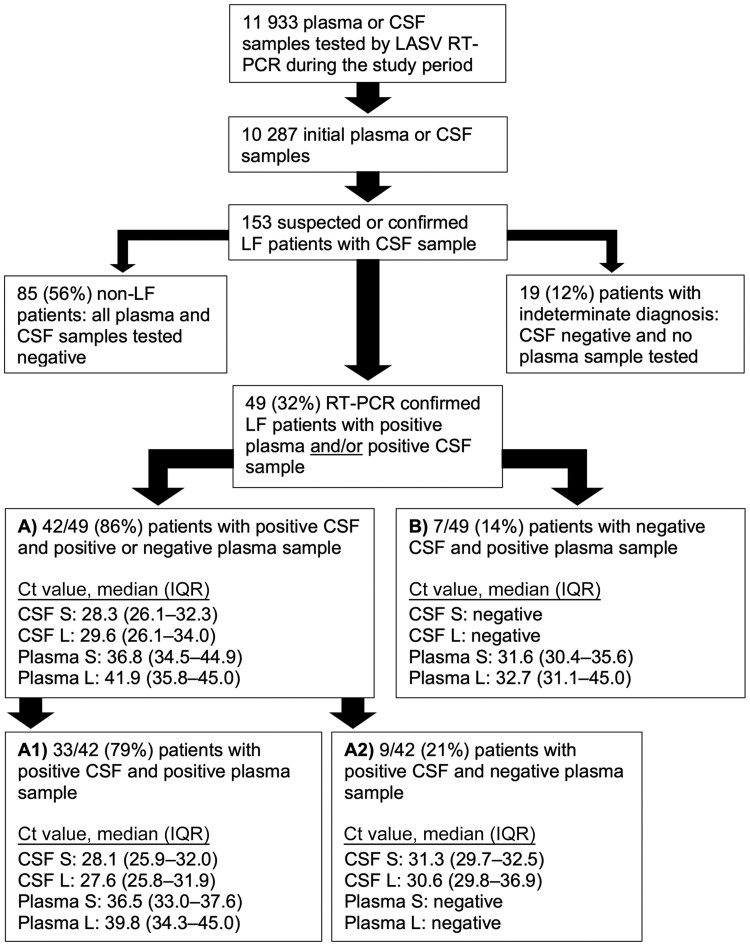 Figure 1
Figure 1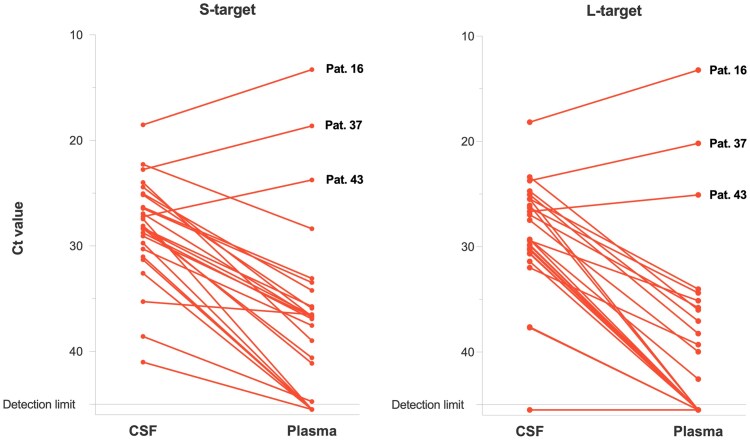 Figure 2
Figure 2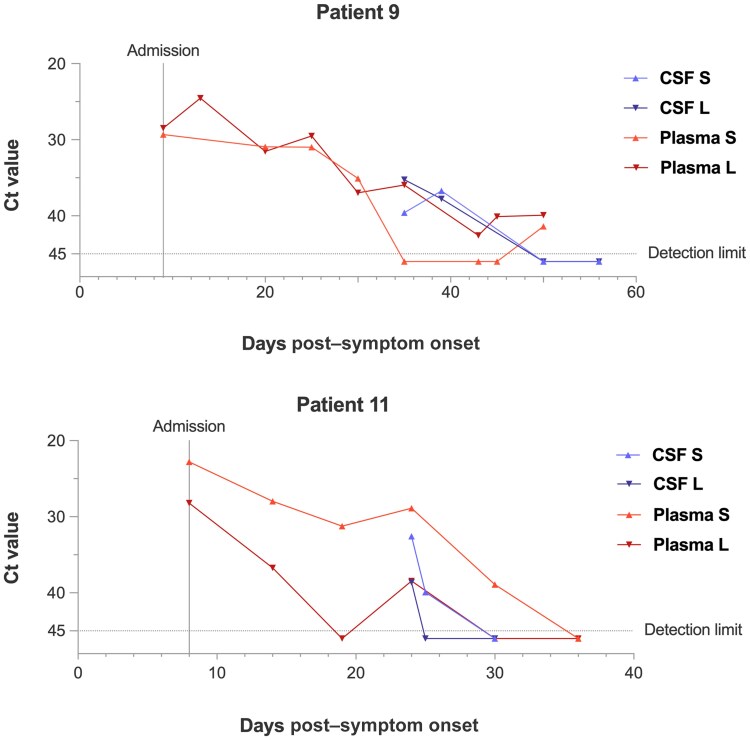 Figure 3
Figure 3| Indications for Lumbar Puncture |
|---|
| Presence of typical signs of meningeal irritation: nuchal rigidity, positive Kerning and Budzinski signs at any age; bulging, tense fontanelle in infants [ |
| Headache and/or photophobia associated with fever in children >3 years of age irrespective of the presence of meningeal signs |
| Irritability and excessive and unconsolable crying in infants and toddlers with fever irrespective of the presence of meningeal signs |
| Febrile status epilepticus |
| Exclusion of meningitis in children <2 y of age with simple or complex febrile convulsions [ |
| Exclusion of meningitis in children aged ≥2 y with complex febrile seizures |
| Exclusion of meningitis in children with alteration of consciousness and fever with or without convulsions [ |
| Exclusion of LF through testing of CSF for LASV in plasma LASV-negative children in whom there is a high suspicion for LF |
| Monitoring of response to LF treatment/appearance of new clinical features during treatment |
| Characteristic | Group A: CSF-Positive LF Patients | Group B: CSF-Negative LF Patients |
| Group C: CSF- and Plasma-Negative Non-LF Patients |
|
|---|---|---|---|---|---|
| Demographic data | |||||
| Sex | |||||
| Female | 18 (43) | 3 (43) | 1 | 37 (44) | .91 |
| Male | 24 (57) | 4 (57) | 48 (56) | ||
| Age, y, median (IQR) | 10.5 (6.3–14) | 13.0 (11.8–14.8) | .38 | 5.0 (1.8–12.3) | .04 |
| Time from symptom onset to CSF PCR, d, median (IQR) | 11.0 (7.0–16.5) | 14.5 (10.8–23.5) | .11 | 4.0 (2.0–9.0) | 1 |
| Clinical characteristics | |||||
| Symptoms on admission | |||||
| Fever | 41 (98) | 7 (100) | 1 | 70 (82) | .01 |
| Headache | 32 (76) | 4 (57) | .41 | 38 (45) | .006 |
| Abdominal pain | 32 (76) | 5 (71) | 1 | 25 (29) | <.0001 |
| Vomiting | 27 (64) | 4 (57) | 1 | 28 (33) | .006 |
| General weakness | 20 (48) | 3 (43) | 1 | 27 (32) | .16 |
| Cough | 11 (26) | 1 (14) | .66 | 15 (18) | .24 |
| Chest or retrosternal pain | 6 (14) | 2 (29) | .58 | 8 (9) | .38 |
