A Population-Based Survey on the Prevalence of Postoperative Nausea and Vomiting in the Qassim Region
Mohammed M Almadhi, Mohammed M Aboelseoud, Ahmad K AlGharras, Abdulaziz A Almadud, Emad A Mohamed, Ibrahim M Alshehri, Radwa M Geddawy, Wajd K AlGharras

TL;DR
This study surveyed surgical patients in Saudi Arabia's Qassim region and found that two-thirds experienced nausea or vomiting after surgery, with women and those under general anesthesia being most affected.
Contribution
The study provides region-specific data on postoperative nausea and vomiting prevalence and identifies gender and anesthesia type as key risk factors in the Qassim region.
Findings
72.7% of postoperative patients experienced nausea, vomiting, or retching within 24 hours of surgery.
Female patients had significantly higher PONV rates (76.8%) compared to male patients (62.9%).
General anesthesia was associated with higher PONV occurrence than local anesthesia.
Abstract
Introduction Despite advances in anesthetic techniques and the routine use of prophylactic antiemetics, postoperative nausea and vomiting (PONV) remains a prevalent and distressing complication within the first 24 hours after surgery. It is associated with reduced patient satisfaction, prolonged hospital stays, and increased healthcare costs. This study aimed to assess the prevalence and severity of PONV and to identify associated risk factors among postoperative patients in the Qassim region of Saudi Arabia. Methods A cross-sectional survey was conducted among patients who had undergone surgery under anesthesia in the Qassim Province of Saudi Arabia. Data were collected using a structured, self-administered questionnaire covering demographic and clinical variables, along with the validated Rhodes index of nausea, vomiting, and retching (RINVR) to quantify PONV severity. Design…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
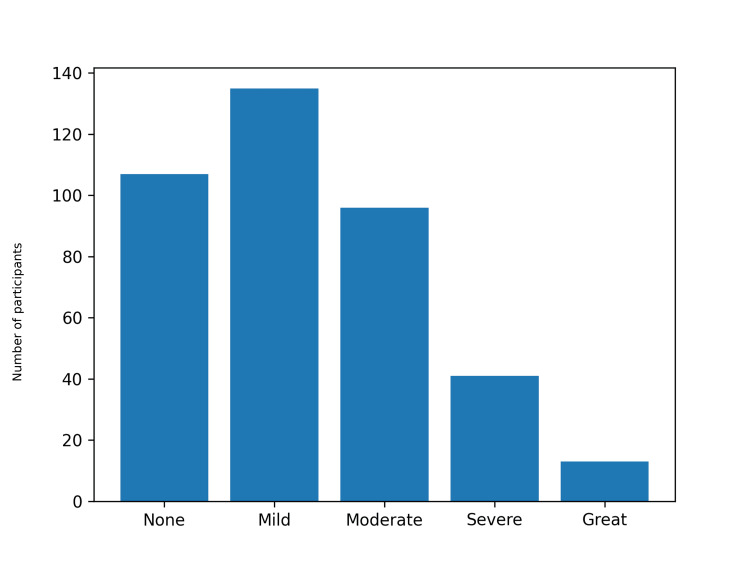 Figure 1
Figure 1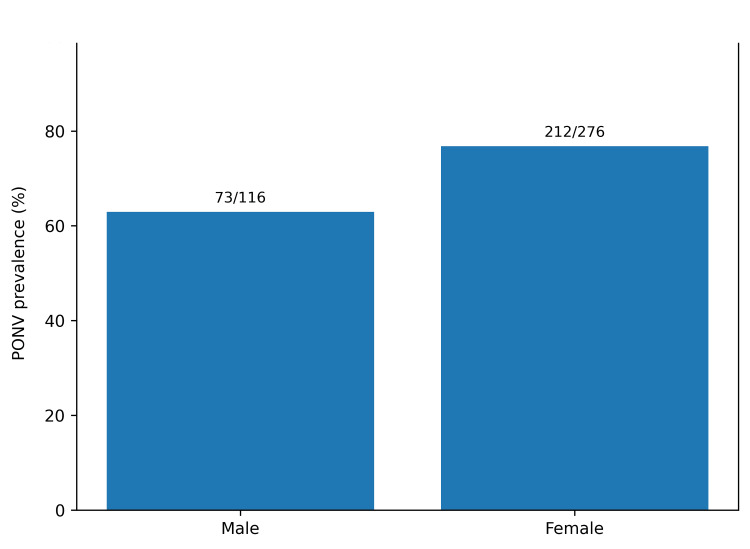 Figure 2
Figure 2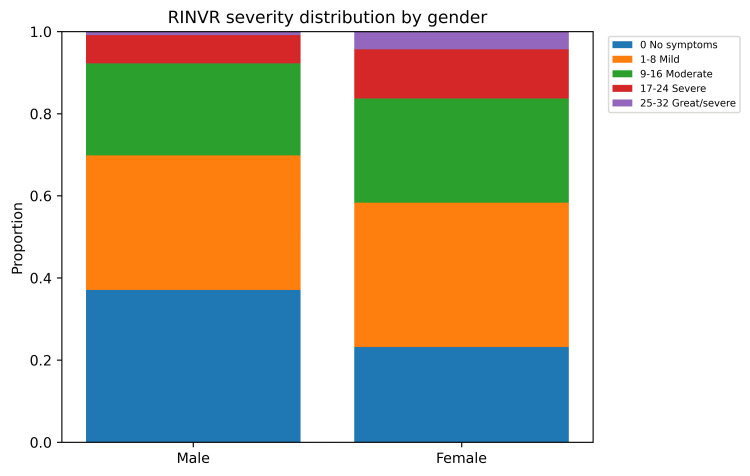 Figure 3
Figure 3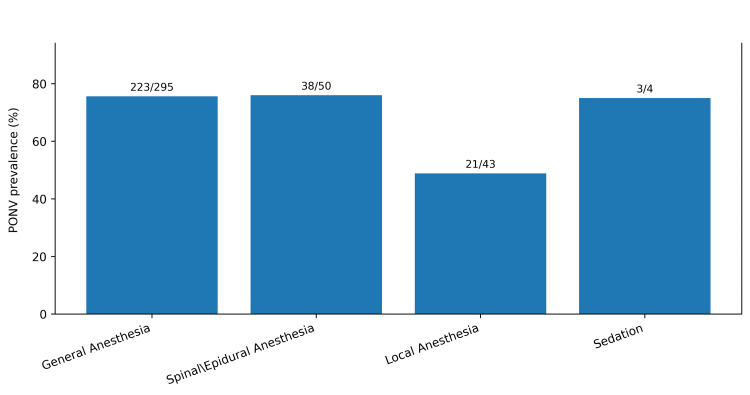 Figure 4
Figure 4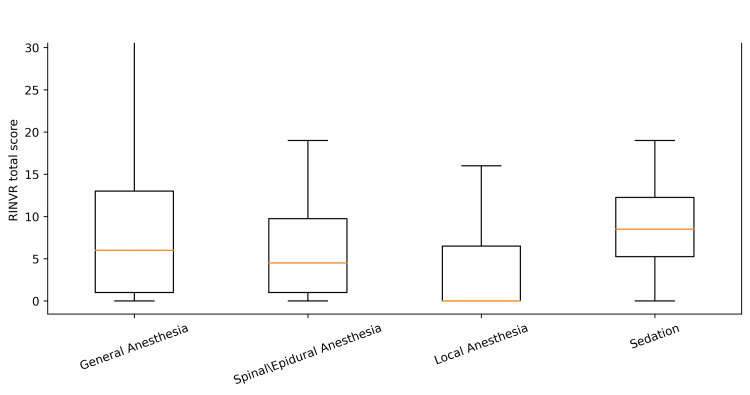 Figure 5