| Sore throat | 5 (12) | 1 (14) | .55 | 3 (4) | .35 |
| Bleeding, any type | 4 (10) | 1 (14) | 1 | 1 (1) | .02 |
| Diarrhea | 3 (7) | 2 (29) | .20 | 12 (14) | .55 |
| Seizure | 1 (2) | 2 (29) | .07 | 2 (2) | 1 |
| Dyspnea | 2 (4) | 0 (0) | 1 | 10 (12) | .51 |
| Outcome | |||||
| Death | 3 (7) | 0 (0) | 1 | 4 (5) | .40 |
| Characteristic | CSF | Plasma | CSF – Plasma Difference |
|---|---|---|---|
| All CSF-positive patients (n = 42) | |||
| Time from symptom onset to date of sampling, d | 11.0 (7.0–16.5) | 8.5 (4.3–14.0) | 1.0 (0–2.0) |
| Ct value S-target | 28.3 (26.1–32.3) | 36.8 (34.5–44.9) | −8.2 (−20.8 to −4.5) |
| Ct value L-target | 29.6 (26.1–34.0) | 41.9 (35.8–45.0) | −12.5 (−20.3 to −6.1) |
| Patients with matched CSF and plasma pairs (n = 26) | |||
| Time from symptom onset to date of sampling, d | 10.5 (8.8–15.0) | 10.0 (8.0–14.0) | 0 (0–1.0) |
| Ct value S-target | 28.2 (25.4–30.1) | 36.7 (34.5–43.8) | −8.1 (−12.3 to −6.3) |
| Ct value L-targetd | 29.3 (25.6–30.5) | 43.7 (35.8–45.0) | −12.5 (−14.6 to −7.3) |
- —German Research Foundation10.13039/501100001659
- —Collaborative Research Center
- —Leibniz Association10.13039/501100001664
- —Global Health Protection Programme
- —German Federal Ministry of Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral Infections and Outbreaks Research · Polyomavirus and related diseases · Disaster Response and Management
(See the Editorial Commentary by Platt and Chertow on pages e593–5.)
Lassa fever (LF), caused by Lassa virus (LASV), is a viral hemorrhagic fever endemic in West Africa, particularly in Nigeria, Sierra Leone, and Guinea. Approximately 100 000–300 000 infections are estimated to occur every year [1]. LF is listed as a priority disease in the World Health Organization Research and Development Blueprint for Epidemics because no licensed vaccine is available; hospitalized cases show high case fatality of 15%–30% [2, 3]; and treatment options are limited to off-label use of ribavirin, despite varying evidence for its efficacy [4, 5], and supportive care.
Severe LF may cause neurological complications, such as meningitis, seizures, hearing loss, and other focal deficits as well as altered mental state [6–13], which are strongly associated with fatal disease outcome [10, 14–16]. Despite this, it remains unknown whether LASV directly infects the central nervous system (CNS) and how neurological complications arise. While seizures, confusion, restlessness, and altered mental state may result from metabolic encephalopathy, meningitis and focal deficits suggest direct CNS involvement.
Thus far, LASV RNA [13, 17, 18] or infectious virus [16] has reportedly been detected in CSF of only a few isolated cases presenting with symptoms of (meningo-) encephalitis, such as fever, clinical meningitis, lethargy, hearing loss, dysarthria and dysphagia [18], persistent fever and headache [13], fever, disorientation, somnolence, and seizure [17]. Notably, in 2 patients, LASV RNA was found in cerebrospinal fluid (CSF) but not in blood [13, 17]. Therefore, replication of the virus within the CNS has been discussed as a pathophysiological mechanism for neurological findings similar to Ebola virus disease [19]. It remains unclear whether these findings are incidental or whether LASV may be detected more consistently in CSF.
Other members of the Arenaviridae family, such as Junín virus (JUNV) and lymphocytic choriomeningitis virus (LCMV), are known to be neuroinvasive in humans [20, 21]. Dependent on factors such as viral load and strain, route of transmission, and host immunocompetence, different courses of CNS disease from asymptomatic to lifelong persistent infection and fatal outcome have been described for LCMV in animal models [22]. In mice, LCMV reduces the blood-brain barrier (BBB) integrity through cytotoxic CD8^+^ cell activation [22, 23] to enter the CNS and causes ventricular damage with CSF perfusion into the brain parenchyma, increased intracranial pressure, and seizures [22]. For JUNV, a mouse model showed virus transport from the skin entry portal via peripheral nerves to the CNS [24]. Apart from this, high viremia with BBB bypassing was discussed as another possible entry route explaining variable development of neurological symptoms and outcome [24, 25].