Figure 5| Variable | Category | n (%) |
| Gender | Male | 116 (29.6%) |
| Female | 276 (70.4%) | |
| Age group (years) | <18 | 20 (5.1%) |
| 18-24 | 87 (22.2%) | |
| 25-34 | 79 (20.2%) | |
| 35-44 | 92 (23.5%) | |
| 45-54 | 66 (16.8%) | |
| 55-64 | 40 (10.2%) | |
| 65+ | 8 (2.0%) | |
| Weight group (kg) | <50 | 33 (8.4%) |
| 50-69 | 125 (31.9%) | |
| 70-79 | 99 (25.3%) | |
| 80-89 | 68 (17.3%) | |
| 90+ | 67 (17.1%) | |
| Anesthesia type | General anesthesia | 295 (75.3%) |
| Spinal or epidural | 50 (12.8%) | |
| Local anesthesia | 43 (11.0%) | |
| Sedation | 4 (1.0%) | |
| Type of surgery | General surgery | 129 (32.9%) |
| Obstetrics or gynecological surgery | 103 (26.3%) | |
| ENT surgery | 56 (14.3%) | |
| Orthopedic surgery | 42 (10.7%) | |
| Urological surgery | 23 (5.9%) | |
| Plastic surgery | 18 (4.6%) | |
| Ophthalmic surgery | 10 (2.6%) | |
| Cardiothoracic surgery | 7 (1.8%) | |
| Neurosurgery | 2 (0.5%) | |
| Missing or not reported | 2 (0.5%) |
| Outcome | n | % |
| Any PONV (RINVR total >0) | 285 | 72.70% |
| Any nausea | 262 | 66.80% |
| Any vomiting | 168 | 42.90% |
| Any retching | 166 | 42.30% |
| Any distress (due to PONV) | 233 | 59.40% |
| RINVR severity: 0 (no symptoms) | 107 | 27.30% |
| RINVR severity: 1-8 (mild) | 135 | 34.40% |
| RINVR severity: 9-16 (moderate) | 96 | 24.50% |
| RINVR severity: 17-24 (severe) | 41 | 10.50% |
| RINVR severity: 25-32 (great/severe) | 13 | 3.30% |
| Variable | Category | PONV positive n/N (%) | Incidence test statistic | Incidence p-value | RINVR median (IQR) | Severity test statistic | Severity p-value |
| Gender | Male | 73/116 (62.9%) | χ²=7.25, df=1 | 0.007 | 4 (0-9) | Z=3.29 | 0.001 |
| Gender | Female | 212/276 (76.8%) | 6 (1-13) | ||||
| Anesthesia type | General anesthesia | 223/295 (75.6%) | χ²=13.87, df=3 | 0.003 | 6 (1-13) | H=13.93, df=3 | 0.003 |
| Anesthesia type | Spinal/epidural | 38/50 (76.0%) | 4 (1-10) | ||||
| Anesthesia type | Local anesthesia | 21/43 (48.8%) | 0 (0-6) | ||||
| Anesthesia type | Sedation | 3/4 (75.0%) | 8 (5-12) | ||||
| Age group | <18 | 15/20 (75.0%) | χ²=4.17, df=6 | 0.654 | 5 (2-11) | H=6.93, df=6 | 0.327 |
| Age group | 18-24 | 64/87 (73.6%) | 8 (0-16) | ||||
| Age group | 25-34 | 62/79 (78.5%) | 6 (2-11) | ||||
| Age group | 35-44 | 67/92 (72.8%) | 6 (0-12) | ||||
| Age group | 45-54 | 42/66 (63.6%) | 5 (0-9) | ||||
| Age group | 55-64 | 29/40 (72.5%) | 6 (0-11) | ||||
| Age group | 65+ | 6/8 (75.0%) | 4 (2-5) | ||||
| Weight group | <50 kg | 20/33 (60.6%) | χ²=4.73, df=4 | 0.316 | 6 (0-15) | H=6.68, df=4 | 0.154 |
| Weight group | 50-69 kg | 98/125 (78.4%) | 7 (1-14) | ||||
| Weight group | 70-79 kg | 70/99 (70.7%) | 5 (0-10) | ||||
| Weight group | 80-89 kg | 49/68 (72.1%) | 6 (0-11) | ||||
| Weight group | ≥90 kg | 48/67 (71.6%) | 6 (0-12) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNausea and vomiting management · Enhanced Recovery After Surgery · Pregnancy and Medication Impact
Introduction
Postoperative nausea and vomiting (PONV) is classically defined as nausea and/or vomiting occurring within 24 hours after surgery. It is among the most common and unpleasant complications of anesthesia and surgery and is reported as the second most frequent postoperative issue after pain [1]. PONV reduces overall patient comfort and satisfaction, may prolong hospital recovery, and ultimately increases healthcare costs [2]. Multiple studies have identified a variety of risk factors for PONV, including patient-specific factors (such as younger age, female sex, non-smoker status, history of motion sickness, and prior PONV) and anesthesia-related factors (notably the use of volatile anesthetics, nitrous oxide, mask ventilation, and perioperative opioids) [3]. Surgical factors, including the type and duration of the procedure, as well as inadequate perioperative hydration, have also been linked to higher PONV risk [3]. PONV may prolong a patient’s hospital stay by approximately 30 minutes on average [4]. Despite advances in anesthetic agents and surgical techniques, the incidence of PONV has remained relatively unchanged over recent decades [5]. Currently, antiemetics are routinely administered preoperatively and postoperatively; yet PONV continues to be a pressing clinical issue that affects a substantial proportion of surgical patients [6].