To treat LF more efficiently, it is crucial to understand whether LASV infection affects the CNS and, if so, by which pathomechanisms. Indirect effects such as cytokine-induced neuronal dysfunction, metabolic disturbances, microbleeding or microclotting, and endothelial dysfunction are conceivable. However, 2 cases reported so far with LASV RNA detected in CSF but not in blood suggest that active LASV replication in CNS might play a role [13, 17]. In this study, we aimed to provide further evidence that LASV may directly affect the CNS. To this end, we took advantage of the recent introduction of real-time polymerase chain reaction (PCR) in the LF diagnostic laboratory at Irrua Specialist Teaching Hospital (ISTH). The cycle threshold (Ct) readout of real-time PCR as a measure of virus RNA concentration facilitates a quantitative comparison of virus load in CSF versus plasma. We retrospectively screened the database of the LF diagnostic unit for patients with suspected or laboratory-confirmed LF who underwent lumbar puncture as part of their routine clinical management and had at least 1 CSF sample tested by LASV reverse-transcription polymerase chain reaction (RT-PCR). We then compared LASV RT-PCR results of CSF and plasma.
MATERIALS AND METHODS
Study Design and Data Collection
We conducted a retrospective laboratory-based study at the LF diagnostic laboratory of the Institute of Viral and Emergent Pathogens Control and Research at ISTH, Edo State, Nigeria. ISTH is a national Center of Excellence for LF management and research. It is among the centers with the highest caseload of LF within West Africa. Patients with suspected or laboratory-confirmed LF who underwent lumbar puncture as part of their routine clinical management and had at least 1 CSF sample tested by LASV RT-PCR between 1 January 2021 and 31 October 2023 were included in the study. The decision to send a blood or CSF sample to the laboratory for testing rested solely with the treating physician. A total of 153 pediatric patients meeting these criteria were included in the study. Children with meningism routinely undergo lumbar puncture to test for bacterial meningitis. Table 1 provides a list of major indications for lumbar puncture in children at ISTH, given there are no contraindications [26–29]. A more cautious diagnostic approach is employed at ISTH for adults with meningism and suspected LF due to concerns for clinically relevant bleeding in this population as well as the increased risk of other diseases such as neoplasia.
In the LF diagnostic laboratory, viral RNA was extracted from CSF and plasma samples using the QIAamp Viral RNA Mini Kit (Qiagen). RT-PCR was conducted using the RealStar Lassa Virus RT-PCR Kit 2.0 (Altona Diagnostics). The RT-PCR assay comprises 2 different reactions targeting the viral S and L genome segments, respectively. Ct values, as a proxy of virus RNA concentration, were recorded for both targets.
The patients’ symptoms and demographical data were reported by clinicians on paper-based laboratory request forms. Together with RT-PCR results, this information was recorded in an electronic database of the laboratory. From here, relevant study information was extracted, de-identified, and compiled into a single spreadsheet for further analysis.
Statistical Analysis
Using descriptive statistics, we analyzed demographic and clinical characteristics of CSF-positive and -negative LF patients. To compare the Ct values for CSF and plasma in the same patient, CSF/plasma sample pairs were defined, collected within 1 day of each other. To exclude potential treatment effects of ribavirin, only paired samples taken on admission were included. Wilcoxon signed-rank test was used to test for significant differences between paired samples, Mann–Whitney U test for unpaired samples, and χ^2^ test or Fisher exact test for proportions. A P value of .05 with Bonferroni correction for multiple testing was considered significant. For nonparametric statistical testing, negative RT-PCR results were given a Ct of 45, above the measurement range of the assay. For 2 patients with multiple follow-up samples of plasma and CSF tested by RT-PCR, the Ct kinetics were analyzed longitudinally. The statistical analysis was performed using RStudio 2023.12.1+402, and plots were created with GraphPad Prism 10.2.3.
Ethics Statement
As this study followed a retrospective design with no harm to patients or their privacy due to de-identification of personal data, an exemption from ethical approval and requirement of patient consent was granted by the local ethics committee at ISTH.
RESULTS
Study Population
During the study period, 11 933 plasma or CSF samples were tested by LASV RT-PCR at ISTH, of which 10 287 were initial samples, that is, the first plasma sample taken to confirm the diagnosis and the first CSF sample taken during hospitalization. Among the initial samples, 153 were CSF samples originating from 153 patients (Figure 1). The diagnosis of LF was confirmed by RT-PCR in 49 of 153 (32%) patients with CSF tested. The 49 patients with LF could further be subdivided into 2 groups according to the CSF findings: (A) 42 of 49 (86%) patients tested LASV RNA positive in CSF, and (B) 7 of 49 (14%) patients tested negative in CSF but had positive results for plasma. Most patients in group A (33/42 [79%]) tested LASV RNA positive in both CSF and plasma, while 9 of 42 (21%) patients were CSF positive but their plasma samples were negative. Thus, the majority of LF patients who underwent lumbar puncture due to CNS symptoms had LASV RNA in CSF. In about 20% of these patients, plasma samples tested negative, that is, the diagnosis of LF was confirmed by CSF testing only.