In light of these challenges, we conducted a population-based study in the Qassim region of Saudi Arabia to determine the current prevalence of PONV and identify associated risk factors in surgical patients. The primary objective was to quantify the prevalence of PONV in the first 24 hours after surgery and examine factors associated with its occurrence. Secondary objectives included assessing symptom severity using a validated nausea, vomiting, and retching severity scale and evaluating the relationships between PONV and patient demographics (age, gender, weight), as well as the type of anesthesia (general, regional, local, or sedation).
Materials and methods
Study design
This study was a cross-sectional, community-based survey conducted in the Qassim region of the Kingdom of Saudi Arabia. We utilized an online self-administered questionnaire to collect data from postoperative patients. The study was carried out over a four-month period.
Study population
Eligible participants were residents of Qassim who had undergone surgical procedures involving any form of anesthesia. Inclusion criteria were broad: we included male and female patients of any age who underwent surgery under general, regional (e.g., spinal or epidural), or local anesthesia, or sedation. There were no restrictions based on previous PONV history, smoking status, body mass index, comorbidities (e.g., diabetes), type of surgery (elective or emergency), surgical technique, or bowel preparation. Participants were required to understand and complete the questionnaire in Arabic or English. Patients were excluded if their surgery was an outpatient procedure with less than 12 hours of postoperative observation or if they had cognitive or language barriers preventing understanding of the survey.
Sample size and sampling
We initially estimated that a sample of approximately 323 participants would be needed to estimate a PONV prevalence of ~30% with a 95% confidence level and ±5% precision. To account for subgroup analyses and possible nonresponse, we aimed to recruit at least 500 participants. Participants were recruited through convenience sampling, including online distribution of the survey link via social media, community forums, and QR codes posted in clinics and hospitals across the region. Ultimately, 392 participants completed the survey.
Data collection
Data were collected using a structured electronic questionnaire (via Google Forms). The questionnaire was divided into sections capturing: (1) demographic information (age, gender, and weight), (2) clinical and surgical information (type of surgery and type of anesthesia received), and (3) PONV outcomes measured by the Rhodes index of nausea, vomiting, and retching (RINVR) [7]. The RINVR is a validated instrument consisting of eight items that assess nausea, vomiting, and retching frequency, amount, and distress, each rated from 0 (none) to 4 (severe) [7]. The scores are summed to yield a total RINVR score ranging from 0 to 32, with higher scores indicating more severe nausea and vomiting symptoms [7]. In this study, any total RINVR score >0 was considered indicative of PONV (i.e., any presence of nausea, vomiting, or retching) [7]. For descriptive purposes, we categorized RINVR severity as: no symptoms (score 0), mild (1-8), moderate (9-16), severe (17-24), and great severity (25-32), based on the instrument’s descriptors [7]. No personally identifiable data were collected; all responses were anonymous, and participation was voluntary. The survey introduction explained the study’s purpose, how the data would be used, and assured participants of confidentiality. Informed consent was obtained electronically from each participant before proceeding to the questionnaire. Participants were free to discontinue the survey at any time without penalty. All responses were automatically recorded and stored securely in a password-protected electronic database accessible only to the research team.