Flowchart of data analysis. The study population comprised all patients with suspected or confirmed Lassa fever with at least 1 cerebrospinal fluid (CSF) sample tested by Lassa virus reverse-transcription polymerase chain reaction (RT-PCR). The RT-PCR results for the different subgroups are indicated. Whenever multiple CSF or plasma samples were available per patient due to follow-up testing, only the initial samples are illustrated to ensure better comparability. Abbreviations: CSF, cerebrospinal fluid; Ct, cycle threshold; IQR, interquartile range; L, reverse-transcription polymerase chain reaction Lassa virus L segment target; LASV, Lassa virus; LF, Lassa fever; RT-PCR, reverse-transcription polymerase chain reaction; S, reverse-transcription polymerase chain reaction Lassa virus S segment target.
LF was not confirmed in 85 of 153 (56%) patients with CSF samples tested; they tested negative in all CSF and plasma samples. In 19 of 153 (12%) patients, LF could not be ruled out with certainty; they were negative in all CSF samples, while PCR for plasma was not conducted (Figure 1).
Demographic and Clinical Characteristics
To explore whether LASV RNA detection in CSF might be associated with demographic or clinical features, the 42 LF patients with LASV RNA–positive CSF were compared with the 7 LF patients with negative CSF as well as with non-LF patients who tested negative in both CSF and plasma (Table 2). The median age of the CSF-positive LF cases was 10.5 years, while the CSF-negative, plasma-positive LF patients were slightly older (median age, 13.0 years; P = .38). Forty-three percent of both groups were female. Non-LF patients had similar sex distribution but were considerably younger than CSF-positive LF patients (P = .04). There were no significant differences in the timespan from symptom onset to first CSF RT-PCR test between the 3 groups. The fatality rate was 7% for the CSF-positive cases, whereas none of the CSF-negative LF patients had fatal outcome. No significant differences were seen with respect to case fatality among the 3 groups.
The most frequently reported symptoms of CSF-positive patients on admission were fever, headache, abdominal pain, vomiting, and general weakness (Table 2). The symptoms of CSF-negative LF patients differed in frequency, but none of the differences were statistically significant due to their small sample size. Non-LF patients generally reported fewer symptoms than CSF-positive LF patients, with only abdominal pain being statistically significant (P < .0001). The clinicians did not report photophobia, hearing loss, disorientation, or coma on the laboratory request forms for any patient. However, in addition to the symptoms in Table 2, the pediatric patients had 1 or several of the CNS symptoms listed as indications for lumbar puncture in Table 1. Which of the indication(s) led to the CSF testing was not recorded in the laboratory database.
Comparative Analysis of Viral Load in CSF and Plasma
The 42 CSF-positive LF patients were first analyzed regardless of a matching CSF and plasma sample pair. Among all patients, the first plasma RT-PCR was performed a median of 8.5 days after symptom onset and the first CSF RT-PCR 11 days after symptoms commenced. Of the 42 patients, 34 (81.0%) had a lower Ct value in their initial CSF RT-PCR compared to their first plasma sample. Accordingly, median Ct values for the initial CSF RT-PCR of all 42 CSF-positive patients were lower than those in the plasma of this group (Table 3). These data point to a higher viral load in CSF. However, due to the time lapse between sampling time points for plasma and CSF in some patients, no firm conclusions could be drawn.