Variables and definitions
The primary outcome was the occurrence of PONV within 24 hours post-surgery, defined as any RINVR score >0 (i.e., any nausea, vomiting, or retching). The secondary outcome was PONV severity as measured by the total RINVR score (0-32). Key independent variables included patient demographics (age, gender, and weight), type of anesthesia (general, spinal/epidural, regional, local, or sedation), and type of surgery. Age and weight were analyzed as categorical variables (age groups: <18, 18-24, 25-34, 35-44, 45-54, 55-64, ≥65 years; weight groups: <50, 50-69, 70-79, 80-89, and ≥90 kg). We also recorded whether the patient had any previous surgery (yes/no) as a characteristic of the sample.
Data analysis
All analyses were performed using IBM SPSS Statistics version 28 (IBM Corp., Armonk, NY). Categorical variables are presented as frequencies and percentages, and continuous variables are summarized as means with standard deviations or medians with interquartile ranges, as appropriate to their distribution. Bivariate comparisons were conducted to explore factors associated with PONV. Chi-square tests (or Fisher’s exact test when expected cell counts were low) were used for categorical variables, and independent-samples t-tests or nonparametric equivalents (Mann-Whitney U test for two groups; Kruskal-Wallis test for multiple groups) were used for continuous or ordinal outcomes. Spearman’s rank correlation was used to assess the relationship between age and total RINVR score. Total RINVR scores are reported as medians with interquartile ranges. A p-value <0.05 was considered statistically significant.
Ethical considerations
The study protocol was reviewed and approved by the Research Ethics Committee of Qassim Health Cluster (ethical approval number 607-47-2236; committee registration number H-04-Q-001) prior to data collection. All participants provided informed consent at the beginning of the online survey. The consent form described the study’s purpose and procedures, emphasized that participation was voluntary, and stated that responses would be kept confidential and used solely for research purposes. No personal identifiers were collected. All data were stored in a secure, password-protected electronic system, with access limited to the research team.
Results
Participant characteristics are presented in Table 1. PONV occurred in 285 of 392 participants (72.7%), defined as a total RINVR score greater than 0 [7]. Nausea was reported by 262 participants (66.8%), vomiting by 168 (42.9%), retching by 166 (42.3%), and distress related to symptoms by 233 (59.4%) (Table 2). The total RINVR score ranged from 0 to 32, with a mean of 7.7 (SD 7.7) and a median of 6 ( interquartile range (IQR) 0-11) [7]. Severity categories were: none 107 (27.3%), mild 135 (34.4%), moderate 96 (24.5%), severe 41 (10.5%), and great severity 13 (3.3%) (Figure 1). PONV incidence was higher in females than in males (212/276, 76.8% vs. 73/116, 62.9%). This difference was statistically significant (chi-square=7.25, df=1, p=0.007) (Table 3, Figure 2). Total RINVR scores were higher in females (median 6, IQR 1-13) than in males (median 4, IQR 0-9) (Mann-Whitney U test, Z=3.29, p=0.001) (Table 3, Figure 3) [7]. PONV incidence differed by anesthesia type (chi-square=13.87, df=3, p=0.003) (Figure 4). Local anesthesia had the lowest incidence (21/43, 48.8%) compared with general anesthesia (223/295, 75.6%), spinal or epidural anesthesia (38/50, 76.0%), and sedation (3/4, 75.0%) (Table 3). Total RINVR scores differed by anesthesia type (Kruskal-Wallis H=13.93, df=3, p=0.003) (Table 3, Figure 5) [7]. Age group and weight group were not associated with PONV incidence (age: chi-square=4.17, df=6, p=0.654; weight: chi-square=4.73, df=4, p=0.316). Total RINVR scores did not differ by age group or weight group (age: Kruskal-Wallis H=6.93, df=6, p=0.327; weight: Kruskal-Wallis H=6.68, df=4, p=0.154) (Table 3) [7]. Age was not correlated with total RINVR score (Spearman’s rho=-0.113, p=0.654) [7].