To better compare the viral load between CSF and plasma, we matched CSF and plasma samples collected not more than 1 day apart (Table 3, Figure 2). To exclude potential treatment effects of ribavirin, only paired samples taken on admission were included. For 26 of the 42 patients, sample pairs meeting these criteria were identified. Of the 26 patients, 23 (88%) had a lower Ct value in CSF compared to plasma. Accordingly, the pairs showed significantly lower median Ct values in CSF than in plasma with P < .00001 for S-targets and P < .0001 for L-targets (Table 3), confirming the results for all 42 patients. The Ct values for S- and L-targets were 8.1 and 12.5 units (median), respectively, lower in CSF compared to plasma (Table 3), which roughly corresponds to a 1000-fold higher LASV RNA concentration in CSF versus plasma. A graphical representation of the differences between CSF and plasma Ct for the 26 paired samples is shown in Figure 2. Apart from 3 patients (numbers 16, 37, and 43) with considerably lower overall Ct values (ie, higher viral load), all other patients had lower Ct values in CSF than in plasma and, hence, a higher concentration of LASV RNA in CSF relative to plasma.
Comparison of Lassa virus cycle threshold (Ct) values between matched pairs of cerebrospinal fluid (CSF) and blood plasma for LASV S- and L-targets. Matched CSF and plasma samples were collected not more than 1 day apart from each other on or shortly after admission. Sample pairs meeting these criteria were identified for 26 patients. Each line represents 1 patient. Negative reverse-transcription polymerase chain reaction results are shown below the detection limit. Three patients with lower Ct value in plasma vs CSF are indicated.
Patients 16, 37, and 43 with higher viral load in plasma than in CSF had a fatal outcome. Patients 16 and 43 were infants with severe LF disease. LF presumably occurred due to intrauterine infection in case of patient 16, whose symptom onset was not precisely recorded, and certainly in case of patient 43, whose symptoms commenced the day after delivery. Both infants underwent same day CSF and plasma RT-PCR tests at the age of 17 and 11 days, respectively. Patient 16 exhibited the lowest Ct values of all patients in CSF (S-target, 18.5; L-target, 18.1) and plasma (S-target, 13.3; L-target, 13.2), while patient 43 also showed very high viral load (CSF: S-target, 22.7 and L-target, 23.7; plasma: S-target, 18.6 and L-target, 20.1). The third fatal case (patient 37) was a 5-year-old girl who presented to ISTH with a 9-day history of fever, abdominal pain, diarrhea, nausea, and vomiting. She died on day of admission before further diagnostic modalities could be initiated.
Multiple RT-PCR results for plasma and CSF were available for 2 patients, showing prolonged LASV RNA detection in plasma over 30 and 50 days after symptom onset (26 and 41 days after admission), respectively, combined with late-stage virus RNA detection in CSF on days 23 and 39, respectively (Figure 3). This duration of virus RNA detection in plasma is substantially longer than in most LF patients treated at ISTH [30]. Because the lumbar punctures were only performed in later disease stages, it remains unclear when the CSF samples initially became positive. Patient 9, a 15-year-old girl, was admitted to ISTH on day 8 post–symptom onset with fever, abdominal pain, and headache. When these symptoms had subsided completely, she was discharged on day 30 post symptom onset while she was still LASV RNA positive in plasma. She was readmitted upon the reoccurrence of fever on day 35 when the first lumbar puncture was performed. The CSF RT-PCR tested positive on that day as well as on day 39. She first tested CSF negative on day 50, after which she was discharged again with low levels of LASV RNA detectable in plasma. Patient 11, a 7-year-old girl, presented to ISTH 9 days after symptom onset with fever, headache, vomiting, abdominal pain, and acute kidney and liver injury, as well as highly deranged inflammatory markers. The first CSF RT-PCR was performed on day 24 after the reported symptom onset with a positive result. She tested CSF negative on day 30 and plasma negative on day 36.
Lassa virus cycle threshold values for cerebrospinal fluid (CSF) and plasma of patients 9 and 11 over the course of disease. Both cases show prolonged detection of viral RNA in plasma with late-stage detection of viral RNA in CSF. Negative reverse-transcription polymerase chain reaction results are shown below the detection limit. Abbreviations: CSF, cerebrospinal fluid; Ct, cycle threshold; L, reverse-transcription polymerase chain reaction Lassa virus L segment target; S, reverse-transcription polymerase chain reaction Lassa virus S segment target.
DISCUSSION
In this retrospective laboratory-based study, we frequently observed LASV RNA in CSF of pediatric LF patients who underwent lumbar puncture due to CNS symptoms, primarily those of meningoencephalitis, as listed in Table 1. In some of these patients, the virus was not detected in plasma, and laboratory confirmation of LF required CSF testing. The viral load in CSF was often higher than in plasma, indicating a neuroinvasive infection with active virus replication in CNS.
Our observations raise the question of whether higher viral loads in CSF may be due to the CNS being an immune-privileged site with preferential viral replication or due to other causal mechanisms. Active immune evasion by downregulating the neural major histocompatibility complex class I expression and thereby reducing the effective immune response by cytotoxic T cells as in human immunodeficiency virus-1 (HIV-1) and cytomegalovirus infection should be investigated as potential mechanism in future studies [31–33]. Furthermore, it is conceivable that host factors, such as varying degrees of immunocompromise, may contribute to the likelihood of cerebral involvement [22].
The course of disease in patients 9 and 11, for whom the CSF RT-PCR was conducted several weeks after admission, might suggest that CNS manifestations occurred only in later stages of disease. This suggests that neuroinvasive LASV infection may also present with postacute sequelae. Virus latency in the CNS, dormancy in nerve ganglia, or autoimmune phenomena causing encephalitis present possible pathomechanisms in these patients. The 3 fatal cases had an opposite distribution of viral load compared to the other patients, with higher concentrations in plasma than in CSF. This proposes a different pathomechanism—likely an overwhelming systemic disease with loss of endothelial integrity including in the BBB.
Despite ongoing research, it remains unclear whether LASV is a neurotropic virus in humans. Viruses are known to target the brain in multiple ways, including inflammation (HIV, tick-borne encephalitis virus) [34, 35], direct neurotropic effects (herpes simplex virus [HSV], West Nile virus, Japanese encephalitis virus) [34–37], and thrombosis and bleeding (severe acute respiratory syndrome coronavirus 2 [SARS-CoV-2], varicella zoster virus [VZV]) [37, 38], as well as virus reactivation from dormancy state in the sensory nerve ganglia (HSV, VZV, Ebola virus) [19, 34, 37, 39]. For HSV type 1, which has been studied extensively, retrograde axonal transport along the trigeminal or olfactory nerve with spread to frontal and temporal lobes or hematogenous dissemination has been discussed [40]. Upon reactivation, HSV may infect other neurons by transmission of infectious viral particles [40]. Furthermore, an induction of autoimmune processes resulting from the immune response to the virus has been described. These lead to autoantibody production, particularly, but not limited to, antibodies against the N-methyl-D-aspartate receptor and to autoimmune encephalitis [41, 42]. For arenaviruses, different CNS entry pathways have been described, particularly a BBB crossing for LCMV [22, 23] and axonal transport for JUNV [24]. Dependent on host immunocompetence, viral load, and strain, both acute and chronic neurological sequelae may occur following LCMV and JUNV infection [22, 25]. In particular, virus-induced BBB permeability with trans- and paracellular CNS penetration, the “Trojan-horse method” [43], and (retrograde) axonal transport [24] require further investigation in LASV research as other members of the Arenaviridae family are suspected to utilize them [24, 43].
Our findings have implications for development of drugs against LF, and viral clearance from CSF should be considered in the design of respective clinical trials. Ribavirin, which is used as a standard yet off-label treatment for LF, has been shown to penetrate the BBB if administered intravenously in high concentrations in subacute sclerosing panencephalitis [44] and may therefore meet relevant pharmacokinetic criteria for use in CNS infections. Clinical trials are currently ongoing to evaluate other LF treatments including favipiravir [45], which showed low brain penetrance when tested against CNS manifestations of SARS-CoV-2 [46].
The main limitation of our study is the retrospective design based on existing data from routine clinical management. Although there are indications for lumbar puncture (Table 1), all findings are biased by the decisions made by the treating physicians. Thus, we could include only children in the analysis, because lumbar puncture was not conducted during the study period in adults. It is an invasive procedure that needs to be weighed carefully against potentially significant bleeding complications in patients with viral hemorrhagic fever. For these reasons, this study cannot provide estimates for the prevalence of LASV RNA detection in CSF in patients with LF. It might be ethically challenging to develop a prospective observational study protocol that involves lumbar puncture in all participants in an unbiased way, irrespective of a clinical indication.