RINVR severity distributionBars show the number of participants in each severity category (n=392) [7].RINVR: Rhodes index of nausea, vomiting, and retching
PONV prevalence by genderBars show the percentage of participants with PONV (RINVR total >0) by gender (n=392) [7].PONV: postoperative nausea and vomiting; RINVR: Rhodes index of nausea, vomiting, and retching
PONV severity distribution by genderStacked bars show the proportion of male and female patients in each RINVR severity category (none, mild, moderate, severe, and great/severe). Female patients had a higher overall incidence of PONV and greater symptom severity compared with male patients [7].PONV: postoperative nausea and vomiting; RINVR: Rhodes index of nausea, vomiting, and retching
PONV prevalence by anesthesia typeBars show the percentage of participants with PONV (RINVR total >0) by anesthesia type (n=392) [7].PONV: postoperative nausea and vomiting; RINVR: Rhodes index of nausea, vomiting, and retching
Distribution of total RINVR scores by anesthesia typeTotal RINVR score by anesthesia type. Box plot of total RINVR scores (0-32) by anesthesia type (n=392). The box represents the IQR, and the center line represents the median [7].RINVR: Rhodes index of nausea, vomiting, and retching; IQR: interquartile range
Discussion
This cross-sectional survey indicates a high burden of PONV among postoperative patients in the Qassim region. The overall rate is higher than that commonly reported in general surgical populations, which is often around 20% to 30% [8]. At the same time, rates in higher-risk settings have been reported to approach 70% to 80% [8]. A multicenter bariatric surgery cohort reported early PONV at similarly high levels [9]. Taken together, these comparisons suggest that many patients in our setting fall into higher-risk profiles and would benefit from consistent prevention strategies.
The high burden observed in this study likely reflects a combination of patient- and perioperative-related risk factors. A large proportion of participants received general anesthesia, and the sample included many women, both of which are recognized risk factors in established models [10]. This finding has practical implications. PONV prevention in routine care should begin with structured risk assessment and standardized prophylaxis rather than relying solely on clinician preference.
Female sex was associated with higher PONV incidence and greater symptom burden in this cohort. This direction of association aligns with extensive literature identifying female sex as one of the strongest predictors of PONV [10]. Large-scale analyses report higher odds of PONV in women compared with men, and this effect persists across age groups [10]. Proposed mechanisms include hormonal influences and biological differences in nausea and vomiting pathways. From a clinical perspective, these findings support classifying female patients as higher risk and applying prophylaxis accordingly, especially when other risk factors are present.
Anesthesia type was also associated with both PONV incidence and symptom severity. Evidence consistently identifies volatile inhalational anesthetics as a major modifiable contributor to PONV [10]. In prior syntheses, volatile anesthesia increased the risk of PONV compared with total intravenous anesthesia [10]. General anesthesia may also increase exposure to perioperative opioids and other emetogenic factors. In contrast, regional techniques and propofol-based approaches are linked to lower PONV rates in many settings [10]. These findings support selecting less emetogenic techniques when clinically appropriate and ensuring multimodal prophylaxis when volatile-based general anesthesia is required.
In our analyses, age was not associated with PONV incidence or severity. Some models suggest that PONV risk decreases with increasing age [10]. Other studies, especially in single-institution cohorts or specific procedures, report no independent age effect after adjustment for other factors [11]. Differences in case mix, prophylaxis patterns, and the age distribution within a sample can influence whether an age effect is detectable. In addition, prophylaxis practices may attenuate observed differences between age groups if clinicians target younger patients for more aggressive prevention.
We also did not observe evidence that body weight was associated with PONV incidence or severity. Although earlier hypotheses proposed a higher risk with obesity, more recent evidence does not support a strong independent association. A systematic review found no meaningful differences in PONV across BMI categories and concluded that obesity is not an independent risk factor [12]. These findings support focusing perioperative prevention efforts on stronger predictors, such as sex and anesthetic exposures, rather than weight alone [12].
Beyond incidence, we assessed symptom burden using the RINVR. Severity patterns were consistent with the risk patterns observed for PONV incidence, supporting the internal consistency of findings across outcome definitions. The RINVR has established validity and reliability in postoperative settings [13]. Prior evaluations report strong internal consistency and correlation with emetic episodes [13]. In this study, the use of the RINVR provided details beyond a binary definition of PONV and allowed a more granular assessment of symptom burden. As with any self-reported instrument, responses may be influenced by recall and comprehension, particularly when symptoms are severe. Even so, the instrument remains a practical tool for measuring PONV severity in clinical research [13].