Additionally, only general symptoms recorded at the time of patient sampling, based on information provided by the clinician completing the LF diagnostic request form, were available. Signs of meningitis and encephalitis, namely neck stiffness and focal deficits, were not among the symptoms routinely assessed on the RT-PCR request form. We tried to extract further clinical and laboratory information from patient files; however, the data were scattered and not suitable for scientific analysis. Leftover samples were not available for additional analyses. Furthermore, there is the seeming lack of hearing loss, a common neurological complication of LF, among our patients. This complication is more common in the subacute than the acute phase of illness, during which patients are usually hospitalized [6, 11, 47, 48]. In addition, hearing assessments in children are difficult because of the nonavailability of sensitive screening methods for children under the age of 5 and due to the challenges with follow-up assessments in older children. In conclusion, the design of this study did not allow to determine clinical manifestations or laboratory parameters associated with the presence of viral RNA in CSF.
Finally, we cannot present data on infectious particles in CSF. The available data were on LASV RNA only and the RT-PCR may have detected defective virus or free virus RNA.
To address the above-mentioned limitations, prospective studies in adults and children combining a structured clinical neurological examination and laboratory analysis of biomarkers in CSF and plasma are warranted. Multiplex PCR for the most common meningitis and encephalitis pathogens may rule out other infections as a rival cause for neurological symptoms. LASV immunoglobulin G and immunoglobulin M antibody testing will help to clarify in which phase of disease neurological symptoms arise. Viral sequencing may provide information on viral characteristics potentially associated with neuroinvasion. Postmortem minimally invasive tissue sampling will help to uncover how LASV gains access to the CNS and answer if and where the virus persists inside the CNS.
CONCLUSIONS
Our results imply that in endemic areas, LF presents an important differential diagnosis for meningoencephalitis and has to be considered even in cases in which plasma PCR tests remain negative. To advance in clinical management and drug development, LF must be acknowledged as a neuroinvasive infection. The mechanisms by which LASV affects the CNS remain poorly understood, and further research is needed to determine why CNS manifestations occur in certain patients and at which stage of disease neuroinvasive infection arises.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Cormick JB, Webb PA, Krebs JW, Johnson KM, Smith ES. A prospective study of the epidemiology and ecology of Lassa fever. J Infect Dis 1987; 155:437–44.3805771 10.1093/infdis/155.3.437 · doi ↗ · pubmed ↗
- 2Kenmoe S, Tchatchouang S, Ebogo-Belobo JT, et al Systematic review and meta-analysis of the epidemiology of Lassa virus in humans, rodents and other mammals in sub-Saharan Africa. P Lo S Negl Trop Dis 2020; 14:1–29.10.1371/journal.pntd.0008589 PMC 747871032845889 · doi ↗ · pubmed ↗
- 3Akpede GO, Asogun DA, Okogbenin SA, et al Caseload and case fatality of Lassa fever in Nigeria, 2001–2018: a specialist center's experience and its implications. Front Public Health 2019; 7:170.31294014 10.3389/fpubh.2019.00170 PMC 6603170 · doi ↗ · pubmed ↗
- 4Eberhardt KA, Mischlinger J, Jordan S, Groger M, Günther S, Ramharter M. Ribavirin for the treatment of Lassa fever: a systematic review and meta-analysis. Int J Infect Dis 2019; 87:15–20.31357056 10.1016/j.ijid.2019.07.015 · doi ↗ · pubmed ↗
- 5Cheng HY, French CE, Salam AP, et al Lack of evidence for ribavirin treatment of Lassa fever in systematic review of published and unpublished studies. Emerg Infect Dis 2022; 28:1559.35876478 10.3201/eid 2808.211787 PMC 9328902 · doi ↗ · pubmed ↗
- 6Cummins D, Mc Cormick JB, Bennett D, et al Acute sensorineural deafness in Lassa fever. JAMA 1990; 264:2093–6.2214077 · pubmed ↗
- 7Okokhere PO, Bankole IA, Iruolagbe CO, et al Aseptic meningitis caused by Lassa virus: case series report. Case Rep Neurol Med 2016; 2016:1–4.10.1155/2016/1978461 PMC 512445527957363 · doi ↗ · pubmed ↗
- 8Cummins D, Bennett D, Fisher-Hoch SP, Farrar B, Machin SJ, Mc Cormick JB. Lassa fever encephalopathy: clinical and laboratory findings. J Trop Med Hyg 1992; 95:197–201.1597876 · pubmed ↗