Several limitations should be considered. The cross-sectional design does not permit causal inference. The online, self-reported survey approach introduces potential recall and selection bias. We did not capture several established predictors, including smoking status, prior PONV or motion sickness, perioperative opioid exposure, nitrous oxide use, and procedure duration. The sample was drawn from a single region, which may limit generalizability. These limitations underscore the need for future prospective studies with standardized perioperative documentation and prophylaxis protocols.
Despite these limitations, the study provides baseline evidence on PONV burden in a Middle Eastern surgical population and identifies clear targets for improvement. Future work should follow patients prospectively through the first 24 to 48 hours postoperatively, record anesthetic and analgesic exposures in detail, and measure adherence to consensus prophylaxis guidelines. Interventional studies comparing total intravenous anesthesia with inhalational techniques, or testing combination antiemetic regimens in higher-risk groups, would directly inform local practice. This progression from prevalence measurement to targeted prevention studies is needed to improve postoperative comfort and recovery.
Conclusions
PONV was common among postoperative patients in the Qassim region, affecting 72.7% of participants. Female sex and anesthesia type were associated with higher PONV incidence and higher RINVR scores, whereas age and weight were not associated with PONV in this sample. These findings support routine PONV risk assessment and targeted prophylaxis for higher-risk patients, including multimodal antiemetic strategies and the use of less emetogenic anesthetic techniques when feasible. Future prospective studies should evaluate local prophylaxis practices and interventions aimed at reducing the burden of PONV.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Identification of risk factors for postoperative nausea and vomiting in the perianesthesia adult patient J Perianesth Nurs Murphy MJ Hooper VD Sullivan E Clifford T Apfel CC 377384212006 https://doi.org/10.1016/j.jopan.2006.09.0021716974710.1016/j.jopan.2006.09.002 · doi ↗ · pubmed ↗
- 2Postoperative nausea and vomiting after oral and maxillofacial surgery: a prospective study Int J Oral Maxillofac Surg Dobbeleir M De Coster J Coucke W Politis C 7217254720182930167510.1016/j.ijom.2017.11.018 · doi ↗ · pubmed ↗
- 3Incidence and factors associated with postoperative nausea and vomiting among elective adult surgical patients at University of Gondar Specialized Hospital, Northwest Ethiopia, 2019: a cross-sectional study Int J Surg Open Ahmed SA Lema GF 5761222020 https://doi.org/10.1016/j.ijso.2020.01.001
- 4Postoperative nausea and vomiting following inpatient surgeries in a teaching hospital: a retrospective database analysis Curr Med Res Opin Habib AS Chen YT Taguchi A Hu XH Gan TJ 10931099222006 https://doi.org/10.1185/030079906 X 1048301684654210.1185/030079906 X 104830 · doi ↗ · pubmed ↗
- 5Prevalence and risk factors of post-operative nausea and vomiting in a tertiary-care hospital: a cross-sectional observational study Med J Armed Forces India Sinha V Vivekanand D Singh S 062782022 https://doi.org/10.1016/j.mjafi.2020.10.02410.1016/j.mjafi.2020.10.024PMC 948577236147426 · doi ↗ · pubmed ↗
- 6Guideline for the management of postoperative nausea and vomiting J Obstet Gynaecol Mc Cracken G Houston P Lefebvre G 600607302008 https://www.sciencedirect.com/science/article/pii/S 170121631632895 X 10.1016/s 1701-2163(16)32895-x 18644183 · doi ↗ · pubmed ↗
- 7The index of nausea, vomiting, and retching: a new format of the lndex of nausea and vomiting Oncol Nurs Forum Rhodes VA Mc Daniel RW 889894261999 https://pubmed.ncbi.nlm.nih.gov/10382187/10382187 · pubmed ↗
- 8Prevalence of postoperative nausea and vomiting: a systematic review and meta-analysis Saudi J Anaesth Amirshahi M Behnamfar N Badakhsh M Rafiemanesh H Keikhaie KR Sheyback M Sari M 48561420203199802010.4103/sja.SJA_401_19PMC 6970369 · doi ↗ · pubmed ↗